
Abstract
Manhood values are highly prioritized among most culturally orientated South African Black communities with an ideology that revolves around the concept of masculinity. The notion of manhood values is deeply rooted in male dominance, sexual drive, and traditional male circumcision. The goals of this study were to (a) explore the experiences of school health nurses in the provision of sexual and reproductive health among adolescent boys; and (b) recommend suggested action to develop adolescent boys to adapt a healthy behavioral lifestyle through a health-promoting school program. This study employed a qualitative approach utilizing a descriptive and exploratory research design. The Ottawa Charter for Health Promotion was used to guide the study. Purposive sampling was used to select participants for individual interviews to collect data. A total of 21 school health nurses were selected to participate in face-to-face interviews. A thematic analysis was conducted using ATLAS ti (version 8) software. Five overarching themes were yielded and categorized as facilitators, barriers, and suggested action to improve sexual and reproductive health services as follows: (a) legislative frameworks and policies; (b) male medical circumcision, and prevention of HIV/AIDS and STIs; (c) lack of support from teachers and school-governing bodies; (d) risky sexual behaviors among the learners; and (e) empowerment and personal skills development. The study concludes with a discussion and recommendations that a comprehensive health-promoting school program should be developed for adolescent boys with guaranteed ownership and sustainability of male sexual and reproductive health.
Keywords
Manhood values are highly prioritized among most culturally orientated South African Black communities with an ideology that revolves around the concept of masculinity (Meyer, 2017; Morrell, 2015; Siweya et al., 2018). The notion of manhood values is highly embedded in male dominance, sexual drive, and traditional male circumcision (Siweya et al., 2018). Meyer (2017) stated that according to traditional manhood values, the concept of “a real man” is deeply rooted and is not without responsibilities. Much pressure is asserted on a man, not only to become a “real man” but also to be a “good man.” The two concepts are used interchangeably and synonymously. Being a “real” man and a “good” man are strongly related to the concept of fatherhood (Meyer, 2017). Manhood values embrace the concept of a “real man” into two roles of fatherhood which include: providing guidance to one’s children and providing for the family biological and financial needs (Meyer, 2017; Rudwick & Posel, 2015).
Masculinity Challenges in the South African Context
In South Africa, masculinity has evolved recently to be a complex concept amongst Black communities within the transformation process of a sociocultural identity (Rudwick & Posel, 2015). The complexity of masculinity is observed among young men and boys through the rise of negative, risky, and unhealthy behaviors including: sexual coercion, teenage pregnancy, multiple partners, sexually transmitted infections (STIs), and HIV/AIDS (Nyembezi et al., 2010; Rudwick & Posel, 2015). In the past three decades, a high increase in traditional male circumcision deaths and complications related to masculinity complexity have been reported in South Africa (World Health Organization, 2016). Because of the current complexity of sociocultural transformation, a majority of adolescent boys start to have sex at an early age of 16 years and below, which is contrary to the acceptable cultural norms and parental guidance (Richter et al., 2015; Zuma et al., 2010). Early sexual debut among young women and men (commonly defined as having first sexual intercourse at or before age 14 years) is associated with male dominance, poor educational achievement as a result of withdrawal from school, and inability to build adult partnerships with loss of marriage prospects (Richter et al., 2015). In response to the high increase of gender-based violence (GBV) cases reported in the media, social actions against male perpetrators are very common in South Africa as an effort to fight risky behaviors imposed on women. For example, recently, thousands of angry protesters marched to the Parliament demanding action from the State President to address GBV, rape, and murder of girls and women by men (Payne, 2019). GBV is one of the reasons that the South African government has embarked on a strategy to develop a school health program to empower girls under the philosophy of reengineering of primary health care (Bheekie & Bradley, 2016; Department of Health, 2015).
