
Abstract
This study aimed to determine the potential association between handgrip strength and nutritional quality in Korean men aged ≥20 years using data from the Korea National Health and Nutrition Examination Survey 2016 to 2018. This population-based cross-sectional study included 5,748 men aged ≥20 years. A dietary intake survey was performed using the 24-hr dietary recall method. Nutritional quality was examined using the Index of Nutritional Quality (INQ) score. A high INQ score reflected poor nutritional quality, with insufficient intake of many nutrients. Multivariate linear regression was used to determine the association between handgrip strength and INQ scores after adjusting for other covariates. The intake of carbohydrates, fiber, calcium, and vitamins B2 and C was significantly positively associated with a higher quartile for handgrip strength for those aged ≥65 years (all p < .01). A significant inverse association was found between the quartiles of handgrip strength and INQ scores among men aged ≥65 years after adjusting for all covariates (β = −0.26, p < .01). This association was not found among those aged <65 years (p = .25). The age-specific association between handgrip strength and nutritional quality underscores the importance of public policies that promote sufficient and comprehensive nutrient intake among older adults. Handgrip strength may be useful in clinical practice as a simple and cost-effective tool for screening for nutritional quality in older adults.
Introduction
Nutrition is an essential aspect of health and quality of life (Cederholm et al., 2019; Chen et al., 2018). Particularly, it is estimated that one in six older individuals is malnourished or at risk of undernutrition in South Korea (Kim et al., 2019). Inadequate nutrition is reported to be associated with declining general health, immune dysfunction, reduced physical and cognitive function, higher hospital admission and readmission rates, delay in recovery from illness, and mortality in older adults (Gabrovec et al., 2018; Kaiser et al., 2010). Numerous studies have attempted to identify and investigate the potential indicators of nutritional status. Various screening tools have been used. These include anthropometric measures such as body mass index and bioelectrical impedance analysis, and laboratory parameters such as serum albumin, prealbumin, and transferrin (Juby & Mager, 2019; Reber et al., 2019; Russell, 2015). There is no single efficient and effective tool to readily measure comprehensive nutritional status in clinical practice.
Handgrip strength, an easy and quick method for measuring muscle strength, has been used to indirectly assess disability and frailty (Bohannon, 2015; Norman et al., 2011). Several studies have focused on the association between handgrip strength and dietary intake, as a potential predictor of nutritional status (Buckinx et al., 2019; Norman et al., 2011). However, most studies on the relationship between handgrip strength and nutritional status have focused on a single nutrient in a specific vulnerable group. Relatively little research has been conducted on the association between handgrip strength and nutritional quality. This would require a comprehensive macro- and micronutrient intake analysis among older and younger adults using a nationwide sample from Asia.
We aimed to determine the association between handgrip strength and nutritional quality in South Korean men aged <65 years and in those aged ≥65 years using data from the Korea National Health and Nutrition Examination Survey (KNHANES).
Materials and Methods
Data Source and Study Participants
This study was based on data collected from KNHANES Ⅶ (2016–2018). KNHANES Ⅶ is a nationwide cross-sectional survey that combines health interviews and physical and laboratory examinations to assess the health and nutritional status of a representative population in South Korea. It is conducted by the Korea Centers for Disease Control and Prevention (Kweon et al., 2014).
The participants were men aged ≥20 years and they had complete health data including a health interview, physical examination, laboratory tests, and nutritional survey data. Participants with a history of cancer, chronic kidney disease, or thyroid disease and those treated for tuberculosis were excluded. These individuals were likely to have specific nutritional requirements or diets. Participants who reported an implausible total calorie intake (<500 kcal/day or >4,000 kcal/day) were excluded from the study to improve the reliability of the analysis. Written informed consent was obtained from all participants, and the KNHANES has been approved by the Institutional Review Board of the Korea Centers for Disease Control and Prevention (2018-01-03-P-A).
Measurement of Handgrip Strength
Handgrip strength was measured using a digital grip strength dynamometer at 0.1 kg intervals (T.K.K. 5401; Takei, Tokyo, Japan) (Kim et al., 2019; Kweon et al., 2014). While exhaling, using only one hand at a time, the participants were asked to squeeze the dynamometer continuously with full force until they were unable to squeeze any harder (Kim et al., 2019). Three measurements were recorded for each hand alternately, with a 60-s rest period between measurements of the same hand. The maximum value among all six measurements was used in the analysis and expressed in kilograms. For the analysis stratified by quantitative handgrip strength in each age group (<65 and ≥65 years), the participants’ final reading was divided into four levels using quartiles.
