
Abstract
Objective
To examine the relationship between urinary cotinine and serum vitamin A levels in Korean adults.
Methods
A total of 4445 adults (age ≥19 years) participating in the Korea National Health and Nutrition Examination Survey (KNHANES) from 2016 to 2018 were classified by sex and as smokers/electronic cigarette users (SE) or non-smokers (NS). Data were analyzed using complex sample general linear models.
Results
There were no differences in dietary intake of vitamin A, carotene, or retinol between the SE and NS groups. Adjusted mean serum vitamin A levels were higher in the SE group compared with those in the NS group (0.63 mg/L vs 0.60 mg/L among men; 0.55 mg/L vs 0.51 mg/L among women). Among all participants, urinary cotinine and serum vitamin A levels were positively correlated (R2 = 0.037). However, no correlation was observed in either the SE or NS groups individually. In a model adjusted for age, body mass index, sex, frequency of binge drinking, and dyslipidemia, a stronger correlation was observed (R2 = 0.244).
Conclusion
In Korean adults, urinary cotinine levels were positively associated with serum vitamin A levels. Mean serum vitamin A levels were significantly higher in the SE group compared with the NS group.
Keywords
Introduction
Evidence from several epidemiological studies has consistently suggested that diets rich in fruits and vegetables are associated with reduced risks of chronic diseases such as cancer and heart disease. 1 , 2 However, in our busy modern society, it is difficult for many people to consume three well-prepared meals a day. Nutritional deficiencies can be mitigated through nutritional supplementation to remove reactive oxygen species from the body and protect health. As such, nutritional supplements have become indispensable for many people, and are commonly supplied separately from regular meals and processed foods. Most people believe that vitamins are safe to consume even if their health benefits may be limited. Therefore, dietary supplements are commonly used to prevent cardiovascular disease and cancer, especially in the USA, where consumption of supplements has increased over time. A recent survey found that 77% of the adult population in the USA uses multivitamin/multimineral supplements. 3 According to 2005 data from South Korea, 29.1% of adults aged 20 years or older used dietary supplements; a higher proportion of women (33.0%) than men (23.6%) used supplements, except among those aged 70 years or older. 4 Despite various studies of the cellular and biological functions of vitamins and ongoing discussion of their roles in health and disease, the long-term health impacts of vitamin supplementation remain unknown. 5
Lung cancer is the leading cause of cancer death in the USA and worldwide. 6 The most common cause of lung cancer is smoking tobacco. Risk of lung cancer can be most effectively reduced by stopping smoking. However, among those who are addicted to smoking tobacco or are exposed to lung carcinogens, other strategies for lung cancer prevention are required. Most studies that analyzed serum beta-carotene levels in prospectively collected blood samples found lower levels of beta-carotene in people who subsequently developed lung cancer. 7 Three large-scale clinical trials tested the effects of beta-carotene supplementation on risk of chronic diseases such as cancer. All three trials concluded that beta-carotene provided no protection against lung cancer, and quite unexpectedly, two trials found a higher risk of lung cancer among patients given beta-carotene supplements. 8 No satisfactory explanation for this result has been given.
There is a significant correlation between cigarette use per day and urinary cotinine levels. 9 Therefore, using data from the Korea National Health and Nutrition Examination Survey (KNHANES) from 2016 to 2018, this study aimed to examine correlations between urinary cotinine levels (as a surrogate measure of tobacco consumption) and serum vitamin A levels.
Subjects and methods
Data source and study population
The KNHANES is conducted annually with rolling sampling. Data are based on a complex stratified multistage probability cluster survey of a cross-sectional and nationally representative sample of individuals from the non-institutionalized civilian population of the Republic of Korea. The survey assesses the health and nutritional status of the Korean population and is administered by the Korea Centers for Disease Control and Prevention (KCDC). The KNHANES received approval from the institutional review board of the KCDC (Ethics Committee reference number 2018-01-03-P-A). All participants in the survey provided written informed consent.
