
Abstract
This article presents a study on the care provided by 11 men from different ethnic, health, and socioeconomic backgrounds to two indigenous Rarámuri males with ankylosing spondylitis. This chronic muscular and bone disease is known to evolve progressively, causing disability and immense suffering to the affected individual. Through anthropological research involving ethnographic description and interviews conducted in an urban setting of the City of Chihuahua in the state of Chihuahua, caring practices performed by men that contest prior assumptions about how men relate to each other in relation to their health and masculinity were encountered. To interpret findings, a “caring of the self” framework, along with elements of the discussion of personhood and masculinities, was used; this led to an analysis made through the elaboration of meaningful coding of patterns of caring practices.
The patterns identified in the ethnographic data were organized into four groups, all of which represented caring practices performed by these men. The first three groups involve access to food, money, and infrastructure goods, which have a material nature that holds a positive relation to the well-being of the two Rarámuri males in regard to the implications of their disease. The last group is unique in that it pertains to circumstantial factors that required improvisations in the forms of favors exchanged by these males that also positively related to their well-being
Impact of Ankylosing Spondylitis
Ankylosing spondylitis (AS) is a chronic inflammatory, painful, and disabling rheumatic disease that affects the spinal, sacroiliac, and lower limb joints and attachments of tendons and ligaments to the bone. It is linked to genetic factors (HLA-B27, ERAP2, IL-23) and predominantly affects young men and less frequently women (Braun & Sieper, 2007; Burgos-Vargas et al., 2008). While current treatment offers a better health-related quality of life, its efficacy is limited due to reduced access and inadequate adherence to therapy (Braun & Sieper, 2007). General AS symptoms include progressive loss of mobility, morning body stiffness, particularly in the back, hips, and shoulders. Usually, back pain occurs at night, disrupting sleep. Aside from the fact that chronic diseases affect people during their productive years, limiting their earning potential, as treatments tend to be expensive, they further exacerbate the financial situation of those affected and their primary caretakers (Mould-Quevedo et al., 2008; Rodríguez-Amado et al., 2016).
Chronic diseases undermine general traits of hegemonic masculinity, such as strength and independence (Gibbs, 2005), mainly when they cause disability. Masculinity and disability are traditionally considered to conflict (Shuttleworth, Wedgwood, & Wilson, 2012). This conflict usually stems from the affected individual’s outward social manifestations and in response to hegemonic masculinity as a perception (Madsen, Jensen, & Esbensen, 2015). Just like masculinities, disability is a condition better understood when examined at its intersection with gender, class, and ethnicity (Shuttleworth, Wedgwood, & Wilson, 2012).
Masculinities
Gender is a social pattern, both a product and a producer of history (Connell, 2005). Its practices are onto-formative because they constitute a social reality that is dynamic through time. Gendered relations are a way in which society organizes itself and people’s personal lives inserted within societies (Montejo, 2005). It also refers to attributes and functions that go way beyond the biological and reproductive aspects of human life, but that are linked to sexual differences (de Keijzer, 2001). It starts as a socializing process when people are infants, and it never stops throughout life (Lozoya, 1998). Both masculinity and femininity should be situated in a world of social agency and configuration of practice within a certain gender relations system (Connell, 2005). Men both engender and are engendered by other men (Gutman, 1998).
Men do not just act on one particular pattern of masculinity; this is because masculinities are not coherent (Connell, 2005). They are relational and therefore cannot be understood on their own but rather concerning other social patterns such as division of labor, politics, or health. There are broader structural factors that have a changing influence in masculinities, such as the labor force, migration, and salary (de Keijzer, 2001); on a personal level, illness affects masculinities too.
Care of the Self
The “care of the self” (Foucault, 2002) refers to a relationship and a glance toward oneself, the others, and one’s surroundings; this becomes an attitude toward the world that allows the person to become responsible for itself continually. This attitude is conditioned by both the masculine and the feminine symbolic dimensions (Garcés & Giraldo, 2013).
The care of the self allows an understanding of how men relate to other persons (Figueroa-Perea, 2015), mainly when the nature of those relationships refer to caring and solidarity (Garcés & Giraldo, 2013). For Muñoz (2006, 2009, 2013), the care of the self-privileges the person’s experience in its sociocultural context on an everyday life basis, where human interactions that involve caring are directly related to the care of the self, which is a conceptual tool more general than caring practices. If one is to speak about caring practices between men, one is inevitably speaking of the caring of the self as a broader category. It also allows them to understand how meaning construction is carried through caring practices, which are observable by the researcher, and reflect a person’s ethics and their relation to gender.
Male Caring Practices
In the context of this analysis, care is defined as “an intervention and style of intervening and interaction between people and between people and materialities” (Nissen, 2017, p. 552). Nissen further noted that caring is an “open-ended” and an “interactive process.” Caring practices conform to the patterns of masculinity. To further develop the theoretical characteristics of caring practices, certain elements mentioned on Marcel Mauss’s “Essay on the gift” (1979) were taken into consideration. The essay emphasizes how the interaction between humans means circulation and flux of material and symbolic goods. These certain elements in the essay can be linked to the ethnographic data and allow for a better interpretation of the illness. Every caring practice has an orientation, meaning it is directed at someone, be it oneself or another person; that other person may or may not have the same characteristics as the person providing the care. A caring practice may be orientated to someone with different age, ethnicity, income, or a “social rank” in general (for example, people with different hierarchal positions on a kinship system; Mauss, 1979). Also, every caring practice involves the distribution and circulation of material and symbolic goods (Mauss, 1979)—from food and shelter to honor and prestige. The gift system, just as much as the caring practices, links people together by producing social relations (referred by Mauss as “associations” [1979, p. 189] such as friendship or kinship [Mauss, 1979]); this is referred in the current paper as co-implication. The orientation, distribution, and circulation involved in caring practices go far beyond a commercial purpose (Mauss, 1979). The co-implication is but a cause and consequence of those practices. It is therefore established that these practices have a moral purpose directly linked to the care of the self as a broader term than caring practices; because when it involves more than one person, it also means a recognition of the other and from the other.