Dietary Intake and Nutrition Assessment
The survey on dietary intake and nutrition was conducted by professional interviewers using a 24-hr dietary recall method. Data on all foods and beverages consumed by the participants in the 24 hr prior to the survey were collected (Kweon et al., 2014). The total daily calorie intake and nutrient intake were further calculated from the collected data using a standard Korean food composition table (Kweon et al., 2014). Diet quality was evaluated using the Index of Nutritional Quality (INQ) based on nutrient density. This index is expressed as the amount of each nutrient per 1,000 kcal. The intake of each nutrient was calculated as a ratio of the nutrient density of the recommended dietary allowance intake of the nutrient. This was calculated per 1,000 kcal according to age (Sorenson et al., 1976; Shayanfar et al., 2018). The standard recommended intakes for protein; fiber; vitamins A, B1, B2, B3, and C; calcium; potassium; and iron were used to calculate the ratios. A ratio ≥1.0 for each nutrient indicated a sufficient nutritional intake, whereas a value <1.0 indicated an insufficient nutrient intake. The number of nutrients with an insufficient intake was defined as the INQ score. The score ranged from 0 to 10. A low INQ score indicated a high-quality diet.
Sociodemographic and Health-Related Covariates
Participants’ sociodemographic data were obtained through interviews or self-reported questionnaires. Participants who were married and lived with their spouses were defined as “married.” A higher educational level was defined as at least the completion of a college education. Individuals were classified into four groups according to their occupation: non-manual workers (general managers, professionals, and office workers), service or sales workers, manual workers (skilled agricultural, forestry, and fishery workers; craft and related trade workers; plant and machine operators or assemblers; and elementary workers), and unemployed individuals.
Health-related behaviors included cigarette smoking, alcohol consumption, and physical activity. Participants who smoked at the time of the survey or had smoked ≥100 cigarettes in their lifetime were regarded as current smokers. Those who consumed seven or more drinks at least twice a week were considered heavy drinkers. Adequate physical activity was defined as moderate-intensity activity for at least 150 min during the week, vigorous-intensity activity for at least 75 min during the week, or an equivalent combination of moderate- and vigorous-intensity activities (Hagströmer et al., 2006).
A health examination, which included anthropometry, blood pressure measurement, and blood analysis, was conducted by trained medical personnel according to standardized protocols. Body mass index (BMI) was calculated as body weight in kilograms divided by the square of height in meters (kg/m2). A BMI ≤18.5 kg/m2 and a BMI ≥25 kg/m2 were used to define underweight and obesity, respectively. Blood pressure was measured using a standard sphygmomanometer (Wall Unit 33 (0850); Baumanometer®, New York, USA) after a 5-min rest in a seated position. Venous blood samples collected after 12 hr of fasting were obtained for blood glucose and lipid profile measurements. Chronic diseases were defined using the following criteria: hypertension, increased blood pressure (systolic ≥140 mmHg or diastolic ≥90 mmHg) or use of antihypertensive medications; diabetes, fasting blood glucose levels ≥126 mg/dL, self-reported medical history of being diagnosed by a health professional, or use of antidiabetic medications; and dyslipidemia, total cholesterol levels ≥240 mg/dL, serum triglyceride levels ≥200 mg/dL in fasting blood samples, or use of medications for dyslipidemia.
Statistical Analysis
Statistical analyses were conducted using SAS 9.4 (SAS Institute Inc., Cary, NC, USA). Sample weights assigned to participants’ data for analysis were used to arrive at estimates representative of the Korean population for the survey period. A multistage clustered and stratified randomized sampling method based on National Census data was used (Kweon et al., 2014). We conducted all analyses for each group (aged <65 and ≥65 years) separately owing to the differences in their cut-off values of handgrip strength and recommended allowances of nutrient intake. The participants were categorized into four groups according to handgrip strength quartiles. Participants’ characteristics were compared between the age groups and among the in-group quartiles. Data are presented as weighted percentages with standard errors for categorical variables using weighted chi-square tests and as mean values with standard errors for continuous variables using weighted t-tests or weighted analysis of variance. Multiple linear regression was used to determine the association between handgrip strength and INQ scores after adjusting for potential confounding covariates, including age; household income; marital status; educational level; occupation; smoking status; heavy drinking; adequate physical activity; obesity; chronic diseases such as hypertension, diabetes, and dyslipidemia; and total calorie intake. P values <0.05 were considered significant.
