
Abstract
The rising prevalence of diabetes mellitus (DM) is a serious global health concern. The world is experiencing type 2 diabetes epidemics and prevalence differs by gender, regions, and level of socioeconomic development. Type 2 diabetes mellitus (T2DM) in men increased at a faster rate and numbers are continuing to rise in some regions of the world. This study aimed to estimate the prevalence of T2DM among men in the Middle East countries. Seventy-four research articles were identified through search engines including Web of Science, Medline, PubMed, EMBASE, Scopus, and Ovid databases by using keywords “epidemiology,” “prevalence,” “diabetes mellitus,” and individual names of the Middle East states. Finally, 17 studies were included for the assessment of prevalence of T2DM among men in the Middle East. In the Middle East, high prevalence of T2DM among men was identified in Bahrain (33.60%), Saudi Arabia (29.10%), United Arab Emirates (UAE; 25.83%), and Kuwait (25.40%), whereas low prevalence was reported in Iran (9.90%) and Yemen (9.80%). The random pooled prevalence in the Gulf Cooperation Council (GCC) states was (24.0%) compared to non-GCC states (16.0%), and in both GCC and non-GCC countries combined, it was 19%. The prevalence was significantly associated with the gross domestic product of these states (p = .0005). Despite different socioeconomic and cultural settings in the Middle East, the rising T2DM prevalence among men was identified in Bahrain, Saudi Arabia, UAE, and Kuwait. These states must incorporate future diabetes defensive strategies targeting the Middle East population to minimize the burden of DM from the region.
Diabetes mellitus (DM) is a major public health concern with rising prevalence and long-lasting impairments. In spite of significant advancement in medical sciences, this lifelong debilitating disease is not curable and, unfortunately, is swiftly growing in different age clusters and both genders (Meo, 2009). Worldwide, the prevalence of DM has augmented dramatically; it impairs numerous physiological functions (Meo, 2009), multiple organs, and body systems with extensive impediments (James, Alberti, Mayer, & Ralph, 2002; Meo et al., 2015). DM is a multifactorial syndrome (Meo et al., 2018), rapidly increasing in all the continents of the globe (Alhyas, McKay, & Majeed, 2012). The worldwide existing prevalence of DM is about 425 million people, of whom 279 million are in urban areas and 146 million are in rural zones (International Diabetic Federation Diabetes, 2018).
The Middle East comprises 17 countries with a population of about 371 million people (World Bank, 2018). In the Middle East, the rapid changes in the socioeconomic conditions have caused swift urbanization and variations in the health and disease pattern. Traditional diet habits have been rapidly wiped out and a deskbound lifestyle has penetrated the society (Zabetian, Keli, Echouffo-Tcheugui, Narayan, & Ali, 2013). In the Middle East, the level of physical inactivity exceeded 40% in most of the states (Sharara, Akik, Ghattas, & Makhlouf, 2018). People are spending long periods sitting in front of televisions with a remote control culture, eating fast food, and exercising rarely, which are the leading reasons for obesity and DM (Zabetian et al., 2013). The gross domestic product (GDP) per capita is also associated with obesity (Egger, Swinburn, & Islam, 2012) and DM (Meo, Usmani, & Qalbani, 2017). DM in men increased at a faster rate and numbers are continuing to rise (Hawkins et al., 2017). This study aimed to investigate the prevalence of type-2 diabetes mellitus (T2DM) among men in the Middle East.
Methods
Selection of Studies
This retrospective study employed a descriptive approach to investigate literature to report the prevalence of T2DM among men in the Middle East states. A literature search was conducted in January 2018 through ISI Web of Science, PubMed, Medline, EMBASE, Scopus, and Ovid databases on articles published since 2008 until December 2018. The relevant studies were explored through key words including “diabetes mellitus,” “prevalence,” and “type-2 diabetes mellitus.” The individual Middle East state names were included in the database in order to obtain the required articles. The literature search revealed a variety of publications published on the prevalence of T2DM in Middle East states and these were used to assess the T2DM prevalence. Seventy-four articles published between the period 2008 and 2018 on the prevalence of DM were identified; the suitability of articles was scrutinized and analyzed by the title and abstract of the study in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (Figure 1; Moher, Liberati, Tetzlaff, & Altman, 2009). The articles were carefully selected and reviewed by two investigators and rechecked by the third investigator for the prevalence of T2DM, and data were recorded.