The Male Person as a Multidimensional Being
Masculinity is conditional and part of processual personhood (Lipset, 2008) related to cultural symbolic frameworks, known as Structures of Belonging (Duch, 2002). The male person is a “concrete center of actions, individuated through space and time” (Scheler, 1957, p. 91); this center refers to an embodied being because it has “organic sensations, affective sentiments and sensations of pain and pleasure” (Scheler, 1957, p. 54).
One of the leading causes of conflict with a person with a progressive disability is the fact that their body suffers pain and seems to hold a failed relationship with space. This conflict, a primary constituent of both the condition of disability and the illness in general, can be surpassed by the persons involved in the illness. It can be accomplished through a person’s processual capacity and their ability to make new sense of the world as they experience reality collectively—while taking care of themselves and others through caring practices—which holds a direct relationship with the caring of the self.
Male caring practices can be understood through the relationship between a male person and their masculinity. This relationship is mediated by a multidimensionality (Cruz, 2015); it involves among an infinite number of things, locality, ethnicity, and health. Multidimensionality makes masculinity conditional, rather than intrinsic (Lipset, 2008, p. 228), where both “surprise” and “improvisation” (Cruz, 2018, p. 124) accompany a male person’s social performance through prescribed gender expectations.
The elements mentioned above that referred the multidimensionality and relationality between a male person and their ethnicity, locality, disability, among others, may situate a person on the margin, in regard to dominant and hegemonic masculinity. Marginality is caused by factors such as class, ethnicity, and religion, which determine the distribution of masculinities (Connell, 2005). For example, ethnicity is linked to historical poverty and general marginalization on a social and symbolic level (Iturriaga, 2011).
Marginal means to be outside of the center and at the edge; persons may be marginalized due to caste, ethnicity, or gender position (Ecks & Sax, 2005). Ethnicity as a constituent of the person’s marginality infers that marginality is relational; “this relationality has important [and negative] effects concerning health” (Ecks & Sax, 2005, p. 208). This relationality extends to masculinity because it influences the particular forms that different representations of masculinity take form on a given context (Cruz, 2018).
Justification
The impact of chronic and degenerative rheumatic diseases has only been recently studied in indigenous populations such as the Rarámuri. The study of illness as a sociocultural drama could shed new light from a perspective of masculinities in relation to ethnicity and disability, given that “information from Latin America is particularly scarce” (Peláez-Ballestas et al., 2011, p. 3). These would all be necessary steps toward a better public and universal health care.
Understanding males’ caring practices, along with their aforementioned theoretical characteristics as well as the multidimensionality (ethnicity-masculinity-health) concerning other forms of the identity of their personhood allows us to understand the relationship between masculinity and health in a more profound way.
Objective
The objective is to describe and analyze the caring of the self through the observation and description of male caring practices related to their masculinity. The focus has been directed toward two sets of relationships between men, where caring practices were orientated toward two Rarámuri men with disability caused by AS.
Methods
Participants
The primary researcher interacted with 15 individuals, 11 of whom were males. The ages of the participants in this study range from 20 to 40 years of age. To better exemplify general caring practices, in the analysis, the focus was narrowed to the practices involving male individuals divided into two sets of relationships. These two sets, respectively, focused on Fermín and Pato, the two Rarámuri males affected by AS. All participants in this study came from different ethnic backgrounds and were residents of the city of Chihuahua. Two sets of human relationships were analyzed through anthropological, health, and masculinity perspectives, emphasizing on the interaction on a day-to-day basis in public and private places. Some of the inferences made on this article were not solely based on people’s statements, but rather on their actions observed during the anthropological research. Their doctor, who confirmed part of the two sets, was an important facilitator.
All these persons performed male caregiving practices that were orientated toward two Rarámuri males from marginal areas of the city, who were diagnosed with AS. These two persons lived in neighborhoods characterized by deficient access to water and public transportation, lack of concrete on the roads, low household income, and high crime rates.
Some of the individuals that comprised the overall network of the two Rarámuris’ relations were mentioned during the interviews but did not interact with the researcher directly. The two Rarámuri males with AS had only met once briefly in their lifetime. These people shared public and private spaces with them and are mentioned in the Results section. In general, it can be stated that it was the people they worked with or the people that occupied the same spaces as them; in some cases, it was even their relatives or their doctor. They were taken into account when jotting down field notes, which were elaborated based on observations and conversations.
The researcher doing fieldwork observed and participated in some of the individual’s life in public and private spaces; the data also included personal descriptions and reflections during social interactions through field notes. The workplace, homes, and especially public spaces such as streets or parks are where these descriptions took place.
Methodology
The research was conducted from 2014 to 2016. It is a product of anthropological research conducted in the city of Chihuahua, which belongs to a State also named Chihuahua in Mexico—one of the many border states with the USA, where the manufacturing industry has played an essential role in the shaping of the city during the last 20 years. Study settings were mainly located in the south side of the city and included public spaces such as sidewalks and parks, as well as houses of the two main participants, which were located on the city periphery.
This is a qualitative study with an ethnographic approach of descriptions of social situations involving people and places (Goffman, 1956, 1967, 2001). The aim was to achieve an exegesis of aspects of culture regarding the illness that is not always explicit, such as gender relations. In these social situations, people’s behaviors can be considered as performance (Goffman, 2001) as they interact face-to-face with other individuals who perform specific roles as well. Ethnographic data can be collected from sources other than verbal communication and may include recording body postures, facial expressions, and the dress code of those involved. Also, material aspects of culture, such as urban settings or personal property, were taken into account (Goffman, 1967).