This study was based on data from the KNHANES from 2016 to 2018. All participants aged 19 years or older were included unless they met the following exclusion criteria: (i) non-participation in vitamin tests or urine cotinine tests, (ii) diagnosis of disease such as stroke, myocardial infarction, angina, renal failure, liver cirrhosis, thyroid disease, or cancer, (iii) pregnancy; (iv) failure to answer at least one questionnaire, and (v) non-smokers with urinary cotinine level ≥300 ng/mL (Figure 1). Finally, 4445 participants were classified into the smoker/electronic cigarette user (SE) group or the non-smoker (NS) group.

Flow diagram of study participants.
Lifestyle habits
Interviews and health examinations were performed by trained interviewers and medical staff using calibrated equipment and a standardized protocol. The interviewers collected data on demographic characteristics including living situation, current medical conditions (hypertension, diabetes, dyslipidemia, cerebrovascular accidents, myocardial infarction, angina, osteoarthritis, and osteoporosis), socioeconomic status, and educational level. Marital status was classified as married only for those currently living with their spouses; participants who were separated, widowed, or divorced were all classified as unmarried. Educational level was classified as elementary school, middle school, high school, or university graduation as the highest level of education. Household income was categorized into quartiles according to sex and age groups.
Smoking status, alcohol use, and physical activity were investigated through self-administered questionnaires. Smokers were defined as those who have smoked more than 100 cigarettes in their lifetime and currently smoke cigarettes. Electronic cigarette users were defined as non-cigarette smokers who answered ‘yes’ to the question, “Have you used electronic cigarettes in the past 1 month?” The NS group included those who were neither smokers nor electronic cigarette users. Binge drinking was defined as average alcohol consumption of seven or more drinks per day for men and five or more drinks per day for women. Self-rated health was classified as ‘healthy’ for participants who answered ‘very good,’ ‘good,’ or ‘average' on the question, “What do you think of your general health?” Activity restriction was classified based on yes/no responses to the question, “Are you currently restricted in your daily life and social activities because of health problems or physical or mental disorders?”
Height and body weight were measured to the nearest 0.1 kg and 0.1 cm, respectively, while participants were wearing light clothes without shoes. Body mass index (BMI) was calculated as weight in kg divided by the square of height in m. We used the World Health Organization criteria for the Asian population, which define underweight as BMI < 18.5 kg/m2 and obesity as BMI ≥25 kg/m2. 10
Nutritional assessment
A nutritional survey of 24-hour dietary recall was conducted by a team of professional interviewers consisting of nurses, a dietitian, and health science professionals. Daily intake of energy and nutrients was further calculated from reported consumed foods or dietary supplements.
Biochemical analysis
Blood and urine samples were collected after at least 12 hours of fasting and were analyzed at a certified laboratory. Vitamin A and vitamin E levels were measured using an Agilent 1200 high pressure liquid chromatography (HPLC) system (Agilent, Santa Clara, USA). Serum vitamin A and E levels were measured only in one third of all participants. Urinary cotinine levels were measured using an Agilent 1100 HPLC system connected to an API 4000 liquid chromatography-tandem mass spectrometry instrument (AB Sciex, Framingham, MA, USA). According to a previous study, urinary cotinine levels of 0 to 300 ng/mL were observed in non-smokers, levels of 400 to 900 ng/mL were observed in those with passive exposure to tobacco smoke, and levels >1000 ng/mL were observed in active smokers in Korea. 11
Statistical analyses
Because the data from the KNHANES were acquired using a complex sampling design method, variance of cluster sampling (primary sampling units), variance of stratified sampling (k strata), and the individual integrated weights were applied. Categorical variables were analyzed using the Rao-Scott χ2 test and continuous variables were analyzed using complex sample general linear models to assess differences between the SE and NS groups by sex. Complex sample general linear models were used to assess differences in serum vitamin A levels between the two groups in the model after adjusting for smoking, age, frequency of binge drinking, self-rated health, and dyslipidemia (in men) and for smoking, age, education level, household income, and frequency of binge drinking (in women). We measured correlations between urinary cotinine and serum vitamin A levels. All data were analyzed using SPSS version 26 (IBM Corp., Armonk, NY, USA). Values of p < 0.05 were considered statistically significant.