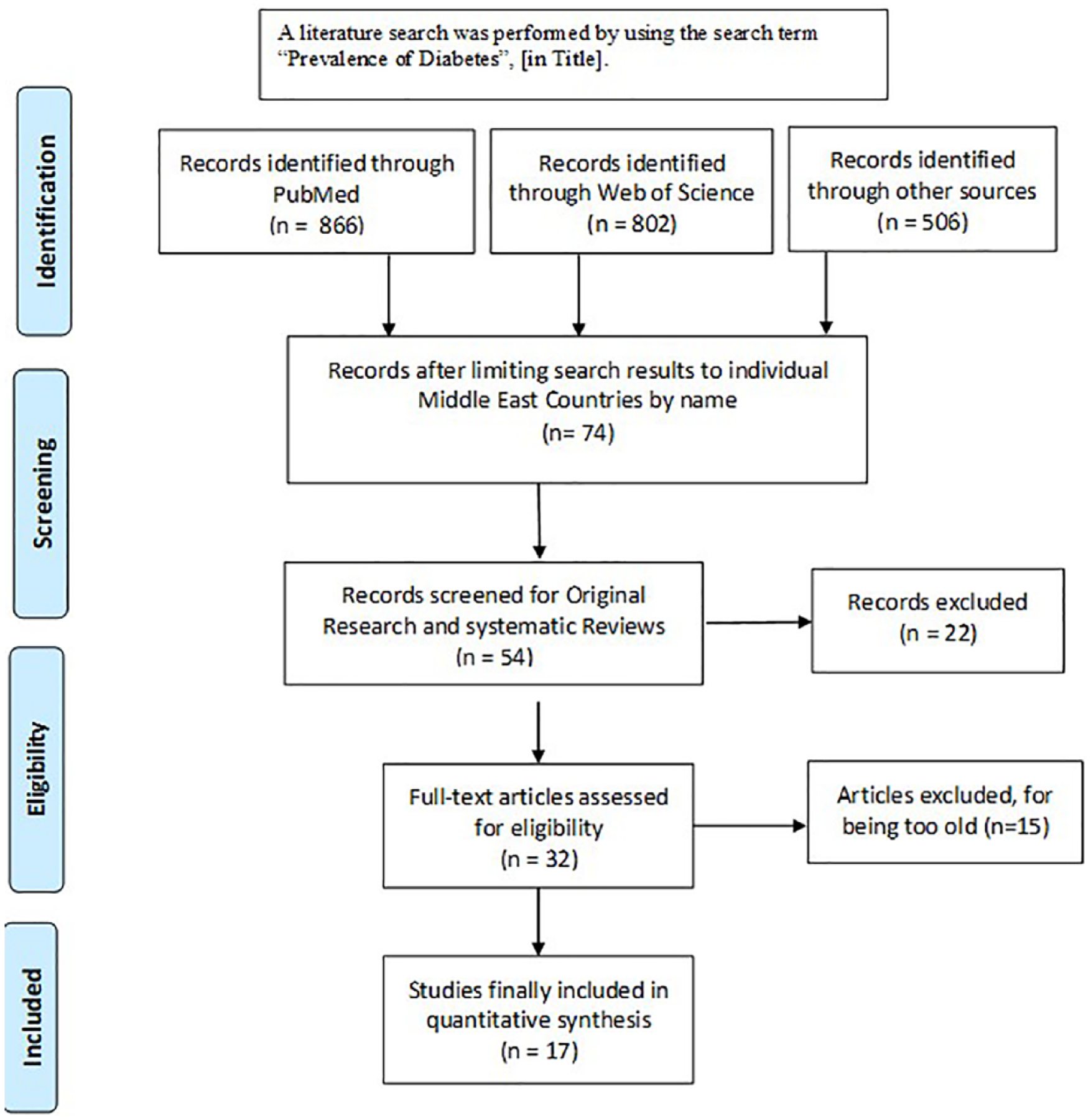
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram for the selection of studies for prevalence of type 2 diabetes mellitus in the Middle East.