Research Strategy
Ethnographic data were collected through descriptions of oral material and descriptions of human interactions, some of whom involved the principal researcher. Participant and nonparticipant observations were adopted as a technique; field notes were written after that. Oral material was collected from casual conversations and semistructured interviews with and without a recorder under controlled environments. Communication was conducted in Spanish, since all the participants spoke it fluently. Thirty unrecorded and five recorded interviews were conducted with these individuals.
The first point of interaction came through their rheumatologist, extending from there to other people living in the city at that time. The term “interlocutor” is used instead of “informant” because it is more accurate since it recognizes the person participating in the information exchange as a protagonist of its own story, someone who will be transformed by the mere interaction with the researcher, who is also transformed by the interaction.
To better understand the multidimensionality of their personhood, the interview questions and prompts focused on the familial, labor, economic, ethical, sexual, and religious aspects, as well as the illness history and general issues.
Study data were also sourced from newspapers and official statistics on Chihuahua’s population; this was used to observe social patterns on a grander scale that could later be linked to the field notes and the content of the interviews
Context of the Study
This study is the product of a project named “Prevalence and Medical Anthropology of Musculoskeletal Illnesses and Rheumatic Diseases in Latin-American Indigenous Peoples,” which provided an academic, doctor, and patient network of people with whom the research team worked.
All of the fieldwork and interviews were carried in the city of Chihuahua, where unemployment is relatively low and public health services are easily accessible. The manufacturing industry has played an essential role in the shaping of the city during the last 20 years. Chihuahua City’s population has grown to more than 800,000 people, 11% of whom identify as Rarámuri, and only about 6,000 speak a Mexican language rather than Spanish (Instituto Nacional de Estadística y Geografía [INEGI], 2010; Figure 1).

This map represents the Statef of Chihuahua, Mexico (modified by the authors from INEGI, 2010).
The Rarámuri Context
The multiple ethnicities in Mexico have historically been among the poorest social groups in the nation and with limited access to health care. Their socioeconomic condition rather than their ethnicity allows them to access health care through the government-funded “Seguro Popular” (Leyva-Flores, Servan-Mori, Infante-Xibille, Pelcastre-Villafuerte, & Gonzalez, 2014). Even as the program’s coverage has increased tremendously in the past decade, this program has been known for having difficulties and deficiencies when it comes to diagnosing and attending musculoskeletal diseases effectively (Gutiérrez & Hernández-Ávila, 2013; Peláez-Ballestas et al., 2011).
Rarámuri people and other groups residing in the state of Chihuahua are the poorest among the general population. This group has been historically and geographically associated with “La Sierra Tarahumara”—a portion of the “Sierra Madre Occidental” (Rodríguez, 1982) in the State of Chihuahua, in northern Mexico. Many Rarámuri choose to migrate to other cities across Mexico as well as to the United States. Once at their destination, they coexist with many other ethnicities and masculinities. In terms of their participation in the economy, the Rarámuri people are known for performing physically demanding jobs in both urban and rural areas. In the city, they tend to work as housemaids or construction workers (Acuña, 2006; Heras, 2007; Pintado, 1995; Rodríguez, 1982). Even though they are people who share a common past and a culture overall, they are a culturally diverse group (Martínez, 2008).
Analysis
Once ethnographic data were collected, information was classified, categorized, and confronted (Coffey & Atkinson, 2003). These steps were all necessary to generate meaningful analyzable units; once these units were created, the original research questions were improved and multiplied, allowing new levels of interpretation, such as the identification of links between theory and data (Coffey & Atkinson, 2003), which were established, mainly concerning caring practices between males and how they relate to caring of the self.
The process of coding is made through the use of reason and logic; tracing logic (and imaginary) relationships within the analyzable units, which come from a social and cultural origin, which makes the research overall of qualitative nature (Coffey & Atkinson, 2003). This coding gives way to a “meta-narrative,” which turns coded data into “significant data” (Coffey & Atkinson, 2003, p. 55), which in turn makes information more accessible for interested audiences that relate to it as a final product. This product is a discursive and written corpus (Pérez-Taylor, 2000). We must mention that there were circumstantial aspects that were not necessarily planned, but due to the spontaneity of social situations, they came to be and proved fruitful when it came to findings that better explained the illness with the two people. The organized sets of relationships were coded this way and narrowed to 11 participants to better exemplify the caring practices poignantly.
Ethical Aspects
This study was approved by the local ethical committee. A complete explanation of the objective, strategy, and data confidentiality of the study was given to participants. Those interviewed with a recorder gave their consent to participate and manifested it in the recording. Overall consent was granted by their governor; no written consent was deemed necessary according to the opinion of the governors for Rarámuri affairs.
Results
The following male caring practices come from two sets of masculine relations that involved 10 persons. The patterns of masculinities observed did not focus on the Rarámuris’ ethnicity, as many of the people they related to were not Rarámuri. What the male persons had in common were space, circumstances, and gendered relations. The persons they interacted with included neighbors, relatives, co-workers, and other members of their locality, and had higher income and better health than the two Rarámuri interlocutors (Figure 2).
