
Abstract
Infective endocarditis (IE) commonly complicates bicuspid aortic valve. We report an uncommon case of bicuspid aortic valve (BAV) IE with aortic root abscess (ARA), presenting initially with abdominal pain due to splenic infarcts, delaying prompt diagnosis. A 38-year-old gentleman presented with fever and abdominal pain. He was treated for intra-abdominal sepsis, was started on intravenous antibiotics and had a computed tomography scan of the abdomen that revealed a large splenic infarct. The patient deteriorated, prompting further investigations, including echocardiography due to findings of a new murmur, signs of embolisation and blood cultures revealing Staphylococcus aureus. This revealed an otherwise unknown BAV with aortic valve vegetation and ARA. IE and ARA commonly affect patients with bicuspid aortic valve, and our case highlights the importance of systemic review, as IE often manifest clinically in various forms.
Introduction
Bicuspid aortic valve (BAV) remains the most common congenital heart defect, affecting 1–2% of the general population. 1 Infective endocarditis (IE) can complicate the condition. 1 We report an uncommon case of BAV IE with aortic root abscess (ARA), presenting initially with abdominal pain due to splenic infarcts, delaying prompt diagnosis.
Case report
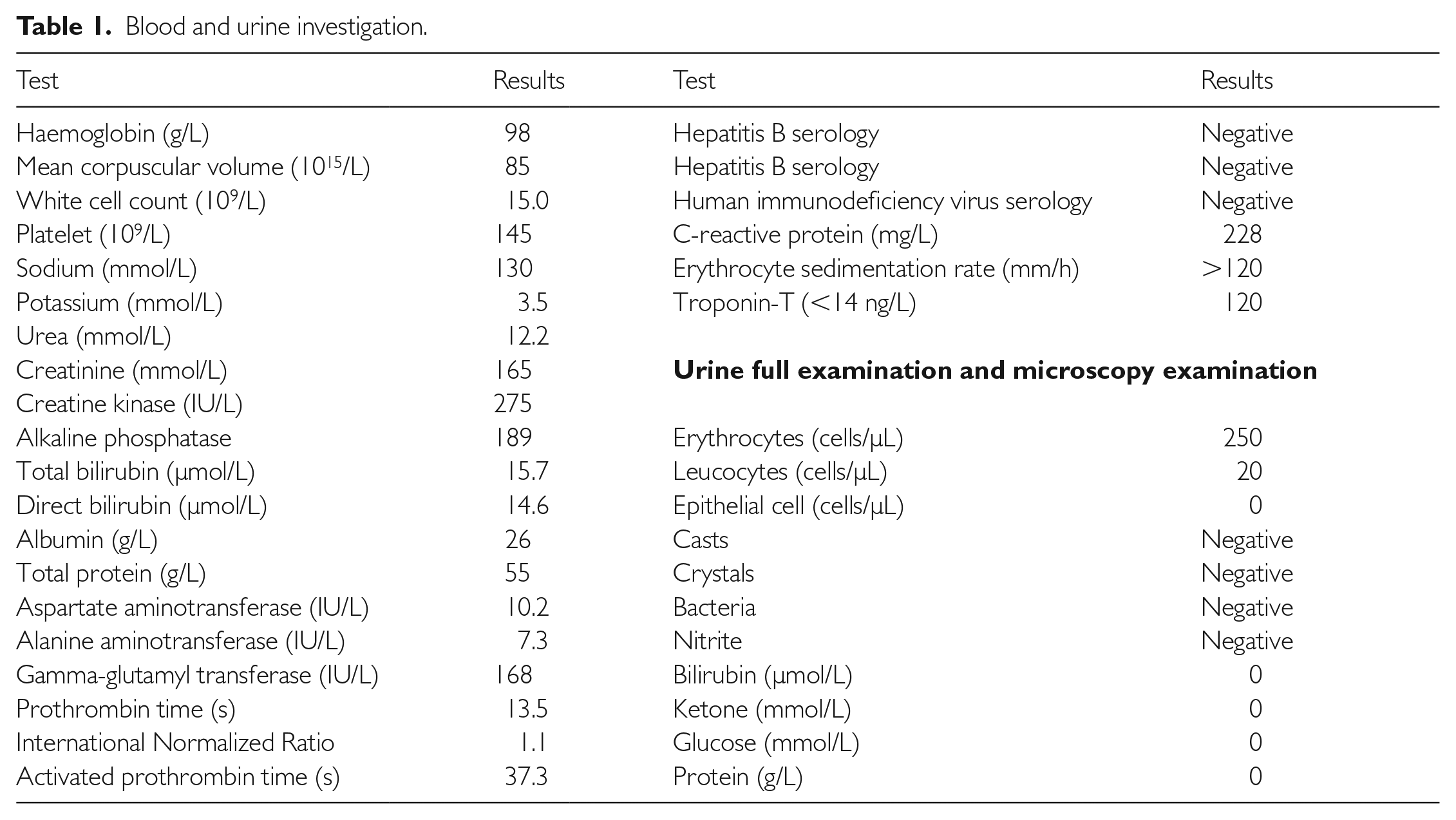
A 38-year-old gentleman, with no prior medical illnesses, presented following a week’s history of left hypochondrial pain and fever. The patient denied any recent hospitalisation, procedures or intravenous drug use, but had been complaining of lethargy and progressively worsened dyspnoea in the past six months. Vital signs included blood pressure of 118/62 mmHg, a heart rate of 110 bpm, temperature of 37.9°C, oxygen saturation of 98% on room air and respiratory rate of 20 breaths per minute. He was admitted to a neighbouring hospital for an acute abdomen and intra-abdominal sepsis under the general surgical team, with possible causes including pancreatitis, pyelonephritis or of biliary origin. Bloods revealed raised inflammatory markers (white cell count of 15×109/L, C-reactive protein of 228 mmol/L and erythrocyte sedimentation rate of 120/min), and the patient was started on intravenous ceftriaxone whilst awaiting further results from blood cultures which had yet to reveal any preliminary results at that point (Table 1). Despite antibiotics, his symptoms persisted, prompting a computed tomography scan of the abdomen which was performed on day 4 of admission. This revealed a large, wedge-shaped hypodensity on the spleen measuring 4.2 cm×3.2 cm×4.8 cm, suggestive of a splenic infarction (Figure 1).