Male Sexual and Reproductive Health
Interventions focusing on adolescent boys in addressing health problems such as the increasing HIV/AIDS statistics, GBV, and teenage pregnancy are undeniably imperative (Notole & Kheswa, 2017; Zuma et al., 2010). For several decades in South Africa, sexual and reproductive health (SRH) services have largely ignored boys and put more emphasis on reactionary responses to address SRH-related problems targeting mainly girls and women as victims (Notole & Kheswa, 2017; Varga, 2001). Male SRH should include promoting sexual health and adolescent development, healthy intimate relationships, safe sexual behavior, and responsible fatherhood (Marcell et al., 2011). Effective SRH services enable young people to delay sexual activity and improve their contraceptive use when they begin to have sex (Boonstra, 2011; Richter et al., 2015).
Health-Promoting Schools
Schools are important institutions where teaching and learning occur and new life skills are imparted to pupils (Department of Health, 2015). They are also important social spaces in which sexuality and sexual behavior converge with particular clarity (Hayter et al., 2008). Schools are a setting for health promotion, and hence the concept of health-promoting schools (HPS) based on the Ottawa Charter for Health Promotion has been globally adopted (Du Plessis et al., 2014; World Health Organization, 1986). Currently, the main role of school health nurses (SHNs) is to focus on screening common health conditions affecting school pupils, on site primary health-care services and health education (Table 1). An HPS is described as a space where all members of the school community work together to provide pupils with integrated and positive experiences and structures, which promote and protect their health (Du Plessis et al., 2014). The aim of this study is to (a) explore the experiences of school health nurses in the provision of sexual and reproductive health among adolescent boys; and (b) recommend suggested action in developing adolescent boys to adapt a healthy behavioral lifestyle through the HPS program.
The Role of School Health Nurses for Senior Phase Pupils (Grades 8–12)

Source: National Department of Health & Integrated School Health Policy 2012.
Methodology
Research Design
This study adopted a qualitative approach utilizing a descriptive and exploratory research design. Semi-structured, face-to-face interviews were conducted with 21 SHNs. The study utilized the Ottawa Charter as a model to guide male sexual reproductive health services improvement targeting adolescent boys in HPS setting as incorporated in the national and provincial KwaZulu-Natal (KZN) Department of Health (Department of Health, 2015; KZNDoH, 2019). The study applied the five key action areas of the Ottawa Charter to structure the interview questions, which include: building healthy public policy; creating supportive environments; strengthening community action; developing personal skills; and reorienting health-care services (Department of Health, 2015; World Health Organization, 1986).
Study Setting
The study was conducted at the selected 21 primary health-care clinics located at eThekwini district in Durban City of KZN Province. eThekwini is a densely populated urban metropolitan district with 3.52 million population (about one-third of KZN’s population of 11.1 million) in 2015–2016 (KZNDoH, 2020). eThekwini is one of the 11 districts in the KZN province. The majority of the population in eThekwini is Black (71.9%), followed by Indian/Asian (16.3%), and colored (2.2%; KZNDoH, 2020). Each clinic had an SHN who was allocated to a number of schools within their perimeter.
Population and Sampling
The total study sample was composed of 21 female SHNs working in the public schools of eThekwini district among a total population of 44 clinical nurse practitioners (21 SHNs + 23 other professional nurses). Purposive sampling was employed to select only clinics with SHNs who met the study’s inclusion selection criteria, which included: a professional nurse; minimum 1-year experience in school health nursing from the three subdistricts (South, West, and North); and providing services to schools in urban, suburban, peri-urban, and rural areas. Only these three subdistricts provided school health services to public schools. The SHNs were selected per clinic rather instead of per school. There were 21 female SHNs who participated in this study; no male nurses were employed as SHNs in the selected clinics.
