
Abstract
The objective of this study was to compare the efficacy and safety of 10 different surgical treatments for benign prostatic hyperplasia (BPH) with volume >60 mL. A systematic literature review and network meta-analysis of randomized controlled trials (RCTs) within a Bayesian framework was performed. A total of 52 parallel-group RCTs included, reporting on 6,947 participants, comparing open prostatectomy (OP), monopolar/bipolar transurethral resection of prostate (monopolar/ bipolar TURP), thulium, holmium and diode laser enucleation of prostate (LEP), bipolar enucleation of prostate, potassium titanyl phosphate laser vaporization of prostate (KTP LVP), bipolar vaporization of prostate (bipolar VP), and laparoscopic simple prostatectomy (laparoscope SP). Compared with OP, laparoscope SP identified better maximal flow rate (Qmax; mean differences [MDs] = 2.89 mL/s) at the 24th month, but bipolar VP demonstrated worse Qmax (MD = −3.20 mL/s) and International Prostate Symptom Score (IPSS; MD = 2.60) at the 12th month. Holmium LEP (MD = 1.37) demonstrated better International Index of Erectile Function–5 at the 12th month compared with OP. However, compared with OP, KTP LVP demonstrated worse postvoid residual volume (PVR) at the sixth (MD = 10.42 mL) and 12th month (MD = 5.89 mL) and monopolar TURP (MD = 6.9 mL) demonstrated worse PVR at the 12th month. Eight new surgical methods for BPH with volume >60 mL appeared to be superior in safety compared with OP and monopolar TURP due to fewer complications. Bipolar VP and KTP LVP maybe not suitable for prostates more than 60 mL due to short- and middle-term worse Qmax, IPSS, and PVR than OP.
Introduction
Benign prostatic hyperplasia (BPH) is one of the most common causes of elderly male urinary system disease (Vuichoud & Loughlin, 2015). It contributes greatly to lower urinary tract symptoms (LUTS), which disturbs the quality of life, interferes with daily activities, and causes a significant burden of economic (Lee et al., 2017; Zhu et al., 2021). According to the estimates of Global Burden of Disease 2019, the number of BPH cases and the standardized incidence rate in 2019 were 11.26 million and 280.4/100,000 around the world, respectively (Launer et al., 2021).
Compared with drug treatment, surgical therapy is the most conventional and effective treatment for patients with obvious LUTS or complications (Gratzke et al., 2015). Monopolar transurethral resection of the prostate (monopolar TURP) has been recognized as the first-line surgical method for LUTS secondary to BPH in normal volume prostate since the 1970s (Madersbacher et al., 2004). The risk of life-threatening complications related to monopolar TURP, especially transurethral resection syndrome, and the huge difficulty in regulating larger prostates shifted the studies toward other alternatives (Reich et al., 2008). Considering the preoperative symptoms and surgical difficulty, the guidelines of American Urological Association (AUA) and European Association of Urology recommend open prostatectomy (OP) as the surgical treatment option for larger prostates (Foster et al., 2018; Gratzke et al., 2015). Compared with minimally invasive surgery, OP may have more postoperative complications and longer postoperative recovery time (Gratzke et al., 2007). We need new minimally invasive surgical techniques to achieve the similar functional outcomes compared with monopolar TURP and OP, but with fewer side effects (Lourenco et al., 2008).
Since the early 2000s, several systems and approaches for surgical treatments of BPH have gradually been developed, including various laser systems, such as the thulium laser, holmium laser, potassium titanyl phosphate laser, and diode laser. Other energy systems included bipolar energy and approaches that use laparoscope et al (Issa, 2008). Different surgical methods for larger prostates have their advantages and disadvantages and these new surgery interventions are desired to replace OP and monopolar TURP.
As AUA Guideline mentioned, “large” is a relative term as some providers have excellent results utilizing transurethral approaches (e.g., bipolar TURP, holmium laser enucleation of prostate [holmium LEP]) in prostates >60 mL (Foster et al., 2018). However, not all providers have access to or are using bipolar TURP or holmium LEP technology and may not wish to approach large glands transurethrally. Meanwhile, although there have been several randomized controlled trials (RCTs) and pairwise meta-analysis in recent years (Jones et al., 2016; Li et al., 2019), there is no consensus among surgeons on the best approach of operation in BPH with volume >60 mL. The objective of this systematic review and network meta-analysis was to explore the prior surgery treatments with better functional outcomes, perioperative parameters, and fewer complications.
Method
Search Strategy
We adhered to the preferred reporting items for systematic reviews and meta-analyses statement to report network meta-analyses of health care interventions (Moher et al., 2009). A systematic electronic databases search was initially conducted using PubMed, Embase, Web of Science, and Cochrane Central Register of Controlled Trials in the Cochrane Library with a combination of MeSH and free text from the inception to March 30, 2021. In addition, individual urological journals and relevant citations were manually searched to retrieve any further studies. Detailed search strategy is illustrated in the Supplementary Table 1.
Selection Criteria
Types of Studies
We only included parallel-group RCTs regardless of their language of publication. In addition, the RCTs must be peer-reviewed publications and methodology was documented in replicable detail.
Types of Participants
We defined the eligible patient population as men with larger prostates (as evaluated by digital rectal examination, ultrasound, and/or cross-sectional imaging) with LUTS (McNicholas, 2016). The larger prostates group was defined as having a mean prostate volume of more than 60 mL and we also undertook analyses with cutoff values of 80 and 100 mL. We excluded studies of men with neurogenic bladder; previous prostate, urethral, or bladder surgeries; and suspected prostate cancer.
Types of Interventions
All operative treatment methods are listed in Supplementary Table 2. We included 10 operative treatment methods in this study, such as OP, monopolar TURP, bipolar TURP, holmium LEP, thulium laser enucleation of prostate (thulium LEP), diode laser enucleation of prostate (diode LEP), bipolar enucleation of prostate (bipolar EP), potassium titanyl phosphate laser vaporization of prostate (KTP LVP), bipolar vaporization of prostate (bipolar VP), and laparoscopic simple prostatectomy (laparoscope SP).
Types of Outcome Measures
The primary objective of this network meta-analysis was to evaluate the functional outcomes of patients concerning the following clinical parameters: postoperative maximum urinary flow rate (Qmax), International Prostate Symptom Score (IPSS), International Index of Erectile Function–5 (IIEF-5), and postvoid residual volume (PVR) at 3, 6, 12, 24, and 36 months after surgical treatment.
The secondary objective was to evaluate the safety of different treatments regarding perioperative parameters: catheterization duration (days), hemoglobin decrease (difference of hemoglobin between preoperative hemoglobin and postoperative hemoglobin), operative time (minutes), hospital stay (days), and bladder irrigation time (days).