Inclusion and Exclusion Criteria
The inclusion method for the selection of studies was based on the study population from the Middle East countries from articles that contained information about “prevalence” and “types of diabetes mellitus.” There were no restrictions on the design or language of the research articles. The secondary reports such as brief communications and nonobservational correspondence without synthesis of novel data were not included. A total of 74 studies were included; type, quality, and sample size were carefully assessed and finally 17 articles were selected for the analysis and remaining studies were excluded (Figure 1). The data about Middle East countries’ per capita GDP for the previous 23 years (1990–2013) were recorded from the World Bank sources.
Ethics Statement
In this study, patients were not directly involved; the prevalence of T2DM-associated data were obtained from databases; hence, ethical approval was not required.
Statistical Analysis
T2DM pooling prevalence was assessed with both fixed effect and random effect models. The prevalence of T2DM was recorded and association with GDP per capita was calculated by Pearson correlation coefficient two-tailed; p < .05 was considered significant. Analysis was performed using the R Foundation for statistical computing (Guido, 2007).
Results
The prevalence of T2DM among men in the Middle East countries is presented in Table 1. In the Middle East, six states are part of the Gulf Cooperation Council (GCC) countries. The prevalence of T2DM among men in Bahrain was 33.60%, Saudi Arabia 29.10%, the United Arab Emirates (UAE) 25.83%, Kuwait 25.40%, Qatar 17.97%, and Oman 13.08% (Table 1). In the other Middle East states, T2DM prevalence was recorded as follows: Lebanon 26.41%, Cyprus 26.00%, Iraq 19.60%, Jordan 18.27%, Palestine 16.90%, Turkey 16.00%, Syria 15.60%, Israel 13.70%, Egypt 12.70%, Iran 9.90%, and Yemen 9.80%. Among these states, the prevalence of diabetes was higher mainly among the GCC countries (Table 1; Figures 2 and 3). The random pooled prevalence in the GCC states was 24.0% compared to 16.0% in non-GCC states, and in the GCC and non-GCC countries combined, it was 19.0% (Figure 4). The prevalence was significantly allied with GDP of these states (p = .0005; Figure 3).
Prevalence of Type 2 Diabetes Mellitus Among Men in Middle East Countries.

Note. DM = diabetes mellitus; GCC = Gulf Cooperation Council; UAE = United Arab Emirates; U/R = urban/rural.
Pooled prevalence fixed and random effect has been recorded for both GCC and Non GCC states.