Results
The demographics for the SE and NS groups are shown in Table 1. Totals of 738 men (weighted number 2,586,872) were in the SE group and 1243 men (weighted number 4,117,208) were in the NS group. Totals of 134 women (weighted number 388,177) were in the SE group and 2330 women (weighted number 5,517,944) were in the NS group. Among men, the weighted proportion of participants with dyslipidemia in the SE group (31.0%) was higher than that in the NS group. In addition, mean age (42.24 years) as well as the weighted proportions of participants who self-rated as healthy (83.0%) and having hypertension (24.5%) in the SE group were lower than those in the NS group (p < 0.05). Among women, mean age (38.97 years) and the weighted proportion of married participants (48.9%) were lower in the SE group compared with the NS group (p < 0.05).
General characteristics of the smoker/electronic cigarette user group and the non-smoker group.

p-values are from Rao-Scott χ2 test for categorical variables and complex sample general linear models for continuous variables.
Values are expressed as unweighted counts (weighted %) or means ± standard errors.
n = unweighted sample size; N = weighted sample size.
Dietary intake of vitamin A (µgRAE) = dietary intake of retinol + 1/12 * dietary intake of carotene; RAE, retinol activity equivalents.
Among women, weighted proportions of participants who had graduated from high school and who had mid-high household incomes were higher in the SE group compared with the NS group (47.6% vs 33% and 32.1% vs 30.8%, respectively; p < 0.05). Among men, the weighted proportion of participants who consumed alcohol monthly or less than once a month was lower in the SE group than in the NS group (p < 0.001). Among women, the highest frequency of binge drinking was weekly in the SE group and never in the NS group (p < 0.001).
There were no significant differences in dietary intake of vitamin A, carotene, or retinol or in supplementary intake of vitamin A between the SE and NS groups. There were also no significant differences in the numbers of participants taking vitamin A supplements between the SE and NS groups. Among men, only mean energy intake was higher in the SE group (2523.98 kcal) compared with the NS group (p = 0.008).
Serum vitamin A and E levels and urinary cotinine levels in the SE and NS groups by sex are shown in Table 2.
Comparison of serum vitamin A and E levels and urinary cotinine levels in each group.
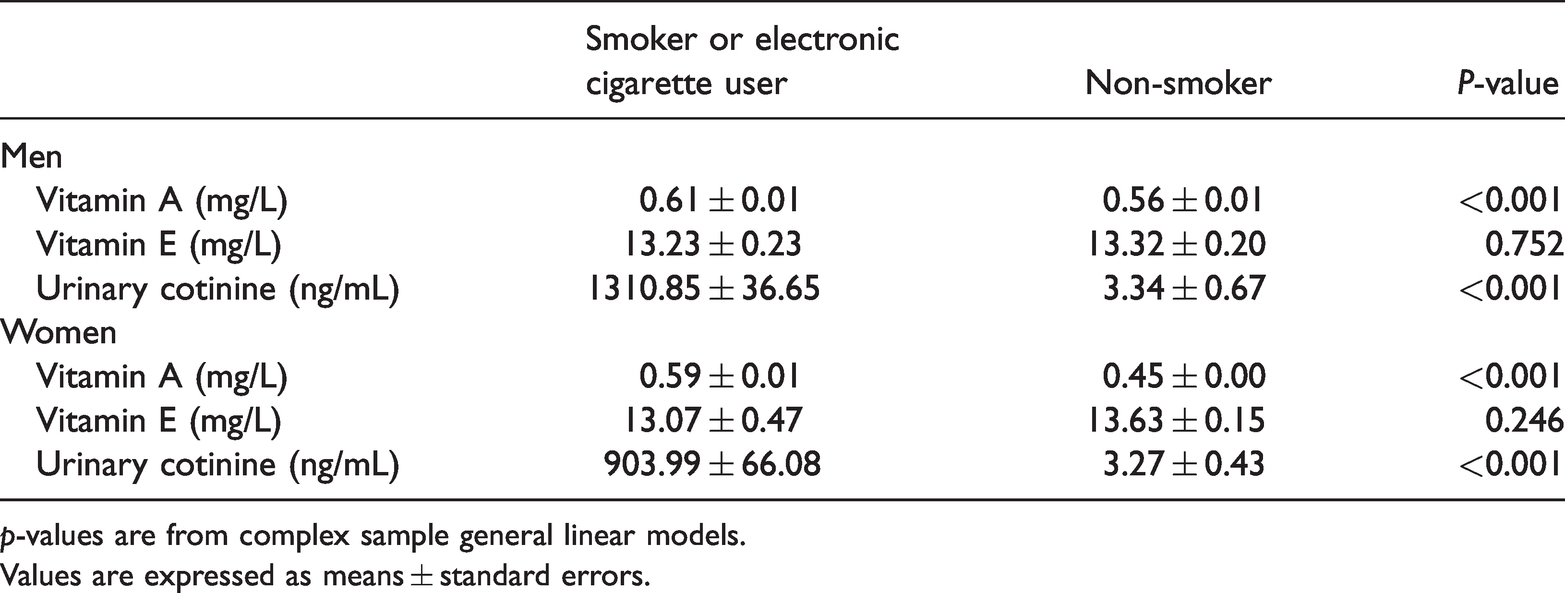
p-values are from complex sample general linear models.