Results
In total, 31,689 (10,806 in 2016, 10,430 in 2017, and 10,453 in 2018) Koreans were selected from the KNHANES Ⅶ (2016–2018) using a two-stage stratified cluster and complex sampling method. Of these, 24,269 (8,150 in 2016, 8,127 in 2017, and 7,992 in 2018) participants who had complete health data, which included a health interview, health examination, and nutrition survey data, were included. We excluded the following participants: individuals aged <20 years (n = 5,072); women (n = 10,732); participants with missing data (n = 657); those with a history of cancer (n = 333), chronic kidney disease (n = 32), or thyroid disease (n = 103); those with tuberculosis (n = 3); and those who reported implausible total calorie intakes (<500 kcal/day or >4,000 kcal/day) (n = 1,589). This study finally included 5,748 South Korean men (Figure 1).

Study Participant Data Obtained From the Korea National Health and Nutrition Examination Survey Ⅶ (2016–2018).
General Patient Characteristics
In total, 5,748 men with complete data were included. The average age was 41.7 years in the group aged <65 years and 72.7 years in the group aged ≥65 years. Those in the group aged ≥65 years who had lower household incomes, lower levels of education, and higher levels of unemployment were less likely to be current smokers or heavy alcohol drinkers. They were also less likely to engage in adequate physical activity than those in the group aged <65 years. Handgrip strength values were significantly higher in the group aged <65 years than in the group aged ≥65 years. In Table 1, the characteristics of both groups are compared according to the quartiles of handgrip strength (the participants’ general characteristics according to age group are presented in Supplemental Table 1).
General Characteristics of Men According to Quartiles of Handgrip Strength.

Data are expressed as weighted % for categorical variables and as mean values for continuous variables with their standard errors. bAnalyzed using weighted t-tests or weighted χ2-tests to assess differences between adults aged <65 years and those aged ≥65 years. cParticipants who smoked at the time of the survey and who had smoked ≥100 cigarettes in their lifetime. dParticipants who consumed seven or more drinks at least twice a week. eParticipants who engaged in moderate-intensity activities for at least 150 min during the week, vigorous-intensity activities for at least 75 min during the week, or an equivalent combination of moderate- and vigorous-intensity activities.
Nutrient Intake and Diet Quality According to Handgrip Strength
The total daily dietary intake data analysis showed that, in the group aged ≥65 years, men in the higher quartiles of handgrip strength had significantly higher intakes of carbohydrates, fiber, calcium, and vitamins B2 and C than men in the lower quartiles. Among this group (≥65 years), the mean daily intakes of carbohydrates, fiber, calcium, and vitamins B2 and C for each quartile were, respectively, as follows: 291.0 ± 5.9 g, 22.7 ± 0.8 g, 403.0 ± 15.5 g, 1.0 ± 0.4 × 10−1 mg, and 58.4 ± 4.2 mg for Quartile 1; 313.7 ± 7.3 g, 26.6 ± 1.0 g, 484.1 ± 20.6 g, 1.3 ± 0.5 × 10−1 mg, and 66.6 ± 4.9 mg for Quartile 2; 323.3 ± 6.7 g, 27.5 ± 0.8 g, 514.4 ± 19.4 g, 1.4 ± 0.5 × 10−1 mg, and 77.1 ± 4.9 mg for Quartile 3; and 340.5 ± 6.8 g, 30.2 ± 0.8 g, 561.3 ± 22.5 g, 1.5 ± 0.4 × 10−1 mg, and 93.0 ± 6.6 mg for Quartile 4 (p < .01) (Table 2).
Nutrient Intakes According to Quartiles of Handgrip Strength.

Data are expressed as mean values with their standard errors. bAnalyzed using a weighted analysis of covariance according to quartiles of handgrip strength among study participants aged <65 and ≥65 years.
Association Between Handgrip Strength and Dietary Quality in Men Aged <65 and ≥65 Years
The INQ scores for the total daily meals decreased with the quartiles among men aged ≥65 years. The mean INQ scores for each quartile among men aged ≥65 years were, respectively, as follows: 5.40 ± 0.15 for Quartile 1, 4.83 ± 0.13 for Quartile 2, 4.68 ± 0.15 for Quartile 3, and 4.42 ± 0.14 for Quartile 4 (p < .01). However, there was no significant association between handgrip strength quartiles and INQ scores among men aged <65 years (p = .25), as presented in Figure 2. A significant inverse association was found between handgrip strength quartiles and INQ scores among men aged ≥65 years after adjusting for all covariates (β = −0.26, p < .01) (Table 3).