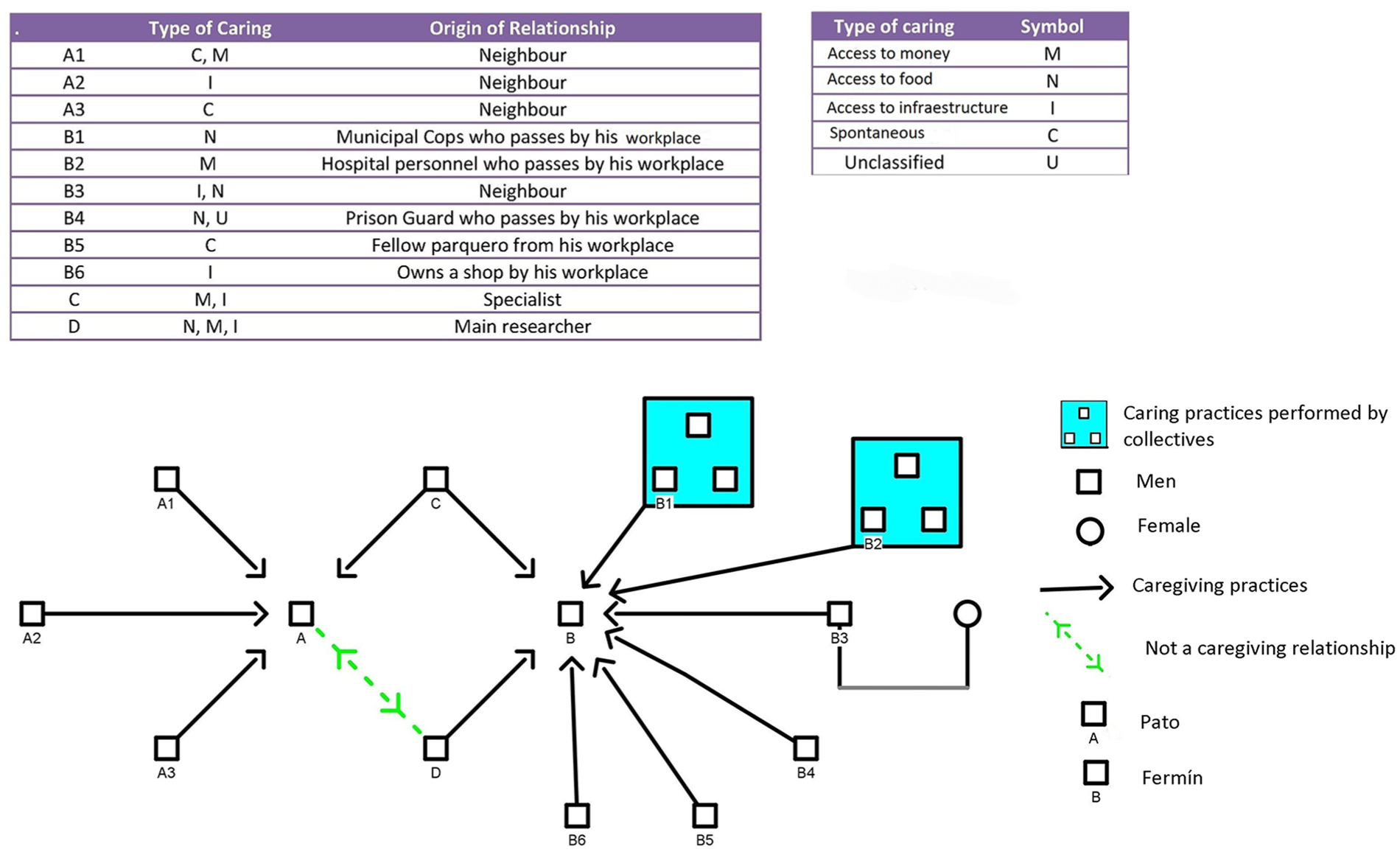
Patterns of caring practices through two sets of relationships among men.
Before discussing the types of caring practices (access to money, access to food, access to infrastructure, and spontaneous caring practices), Fermín and Pato’s illness stories shall be presented in the form of pilgrimage, pointing out their similarities and differences. The sets of human relationships used to describe the male caring practices are also present in their pilgrimage stories. The two Rarámuri males share common structural factors such as gender and ethnicity, as well as their disability caused by AS.
Pilgrimage Stories
Pilgrimage is a temporal–space trajectory triggered by the event of the disease and involves the perception of the disease as a never-ending process (Peláez-Ballestas et al., 2011). It is a process of living with a chronic disease such as AS and continuously trying to make sense of it. It is a good way to disclose the study findings because it focuses on the affected individuals and their experience of illness as a sociocultural drama. The process extends to the supporting human network (such as the two sets), as well as spirituality and future expectations. Pilgrimage can be divided into two stages: before the diagnosis and after it. Proper diagnosis of a disease such as AS takes about a decade from the appearance of symptoms due to unpreparedness on behalf of medical personnel to promptly recognize it (Maksymowych, 2004). Pato and Fermín were not exceptions to this late diagnosis. Both of them experience daily inflammation of their knees and ankle joints as well as general pain in their feet.
Fermín is 34 years old, while Pato is only 19. Clinically speaking, they both started having acute symptoms before turning 15 with an “unfortunate clinical course,” according to their doctor. Their specialist met them in a public hospital that, while “underfunded” by his assessment, nonetheless provides primary care to thousands of people who would not receive it otherwise. Since the hospital is located in the capital city, many people of low income, like Pato and Fermín, have to travel or permanently migrate to the local area in order to access treatment.
The cost of the pharmaceutical treatment for AS is estimated at around USD 1,080 per month, which neither Pato nor Fermín can afford since they both earn less than USD 300 monthly. Their doctor has managed to get them treatment for free by participating in clinical trials held by private companies. The National Commission for the Indigenous People’s Development is a federal institution that promotes the human rights of indigenous groups across Mexico; this institution covers part of Pato’s treatment. Searching for better health care and access to treatment, both men migrated from a small town called Témoris, the main town in the Guazapares municipality. This town is located in a remote area in the La Sierra Tarahumara (Figure 1).