Values are expressed as means ± standard errors.
The mean serum vitamin A and urinary cotinine levels in the SE group were higher than those in the NS group (0.61 mg/L vs 0.56 mg/L and 1310.85 ng/mL vs 3.34 ng/mL among men, respectively; 0.59 mg/L vs 0.45 mg/L and 903.99 ng/mL vs 3.27 ng/mL among women, respectively; p < 0.001).
In a model adjusted for smoking, age, frequency of binge drinking, self-rated health, and dyslipidemia, serum vitamin A levels differed significantly between men in the SE and NS groups (Table 3). The adjusted mean serum vitamin A level was 0.63 ± 0.01 mg/L in the SE group and 0.60 ± 0.01 mg/L in the NS group (R2 = 0.159, p = 0.003)
Analysis of covariance of serum vitamin A levels between the smoker/electronic cigarette user group and the non-smoker group

Among men, R2 = 0.159; the complex sample general linear model was adjusted for smoking, age, frequency of binge drinking, self-rated health, and dyslipidemia. The adjusted mean serum vitamin A level was 0.63±0.01 mg/L in the smoker/electronic cigarette user group and 0.60±0.01 mg/L in the non-smoker group (p=0.003).
Among women, R2 = 0.131; the complex sample general linear model was adjusted for smoking, age, education level, household income, and frequency of binge drinking. The adjusted mean serum vitamin A level was 0.55±0.01 mg/L in the smoker/electronic cigarette user group and 0.51±0.01 mg/L in the non-smoker group (p=0.003).
In a model adjusted for smoking, age, education level, household income, and frequency of binge drinking, serum vitamin A levels differed significantly between women in the SE and NS groups (Table 3). The adjusted mean serum vitamin A level was 0.55 ± 0.01 mg/L in the SE group and 0.51 ± 0.01 mg/L in the NS group (R2 = 0.131, p = 0.003).
Correlation between urinary cotinine and serum vitamin A levels are shown in Figure 2. Among all participants, a weak positive correlation between urinary cotinine and serum vitamin A levels was observed (R2 = 0.037; parameter estimate (standard error), 5.273 × 10−5 (5.313 × 10−6); p < 0.001). The same analysis was performed separately for the SE group and the NS group and showed no correlation between urinary cotinine and serum vitamin A levels in either group.

Correlation between urinary cotinine and serum vitamin A levels. (a) Correlation among all eligible participants: R2 = 0.037; parameter estimate (standard error), 5.273 × 10−5 (5.313 × 10−6); p < 0.001. *R2 = 0.244; parameter estimate (standard error), 1.473 × 10−5 (4.981 × 10−6); *p = 0.003. *Adjusted for age, body mass index, sex, frequency of binge drinking, and dyslipidemia. (b) Correlation in the smoker or electronic cigarette user group: R2 = 0.001; parameter estimate (standard error), 8.254 × 10−6 (8.821 × 10−6); p = 0.350. (c) Correlation in the non-smoker group: R2 = 0.001; parameter estimate (standard error), 0.000 (0.000); p = 0.167.