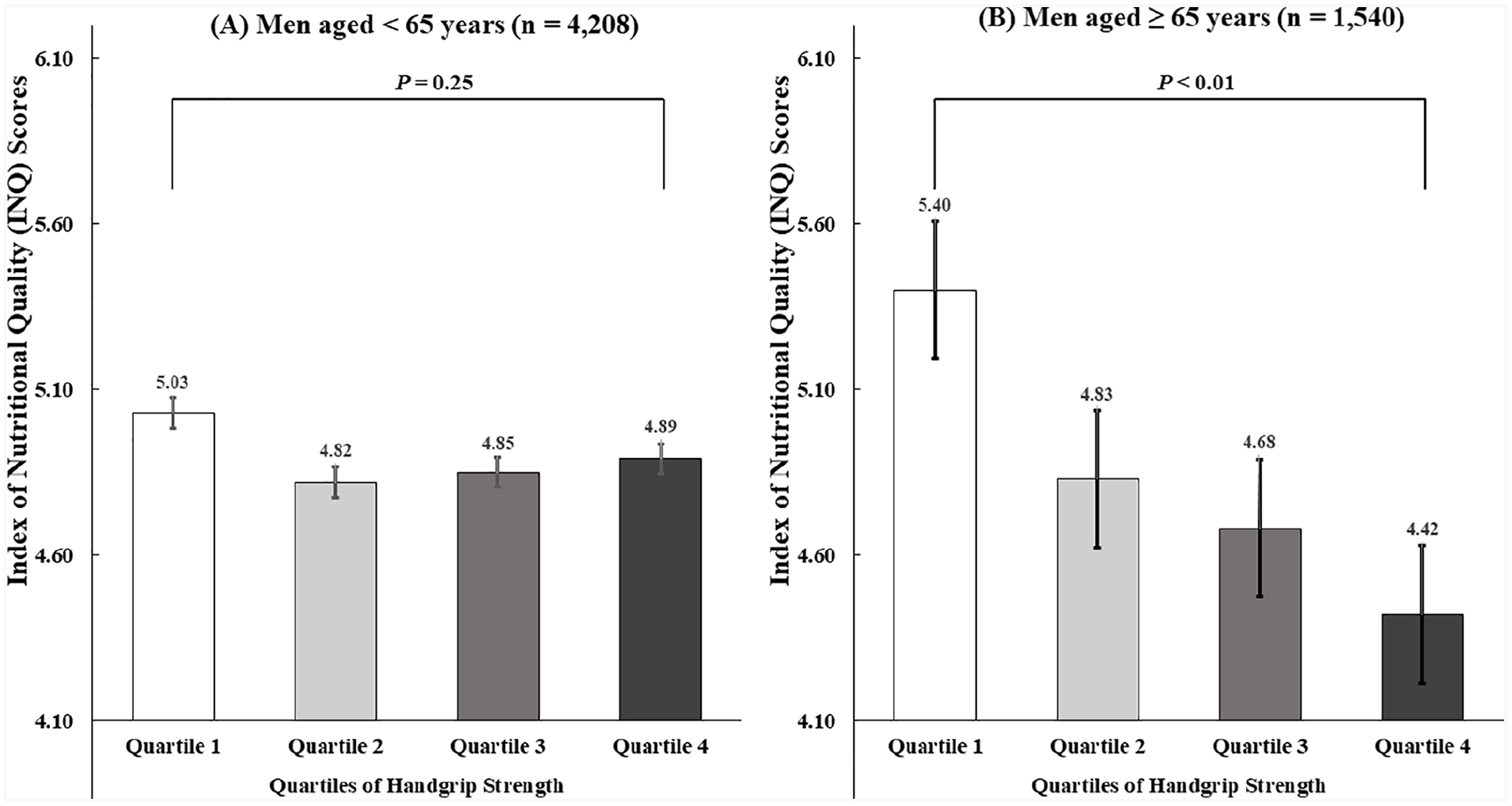
Comparison of the Index of Nutritional Quality (INQ) Scores From Total Meals Per Day According to Quartiles of Handgrip Strength Among Study Participants Aged <65 Years and Those Aged ≥65 Years Using Weighted Linear Regression Analysis.