The third objective was to evaluate the safety of different surgery methods regarding postoperative complications. Complications for the analysis included short-term complications (blood transfusion, incontinence [include stress and urge incontinence <1 month after surgery treatment, chose the earliest incontinence rate if multiple time points were recorded], urinary tract infection [need antibiotics treatment], capsule perforation and bladder neck contracture) and long-term complications (urinary stricture [include urethrae stricture and meatal stenosis] and retrograde ejaculation). Long-term complications were included only when the trials were followed for more than 3 months. The Qmax, IPSS, IIEF-5, and PVR at 6 and 12 months after surgical treatment were chosen as primary outcomes and other clinical measurements as secondary outcomes.
Data Collection and Risk of Bias Assessment
Two investigators independently screened the titles and abstracts. The full articles were then assessed. Two reviewers extracted data independently and then cross-checked the data using predefined data fields.
We used the Cochrane Risk of Bias Tool 2.0 (RoB 2.0) to assess the methodological quality of RCTs (Ma et al., 2020; Sterne et al., 2019). Any unresolved discrepancies in data extraction and quality assessment were evaluated by a third author.
Data Synthesis and Analysis
First, we performed a pairwise random-effect meta-analysis. The mean differences (MDs) and odds ratios (ORs) were reported for continuous and binary variables, respectively. If the authors only reported medians and interquartile ranges, we used medians as means and interquartile ranges/1.35 as the standard deviations (Follmann et al., 1992). Heterogeneity was assessed using I2 statistics (Chaimani et al., 2019). I2 ≤ 50% indicated small interstudy heterogeneity and I2 > 50% indicated high interstudy heterogeneity.
Next, we conducted a network meta-analysis in the Bayesian framework. For dichotomous variables such as complications, we noted rare and zero events. Trials with zero events in all arms of each outcome were deleted during the analysis because they offered no valuable information. Any treatments not connected to the other treatments through the network plot were excluded from the analysis of that outcome. The primary reference treatment was selected to be the OP. If OP was not existed in a special outcome, the reference treatment was selected to be the monopolar TURP.
A multiple treatments comparison was conducted by a Monte Carlo Markov Chain (MCMC) model. We conducted four MCMC chains simultaneously; the number of simulations was set up to 5,000; the number of iterations was set up to 20,000. The deviance information criterion (DIC) was used for assessing between-study heterogeneity. Two different models were run for each outcome: random-effects consistency model and random-effects inconsistency model. The choice of model was based on the model fit. The DIC provided a measure of model fit that penalized model complexity; a lower DIC indicated a better model fit. The simpler model, which is the random-effects consistency model, was used if the DIC values were similar between the random-effects consistency and random-effects inconsistency models. The random-effects inconsistency model was used if it resulted in a better model fit as indicated by a DIC lower than that of a random-effects consistency model by at least 5. All models used potential scale reduced factor (PSRF) to judge the convergence of the results. When the PSRF value was between 1.00 and 1.05, it indicated that the convergence of the iteration effect was good. Otherwise, iterative calculations with larger parameters were used until the PSRF value was between 1.00 and 1.05. Next, the consistency analysis of direct and indirect comparisons was conducted by the method of node-splitting test if closed cycle was existed (Lu & Ades, 2006). If p value ≥ .05, it suggested that the consistency of the model was satisfying.
We estimated the probabilities of each treatment being at each rank for each intervention and outcome. Besides, we used the surface under the cumulative ranking curve (SUCRA) to rank the different treatments and define the best interventional strategy and the larger value of SUCRA implied a higher hierarchy (Salanti et al., 2011).
We assessed the transitivity assumption by comparing characteristics of participants and the distribution of potential effect modifiers, including age, prostate volume, and severity of LUTS, including preoperative Qmax, IPSS, IIEF-5 and PVR.
We supposed that prostate size could affect the outcomes of the different surgical methods. We performed subgroup analyses based on the mean prostate volume data provided in each trial report (>80/≤80 and >100/≤100 mL). We also compared the mean differences in Qmax, IPSS, IIEF-5, and PVR between these types of surgical methods at postop 6 and 12 months.
The pairwise and network meta-analysis were implemented using the package “gemtc” V.0.8.2 of R-4.0.3 software. The network plots were drawn using STATA software (version 14.0; StataCorp, College Station, TX, USA). The comparison-adjusted funnel plots were used to assess the publication bias using STATA 14.0 software. And the subgroup analyses were implemented using the Open BUGS software (V.3.2.3).
Results
Eligible Studies
We identified 1,245 and 40 articles from database searching and records identified through references lists, respectively. After eliminating 305 duplicate articles, the total number of articles was 980. Of those, 893 articles were excluded on the basis of the abstract and title reviews. Of the remaining 87 articles with the full texts reviewed, 54 articles in 52 trials met our inclusion criteria for the systematic review and meta-analysis. The 52 eligible RCTs enrolled a total of 6,947 participants and evaluated 10 different surgical treatments for BPH with volume > 60 mL. Figure 1 presents the flow diagram detailing the search strategy and identification of studies used in evidence synthesis.