Discussion
The total number of cancer cases in Korea in 2017 was 232,255, representing an increase of 1019 cases (0.4%) over the previous year. The incidence of cancer in Korea in 2017 was 264.4 cases per 100,000 individuals, lower than the Organization for Economic Cooperation and Development average of 301.1 cases per 100,000 individuals. Lung cancer incidence ranked second among men and fourth among women. 12
A total of 1,762,450 new cancer cases and 606,880 deaths from cancer were expected to occur in the USA in 2019. In the USA, lung cancer is the second most common cancer in both men and women and is also the leading cause of cancer-related death. Although smoking tobacco is the major etiological factor accounting for 80% to 90% of all lung cancer diagnoses, numerous risk factors have been identified as casually associated with lung cancer. 13
Increased consumption of vegetables, fruits, fish, and soy products may reduce the risk of lung cancer, while consumption of red meat and processed foods can increase the risk. 14 However, almost all trials of nutritional supplementation, including with vitamin A, vitamin E, vitamin C, folic acid, selenium, and carotenoids, have failed to demonstrate effectiveness in preventing lung cancer. 15
Three large-scale clinical trials have been conducted of beta-carotene supplementation: (i) the Alpha Tocopherol Beta Carotene [ATBC] trial, conducted among 29,133 Finnish men who were heavy smokers; (ii) the Beta-Carotene and Retinol Efficacy Trial [CARET], conducted among 18,314 current and recent ex-smokers (men and women) and asbestos workers (men); and (iii) the Physician's Health Study (PHS), conducted among 22,071 US male physicians, approximately half of whom were current smokers.16–18
In the ATBC trial, participants received alpha-tocopherol (50 mg per day) alone, beta-carotene (20 mg per day) alone, both alpha-tocopherol and beta-carotene, or placebo. In the CARET, participants received a combination of 30 mg of beta-carotene and 25,000 international units of retinol (vitamin A) per day or placebo. The PHS was a placebo-controlled trial of beta-carotene (50 mg administered on alternate days). The median duration of follow-up of the ATBC trial, the CARET, and the PHS were 6.1, 4, and 12 years, respectively.
Results from the ATBC trial and the CARET revealed that individuals at high risk of developing lung cancer (heavy smokers and asbestos workers) who received high-dose supplemental beta-carotene had increased relative risks (18%–23%) of developing lung cancer than participants who did not receive beta-carotene supplements. The trial with the longest duration of follow-up, the PHS, found that neither smokers nor non-smokers had any change in their relative risks of lung cancer associated with supplemental beta-carotene. These results were quite unexpected. Several authors concluded from these beta-carotene trials that the protective effects of antioxidants against chronic diseases had been overhyped. Although beta-carotene may or may not be an antioxidant; it certainly differs in many aspects from the prototypical antioxidant, vitamin E. 8 In addition, high-dose beta-carotene supplementation appears to increase the risk of lung cancer among current smokers.19–21
The SU.VI.MAX Study showed that after 7.5 years, low dose antioxidant supplementation (including 6 mg of beta-carotene) lowered overall cancer incidence and all-cause mortality in men, but not in women. Dietary supplementation may be effective in men only because of their lower baseline levels of beta-carotene. 22 The beneficial effects of antioxidant supplementation in men disappeared at 5-year post-intervention follow-up. 23
Agreements and disagreements between studies may be caused by differences in design (e.g., observational or interventional) or differences in participants’ serum vitamin A levels. For adults over 18 years of age, the reference values for serum vitamin A are 32.5 to 78.0 µg/dL. 24 In the current study, participants’ vitamin A levels were almost normal. The mean serum vitamin A level in the SE group was higher than that in the NS group (63 µg/dL vs 60 µg/dL among men; 55 µg/dL vs 51 µg/dL among women; p = 0.003), even though there were no differences in vitamin A intake (dietary and supplementary) between the two groups or between men and women. According to a previous study, serum levels of vitamin A in men are higher than those in women. There were no significant differences between the sexes in serum carotene or vitamin E levels. The previous study also found that serum levels of vitamin A were higher in men than in women, 25 so in the current study data were analyzed by gender. Men had higher energy intakes than women and energy intake among men in the SE group was higher than that among men in the NS group. However, this difference in energy intake did not have a significant effect on serum vitamin A levels. Thus, providing high concentrations of vitamin A to smokers who have normal vitamin A levels may be harmful.
