
Abstract
The prostatic abscess is a rare complication of a bacterial infection of the prostate. Since the early use of potent antibiotics to treat urinary tract infections, the incidence of the prostatic abscess has declined significantly. In keeping with that, prostatic abscess combined with abscesses in the spleen or other distant organs become an extremely rare but fatal clinical condition. Here, we present a case of prostate and spleen abscess due to multi-drug-resistant gram-negative bacilli without obvious risk factors. The patient initially complained of high-grade fever and dysuria. After screening the source of infection by computed tomography (CT) scans, prostate and spleen abscesses were diagnosed. In addition, extended-spectrum beta-lactamase positive Escherichia coli was detected both in urine and blood culture. The patient was successfully treated by a transurethral resection of the prostate followed by splenic puncture and drainage, as well as intravenous administration of meropenem. Although the prostate abscess combined with spleen abscess was rare, the possibility of dissemination in remote tissues should be taken into consideration before the surgical treatment of prostatic abscesses. The concurrent drainage of multiple abscesses followed by intensive and sensitive antibiotics was safe and effective for indicated patients.
Background
Prostatic abscess combined with an abscess in distant organs is a rare clinical condition with the widespread application of antibiotics (Liao et al., 2016; Deshpande et al., 2013). Overall, the annual incidence of prostatic abscess can be 0.5% of all urological disorders, and the mortality rate is between 1% and 16% (Ha et al., 2008). The severe infection of the prostate is frequently caused by the reflux of infected urinary contents into prostatic ducts, especially in patients with diabetes, immunosuppressive state, chronic prostatitis, epididymitis, gonorrhea, or undertaking prostate biopsy, and so on (Caulier et al., 2009; Dell’atti, 2013; Nomura et al., 2021; Tay et al., 2021). Gram-negative Enterobacteriaceae causing urinary tract infections is the dominant pathogenic bacteria, while Gram-positive bacteria had also been reported as the cause of prostate abscesses in uncontrolled diabetes patients (McCormick et al., 2021; Merchant et al., 2016). Hematogenous dissemination from the primary infected focus includes appendicitis, peritonitis, liver or perirenal abscess, diverticulitis, or from severe subcutaneous infections of Staphylococcus aureus, could also lead to an abscess in prostatic tissue (Liao et al., 2016). Due to the limited incidence, official diagnostic and treatment guidelines have not been organized and recommended. As a result, the prostate abscess could be a clinical challenge or a fatal disease in the real world, especially in developing countries (Abdelmoteleb et al., 2017).
In this study, we report a case of prostatic abscess and splenic abscess in a patient without apparent risk factors that were successfully treated by transurethral resection of the prostate and spleen abscess drainage. Notably, the abscess of the spleen is also a life-threatening disease that is typically caused by systemic septic emboli. Metastatic infections are one of the most common causative factors for splenic abscesses (Mustafin & Orlova, 1988). More importantly, splenic abscess frequently became a complication of cancer treatment, especially in immunocompromised patients (Ismail et al., 2015). However, the hematogenous dissemination of prostatic abscess to the spleen is extremely rare, which is also challenging in diagnosis. Based on our case, we recommended that physicians be vigilant for hematogenous dissemination of prostatic infection to prevent significant morbidity and mortality.
Case Presentation
The patient was a 50-year-old male patient who complained about fever and dysuria. One month before admission, he had been experiencing lower urinary tract symptoms, including dysuria and frequency. Ten days previously, he had an outpatient visit to the community hospital because of a high-grade fever (39.4°C) and chills and worsening dysuria. After 10 days of treatment with quinolones antibiotics, the patient’s fluctuated body temperature remain, ranging from 36.6°C to 38.9°C. At the time of attending our hospital, the patient complained of loss of appetite and constipation, as well as an inability to pass gas for over 24 hr. He denied any trauma to the genital area, and he was not sexually active. The patient’s medical history has been screened for risk factors for infections.
Moreover, he did not have any urinary problems before this episode. Accordingly, he had an outpatient visit to our department for further diagnosis and treatment and was admitted for a fever workup. On admission, his blood pressure was 136/92 mmHg, body temperature was 39.1°C, heart rate was 108/min, and oxygen saturation was 95%. The abdomen was soft without guarding, rigidity, or rebound tenderness on examination. The costovertebral angle tenderness of both sides was negative.