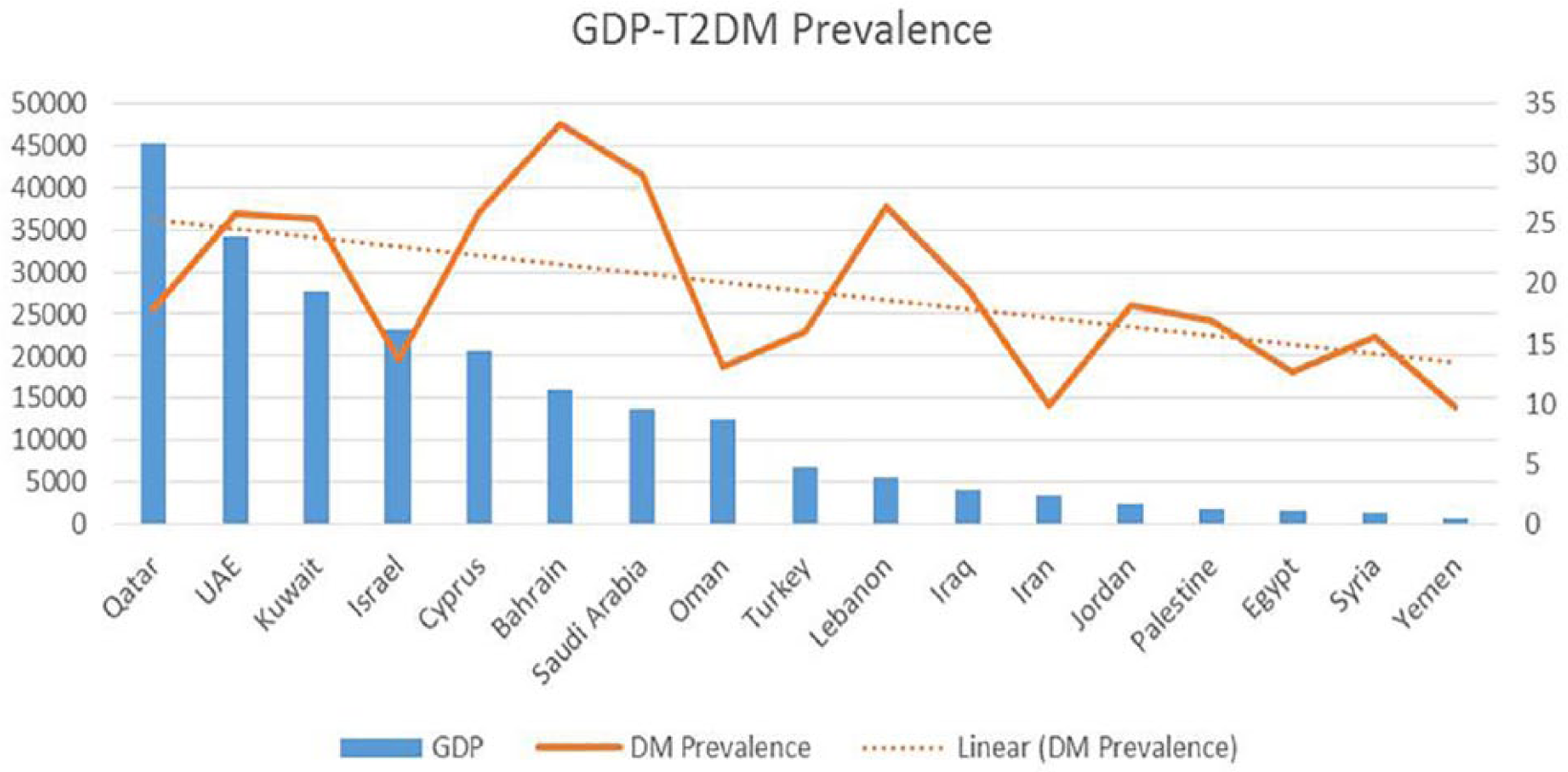
Prevalence of type 2 diabetes mellitus (T2DM) among men in Middle East countries and gross domestic product (GDP). UAE = United Arab Emirates.

Correlation between gross domestic product (GDP) per capita and prevalence of type 2 diabetes mellitus (T2DM) among men in Middle East states.

Pooled prevalence of type 2 diabetes mellitus (T2DM) among men in the Middle East: fixed and random model effect.
The mean GDP per capita of the past 24 years from 1990 to 2013 in USD is presented in Table 2. Among Middle East countries, the highest GDP is that of Qatar (US$ 45,231) followed by UAE (US$ 34,166), Kuwait (US$ 27,739), Israel (US$ 23,215), Cyprus (US$ 20,583), Bahrain (US$ 15,993), and Saudi Arabia (US$ 13,653); the lowest are those of Palestine (US$ 1,752), Syria (US$ 1,354), and Yemen (US$ 831). The average GDP per capita and prevalence of T2DM in GCC states are US$ 24,858.33 and 25.03%, in non-GCC states US$ 6528.39 and 12.69%. However, in both GCC and non-GCC nations, the combined GDP is US$ 12,966.78, and prevalence is 16.80% (Table 1; Figures 2 and 3).