According to their doctor, rare diseases like AS are not appropriately diagnosed in remote and rural areas, where health centers lack relevant specialists. This could be avoided if there was better coordination between health-care centers in remote areas and the hospitals in metropolitan areas. At the time of the present study, both Pato and Fermín were struggling to complete their high school education. Despite identifying as Catholics, neither man attended mass, prayed, or participated in any religious rituals.
They both reside in impoverished areas of the city. They did not live in traditional Rarámuri neighborhoods or Rarámuri shelters, where most members of this ethnic group live. The city hall has granted them both with a card that officially recognizes them as disabled.
Fermín had a municipal card, which legally allowed him to work as a “parquero”—a job that consists of assisting drivers with parking and watching over their cars until they return. Fermín has no benefits, such as insurance or even access to a bathroom or resting areas. Therefore, the consequences of his illness and poverty are exacerbated further. His wife and children no longer lived with him, and he had no contact with them at the time of the study. Although they used to look after him, according to Fermín, they had abandoned him. Fermín’s job environment allowed him to have social contact with other men whose life circumstances were often better than his own. He had formed long-lasting relationships with some of those men, as he would see them regularly in his workplace. This contact generated trust that opened the way for Fermin to establish help-seeking and caregiving bonds.
On the other hand, Pato lived with a family, naming his aunt as his primary protector and caregiver. That person was, in fact, not his aunt, but did take care of him, claiming to have “picked him up” from the street. Pato lived with her and her husband and children. He had some friends from school, but his central friendships involved neighbors, who were men of all ages living on a low income, studying at public high schools, or taking part in the economy as workers in the manufacturing industry or other poorly paid jobs.
According to their doctor, Pato’s situation will not worsen due to earlier treatment, while Fermín will be utterly dependent on others in around 5 years when his progressive disability reaches a critical point. Fermín’s treatment also involves medicine for his emotional problems, which Pato claims not to suffer. Pato’s earlier diagnosis and better family support allowed him to receive help from a nongovernment organization that specializes in assisting underprivileged children with disabilities and helps them with accessing medical treatment. Although not completely free of charge, the option this brings does improve the future of the children under their care through proper rehabilitation and surgery. The treatments that individuals with a disability, autism, or cancer receive are funded through donations and from the fees charged to the families of the diseased.
Both Fermín and Pato reflect a severe problem regarding the proper identification of rare musculoskeletal diseases in marginalized men who live in remote areas of Mexico. Their doctor explicated: The [public] health structure [supposed to provide treatment] did not respond appropriately to the early stages of their disease and their needs. Fermin and Pato had a delayed diagnosis, which had an evident [impact]. There was a delay. The principal researcher met Fermin after he had his [hip] surgery, by then many years had been lost in both of their cases. Surgery is a common situation for AS patients. Interestingly, they [the healthcare system] take much time to diagnose them even though they [patients] generally seek help very early.
These marginalizing issues noted above are due to the inefficiency in the health-care system, which is supposed to be universal. This may be related to the fact that it is usually inexperienced young doctors that offer public access to health care in remote areas.
Patterns of Caring Practices Between Men
Through the analysis of patterns identified in the ethnographic data, caring practices performed by these men were classified into four groups. Three of these groups pertain to the characteristics of caring practices that involve goods (monetary, nutritious, and infrastructural) provided by fellow men to both individuals with AS. The last group is unique in that it pertains to circumstantial factors that required improvisations in the forms of favors exchanged by these males that also positively related to their well-being. To exemplify some of these practices better, certain parts from the field notes and interviews will be included. These caring practices have been organized into four groups: access to food, access to money, and access to infrastructure, and a final one regarding circumstantial caring practices.
Access to Food
The scarcity of food was particularly problematic for Fermín, as he lacked familial support. On many days, he would spend two-thirds of his income on the food he bought in the street. Most of this food was not nutritious or even sufficient. He was therefore marginalized due to his limited access to nutrition.
On one occasion, the municipal police officers handed a plate with beef and broccoli to Fermín; they just suddenly approached him from their car and handed him the plate, as it can be observed in the following extract from the ethnographic fieldnotes taken on July 5, 2015: A lady wearing a white robe descended from a BMW car and gave Fermin a plastic dish with papaya and some condiments for it, Fermín said: “Look at what they brought for us.” It was during that moment when he mentioned that the other day, some male “officers” gave him some “mashed potato and little trees.” I asked him what he meant by “little trees”; after some discussion, it was concluded that he meant broccoli.
Realizing that Fermín spent most of his income on food bought on the streets, the principal researcher helped him to devise a plan that involved three men other than Fermín. It implicated many types of caring practices through masculine relationships that go beyond the one-to-one bonds. The first step was to get both a stove and a refrigerator, as this would allow Fermín to both cook and store food and would save him much money. Through a monetary donation by the doctor to buy a stove and a municipally donated refrigerator, both objects were obtained and delivered to his home through the vehicle assistance of the principal researcher, who was also male. The main goal for everybody was to allow Fermin to have better access to food by owning both a stove and a refrigerator to store that food. Since the stove needed a gas source, a gas tank was also bought and installed with the help of his neighbor, who assisted Fermín as it can be observed in the following extract from the ethnographic field notes taken on July 29, 2015: He then told me about his neighbor, the one that works for the train company. He usually travels between the cities of Juárez and Torreón [832 km between each city]. His house is next door and in a better condition than Fermin’s. He also owns a vehicle. He gave him a reflective vest he uses for work. He was the one who helped him install certain things needed for both the bathroom and the stove in the kitchen.
Access to Money
Money plays a role during illness, mainly because having adequate financial resources facilitates wellbeing. As both Fermín and Pato lacked money, this imposed severe limitations in their lives. Since money means access to many things, its scarcity limited possibilities related to food, transportation, medicine, leisure activities, and even status on a symbolic level.