Among all participants, serum vitamin A levels increased slightly as urinary cotinine levels increased. Thus, serum vitamin A levels may have increased depending on the number of cigarettes smoked per day. However, in both the SE and NS groups individually, there was no correlation between urinary cotinine levels and serum vitamin A levels. This lack of correlation could have several explanations. First, there were some active smokers with urinary cotinine levels < 300 ng/mL in the SE group. Second, second-hand smoke may increase urinary cotinine levels. Third, the smoking status of participants was investigated through a self-administered questionnaire.
To evaluate potential selection bias, we compared the general characteristics of non-participants aged 19 years or older (e.g., individuals who were excluded because of the absence of dietary data, serum vitamin A and E levels, and urinary cotinine levels). The reason for the large difference in the number of potential participants in the original database and the study sample size was that only one third of participants’ serum vitamin A and E levels were measured. The general characteristics of the SE and the NS group among non-participants were similar to those of participants included in this study. Among non-participants, 1814 individuals (weighted number 5,749,427) were in the SE group and 9537 individuals (weighted number 23,203,941) were in the NS group. There were significant differences in mean age and the weighted proportions of individuals according to sex and BMI between the SE group and NS group (44.33 years old vs 49.66 years old, 86.1% vs 39.0%, and 24.25% vs 23.88%, respectively; p < 0.001). Additionally, there were significant differences in the frequency of binge drinking, self-rated health, and dyslipidemia between the SE and NS groups of non-participants. Mean energy intake also showed significant differences between the SE and NS groups of non-participants (2377 kcal vs 1907 kcal, p < 0.001). There were no significant differences in dietary intake of vitamin A, carotene, or retinol or in supplementary intake of vitamin A between the SE and NS groups of non-participants. There were no significant differences in the numbers of individuals taking supplemental vitamin A between the SE and NS groups of non-participants.
Because vitamin A is a fat-soluble vitamin and potentially toxic at high concentrations, administration of high doses of vitamin A may carry safety risks. Therefore, it may be better for individuals to supplement their diets with a small amount of vitamin A after taking the nutritional status survey.
As mentioned above, vitamin A supplementation can have negative effects when levels are already high. In the SU.VI.MAX study, a group of male participants could have had positive effects because they consumed a small amount of beta-carotene with other micronutrients or they had baseline levels of beta-carotene around 24.5 µg/dL, lower than the reference value. 22
Together, the data show that smoking does not cause a decrease in vitamin A levels, but instead slightly increases its levels. The correct way to provide supplemental vitamin A to individuals, especially smokers, is to either provide a sufficient dose to those with low baseline levels until a standard level is reached, or to provide a small dose with other micronutrients to those who have normal vitamin A levels.
A limitation of this study was uncertainty in the degree that urinary cotinine levels could reflect amount of smoking. A prior study showed that the number of cigarettes smoked per day was associated with total urinary cotinine, but not in a linear fashion. When a high level of smoking was reported (e.g., >40–45 cigarettes per day), urinary cotinine levels did not increase consistently or to the same degree as for lower doses. 9 In this study, almost all smokers smoked ≤40 cigarettes a day, except for one individual who smoked 55 cigarettes a day. Therefore, urinary cotinine levels were probably reflective of the amount of smoking. Additional limitations of this study were that dietary intake was recorded using only a single 24-hour recall survey and its cross-sectional design. Although the 24-hour recall method may be inaccurate, it enabled comparison of serum vitamin A and urinary cotinine levels. To increase accuracy, professional interviewers visited participants’ homes and provided proper management. Despite these limitations, this study was meaningful as a large-scale study of the Korean population.
Conclusion
As urinary cotinine levels increased, serum vitamin A levels also increased. Hence, increased serum vitamin A levels depend on the number of cigarettes smoked per day. Mean serum vitamin A levels in smokers were higher than in non-smokers. Therefore, vitamin A or beta-carotene supplementation is not needed in smokers and smoking does not result in decreased vitamin A levels in serum.
Footnotes
Acknowledgment
I express my sincere thanks to Tae Hyek Yim (South Baylo University) for correcting the text of the manuscript.
Declaration of conflicting interest
The author declares that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.