Multivariate Linear Regression Analysis of Handgrip Strength According to INQ a Scores in Men Aged <65 and ≥65 Years.

The Index of Nutritional Quality (INQ) of each nutrient, including proteins; fiber; vitamins A, B1, B2, B3, and C; calcium; potassium; and iron, was calculated as a ratio of the nutrient density of the intake to the recommended dietary allowance of the nutrient per 1,000 kcal according to age and sex. bModel 1: adjusted for age, household income, marital status, educational level, and occupation. cModel 2: additionally adjusted for smoking status, heavy drinking, adequate physical activity, obesity, and chronic diseases such as hypertension, diabetes, and dyslipidemia. dModel 3: additionally adjusted for total calorie intake.
Discussion
This study identified the association between handgrip strength and nutritional quality in men aged <65 and ≥65 years selected from a nationally representative sample of South Korean men. Our findings indicate that a sufficient intake of nutrients, including proteins; fiber; vitamins A, B1, B2, B3, and C; calcium; potassium; and iron, to meet the daily intake requirements can contribute to the maintenance of muscle health. This has a greater influence on older adults than on younger adults. We also found that in both age groups, men in the higher quartiles of handgrip strength reported adequate intakes of total calories, protein, fat, iron, sodium, and vitamins B1 and B3. However, handgrip strength was significantly associated with sufficient intakes of carbohydrates, dietary fiber, calcium, and vitamins B2 and C only in men aged ≥65 years.
Previous studies on the relationship between handgrip strength and nutritional status have primarily been conducted on hospitalized patients or older patients (Power et al., 2018; Stechmiller, 2003). Handgrip strength has been demonstrated to reflect the nutritional status in older people. However, some studies have reported mixed results. Norman et al. suggested that low handgrip strength is not suitable for supporting a diagnosis of moderate malnutrition (Norman et al., 2011). In some previous studies, the insufficient intake of specific nutrients, such as proteins, essential amino acids, vitamin D, calcium, and some antioxidants, was observed among older people with low handgrip strength (Cruz-Jentoft et al., 2020). Dietary protein and amino acids have been considered to play an essential role in muscle health owing to their anabolic effects on the musculoskeletal system. Poor intake of proteins or essential amino acids can lead to decreased muscle mass and atrophy of muscle fiber. This in turn can result in impaired muscle function (Candow et al., 2012; Cruz-Jentoft et al., 2020; Mithal et al., 2013). Vitamin D has been reported to improve muscle mass and muscle strength, and calcium functions as a collaborator in this process (Cruz-Jentoft et al., 2020; Robinson et al., 2018). While some studies have reported inconsistent results, some vitamins are known to have protective effects against oxidative stress. They have also been suggested to be highly correlated with muscle strength. Oxidative stress has been reported to have a harmful impact on muscle function with increasing age (Candow et al., 2012). Vitamins A and C have antioxidant functions that block free radical chain reactions. This process protects body tissues and slows aging. Vitamins B and C are essential for converting food intake into energy (Cruz-Jentoft et al., 2020; Mithal et al., 2013; Williams, 1989).
For quantitative and qualitative analyses of the participants’ diets, we used INQ scores to assess and compare nutritional quality (Sorenson et al., 1976). The number of nutrients for which the intake was insufficient was used to determine the INQ score. High INQ scores reflected poor nutritional quality and insufficient intake of many nutrients. Vitamins and minerals are required in small quantities in our bodies as they maintain the proper function and structure of cells and facilitate various metabolic processes (Turnlund, 1994; Williams, 1989). A balanced intake is necessary to ensure that there is no shortage of a specific nutrient.