Pato could not go out at night with his friends, as he was unable to pay for his drinks or transportation. One of his neighbors would thus often provide both. They would go out in groups of three or more, sometimes accompanied by women as it can be observed in the following extract from the ethnographic field notes taken on May 27, 2016: He told me that he once went to a bar [it appears as if it was a strip club] with some male friends, who paid for him to have a private lap dance, he referred the dance as merely a “privado.”
It was usual for Fermín to ask other men that passed by his workplace for money. He claimed to have borrowed money from his specialist on more than one occasion, which he never really seemed to pay back. Given that the treatment for AS is expensive, especially for people with Fermín’s and Pato’s incomes, the doctor also helped by searching for experimental treatments they would benefit from without having to pay.
Regarding how he tends to ask for money to other men, Fermin shared on a recorded interview in January 2016 that: There is the physician, the male nurses, men that work in the hospital, [his friend] Joe; they lend me money, and I never give it back [laughs]. I ask them if they have any money on them, if they do, they lend it. If they do not, well, they do not then. I don’t ask for much, a hundred or two hundred pesos [equivalent to USD 5 -10].
Interestingly, asking women for money did not seem right to either man; while as it seemed acceptable between fellow men in the Mexican context.
Access to Infrastructure
Both Pato’s and Fermín’s well-being depended on access to infrastructure that would allow them to rest, recover, eat, go to the bathroom, store their medicine, and spend time freely. While Pato’s family ties facilitated most of that for him, he nonetheless relied on a male neighbor that would let him hang out in his home and play guitar, eventually selling him one for a reasonably low price.
On the other hand, Fermín’s use of his relationships with other males further exemplifies what is described here as the provision of infrastructure and other goods. Before obtaining the previously mentioned refrigerator, he did not have a place to store his medicines that required refrigeration. To help him overcome this issue, the same male neighbor that eventually set up his stove would let him keep the medicine in his refrigerator. As we can see on this extract from July 23, 2015, the need for a refrigerator would not only allow him to keep his own medicine, it could also allow him to eat healthier food and lower his spending as mentioned above.
Fermin told me that he went home at 19:30hs yesterday. He said that in total he earned sixty pesos [equivalent to USD 3], and that is only because a woman decided to pay him fifty pesos [equivalent to USD 2.5] for watching over her car. He told that he had “Ruffles [chips] and juice [ a juice box]” for dinner. After Fermin finished the two burritos he was having during our conversation; I told him I would go home to try to send letters to different organizations to get him a refrigerator. He then told he was worried because “those at home” [his neighbors] were planning on going out for vacations, and he needed to locate his medicine elsewhere. Right before I left, he mentioned that his tummy ached.
That neighbor would also ask his wife to wash some of Fermín’s clothes. The neighbor’s wife seemed to be aware of Fermín’s needs but, given the “macho culture” in Mexico, his relationship with her, and the access to the family’s infrastructure was mediated by her husband. During one of the Christmas celebrations, the couple invited him in to have dinner with them once they realized that he was going to spend it alone.
It was not just men that lived in his neighborhood that offered help to Fermín. Other men he would share time and space with during work would engage in similar caring practices. Some of these relationships rendered more profit than did his job. Perhaps this is one of the reasons why he would continue to work on the streets, as he benefited much more than financially.
Spontaneous, Caring Practices Defined by Circumstantial Characteristics
The caring practices encountered were not just about providing access to material goods, such as food, money, or infrastructure in general. The fourth type of caring practice was, as previously noted, different in nature, in that it was defined by the temporality of the circumstance rather than its materiality. These practices were improvisational resolutions made at a particular moment, and their mere purpose was to ensure the well-being of Pato or Fermín.
These practices could come from unsuspected places and people, such as Fermín’s rival “parquero” from the next block. Even though they would get in casual territorial arguments where they would curse at each other, Fermín requested his protection on one occasion, and it was not denied. A person whom Fermín met as a patient in the hospital supposedly wanted to beat him up over a cell phone, and since none of his acquaintances from that block were around to help him, he moved as fast as he could, using his cane, toward his fellow “parquero” (referenced in Figure 2 as “B5”). He explained the predicament to him and requested his assistance in case of physical confrontation. Although nothing happened, Fermín remained with the “parquero” until he felt that it was safe to return to his block. In subsequent discussions, the “parquero” claimed to have been ready to back him up, as it can be seen on the following field notes from July 20, 2015: Today I spoke with Fermin’s rival “parquero,” I hollered while Fermin went inside the hospital to use the bathroom. We spoke of how the sunlight comes and goes; he said it was because the sun was “drunk.” He then proceeded to tell about the “bronca” [quarrel] Fermin had with some guy. He told that when that happened, Fermin came to him; even though they tend to complain about each other. According to B5., Fermin seemed “scared,” and he urged me to take measures to protect him.
Pato’s friends’ caregiving practices did not seem strictly related to his AS, but had a positive impact on his general well-being and integration into the society; some of them were spontaneous and defined by circumstantial characteristics. According to an unrecorded interview from March 2016, there was one occasion where they were at the bar accompanied by some lady friends. Completely drunk, he had laid his head down against the table, and nobody seemed to mind him. Then he started vomiting under the table, splashing his pal’s shoes with the fluid. No one seemed to realize it because the music was loud, and the lights were dim until eventually, one of his pals did. They tried not to make a scene about it. One of them, W, who is the same age as Pato but earns a little more by working as a mechanic, took him as discreetly as possible into the bathroom to get him cleaned up. Eventually, everyone at the table found out and even laughed about it. However, this did not deter L’s night with his mates; they moved on to another bar that same night to continue guzzling beer.