Investigations
Admission laboratory data included the following: white blood cells (WBCs), 15.37 × 109/L; lymphocyte, 0.77 × 109/L; platelets, 132 × 109/L; high sensitive C-reactive protein, >9.65 mg/L; procalcitonin, 0.73 ng/mL; aspartate aminotransferase (AST), 91 U/L; alanine aminotransferase (ALT), 53.5 U/L; and creatinine, 56.00 μmol/L. Bacterial cultures of urine and blood were performed to identify the pathogenic bacteria. As a result, extended-spectrum beta-lactamase positive (ESBL+) Escherichia coli was detected in urine and blood culture. Drug sensitivity tests indicated that amikacin, imipenem, meropenem, and tigecycline were potential candidates for infection treatment. Here, meropenem was selected for antibiotic therapy. Total body computed tomography (CT) was performed to identify the focus of infection further. Pneumonia or bronchitis could be ruled out by plain chest CT. An abdominal CT scan found a single low-density focus with 6.5-cm diameter on the spleen (Figure 1A). In addition, pelvic CT revealed multiple low-density foci, measuring 20 mm in diameter within the prostate (Figure 1B).

The Computed Tomography (CT) Scan of Prostatic Abscess and Spleen Abscess. CT Scan of Spleen Abscess (A) and Prostate Abscess (B) Before the Transurethral Surgery and Splenic Puncture.
Treatment
Transurethral resection of the prostate was performed to drain the abscess and relieve the obstruction. During the resection, prostatic pus was spilled out into the washing fluid, by which the prostatic abscess was confirmed during the surgery (Figure 2A). Prostatic abscess was further confirmed by pathologists according to the specimens from the resection of his prostate. Splenic puncture and drainage were applied, and a spleen abscess was further confirmed (Figure 2B). ESBL+ E. coli was confirmed in the splenic drain culture. After the abscess drainage, meropenem was used to strengthen infection control, and the body temperature returned to normal ranges.
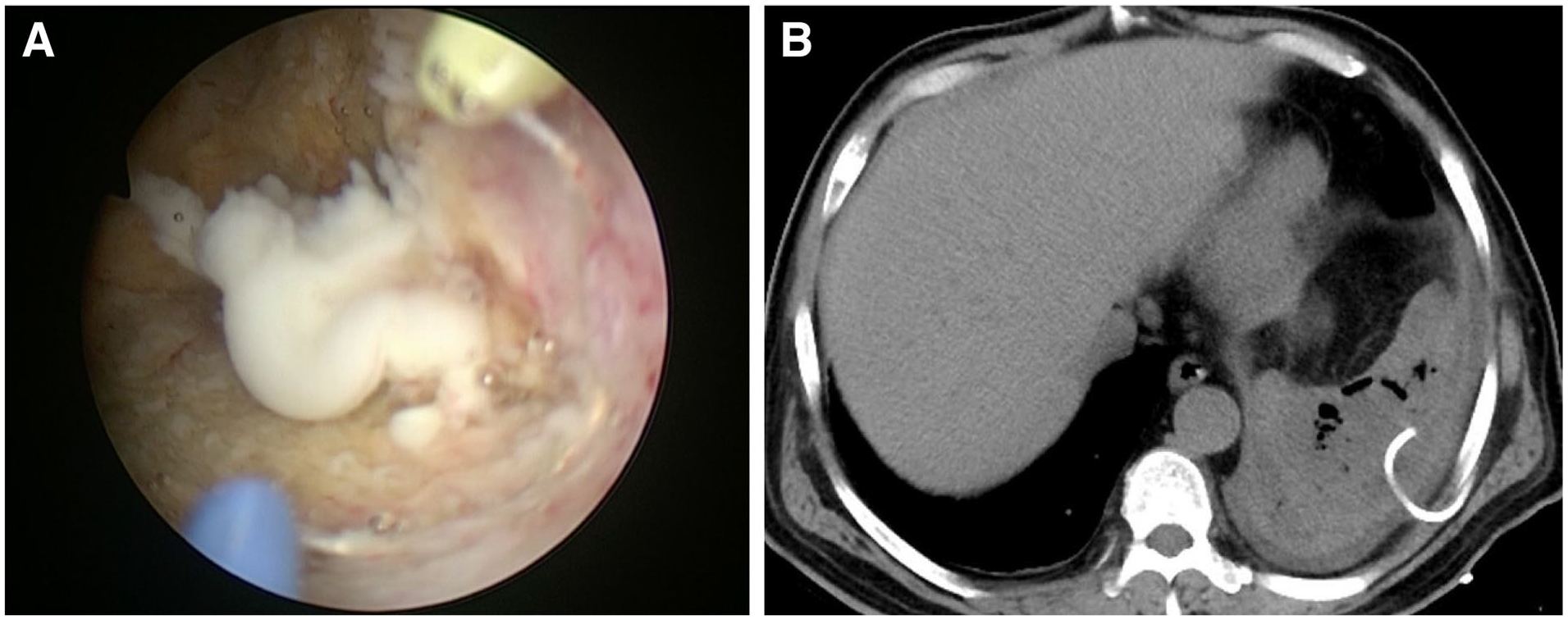
The Photography of Prostate Abscess During the Transurethral Surgery and Computed Tomography Image of Spleen Drainage. (A) The Representative Photography of Prostate Abscess During the Transurethral Surgery. (B) The Computed Tomography Scan of the Spleen After Splenic Puncture and Drainage.