Middle East Countries With GDP Per Capita (USD) From 1990 to 2013.
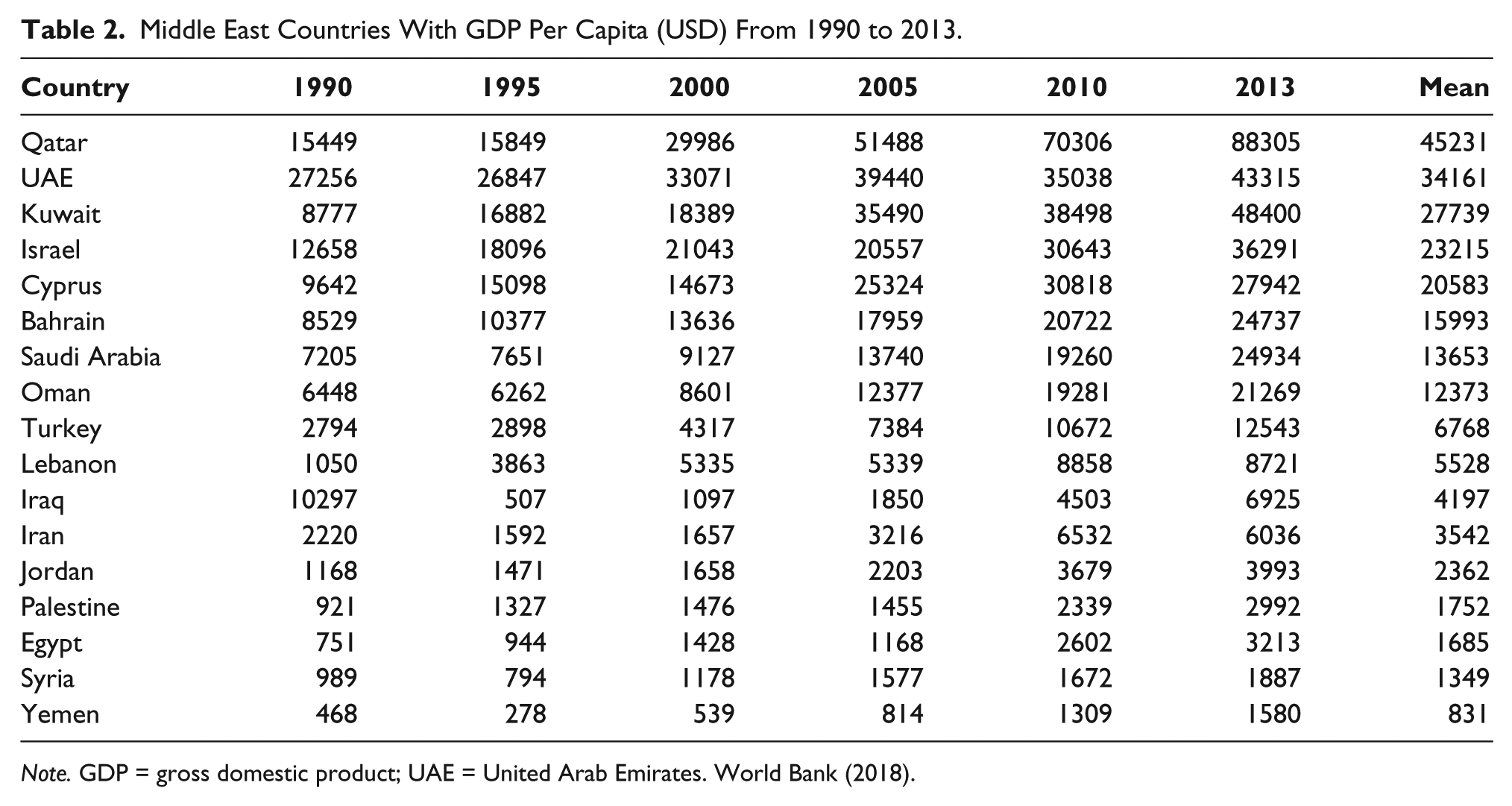
Note. GDP = gross domestic product; UAE = United Arab Emirates. World Bank (2018).