Discussion
Both the needs and health-seeking behavior of these Rarámuri disabled men served as switches (Bateson, 1978) that ignited caring practices that conformed patterns from men who had more economic resources, no disability, and were not Rarámuri. These caring practices were the procuration of access to food, money, and infrastructure. The fourth type of caring practice was identified. However, it differed from the other because it was determined by circumstantiality and improvisation. All of these practices served as a positive and productive response to these particular Rarámuri disabled males’ needs. During research, the concept of “care of the self” (Foucault, 2002), were men act as caregivers, emerged throughout analysis. These were evidenced through caring practices among men that do not share ethnicity, income, or health situation.
O’Brien, Hunt, and Hart (2005) sustain that men, in general, tend to avoid seeking health care. In the present study, there was a broader perspective of the health-seeking practices by these disabled men, because the care offered to them by other men was also acknowledged. This reluctance to seek care is perhaps related to Lozoya’s (1998) hypothesis that men tend to deny or minimize health problems because they have been brought up to believe that ability to withstand pain is a male trait and thus have difficulty admitting it. However, Fermín was able to readily express the existence of physical pain due to his disease and even used his suffering to obtain favors and money (the caring practice identified as access to money). It must be noted that Pato’s case is more benign due to the relatively early AS diagnosis and more significant familial support, which Fermín sadly lacked. Nonetheless, in both cases, their masculinity leads to solidarity bonds with other males in a marginal context that involves social and symbolic exclusion.
These caregiving and health-seeking actions between men could be considered as engendering (Gutman, 1998) and therefore paint a broader and more benign picture of what men do and are capable of doing. If competitiveness (Riska, 2002) is recognized as a heterosexual masculinity trait, cooperativeness and caregiving should be considered as well.
Generally speaking, the aforementioned caring practices in between men relate to the concept of sisterhood as used by Lagarde de los Ríos (2006), and the concept of “cuatismo,” as used by Adler (2016). These caring practices conform a broader set of male practices that are, according to Connell (2006), incoherent, and may involve everyday acts of domination, recognized by Bonino (2004) as “micromachismos.”
Sisterhood speaks of inter-gender solidarity and companionship. The ethical, political, and practical dimensions from contemporary feminism that Lagarde links directly to her concept and as a solidarity mechanism against misogyny differentiate it from the caring practices observed in the present research. In the cases described, the men’s acknowledgment of their solidarity seems to be less explicit and not founded on patriarchal antagonism.
The caring practices described in this research relate to the concept of “cuatismo” (Adler, 2016), which is a native category that describes norms, values, and social relationships that are established between male friends that share Mexican culture. It is a type of relationship that despite being positive, also involves physical and verbal aggression, activities that were also observed through the research. The “cuatismo” relationship implicates favors that involve fixing things in each other’s household, such as plumbing. Again, these types of behavior were also observed, particularly within neighborhood relationships. Even with all these similarities, the concept does not fully apply to what was observed through the research, because “cuatismo,” as described by Adler, does not involve health as a fundament of these relations. The author links these relationships and practices to drinking activities as something crucial. Drinking is a bonding activity for males, and while it was observed and described, it was not as crucial. Also, unlike the present study, Adler examined the roles of these males’ wives in those relationships. These differences may also be due to the methodological factors characterizing the two studies (Adler, 2016). Adler was a female and her idea of “cuatismo” derived merely from interviews and oral descriptions of interactions. Another fundament for her conclusions stems from surveys of families and wives of men studied, something that was not done for the present research.
Male caring practices reflect solidarity. However, just as masculinities are incoherent (Connell, 2005), observations revealed that the same men that carried out these graceful actions hurt each other as well. The men that cared for Fermín would also insult him, mock him, and even physically subdue him. These practices, in general, seem undifferentiated or simultaneous to opposing practices between men. In this case, the idea of “micro-machismos” (Bonino, 2004) is supported, as acts that perpetuate dominance coexist with the caring practices.
It should be noted that these caring practices merely mitigated the suffering and did not contest the actual position of subordination and marginality these men represented. As benign as they were, they did not address the structural factors behind their illness—factors such as discrimination and marginalization based on economic, health, and ethnic status. These practices did not challenge the hierarchy status between the males involved, about hegemonic masculinity. This phenomenon could be related to the fact that the actions described were mostly ephemeral and implicit, not recognized by the men who participated in such solidarity practices.
Even if the supposed patriarchal order prohibits outward displays of emotion, attachment, or pleasure (Connell, 2005), these still appeared in ordered and institutionalized ways through the gender order. Emotion, attachment, and pleasure were involved in these caring practices. The care of the self (Foucault, 2002) concerning gender proves that an attitude toward the world, oneself, and others may contradict a reductionist view of masculinities based solely on a patriarchal order. The masculine and feminine as symbolic dimensions of the care of the self (Garcés & Giraldo, 2013) can be linked to an idea of a masculine ethos (Bateson, 1990). Bateson’s idea of a masculine ethos refers to a system of values and emotions, that in these cases are related to masculinity, a gender ethos within a given context that is plural, and it could further develop the idea of care of the self, since both of them relate to ethical aspects of a person’s life. This male ethos could, at last partially, be behind the person’s motivation to provide care. It can also relate to meaning construction carried through practices, which in turn reflect ethics and their relation to gender.