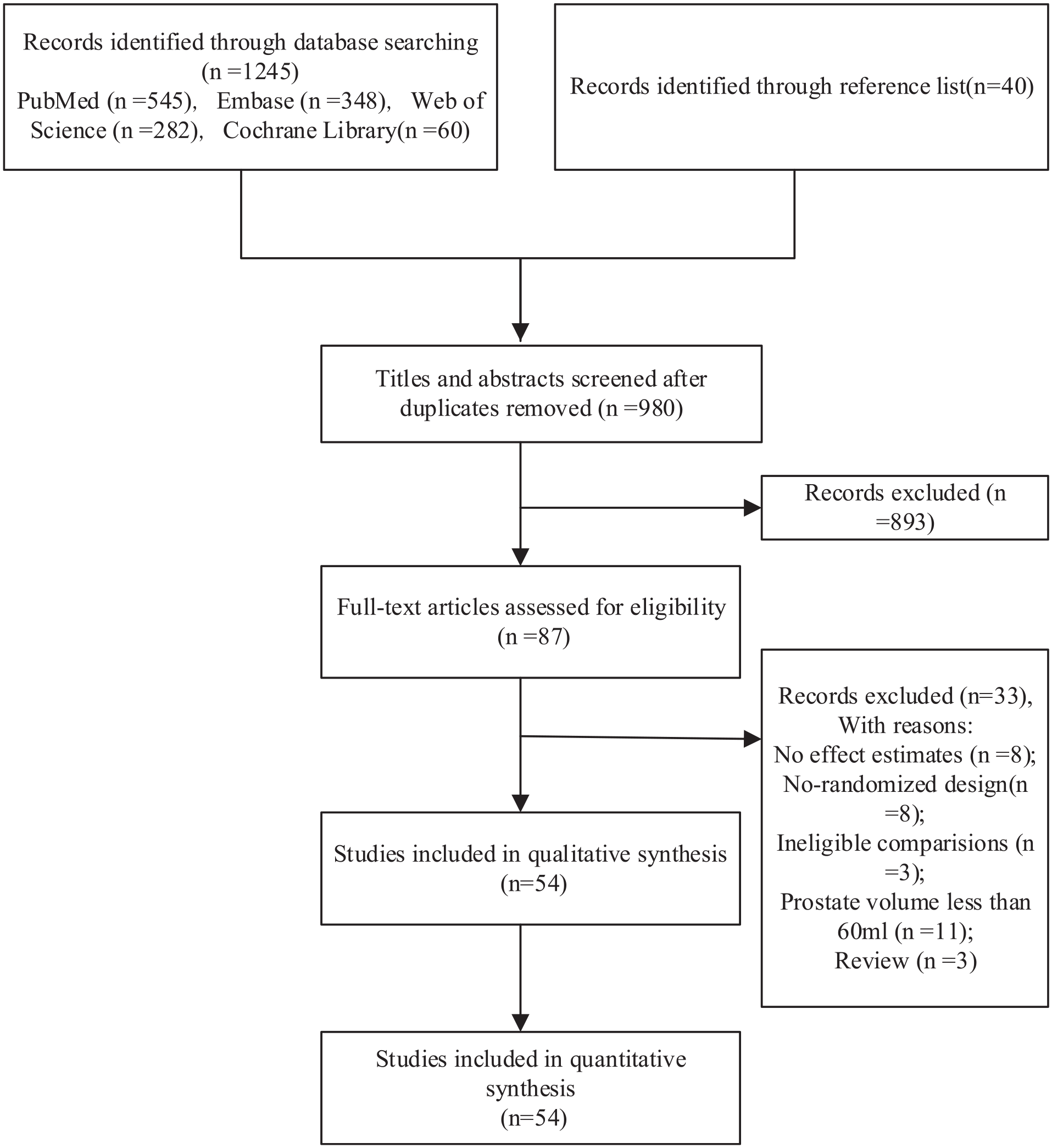
Flow Diagram for Identification of Relevant Articles for the Meta-Analysis.
Overall Analysis
Among those 52 trials, two had three arms and 50 had two arms. The clinical and methodological characteristics and the studied outcomes of each trial are summarized in Supplementary Tables 3 and 4, respectively. Baseline characteristics, including intervention treatments, follow-up, number of participants, age, preoperative Qmax, IPSS, IIEF-5, PVR, were similar among all trials, but prostate volume was not.
The RoB 2.0 assessment is presented in Supplementary Figure 1. Of the 52 included RCTs, high risk of bias was rare in any domain. Unclear assessments were common because most articles did not describe the randomization methods, such as the methods of generation of randomization sequence or sufficient details to make a judgment on the adequacy of allocation concealment. In addition, most studies did not involve blinding of patients or study personnel and did not report details on blinding of outcome assessors. Regarding overall bias, only eight articles were judged as having low risk of bias.
Network of eligible comparisons for primary and secondary outcomes are presented in Figure 2 and Supplementary Figure 2, respectively. We summarized our random-effects pairwise comparison and network meta-analysis of outcomes in Supplementary Tables 5 and 8, respectively. The rank plots of the 10 methods of BPH for primary and secondary outcomes are presented in Figure 3 and Supplementary Figure 3, respectively. The ranking probability based on SUCRA of the 10 methods of BPH for outcomes are presented in Figure 4. And the assessments of the global consistency and degree of model convergence are presented in Supplementary Table 6. The DIC of the consistency and inconsistency models were almost similar (the difference of DIC was less than 5), which means that the results of the consistency model could be considered stable and reliable. Therefore, in this study, the consistency model was used for all analysis. And the PSRF values were all between 1.00 and 1.05, which indicated that the convergence of the iteration effect was good. The node-splitting method separated evidence on a particular comparison into direct and indirect evidence and then assessed their differences. The results are presented in Supplementary Table 7. No substantial inconsistency between direct and indirect comparisons was observed due to most p values were ≥.05. Heterogeneity was high in various pairwise comparisons of functional outcomes and perioperative parameters. By contrast, we saw low heterogeneity in complications (Supplementary Table 5).
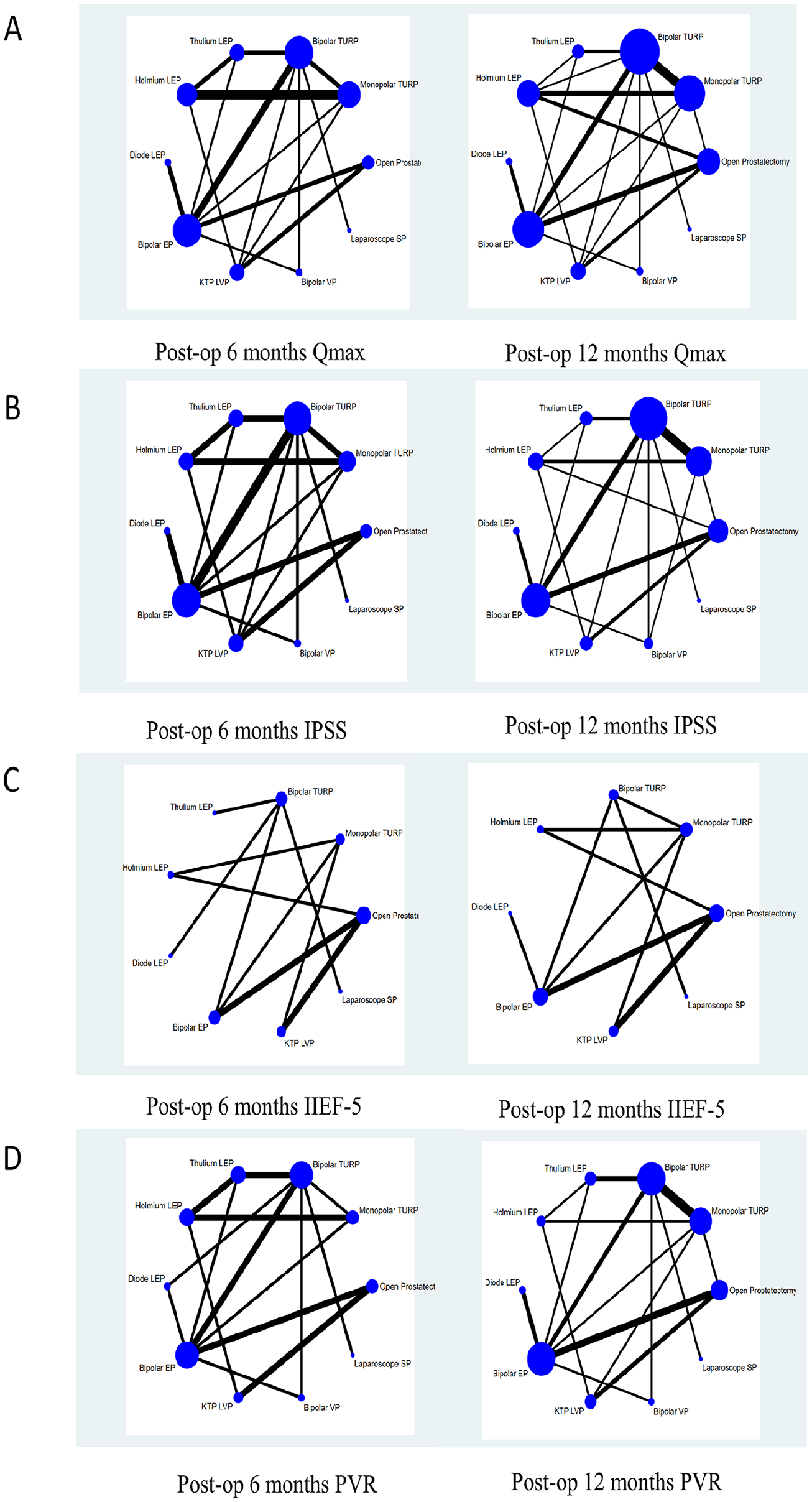
Network of Treatment Comparisons of Functional Outcomes at 6 and 12 Months: (A) Qmax at 6 and 12 Months, (B) IPSS at 6 and 12 Months, (C) IIEF-5 at 6 and 12 Months, and (D) PVR at 6 and 12 Months.