The age-specific difference in the relationship between handgrip strength and sufficient intake of comprehensive micronutrients in this study is yet to be clarified. However, various mechanisms for this difference can be suggested. Handgrip strength in older adults is strongly correlated with muscle mass and physical performance (McKee et al., 2017; Robinson et al., 2019). A gradual decline in muscle mass and strength in older adults is a common consequence of the aging process (Mithal et al., 2013). Sarcopenia, which involves the loss of muscle mass and physical performance as well as a decline in muscle strength, occurs in relation to aging (Cruz-Jentoft et al., 2019; Drey, 2011). A reduction in muscle fiber due to atrophy, apoptosis, or denervation results in the loss of muscle mass (Candow et al., 2012). It has been identified that age-related muscle mass reduction is, in part, a result of inadequate muscle protein synthesis after anabolic stimuli and an increased breakdown of muscle protein (Fry et al., 2011). Older adults have impaired signaling pathways that are involved in muscle protein kinetics compared with young adults. We found that the group with high handgrip strength had sufficient intake of B-group vitamins. These vitamins have an essential function in the regulation of cellular metabolism and energy-producing processes of the mitochondria (Turnlund, 1994; Williams, 1989). An insufficient intake of these vitamins can influence muscle strength by reducing muscle protein synthesis or increasing muscle protein degradation, with decreased energy and capacity to regulate the signaling pathway (Mithal et al., 2013). Ahn et al. (2020) reported found that age had a distinct influence on the relationship between handgrip strength and thyroid-stimulating hormone levels in euthyroid Korean men (Ahn et al., 2020). Handgrip strength was positively associated with serum thyroid-stimulating hormone levels in older adults. In younger adults, handgrip strength was negatively associated with the level of this hormone. Accordingly, the high catabolic rate in older people and the reduced rate of muscle development and maturation in younger adults have been suggested as underlying factors leading to muscle weakness in the presence of thyroid dysfunctions. Oxidative stress associated with aging, as well as its effects on chronic inflammation, has been reported to contribute, in part, to muscle fiber apoptosis and denervation, which could lead to the development of sarcopenia (Mithal et al., 2013). Micronutrients that have antioxidant properties, such as vitamins B and C, are important for muscle fiber integrity. Owing to these potentially complex changes in the intramuscular network that are associated with aging, the influence of insufficient intake of comprehensive micronutrients on reduced handgrip strength might be much more pronounced in older adults than in younger adults (Robinson et al., 2018, 2019; Romagnoli et al., 2019). As these vitamins are not produced by the body, the importance of micronutrients that can only be replenished through dietary intake becomes evident and the difference in muscle strength resulting from differences in nutritional quality becomes more noticeable. In particular, water-soluble vitamins, including B-group vitamins, are absorbed directly into the blood and used as necessary. The remainder are released into the urine. Thus, daily intake of these vitamins is essential (Williams, 1989).
We found that a sufficient intake of various micronutrients was more effective in preventing muscle weakness in older adults than in younger adults. Previously, low handgrip strength has been reported to be associated with many poor health-related outcomes such as frailty, disability, and mortality (Bohannon, 2015; Norman et al., 2011). We may be able to determine the relationship between muscle strength and nutritional quality by evaluating the association between handgrip strength and various nutrient intake levels in both younger and older adults. However, further studies are required to identify the mechanisms underlying our results.
There are some limitations to this study. Owing to the cross-sectional design of this study, we could not report causality. In addition, as the data on nutrient intake were based on self-reports using the 24-hr recall method, under- or overestimation of consumption cannot be ruled out. Although the use of this method may not provide data that fully reflect long-term dietary habits and behaviors, this concern was mitigated by the high statistical power owing to the large sample size and the probability of revealing diverse dietary behaviors. The possibility of unmeasured confounders cannot be ruled out, and this requires analyses in further studies. However, this study included current data from a large, nationally representative sample of Korean adult men over 20 years of age.
Our finding of an age-specific association between handgrip strength and nutritional quality is crucial regarding public health concerns for healthy aging. These could be helpful in developing policies on adequate nutrition for older adults. Handgrip strength may be useful in daily clinical practice. It is a simple and cost-effective tool for assessing the nutritional quality of older people vulnerable to malnutrition. This method may assist in improving muscle strength, frailty, and quality of life.
Supplemental Material
sj-docx-1-jmh-10.1177_15579883211063339 – Supplemental material for Age-Specific Association Between Handgrip Strength and Nutritional Quality in Korean Men: A Nationwide Cross-Sectional Study
Supplemental material, sj-docx-1-jmh-10.1177_15579883211063339 for Age-Specific Association Between Handgrip Strength and Nutritional Quality in Korean Men: A Nationwide Cross-Sectional Study by Woo-young Shin and Jung-ha Kim in American Journal of Men's Health
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Written informed consent was obtained from all participants, and the KNHANES has been approved by the Institutional Review Board of the Korea Centers for Disease Control and Prevention (2018-01-03-P-A).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.