Nissen (2017) mentions men’s profound commitment for caring for self and others, focusing on men’s statements on their individualized experiences. In particular, the author acknowledges the complex patterns of masculinity that emerge in health and illness through the idea of caring practices. However, methodologically, researching those statements of caring practices is also essential. Just like Nissen, practices of care/caring from a broader life situation in the context of sociality were studied, rather than focusing on the biomedical perspective. The difference between the present work and that of Nissen stems from the fact that in this research, aspects of interactions of disabled males with other men and how they care for each other were studied, rather than focusing on self-care. It is valuable to speak of a “caring masculinity” that is associated with values, processes, and activities that reflect co-responsibility and commitment. Nissen argued that this commitment and responsibility is directed toward one’s health. However, this paper posits that it is directed toward well-being that goes beyond biomedical health and is not necessarily focused on self-care, but rather caring for others.
Mauss’s “Essay on the gift” (1978) helps fathom Nissen’s idea of the intervention and interaction involved in male’s caring practices. The caring characteristics previously outlined in the Introduction section (orientation, distribution and circulation, co-implication, and a moral purpose) traverse all the ethnographic data and al the excerpts of the interviews, and could help develop a male’s caring practices theory approach.
Most of the caring practices described were not remunerated; however, they did involve a symbolic type of distribution (Mauss, 1979), in the sense that they may have generated a sense of honor as gratification by their doing. This symbolic circulation and distribution are directly linked to a moral purpose, which could also explain why the caring practices would many times go unnoticed, as they were not always acknowledged explicitly or simultaneously by the parties involved.
Masculinity conforms part of the multidimensionality of someone’s personhood. The results of the study suggest that masculinity is conditional (Lipset, 2008) because it also intertwines with other dimensions of the personhood such as health (in this case focused on their disease and its consequences such as disability), ethnicity (being Rarámuri), and socioeconomic status (both cases lacked economic resources)—all of these factors seem to condition a person’s masculinity.
If gender is a socializing process that starts when we are infants and continues throughout one’s lifetime (Lozoya, 1998), there is no reason to believe that Pato, Fermín, and other men discussed in this article should stop constituting themselves as men. Although it might appear that disability conflicts (Shuttleworth, Wedgwood, & Wilson, 2012), with Pato’s and Fermín’s masculinity, the men around them, and the relationships they developed with each other prove the opposite; this may be related to the processual personhood identified by Lipset (2008). In this sense, there is plasticity to how different persons embody their masculinity, mainly through improvisation and imagination (Cruz, 2015). Indeed, there is no such thing as less of a man; they are simply men under different and subordinate circumstances. It is these circumstances that give way to a set of gender relations that prove that, regardless of their different conditions, men play a role in gender relations, and are prone to acts of solidarity involving other men in worse circumstances. Therefore, these solidarities also constitute manhood. In the course of this research, masculinities embodied beyond that apparent conflict were encountered. These relationships prove that a conflict does not necessarily exist, but rather predisposed ways of caregiving and help-seeking, all of which can only be understood to other masculinities (Connell, 2005).
Another way observed on how this multidimensionality is intertwined through Fermín’s and Pato’s ethnicity and health status in regard to their relationship with the Government. Both of these statuses were recognized by the government, to a point where the distinction between those two statuses blurred. For example, the government would pay for Fermin’s medicine due to his ethnicity. Also, their socioeconomic status identity made them eligible for other benefits, such as access to a health-care system. The Mexican health regulations focus more on vulnerability than ethnicity, even though ethnicity may be considered as a vulnerability (Colmenares-Roa & Peláez Ballestas, 2019, p. 3).
Fermín and Pato capitalized on their official recognition as either Rarámuris, disabled, or poor, to receive different types of economic support, but did not seem to have current ties with their fellow Rarámuris. They did not take part in the Rarámuri community life or follow their traditions and barely spoke their language.
Finally, men like Fermín and Pato (who could represent subordinate masculinities) should also be seen as caregivers, rather than just inanimate beings who merely receive care. This perspective could prove to be engaging in further masculinity and health studies among men with chronic musculoskeletal diseases and progressive disability.
Conclusion
Reflections have been drawn from every day unnoticed practices that men carry out to one another, and which try to contribute to the well-being of the other. The situations chosen for a more detailed analysis that are presented here prompt us to conclude that masculinities exhibited in situations characterized by inequity lead to the emergence of solidarity between males, especially if among the chain of male relationships there is marginality, mainly in the form of poverty, disease, and their consequences (Figure 3).

Masculinities and health.
de Keijzer (2001) recognized the need to build health policies directed at men, and this onset of relationships offers a model of how to do that. These actions between men could be promoted for better caregiving and to better understand health seeking by men outside professional health-care settings, such as clinics or hospitals.
If being a man constitutes a risk factor (Lozoya, 1998), being a man and having men around could also constitute a protective factor under certain conditions, such as the ones observed. Not all help and caregiving have to be medical, in the allopathic sense of the word and does not require specialized health professional knowledge. Even if expert medical knowledge and treatment are crucial for patients with AS, their well-being also depends on day-to-day circumstances that involve food, money, shelter, and having recreational activities, all of which are directly related to a broader term that could be conceptualized as well-being. Public programs could have a gender perspective when it comes to men and caregiving, with a scope beyond other more traditional figures.
Limitations
The qualitative nature of the research limited the number of participants to 11 in order to allow an in-depth analysis of the relationship between masculinity and health. Also, the relational component of gender identity might have been hindered by the fact that female participants were discarded for the Results section. Since none of the researchers identify as Rarámuri, the study could be considered as an academic’s perspective. In addition, the Rarámuri participants involved individuals that have been living in the city for most of their lives, and their representation of their Rarámuri identity could differ from that of Rarámuri the people still living in La Sierra Tarahumara.
Footnotes
Acknowledgements
Our thanks to Dr. Comenares-Roa, Dr. Claudia Infante, Dr. Rubén Burgos-Vargas, Dr. Margarita Hope, and Erick Luévano for their valuable comments and contributions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Council for Science and Technology (CONACYT)- Salud 162154.