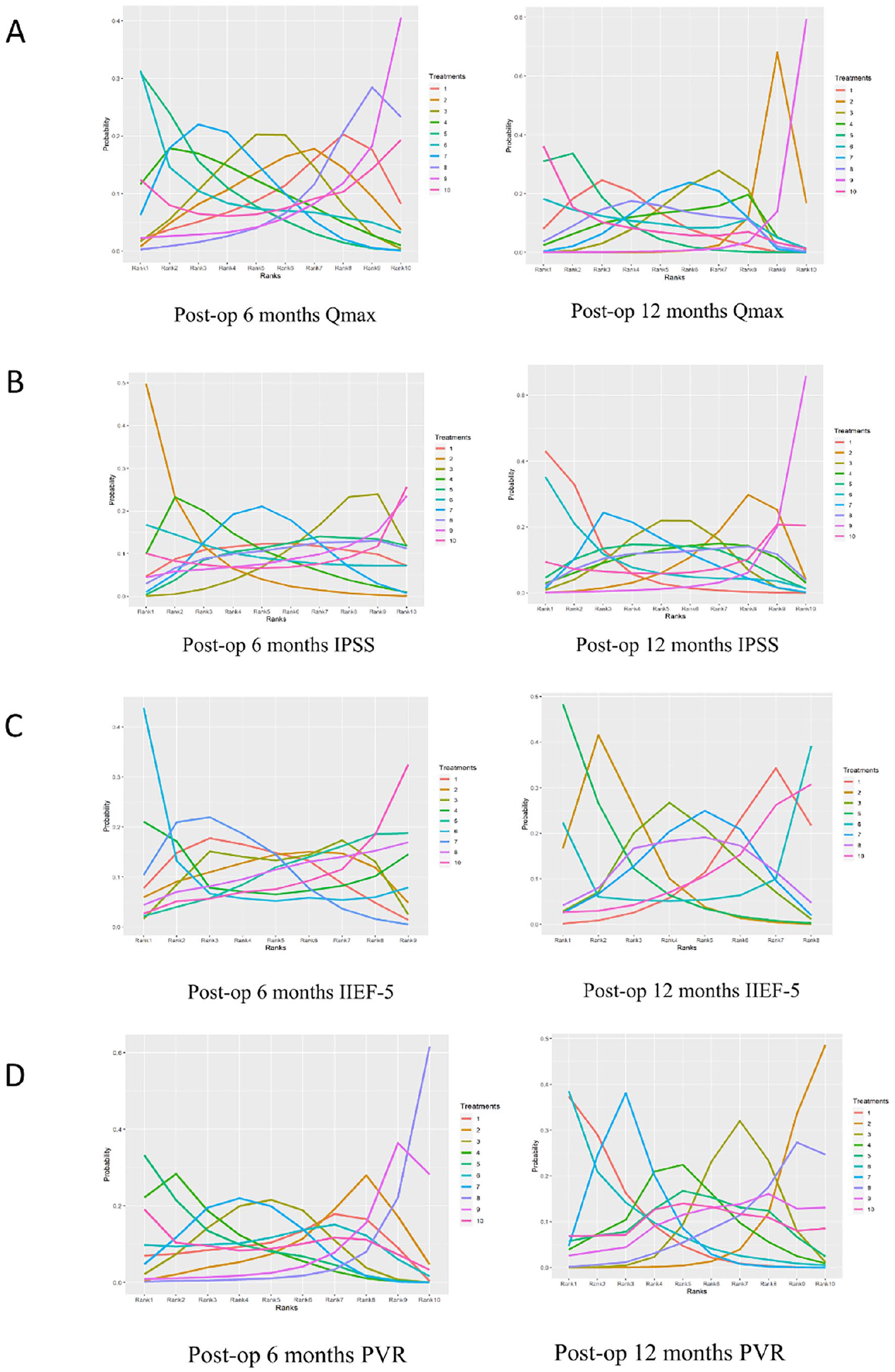
Rank Plot of 10 Surgical Methods of BPH for Functional Outcomes at 6 and 12 Months: (A) Qmax at 6 and 12 Months, (B) IPSS at 6 and 12 Months, (C) IIEF-5 at 6 and 12 Months, and (D) PVR at 6 and 12 Months.