Outcome and Follow-Up
The intravenous administration of meropenem was switched to oral antibiotics on Day 10 after spleen abscess drainage, and the patient was discharged from the hospital on Day 14. Antibiotic treatment for the abscess was then continued for another 4 weeks with complete resolution of symptoms. After treatment, there were no symptoms of recurrence for 12 months.
Discussion
The prostatic abscess is a complication of acute urinary tract infection but is extremely rare due to the usage of antibiotics. However, in patients with uncontrolled diabetes or immunosuppression, the presentation of prostate abscess should be considered. In addition, the prostate abscess shares the risk factors of sepsis, as an abscess in the liver could disseminate to prostate tissues (Lim et al., 2002). In this case, the patient had no obvious risk factors, such as diabetes or immunosuppressive states. After screening, the infection causes for high-grade fever, prostate abscess, and spleen were confirmed and treated by transurethral resection of the prostate and splenic puncture. The meropenem was administrated intensively and appropriately according to the antimicrobial susceptibility test for 14 days. Overall, the disseminated prostatic abscess was cured and did not recur during the follow-up.
As the patient developed symptoms of prostatitis before fever in the presented case, the spleen abscess is probably disseminated from the prostate through blood circulation. Various strategies for the drainage of prostatic abscesses are available, including ultrasound-guided drainage, transurethral drainage, or open surgical drainage (Abdelmoteleb et al., 2017). Moreover, a holmium laser for transurethral deroofing of a prostatic abscess could also ensure successful drainage of the entire abscess cavity (Lee et al., 2015). For specific cases, trans-rectal ultrasound (TRUS)–guided aspiration or transperineal ultrasound-guided aspiration could be served as both diagnostic and treatment methods (Soga et al., 2021; Somuncu et al., 2003). As a minimally invasive method, the TRUS-guided aspiration was reported to achieve a success rate of 75% for pelvic abscesses (Giovannini et al., 2003). However, a relatively high recurrence rate was expected for the multiloculated prostate abscess. In this case, transurethral resection of prostatic was applied instead of percutaneous drainage to achieve complete drainage of the abscess cavity and minimize the recurrence rate. Compared with limited drainage techniques, transurethral surgery alleviates the need for secondary procedures, having an obvious advantage (Goyal et al., 2013).
In this study, ESBL+ E. coli was the pathologic bacteria in this case, and meropenem was one of the sensitive antibiotics for the pathogen. The patient underwent insufficient antibiotic intensity and treatment course before attending our medical center. As a result, the development of multi-drug-resistant features of the gram-negative bacilli might contribute to disseminating prostatic abscess to the spleen (Chrystle et al., 2021; Mucke et al., 2017). However, blood and urine cultures suggested that amikacin was also a sensitive alternative, in this case, practical usage of carbapenems antibiotics was reported to shorten the postinfection length of stay and benefited the patient eventually (Zilberberg et al., 2019).
There are several limitations of this study. First of all, the research design is a case report, the evidence level of which is limited. Second, long-term follow-up is needed, as the follow-up period of this research is 12 months. Further studies of the prostate abscess are required to draw a conclusive consensus or guidelines toward the standardized treatment for this disease.
In conclusion, we present a disseminated abscess from the prostate to spleen treated by transurethral resection of prostatic and splenic puncture and drainage, followed by intensive and sensitive antibiotics. This case highlights the importance of timely and complete diagnosis of the disseminated focus besides the primary infectious site and the safety and effectiveness of concurrent invasive strategies of abscess drainage to prevent significant morbidity and mortality.
Footnotes
Acknowledgements
The authors thank Dr. Yang Sun for her assistance and proofreading the manuscript.
Author Contributions
Fei Wu: Involved in writing the manuscript text. Shun Li and Zeqiang Sun: Involved in collecting clinical information and literature. Ning Di: Involved in proofreading the manuscript. Fei Wu and Qingyong Liu: Supervising consultant in the study and reviewed the manuscript text.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Nature Science Foundation of China (NSFC82002719), Nature Science Foundation of Shandong Province (ZR2020QH240), the Clinical Medicine Innovation Program of Jinan City (202019125) the second-class General Financial Grant from the China Postdoctoral Science Foundation (2022M711977), and the Shandong Provincial Key Research and Development Project (2019GSF107058 and 2019GSF108232).
Ethics Approval
This study was approved by the Ethics Committee of The First Affiliated Hospital of Shandong First Medical University & Shandong Provincial Qianfoshan Hospital (No.2020S141).
Informed Consent
Written informed consent for the publication of this case report was obtained from the patient.
Guarantor
Fei Wu