Data Collection
Individual face-to-face interviews were conducted in English until data saturation was reached. Data collection was conducted using a semistructured interview guide; a digital voice recorder was used to record interviews. Interviews were verbatim transcribed in order to accurately reflect participants’ views. Each interview lasted from 45 min to 1 hr, and provided a narration of the understanding and experiences of SHNs working with adolescent pupils in school health services. An open-ended question was asked in the interviews: “What are your experiences in delivering the sexual and reproductive health in schools among adolescent boys from age 10 to 19 years old?” The researcher also asked relevant probing questions to allow participants to share more information freely without fear or prejudice. Probing questions included: “Can you please tell me more about the current available policies that facilitate sexual and reproductive health at school?” “How accessible are medical male circumcision services in Kwa-Zulu Natal province?” “Are schools supporting the provision of sexual and reproductive health for adolescent boys?” “What health promotion activities are available at schools for boys related to sexual and reproductive health?”
Ethical Considerations
Data were collected after researchers obtained an ethical clearance certificate from the Humanities and Social Sciences Research Ethics Committee at the University of Kwa-Zulu Natal (Reference Number: HSS/1448/015M). Permission to conduct the study was obtained from each community health center involved in the study, the selected health District Department of Health, and Kwa-Zulu Natal Provincial Department of Health (Reference Number: 345/15). Consent from all participants was obtained through written and signed informed consent forms.
Data Analysis
The collected data were analyzed and presented utilizing a thematic analysis method, which emphasizes examining, pinpointing, and recording patterns within data (Miles et al., 2013). Data were analyzed by first transcribing the interviews verbatim and prepared for analysis using ATLAS ti (version 8) software. The three researchers of this study analyzed the data. A six-phase process was used to enable data organization, which included: (a) familiarization with the data, (b) generating initial codes, (c) searching for themes among codes, (d) reviewing the themes, (e) naming themes, and (f) producing the final report (Braun and Clarke, 2006). The themes emerged from the data as follows: repeating ideas, indigenous terms, shifts in topic, and similarities and differences of participants’ linguistic expression of the interviewers (Braun and Clarke, 2006). Data excerpts were used to qualify these themes. Themes and categories were compared with those identified by the researcher. There were similarities and differences in the categories and themes.
Trustworthiness of Findings
Validity and Reliability
Two peer researchers were requested to check the transcripts of the collected data with clear written instructions to ensure validity and reliability (Streubert & Carpenter, 2007). They also categorized and developed themes from the data. Categories and themes were compared with those identified by the primary researchers. The researchers constantly maintained alertness against bias by opposing personal opinions against the collected data. Similar themes were adopted and the different codes were re-examined, regrouped, and given new names (Streubert & Carpenter, 2007).
Dependability, Credibility, and Confirmability
The study used Guba’s model of trustworthiness to ensure appropriateness of inquiry through dependability. There was consistency across the process of study, time taken by the primary researchers and peer researchers, and the analysis techniques—all of which rest on credibility and confirmability (Lincoln & Guba, 2005).
Results
Data analysis yielded five overarching themes inclusive of facilitators, barriers, and suggested action to improve SRH services as follows:
Legislative Frameworks and Policies
Most participants were cognizant of the Integrated School Health Policy (ISHP) of 2012 as a policy that facilitates SHNs to deliver health education and promotion of SRH to all learners in different developmental stages (Table 2). This policy is in line with the key area of the Ottawa Charter—the development of healthy public policies. It also requires all boys specifically in the senior phase to be informed about the health benefits of male medical circumcision (MMC).
The Integrated School Health Policy (ISHP) of 2012 is one example of the policies that speaks specifically to boys in the senior phase to inform them about the health benefit of MMC. [Participant #3] We have a list of policies addressing SRH in South Africa, but they address the needs of all school children in general from grade 1 to 12 and do not speak specifically to sexual and reproductive health challenges facing boys. [Participant #15]
Policies Addressing Sexual Reproductive Health in South Africa.