Discussion
This study is considered the first of its kind that presents the prevalence of T2DM among men in the Middle East. High T2DM prevalence was identified among men in Bahrain, Saudi Arabia, UAE, and Kuwait, whereas low prevalence was identified in Iran and Yemen. The random pooled prevalence in GCC states was 24.0% compared to 16.0% in non-GCC states, and GCC and non-GCC countries’ combined pooled prevalence was 19%. The prevalence was significantly allied with GDP of these states.
Wild, Roglic, Green, Sicree, and King (2004) reported the global number of diabetic patients as 171 million in 2000 and projected this figure to be 366 million in year 2030. Van Dieren, Beulensm, Van der Schouw, Grobbee, and Neal (2010) reported 250 million T2DM patients and expected this figure to rise to 380 million by 2025. In another study, Shaw, Sicree, & Zimmet (2010) reported that the worldwide approximate diabetes prevalence was 6.4%, which would be expected to rise to 7.7% by 2030. In 2018, the International Diabetes Federation’s IDF Diabetes Atlas, 8th edition displayed new statistics, which completely broke all the previous prevalence records reported by Wild et al. (2004), Van Dieren et al. (2010), and Shaw et al. (2010). It specified that worldwide prevalence of diabetes is 8.8%, showing that 425 million adult people are diabetics, of whom 279 million people are in urban and 146 million in rural zones (International Diabetic Federation-Diabetes, 2018).
In Saudi Arabia, few studies were performed to assess the prevalence of T2DM. In 1990, the prevalence was 6% (Anokute, 1990); in 1997, 10.3% (Al-Nuaim, 1997); and in 2004 it rose to 23.7% (Al-Nozha, Al-Maatouq, & Al-Mazrou, 2004). Recent literature described that the T2DM prevalence in Saudi Arabia is 29.8% for men (Al-Rubeaan et al., 2015). All these reports confirmed the rising pattern of DM. The present study identified that T2DM prevalence is swiftly increasing among men in the Middle East nations (Table 1 and Figure 2).
Similarly, in Bahrain, Musaiger (1992) reported that the DM in Bahraini people was 0.8% in 1980, and in 1982, it was 10.2%. In 1996, Zurba and Al-Garf (1996) conducted an epidemiological study among Bahraini population and identified that DM prevalence was 25.5% in men. In another study, Al-Zurba (2001) reported that 25.5% prevalence of T2DM was identified among Bahraini residents aged 20 years or above. Aloia and Jassim (2017) identified that T2DM among men in Bahrain has increased by a prevalence rate of 33.60%.
Another GCC country, Kuwait is also facing the rising occurrence of T2DM. Al Khalaf, Eid, Najjar, Alhajry, and Doi (2010) reported 21.4% prevalence of diabetes in the Kuwaiti natives. Channanath et al. (2013) demonstrated that the crude prevalence of T2DM in Kuwait was 25.4%. A similar pattern was identified in UAE where the prevalence of DM was 25% among UAE citizens and the percentage amplified with age (Malik, Bakir, Saab, & King, 2005). In Oman, Al-Lawati, Al-Riyami, Mohammed, and Jousilahti (2002) reported that the crude prevalence of DM was 16% in men. It was 22% and 21% in Adh-Dhahirah and Dhofar zones, higher in urban than rural regions. In a study performed in Qatar, the authors identified that the average prevalence of DM among adult Qatari people was 16.7%, increasing up to 29.2% among people aged 30–49 years (Bener et al., 2009). T2DM prevalence has also increased in non-GCC states of the Middle East. In Jordan, Ajlouni et al. (2008) reported that the age-consistent DM prevalence among Jordanian population rose from 13.0% to 17.1% during the past few years. In Egypt, DM prevalence was 17% and in Syria it was 15.6% (Albache et al., 2010). Gunaid and Assabri (2008) recorded the DM prevalence among the adolescent population of Yemen. The authors identified that the crude prevalence of DM was 6.57% and age-adjusted prevalence for 30–64 years was 9.75%. They concluded that the crude prevalence of T2DM in the capital of Yemen was 10.4%.