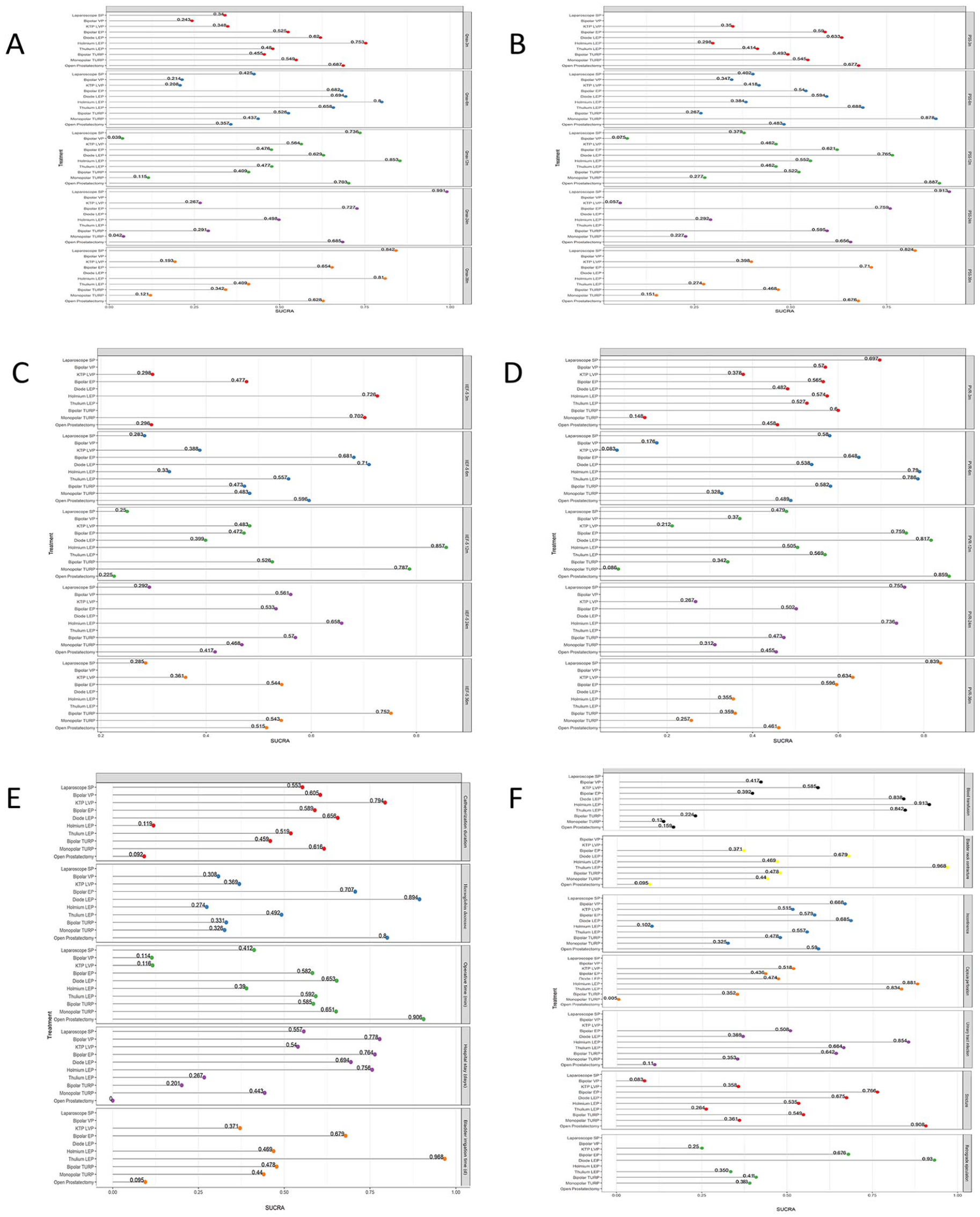
SUCRA of 10 Surgical Methods of BPH for Functional Outcomes, Perioperative Parameters, and Complications: (A): Qmax at 3, 6, 12, 24, and 36 Months; (B) IPSS at 3, 6, 12, 24, and 36 Months; (C) IIEF-5 at 3, 6, 12, 24, and 36 Months; (D) PVR at 3, 6, 12, 24, and 36 Months; (E) Catheterization Duration, Hemoglobin Decrease, Operative Time, Hospital Stay, and Bladder Irrigation Time; and (F) Blood Transfusion, Bladder Neck Contracture, Incontinence, Capsule Perforation, Urinary Tract Infection, Urinary Stricture, and Retrograde Ejaculation.
Functional Outcomes
Qmax
There were 26, 25, 31, 13, and nine trials reported Qmax values at postop 3, 6, 12, 24, and 36 months, respectively. Overall, holmium LEP, diode LEP, bipolar EP, and laparoscope SP achieved better Qmax than monopolar TURP at postop 6 to 36 months (Figure 4A). The SUCRA indicated holmium LEP (SUCRA, 0.753), OP (SUCRA, 0.687), and diode LEP (SUCRA, 0.620) demonstrated higher probability for superiority, but bipolar VP (SUCRA, 0.243) had the lowest ranking probabilities to be the best at postop third month follow-up. At postop sixth month, holmium LEP (SUCRA, 0.800), diode LEP (SUCRA, 0.694), and bipolar EP (SUCRA, 0.682) were the top three effective surgical methods according to SUCRA values, but KTP LVP (SUCRA, 0.208) and bipolar VP (SUCRA, 0.214) were ranked lower than other surgical methods. At postop 12th month, holmium LEP (SUCRA, 0.853) and laparoscope SP (SUCRA, 0.736) were ranked higher than other treatments, but bipolar VP was ranked the lowest (SUCRA, 0.039). At postop 24th month, laparoscope SP (SUCRA, 0.991) and bipolar EP (SUCRA, 0.727) performed better than other treatments, but monopolar TURP (SUCRA, 0.042) was ranked the lowest. Laparoscope SP (SUCRA, 0.842), holmium LEP (SUCRA, 0.810), and bipolar EP (SUCRA, 0.654) were ranked higher than others, but monopolar TURP (SUCRA, 0.121) was ranked the lowest at 36th month. With OP as the common comparator, monopolar TURP (MD −2.14 mL/s, 95% credible interval [CrI] = [−3.62 to −0.70]) and bipolar VP (−3.20 mL/s, 95% CrI = [−5.83 to −0.67]), demonstrated worse Qmax at 12th month, respectively (Table 1). Monopolar TURP identified worse Qmax (MD = −2.51 mL/s, 95% CrI = [−4.56 to −0.50]), but laparoscope SP identified better Qmax compared with OP (MD = 2.89 mL/s, 95% CrI = [0.01, 5.71]) at 24th month (Supplementary Table 8).
Network Estimated Mean Difference (95% Credible Intervals) of 10 Surgical Methods of BPH for Functional Outcomes at 6 and 12 Months.