Blood and urine investigation.

Evidence of embolic phenomenon, including (a) splenic infarction on computed tomography imaging of the abdomen and (b) digital and distal limb ischaemia and infarction clinically.
The patient further deteriorated and was transferred to our centre for further care by day 5 of hospital admission. Vital signs include blood pressure of 95/42 mmHg requiring intravenous vasopressor, a heart rate 130 bpm, temperature of 39°C, oxygen saturation of 88% on room air requiring oxygen supplementation and a respiratory rate of 24 breaths per minute. Clinical examination revealed a soft but tender abdomen predominantly in the left hypochondria, with no evidence of guarding. Interestingly, there was evidence of dusky skin lesions in his extremities (Figure 1) and a grade 4 early diastolic murmur which had not otherwise been recognised since admission. Electrocardiogram revealed sinus tachycardia, and chest radiography showed evidence of acute pulmonary oedema. By then, results from the initial blood cultures performed on initial admission six days earlier revealed Staphylococcus aureus. Unfortunately, we were unable to delineate a likely source for this microorganism on both history and physical examination.
Following this, a transthoracic echocardiogram and transoesophageal echocardiogram (TOE) were both performed, demonstrating a type 1 BAV with right and non-coronary cusps fusion, severe aortic regurgitation, ascending aorta dilatation, as well as a 1.1 cm×0.5 cm vegetation in the left coronary cusps and a 1.4 cm×0.6 cm ARA on the aortic-mitral curtain, with no other valvular involvement (Figure 2). The left ventricle was not dilated, and left ventricular ejection fraction was preserved, measuring 55%. There was mal-coaptation of both aortic cusps which led to severe regurgitation, with no evidence of leaflet perforation seen on TOE, although three-dimensional TOE was not performed to support this further, as it was not available at the time. Alongside a change in intravenous antibiotics to cloxacillin, urgent cardiothoracic consult was sought, but unfortunately the patient succumbed intraoperatively during emergency surgical aortic valve replacement performed on day 7 of admission.

Transthoracic echocardiography on (a) and (b) parasternal short-axis view demonstrating a type 1 bicuspid aortic valve with right and non-coronary cusps fusion and on (c) apical five-chamber view demonstrating severe aortic regurgitation evident from a pressure half-time of 161 ms. Transoesophageal echocardiography demonstrating (d) dilatation of the ascending aorta, and (e) a 1.1 cm×0.5 cm vegetation in the left coronary cusps and (f) a 1.4 cm×0.6 cm aortic root abscess on the aortic-mitral curtain.
Discussion
IE commonly affects patients with BAV (7–25% according to autopsy studies), and often occurs in male patients. 1 Furthermore, IE has been shown recently to occur more commonly in predominantly regurgitation BAV versus those with predominantly stenotic lesions. 2 However, determining if a BAV would cause a predominant regurgitation versus stenotic lesion remains difficult. 3 Although the exact pathophysiology remains uncertain, proposed mechanisms include altered blood flow patterns across the valve that leads to endothelial injury, and platelet and fibrinogen deposition, which allows seeding of haematogenous microorganisms. 4 It remains debatable whether S. aureus IE commonly occurs in BAV patients.5,6 However, it has been shown to be an independent mortality risk factor when present. 7
Several studies have reported higher rates of concurrent ARA in BAV patients with aortic valve IE, irrespective of the causative organism.7,8 Peri-annular complications via soft-tissue dissemination, including abscesses, pseudoaneurysms and fistulas, occur in 30–50% of aortic valve IE, with possibly higher rates in BAV cases. 9 Despite this, the use of prophylactic antibiotics prior to predisposing procedures or instrumentation remains debatable.
Another unique aspect to our case was the atypical initial clinical presentation. Although splenic infarction is well described, IE patients often present predominantly with fever, cardiac and neurological signs and symptoms, and rarely with isolated abdominal symptoms. 10 In fact, only 0.1% of patient with IE present initially with abdominal symptoms, and often fall under the care of our surgical colleagues initially. 11 Furthermore, only a third of IE patients have a cardiac murmur on initial presentation.1,7 This highlights the importance of a full systemic review when managing IE patients, as they can manifest clinically in various forms.
Footnotes
Acknowledgements
The authors would like to acknowledge Universiti Teknologi MARA Sungai Buloh for supporting the submission of this case report.
Authors’ contributions
R.E.F.R.S. was responsible for data collection and analysis and for drafting the manuscript. H.A.Z.A. and S.S. were responsible for drafting and revising the manuscript.
Availability of data and materials
The data that support the findings of this study are available from UiTM Sungai Buloh, but restrictions apply to the availability of these data, which were used under license for the current study and so are not publicly available. Data are, however, available from the authors upon reasonable request and with permission of UiTM Sungai Buloh.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Ethical approval to report this case was obtained from the Universiti Teknologi MARA (UiTM) Sungai Buloh Ethics Committee.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for his anonymised information to be published in this article.