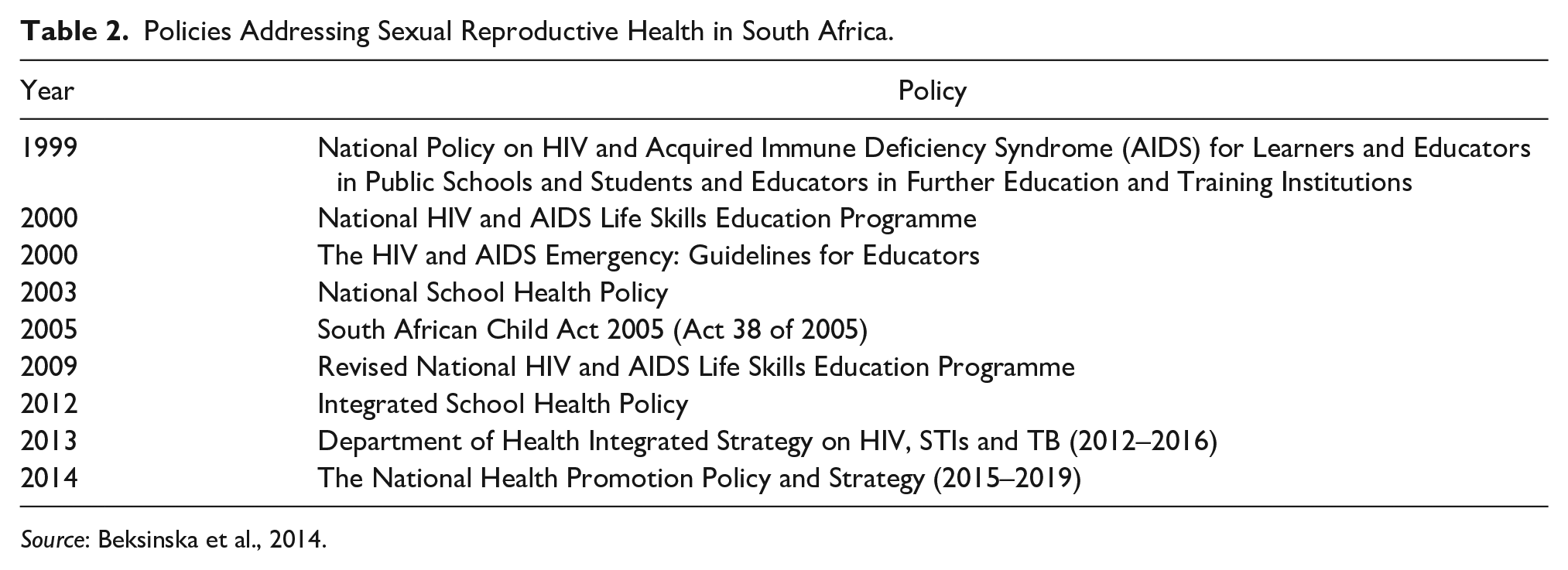
Source: Beksinska et al., 2014.
Male Medical Circumcision, and Prevention of HIV/AIDS and STIs
Participants regarded health education as facilitating the acceptance of MMC and prevention of HIV/AIDS among male adolescents in schools, and strengthening community action in accordance with the Ottawa Charter to encourage boys to undergo MMC services which are readily accessible in the health-care system.
We talk about male medical circumcision and tell them that since there are these infectious diseases like HIV and STI’s, they need to do circumcision. It is not like they don’t get such diseases but it decreases the chances of getting the STIs including HIV after they have done circumcision. [Participant #2] We encourage boys to undergo male medical circumcision. Telling them the importance of removing the foreskin, so as to prevent themselves from contracting STIs and to minimise the chances of being infected with HIV. [Participant #13] Boys are always embarrassed to talk about male circumcision among girls and female nurses. There is no other alternative, it is only female nurses who visits the schools for school health nursing. [Participant #9] We tell them that if the boys have sexual intercourse with girls without applying safe sex measures like using a condom, there are bigger chances of teenage pregnancy, STIs and HIV/AIDS. Real men love and protect their female partners in a responsible way. [Participant #4]
Lack of Support From Teachers and School-Governing Bodies
Participants perceived that the SRH program lacks support from some teachers and members of the school-governing body, which is against creating a supportive environment—one of the key areas of the Ottawa Charter. Participants viewed the attitude of authorities and lack of support toward SRH as a barrier, thereby not allowing them to provide information on SRH effectively. In some cases, the teachers would insist that the participants show them their teaching material for prior approval. Participants stated that some school-governing bodies are of the view that the provision of SRH services in schools encourages adolescents to engage in premarital sex.