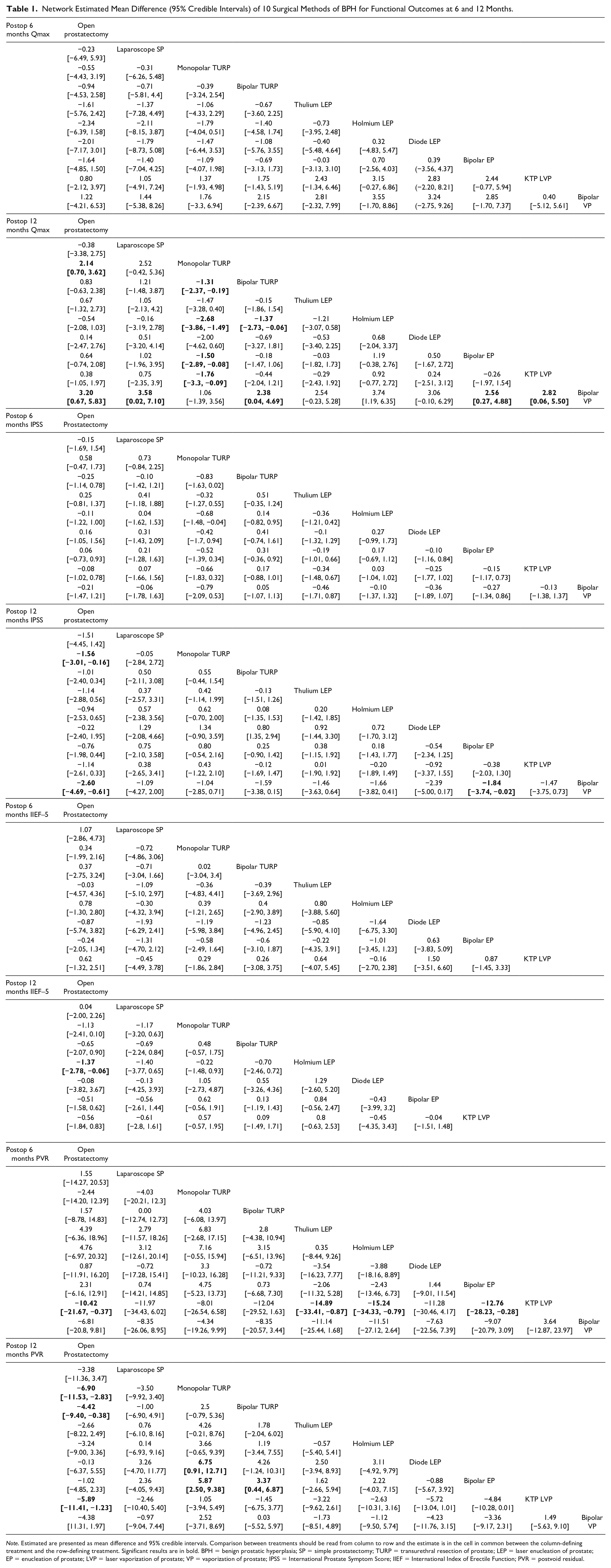
Note. Estimated are presented as mean difference and 95% credible intervals. Comparison between treatments should be read from column to row and the estimate is in the cell in common between the column-defining treatment and the row-defining treatment. Significant results are in bold. BPH = benign prostatic hyperplasia; SP = simple prostatectomy; TURP = transurethral resection of prostate; LEP = laser enucleation of prostate; EP = enucleation of prostate; LVP = laser vaporization of prostate; VP = vaporization of prostate; IPSS = International Prostate Symptom Score; IIEF = International Index of Erectile Function; PVR = postvoid residual.
IPSS
There were 14, 23, 27, nine, and eight trials reported IPSS values at postop 3, 6, 12, 24, and 36 months, respectively. At third month, OP (SUCRA, 0.677), diode LEP (SUCRA, 0.633), and bipolar EP (SUCRA, 0.590) were ranked better than other surgical methods (Figure 4B). At sixth month, monopolar TURP (SUCRA, 0.878), thulium EP (SUCRA, 0.688), and diode LEP (SUCRA, 0.594) were ranked better than other surgical methods. At 12th month, OP (SUCRA, 0.887), diode LEP (SUCRA, 0.765), and bipolar EP (SUCRA, 0.621) were ranked better than other surgical methods, but bipolar VP (SUCRA, 0.075) was ranked the lowest. At 24th month, laparoscope SP (SUCRA, 0.913) and bipolar EP (SUCRA, 0.759) were ranked better than other surgical methods, but KTP LVP (SUCRA, 0.057) had the lowest probability of being were ranked best. At 36th month, laparoscope SP (SUCRA, 0.824) and bipolar EP (SUCRA, 0.710) were ranked better than other surgical methods, but monopolar TURP (SUCRA, 0.151) was ranked the lowest. Compared with OP, monopolar TURP (MD = 1.56, 95% CrI = [0.16, 3.01]) and bipolar VP (MD = 2.6, 95% CrI = [0.61, 4.69]) demonstrated worse IPSS at 12th month (Table 1).
IIEF-5
There were six, 12, 12, seven, and six trials reported IIEF-5 values at postop 3, 6, 12, 24, and 36 months, respectively. At third month, holmium LEP (SUCRA, 0.726) performed the best, but OP (SUCRA, 0.296) and KTP LVP (SUCRA, 0.298) performed worse than other surgery methods (Figure 4C). At 6th month, diode LEP (SUCRA, 0.710) and bipolar EP (SUCRA, 0.681) performed better than other surgical methods, but laparoscope SP (SUCRA, 0.283) was ranked the lowest. At 12th month, holmium LEP (SUCRA, 0.857) performed the best, but OP (SUCRA, 0.225) was ranked the lowest. At 24th month, holmium LEP (SUCRA, 0.658) performed the best, but laparoscope SP (SUCRA, 0.292) was ranked the lowest. At 36th month, bipolar EP (SUCRA, 0.752) performed the best, but laparoscope SP (SUCRA, 0.285) was ranked the lowest. Compared with OP, holmium LEP (MD = 1.37, 95% CrI = [0.06, 2.78]) demonstrated better IIEF-5 at 12th month (Table 1).
PVR
There were 18, 19, 23, eight, and eight trials reported PVR values at postop 3, 6, 12, 24, and 36 months, respectively. At third month, laparoscope SP (SUCRA, 0.697) were ranked the best and monopolar TURP (SUCRA, 0.148) was ranked the lowest (Figure 4D). At sixth month, holmium LEP (SUCRA, 0.790) and thulium EP (SUCRA, 0.786) performed better than other surgical methods and the lowest ranked method was KTP LVP (SUCRA, 0.083). At 12th month, OP (SUCRA, 0.859), diode LEP (SUCRA, 0.817), and bipolar EP (SUCRA, 0.759) performed better than other surgical methods and monopolar TURP (SUCRA, 0.086) was ranked the lowest. At 24th month, laparoscope SP (SUCRA, 0.755) and holmium LEP (SUCRA, 0.736) performed better than other surgical methods and the lowest ranked method was KTP LVP (SUCRA, 0.267). At 36th month, laparoscope SP (SUCRA, 0.839) performed the best and monopolar TURP (SUCRA, 0.257) was ranked the lowest. Compared with OP, KTP LVP demonstrated worse PVR at sixth (MD = 10.42 mL, 95% CrI = [0.37, 21.67]) and 12th month (MD = 5.89 mL, 95% CrI = [1.23, 11.41]), and monopolar TURP (MD = 6.90 mL, 95% CrI = [2.83, 11.53]) and bipolar TURP (MD = 4.42 mL, 95% CrI = [0.38, 9.40]) identified worse PVR at 12th month (Table 1).