Abdul-Rahim, Husseini, Giacaman, Jervell, and Bjertness (2001) investigated the prevalence of DM among the urban population of Palestine and reported that 12.0% of the population was suffering from diabetes. Husseini, Abdul Rahim, Awartani, Jervell, and Bjertness (2000) reported the estimated prevalence of diabetes among the Palestinian rural population aged 25–65 years was 9.7% in 2000, which increased to 15.3% in 2010, and in men, DM increased from 9.1% to 16.9%.
Majeed et al. (2014) reported the prevalence of DM in the Middle East and North Africa (MENA) region and reported that the prevalence in Saudi Arabia was 23.87%, Kuwait 23.09%, Qatar 22.87%, Bahrain 21.84%, UAE 18.98%, Egypt 16.80%, Lebanon 14.99%, Oman 14.24%, Jordan 11.40%, and Iran 9.94%. Meo et al. (2017) reported that in Arab-speaking states the prevalence of DM was higher in GCC states. In the present study, it has been identified that the Middle East states have the maximum prevalence of T2DM. The highest prevalence of T2DM was identified among men in Bahrain, Saudi Arabia, UAE, and Kuwait and lowest prevalence was identified in Iran and Yemen (Table 1, Figure 2). The random pooled prevalence in GCC states was 24.0%, that in non-GCC states was 16.0%, and in GCC and non-GCC countries combined, it was 19.0% (Figure 4). The prevalence was significantly allied with GDP of these states (Figures 2, 3).
While debating the reasons for the rising prevalence of T2DM in Middle East, Badran and Laher (2012) reported that the high-income oil-producing GCC countries in the Middle East have higher TD2M prevalence. In Middle East states the increased prevalence has been seen mainly due to swift monetary development, urbanization, changes in lifestyle, obesity, reduced physical activity, and the possibility of region-specific genetic mutations associated with diabetes (Zabetian et al., 2013). These elements are the leading causes of growing prevalence of T2DM in Middle East countries.
Study Limitations
This is the first study added in the literature to investigate the prevalence of T2DM among men in the Middle East. The limitations of this study are that the authors tried to select homogeneously designed, randomized, cohort, large-sample-sized, community-based studies with American Diabetes Association (ADA) or World Health Organization (WHO) criteria, but the authors faced some methodological challenges as all the 17 Middle East states were included and in every country, various methodological approaches were adopted to investigate the prevalence of T2DM. Therefore, the authors were unable to choose all the homogeneous studies. Furthermore, some states lacked literature. Hence cohort, randomized, cross-sectional, community, and hospital-based studies were selected. The data presented for all the Middle East countries may not represent the entire population of the said country. Hence; it might not be a representative of the holistic picture of the prevalence of T2DM in men in Middle East countries.
Conclusions
Despite the different socioeconomic and cultural settings in the Middle East, rising T2DM prevalence among men was identified in Bahrain, Saudi Arabia, UAE, and Kuwait; however, low prevalence was identified in Iran and Yemen. The high prevalence was seen in GCC countries compared to non-GCC states. Irrespective of the limitations, the prevalence of T2DM among men in Middle East seems to be substantial. These states must incorporate future diabetic defensive strategies targeting Middle East populations to minimize the burden of the disease from the region. More attention should be given not only to diabetes screening but also to educational and health promotion programs; avoiding sedentary lifestyle and doing regular physical activities should be encouraged to reduce the prevalence of T2DM in the region.
Footnotes
Acknowledgements
The authors are thankful to the Deanship of Scientific Research, King Saud University, Riyadh, Saudi Arabia for supporting the work (RGP-VPP 181).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Deanship of Scientific Research, King Saud University, Riyadh, Saudi Arabia supported the work through the Research Group Project (RGP-VPP 181).