In certain schools governing bodies, depending on the cultural predominance at that school, some of them prefer not to have these programmes done by us but they cover it in their own school life orientation topics with their educators. So, the school actually gives us a guide as to what we can cover and what we shouldn’t cover because it is quite a sensitive issue in their school to talk about sex. [Participant #10] Some teachers and parents are very sensitive to see pictures of common STI symptoms affecting adolescents like genital warts, sores, ulcers, vaginal discharges and condoms. Others were of the view that if adolescents were introduced to sexual and reproductive health issues they would engage in premarital sex. [Participant #17] In some schools the teachers did not want me to discuss certain topics with the learners such as use of male and female condoms in prevention against STIs and HIV/AIDS. But now what I have learnt as well with my years, before I do talks at schools, whatever method or poster I used, I should show it to the teachers or principal first then after their approval I can go ahead. [Participant #4]
Risky Sexual Behaviors Among the Learners
Participants were aware that some adolescent girls still got pregnant and engaged in risky sexual behaviors. Developing personal skills among adolescent learners has not yet been achieved as recommended by the Ottawa Charter.
A lot of boys and girls are still taking risk of having unprotected sexual intercourse. They know about the availability of condoms and morning-after pills but still they usually don’t take attention to access the primary health care services. [Participant #7] We find a lot of adolescent girls that are pregnant at school. We give them health advice or health education on the importance of attending antenatal clinic, usually adolescent boys are not interested in listening to the topics because they are not relevant to them but only to girls, they leave the venue and we are only left out with girls. [Participant #19]
Empowerment of Adolescent Boys
The suggested action is to develop an effective HPS program with specific behavioral and lifestyle objectives to target boys, which is beyond the health education strategy provided by SHNs. A lack of knowledge and understanding in applying behavioral change models among SHNs was noted as a serious challenge, as it is not part of the competencies of nursing training and academic curriculum. Reorienting health-care services is a highly essential step toward empowerment of boys regarding behavioral change and lifestyle. Behavioral change and lifestyle modification is an enabling process which demands collaborative activities with other relevant stakeholders.
I cannot say a lot because we haven’t been trained in behavioural change methods related to health promotion for school kids, we just pick up health talks along the way. We have qualified health promotion practitioners in the province but they are not part of school health services. [Participant #12] Talking about sex in front of boys and girls at the same time can be very sensitive, more skills are essential to deal with that. The evidence is always available on our records on yearly basis that these kids are vulnerable to STIs, teenage pregnancy and HIV/AIDS. [Participant #14] The school kids say that as school health nurses, we should not be parenting them, or impose our health education, cultural and religious beliefs on them or be judgmental, they say, we should just guide them on safe options to choose from in a right way. [Participant #16]
Discussion
The study identified facilitators and barriers in the provision of SRH in South Africa using the Ottawa Charter as a guide (World Health Organization, 1986). These facilitators and barriers can be utilized to guide and design HPS programs to help empower boys to become real men and responsible citizens. The ISHP of 2012 is one example of such a policy that facilitate SHNs to deliver health education and promotion of SRH to all learners in different developmental stages (Table 2). In addition to ISHP, HPS programs are guided by the National Health Promotion Policy and Strategy (Department of Health, 2015).
The participants in this study stated that the current SRH program lacks support from school teachers and members of the school-governing body. They viewed the attitude and lack of support from teachers and parents toward SRH as barriers, due to which SHNs are unable to provide information on SRH effectively. There is a gap in health-promotion practitioners that need to be filled in HPS and SRH; health-promotion practitioners are trained to assess and design relevant behavioral and lifestyle change programs utilizing facilitators and barriers (Egger et al., 2013).