Subgroup Analysis
Among these trials that provided preoperative mean prostate volume data, 22, 11, and 15 trials identified mean prostate volumes of 60 up to 80, 80 to 100, and more than 100 mL, respectively. For the Qmax, IPSS, and IIEF-5 at postop 6 month, there were no significantly statistical difference between different surgery methods and OP in the subgroups of different mean prostate volume (>80 or ≤80 mL, ≤100 or >100 mL; Supplementary Tables 9 and 10). Bipolar VP performed worse than other surgery methods in terms of Qmax and IPSS, KTP LVP performed worse than other surgery methods in terms of PVR in the subgroup analyses of prostate volume >80 and >100 mL at postop 12th month.
Perioperative Parameters
Duration of Catheterization
The duration of catheterization was reported in 36 trials. The SUCRA score identified that among the included studies, KTP LVP (SUCRA, 0.794) and diode LEP (SUCRA, 0.656) demonstrated higher rank probability, and all treatments performed better than OP (SUCRA, 0.092; Figure 4F and Supplementary Figure 3). Compared with OP, catheterization duration decreased from 3.69 days (95% CrI = [0.66, 6.70]) for monopolar TURP to 0.22 days (95% CrI = [−3.36, 3.82]) for holmium LEP (Supplementary Table 8).
Hemoglobin Decrease
The hemoglobin decrease was reported in 14 trials. Diode LEP (SUCRA, 0.894) was ranked higher than OP (SUCRA, 0.800). However, none of the comparisons reached statistically difference.
Operative Time
The duration of operative time was reported in 41 trials. OP (SUCRA, 0.906) was ranked the highest and bipolar VP (SUCRA, 0.114) and KTP LVP (SUCRA, 0.116) performed lower than other methods. Compared with OP, bipolar VP (MD = 26.23 min, 95% CrI = [5.73, 46.72]) and KTP LVP (MD = 24.00 min, 95% CrI = [11.80, 36.38]) demonstrated longer operative time.
Hospital Stay
The duration of hospital stay was reported in 36 trials. Bipolar VP (SUCRA, 0.778), bipolar EP (SUCRA, 0.764), and holmium LEP (SUCRA, 0.756) were ranked higher and all treatments performed better than OP (SUCRA, 0.000). Compared with OP, hospital stay decreased from 5.54 days (95% CrI = [3.35, 7.76]) for diode LEP to 3.65 days (95% CrI = [2.36, 4.97]) for monopolar TURP.
Bladder Irrigation Time
The duration of bladder irrigation time was reported in nine trials. Thulium LEP (SUCRA, 0.968) and bipolar EP (SUCRA, 0.679) were ranked higher and all treatments performed better than OP (SUCRA, 0.095). Compared with OP, bladder irrigation time decreased from 6.09 days (95% CrI = [1.63, 10.57]) for diode LEP to 4.50 days (95% CrI = [0.57, 8.40]) for monopolar TURP.
Complications
Short-Term Complications
Blood transfusion events were reported in 25 trials. Enucleation and vaporization methods using either laser or bipolar energy were ranked higher than bipolar/monopolar TURP and OP (Figure 4G). Compared with OP, thulium LEP, holmium LEP, and diode LEP performed better and reached statistical significance, respectively (Supplementary Table 8).
In the 12 trials reporting bladder neck contracture events, thulium LEP (SUCRA, 0.968) and diode LEP (SUCRA, 0.679) were ranked higher than monopolar TURP (SUCRA, 0.440) and OP identified the worst rank probability (SUCRA, 0.095). Compared with OP, thulium LEP and bipolar EP performed better and reached statistical significance, respectively.
In the nine trials reporting capsule perforation events, holmium LEP (SUCRA, 0.881) and thulium LEP (SUCRA, 0.834) were ranked higher than other surgery methods and monopolar TURP identified the worst rank probability (SUCRA, 0.005). Compared with monopolar TURP, all treatments performed better and reached significantly statistical difference.
In the 15 trials reporting urinary tract infection events, holmium LEP (SUCRA, 0.854) was ranked higher than monopolar TURP (SUCRA, 0.353), whereas OP (SUCRA, 0.110) identified the worst rank probability. Compared with OP, all treatments did not reach statistical difference.
The incontinence events were reported in 23 trials. We did not find significantly statistical difference between these different surgery methods.
Long-Term Complications
In the 30 trials reporting urinary stricture events, OP (SUCRA, 0.908) was ranked higher than other treatments, whereas bipolar VP (SUCRA, 0.083) identified the worst rank probability. Compared with OP, monopolar TURP, thulium LEP, and bipolar VP reached significantly statistical difference, respectively.
In the six trials reporting retrograde ejaculation events, diode LEP (SUCRA, 0.930) and bipolar EP (SUCRA, 0.676) were ranked higher than other surgery methods, whereas KTP LVP (SUCRA, 0.250) identified the worst rank probability. We did not find significantly statistical difference between these different surgery methods.
Publication Bias
We conducted comparison-adjusted funnel plots for the functional outcomes, perioperative parameters and complications and found that the left and right distributions of each research point in most outcomes were asymmetrical, suggesting that there may be small study bias (Supplementary Figure 4).
Discussion
Monopolar TURP is regarded as the gold standard surgical method for BPH, but its role in treating larger glands is limited mainly due to the severe preoperative symptoms. OP was recommended as an alternative to monopolar TURP for larger glands (Geavlete et al., 2015). In our systematic review and network meta-analysis, we found that holmium LEP, diode LEP, bipolar EP, and laparoscope SP appeared to be superior in efficacy compared with OP and monopolar TURP in the treatment of BPH with volume > 60 mL. Bipolar VP and KTP LVP maybe not suitable for larger prostates due to worse short- and middle-term Qmax, IPSS, and PVR than OP. In addition, bipolar VP performed worse than other surgery methods in terms of Qmax and IPSS, KTP LVP performed worse than other surgery methods in terms of PVR in the subgroup analyses of prostate volume >80 and >100 mL at postop 12th month. Moreover, eight new surgery methods were safer than OP because OP had longer time of catheterization, hospital stay and bladder irrigation, and higher rates of blood transfusion, bladder neck contracture, and urinary tract infection. In addition, eight new surgery methods were safer than monopolar TURP, resulting in fewer rates of blood transfusion, bladder neck contracture, and capsule perforation.