In some instances, teachers insist that participants show them their teaching material for prior approval. Some school-governing bodies are of the opinion that the provision of SRH services in schools encourages adolescents to engage in premarital sex, which is against Zulu culture. Thus, this study identified a knowledge gap among SHNs, teachers, school-governing bodies about what HPS and SRH are, and how these initiatives can make a difference to empower adolescent boys’ health behaviors. Again, the findings portray the lack of knowledge, understanding, and application of health-promotion approaches, methods, and strategies in addressing risky health behaviors; hence, the SHNs are viewed by learners as being irrelevant and judgmental. The suggested action is to develop a comprehensive effective HPS program with specific SRH objectives to target boys, which is beyond the common top-down approach of health education intervention provided by SHNs. An effective health-promotion program requires extensive competencies in the application of experiential small group methods such as focus groups of boys for planning and assessment, learning groups for behavioral and skill training, and peer discussion groups for education and awareness raising (Egger et al., 2013). Health-promotion programs are well supported by the National Department of Health in the reengineering of primary health care. The National Development Plan 2030 initiative has been undertaken to address all the health needs of school children under an HPS setting (National Planning Commission, 2010; NDoH, 2011).
In South Africa, the National Health Promotion Policy and Strategy embraces all health-promotion programs including HPS, but there’s a lack of proper training for SHNs in health promotion. The academic curriculum of nurses was never reviewed to include health promotion as a module in their training (Department of Health, 2015).
Conclusion
This study analyzed the data collected from SHNs on their experiences related to SRH services among adolescent boys. The knowledge gap identified requires a collaborative intervention of key relevant stakeholders facilitated by teachers working with a qualified health-promotion practitioner, a reflective practitioner to design and facilitate an HPS program. The challenge is the lack of knowledge and implementation capacity of SHNs in behavioral and lifestyle change programs for boys. SHNs are always female and are unable to deal with male-related sexual and reproductive behaviors (Table 3). However, SRH should be viewed as a lifestyle empowerment initiative and a normal developmental process that extends from adolescence to adulthood in both males and females. A specific comprehensive HPS program targeting adolescent boys has been recommended as an effective strategy to enhance sustainable interventions. Comprehensive health-promotion programs if properly designed will be instrumental in developing boys toward adaptation of male SRH in their communities with embedded cultural manhood values.
Demographic Characteristics of Participants (n = 21).

Note. SHN = school health nurse.
Recommendations
Developing boys into being real and responsible men with particular focus on sexual and reproductive behavioral modification and lifestyle changes requires a collective effort of relevant stakeholders inclusive of the parents, communities, and schools, which creates a supportive environment.
Empowerment of the target groups—boys, parents, school-governing bodies—and tactful respect of cultural norms and values should be part of the whole comprehensive health-promotion package to enhance impact and acceptability, working together with qualified male and female health-promotion personnel.
Schools have been identified as important social institutions in which sexual and reproductive health behavior converge with particular clarity. They are also convenient settings to target boys in different age groups for programs which can be implemented and incorporated into the teaching and learning curricula.
The teachers and the school-governing bodies are in the forefront to facilitate the integration of teaching and learning, HPS programs, and male sexual reproductive health on a yearly schedule of the school program. This kind of facilitation does not happen spontaneously; it requires proper empowerment and special training of teachers and school health nurses. A properly coordinated HPS program should yield achievable outcomes, guaranteed ownership, and sustainability of male sexual and reproductive health.
Study Limitations
One limitation of this study is that the findings are based only on the experiences of SHNs who were interviewed. The female SHNs are the sole health-care workers visiting schools for school health services. This limitation can be alleviated by conducting further research that involves boys themselves and male school health personnel. Another limitation is the small sample size of 21 SHNs, which implies that this study cannot be generalized to the whole South African population.
Footnotes
Acknowledgements
This study is based on the dissertation of the main author, approved in partial fulfilment of the academic requirement for the degree of Master of Nursing Sciences (Community Health Nursing), in the School of Nursing and Public Health, College of Health Sciences, University of Kwa-Zulu Natal.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.