From the above results, we could recognize that these better improvements in the efficacy of enucleation methods are not only related to the type of energy used, whether laser or bipolar, but are also related to the technique itself (Placer et al., 2009). Enucleation separates rapidly the adenoma from the prostatic capsules using the resectoscope sheath and mimicking the surgeon’s finger, and resulting in more complete adenoma removal (Kuntz et al., 2004), thus optimizing coagulation and prostate ablation. Bipolar system can more effectively relieve bladder outlet obstruction, reduce bladder pressure, and change the high-pressure state of bladder detrusor muscle, so as to facilitate the recovery of physiological function of bladder detrusor muscle and improve urination function (Kim et al., 2017). In addition, there was no electric current to stimulate the surrounding tissues during the operation, thus reducing the stimulation to the erectile nerve, which has a positive effect on the recovery of postoperative sexual function. Laser has the advantages of more complete and thorough removal of tissue (Guo et al., 2016). The vaporization appears marked by a somewhat lower ability to improve functional outcomes when compared with the resection and enucleation methods as well as with the OP. KTP and bipolar vaporization bring in the upper hand of superior hemostatic properties and cause very little bleeding, but serious questions about the ability to remove tissue must be addressed, especially when larger prostates bulks are involved (Geavlete et al., 2015). For the operative time, vaporization was the worst method, which may be related to the longer time required for complete evaporation.
The treatment targets for BPH are not only to relieve LUTS but also to prevent adverse events related to BPH (Stroup et al., 2012; Vela-Navarrete et al., 2005). Through this network meta-analysis, we found that OP was more invasive and OP and monopolar TURP had worse perioperative complications than other minimally invasive surgeries. Our results supported changes in the treatment of BPH from OP and monopolar TURP to new surgical methods. In our study, patients who have undergone the treatment of enucleation methods recovered significantly faster after surgery and there were fewer postoperative complications (Sturch et al., 2015; Vincent & Gilling, 2015; Zhang et al., 2013).
The use of resection, enucleation, or vaporization methods depends on the patient’s condition, surgeon’s skill and experience, availability of required equipment, and factors such as prostate volume and comorbidities. Within different health services, cost differences could be influenced by a variety of factors. Widespread use of lasers and bipolar energy in developing countries was limited by long learning curves, high costs, and lack of expertise and endoscopic equipment. Studies have reported that holmium LEP requires a long learning curve of more than 40 cases (Elshal et al., 2017) and increasing surgical experience can help shorten the operation time (Gilling, 2020; Shigemura et al., 2017). Compared with laser systems, bipolar energy machine have more functions and cheaper equipment and medical consumable materials (Rai et al., 2018). With the increasing understanding of the local fine anatomy of the prostate and its surrounding tissues, the continuous improvement of surgical techniques, and the continuous reduction of laser equipment prices, these technologies will become more and more popular.
Our study has several strengths as follows. First, this is the first network meta-analysis to compare 10 different surgical treatments for BPH with volume >60 mL and to conduct subgroup analyses according to prostate volume (>80/≤80 and >100/≤100 mL). Second, we compared IPSS, Qmax, PVR, and IIEF-5 values at postop 3, 6, 12, 24, and 36 months to assess the short- to middle-term effects of different treatments. Third, we included RCTs without language restrictions to avoid bias.
Our study has several potential limitations. First, most complications were rare, several RCTs recorded zero events, and several interventions were lacking data for comparisons. As a result, the estimation of pooled odds ratio is less precise. Anyway, the heterogeneity was low in pairwise comparisons. Although the number of studies on complications was small, the results of network meta-analyses were relatively consistent. Therefore, we did not conduct further subgroup analysis. Second, OP was performed in only 11 of the 52 papers reviewed. We must concern the inaccuracy against OP when it is not performed in the overwhelming majority of the studies included and relatively small participants. The same is true for the other procedures as well. More high-quality RCTs with a larger sample size are urgently needed. Third, although the definitions and techniques are relatively standardized for the 10 surgical methods, there could be several modifications in several surgical methods. We need to be cautious about the results of comparing different surgical procedures. Fourth, prostate size is an important factor for translating results into clinical practice and decision-making and is not rigorously displayed in all studies. We used the mean prostate volume of each article in the subgroup analysis on the relationship between prostate size and outcome, as we cannot obtain individual patient data. This method is prone to ecological bias and confusion of study level. Firth, outcomes were evaluated blindly in only a few trials, which might cause bias in favor of the new surgery treatments. Sixth, we did not analyze early urinary symptoms, such as urgency, dysuria, or pain after urination, because these symptoms generally improve at postop 2 to 3 months with medication. Intermediate- and long-term studies often harbored a high rate of dropouts. Finally, our study did not include several new surgery treatments for BPH, such as prostatic urethral lift, prostate artery embolization, robot-assisted prostatectomy, and water vaporization. Urethrae lift and prostate artery embolization are largely applied in patients not appropriate for operation or anesthesia. As the target patient population of these new approaches are different from that in our study, we excluded these approaches from our meta-analysis. Moreover, water vaporization and robotic simple prostatectomy have not yet been compared with TURP or OP in any RCTs.
Conclusion
Eight new surgical methods for BPH with volume >60 mL appeared to be superior in safety compared with OP and monopolar TURP. Holmium LEP, diode LEP, bipolar EP, and laparoscope SP appeared to be superior in efficacy compared with OP and monopolar TURP. KTP LVP maybe not suitable for larger prostates due to worse short- and middle-term Qmax, IPSS, and PVR than OP. The efficacy of these new surgical methods in larger prostates requires further research for more evidence. Long-term assessment is lacking and evaluation of adverse events is not sufficient. A larger sample size and high-quality RCTs are needed to confirm and support this network meta-analysis.
Supplemental Material
sj-docx-1-jmh-10.1177_15579883211067086 – Supplemental material for Comparison on the Efficacy and Safety of Different Surgical Treatments for Benign Prostatic Hyperplasia With Volume >60 mL: A Systematic Review and Bayesian Network Meta-Analysis of Randomized Controlled Trials
Supplemental material, sj-docx-1-jmh-10.1177_15579883211067086 for Comparison on the Efficacy and Safety of Different Surgical Treatments for Benign Prostatic Hyperplasia With Volume >60 mL: A Systematic Review and Bayesian Network Meta-Analysis of Randomized Controlled Trials by Yong-Bo Wang, Si-Yu Yan, Xiao-Feng Xu, Xing Huang, Li-Sha Luo, Yu-Qing Deng, Xu-Hui Li, Qiao Huang, Yun-Yun Wang, Jiao Huang, Ying-Hui Jin and Xian-Tao Zeng in American Journal of Men's Health
Footnotes
Author Contributions
Y.-B.W., Y.-H.J., and X.-T.Z. designed the research, analyzed the data, and wrote the draft manuscript. Y.-B.W., S.-Y.Y., and X.-F.X. performed literature search, extracted, and analyzed the data. X.H., Q.H., L.-S.L., and Y.-Y.W. analyzed data and provided critical scientific input. Y.-B.W., Y.-Q.D., and X.-H.L. were responsible for resolving discrepancies regarding quality of the included studies, reviewing the manuscript, and providing critical scientific input. All authors made contribution to this article, read, and approved the final version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Key Research and Development Plan of China (Technology helps Economy 2020; 2016YFC0106302), without any financial interest or benefit.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.