
Abstract
The use of mobile phones has remarkably increased and become a basic need of daily life. Increasing subscriptions of mobile phones boost the installation of mobile phone base station towers (MPBSTs) in crowded commercial and residential areas including near school buildings. This study investigated the impact of exposure to radiofrequency electromagnetic field (RF-EMF) radiation generated by MPBSTs on cognitive functions. Two hundred and seventeen volunteer male students aged between 13 and 16 registered from two different intermediate schools: 124 students were from School 1 and 93 students were from School 2. The MPBSTs were located within 200 m from the school buildings. In School 1, RF-EMF was 2.010 µW/cm2 with a frequency of 925 MHz and in School 2, RF-EMF was 10.021 µW/cm2 with a frequency of 925 MHz. Students were exposed to EMFR for 6 hr a day, 5 days a week for a total period of 2 years. The Narda Safety Test Solution device SRM-3006 was used to measure RF-EMF in both schools, and cognitive functions tasks were measured by the Cambridge Neuropsychological Test Automated Battery (CANTAB). Significant impairment in Motor Screening Task (MOT; p = .03) and Spatial Working Memory (SWM) task (p = .04) was identified among the group of students who were exposed to high RF-EMF produced by MPBSTs. High exposure to RF-EMF produced by MPBSTs was associated with delayed fine and gross motor skills, spatial working memory, and attention in school adolescents compared to students who were exposed to low RF-EMF.
In recent years, tremendous developments in mobile phones have revolutionized the telecom industry by making telecommunication faster, economical, and more convenient (D’Silva, Swer, Anbalagan, & Bhargavan, 2014). With the introduction of new applications and multifunctional technology in mobile phones, the telecom industry is appealing to both youth and adults. The usage of mobile phones has dramatically increased, which is considered as a basic tool in daily life (Al-Khlaiwi & Meo, 2004). Worldwide, the number of subscriptions of mobile phones is about 7.52 billion. This number is more than the worldwide population, as many users own more than one mobile phone (World Bank, 2018). The extensive usage of cellular phones has led to the growing installation of mobile phone base station towers (MPBSTs) in crowded commercial and residential areas, which raises community concerns (Buckus et al., 2017; Meo et al., 2015; Wiedemann, Freudenstein, F., Böhmert, Wiart, & Croft, 2017; Zhang et al., 2017; Figure 1).

Mobile phone base station tower located in a residential area.Source: Photo taken by a coauthor.
MPBSTs are mainly installed on tall trees, water tanks, or tall commercial and residential buildings to provide the best possible network services (Meo et al., 2015). Mobile phones communicate with nearby MPBSTs mainly through EMF radiofrequency waves operating at the frequencies of 1.8–2.2 GHz for digital systems and 400–900 MHz for analogue systems (Buckus et al., 2017). The EMFs absorbed by MPBSTs are based on the properties of the absorbing tissue, antenna position, magnetic field frequency, the power emitted, and distance of their placement (Wiedemann et al., 2017). Exposure to RF-EMF has several effects on human health including fatigue, tension, headache, sleep disturbance (Al-Khlaiwi & Meo, 2004), physiological and psychological problems (Deniz et al., 2017), hearing and vision complaints (Meo & Al-Drees, 2005), risk of type 2 diabetes mellitus (Meo et al., 2015), and cancer (Moulder, Foster, Erdreich, & McNamee, 2005).
Extensive fixing of MPBSTs in densely populated commercial, residential areas, and school buildings has started community concerns about adverse effects on human health (Meo et al., 2015), mainly brain function (Saikhedkar et al., 2014). Therefore, this study explored the association of exposure to radio frequency electromagnetic field radiation (RF-EMFR) generated by MPBSTs on cognitive function amongst school-going adolescents.
Methods
Study Design and Participants
Students were recruited based on their apparently healthy status, voluntary participation, same gender, age, height, weight, ethnicity, and from homogenous educational, socioeconomic, and residential backgrounds. Initially, 300 students (150 from School 1 and 150 from School 2) were registered. A detailed clinical history was obtained to consider whether the students should be included or not. After clinical history, finally 217 were selected:124 students from School 1 and 93 from School 2. The age of School 1 group was 13–16 years (mean age 14.25 ± 0.98) and that of School 2 group was 13–16 years (mean age 14.10 ± 1.01). The study was piloted as permitted by the Institutional Review Board, College of Medicine King Saud University, Riyadh, Saudi Arabia (Ref # E-16-2124). Written consent was obtained from the students and or their parents.
Exclusion Criteria
Students with clinical histories of blood disease, anemia, diabetes mellitus, obesity, asthma, seizures, malignancy, and those who smoked tobacco were excluded from the study. Known cases of anxiety, vision problems, attention deficit, skeletal muscle disorders, physical disability, those on sedatives, and those with sleep disturbance history were also excluded from the study (Meo, Bashir, Almubarak, Alsubaie, & Almutawa, 2017; Timothy, Durazzo, Meyerhoff, & Nixon, 2010). Students whose residence was near the high transmission lines or MPBST were also excluded (Meo et al., 2015). Students who frequently used and kept cordless phones and Wi-Fi routers in their bedrooms were also excluded from the study (Meo et al., 2015).
Radiofrequency Field Exposure
Two different intermediate schools were selected; both had MPBSTs situated nearby and were operational for about 3 years. The source of RF-EMF around the schools was visually checked by two coauthors to exclude the presence of any other source of RF-EMF, overhead power lines, or high transmission electricity lines in the surrounding area. RF-EMFR measurements were done in three different sites of the classrooms (center and two corners), twice a day before and after recording the test parameters during the study period in a similar research methodology approach used by (Meo et al., 2015).
The Narda Safety Test Solution SRM-3006 was used to measure the RF-EMF. In School 1, the RF-EMF was 2.010 µW/cm2 and in School 2 it was 10.021 µW/cm2 at a frequency of 925 MHz; students were exposed to RF-EMFR for 6 hr daily, 5 days a week (Meo et al., 2015) for a total period of 2 years.
Neuropsychological Tests Procedure
Cognitive function was tested using the Cambridge Neuropsychological Test Automated Battery (CANTAB) research suite 6.0.37. Measurements were recorded at a fixed time of the day (9:00–11:00 am) to minimize the physiological diurnal variations. Each subject was tested in two tasks; the total time required to complete the tasks was about 15–20 min. Sitting well on a chair, with a flat touch screen in front, students were asked to complete the tasks by stirring the screen with the index finger of the dominant hand. There was a distance of 25 cm between the participant and the screen.
Motor Screening Task
The Motor Screening Task (MOT) is a simple reaction time test; it measures the psychomotor functions, speed, and accuracy. The MOT is an essential test of fine and gross motor skills appraised in a visuomotor accuracy-tracking task (Geertsen et al., 2016). It is vital for global understanding abilities, mainly the attention and information on the sensorimotor function or comprehension (Cercel et al., 2014). It provides a general assessment of sensorimotor deficits or lack of comprehension and measures the person’s response time to a visual stimulus. Fine and gross motor skills are highly essential in managing the routine activities in everyday life; these skills are linked to objective performance with higher cognitive functions (Geertsen et al., 2016).
Spatial Working Memory Task
The Spatial Working Memory (SWM) task is a test of memory retention and visuospatial information (Deniz et al., 2017). This test is essential to measure the working memory for spatial stimuli and requires the subject to use prompt reminding information to work toward the objective. A number of boxes appear each time, the task requires the participant to press the boxes until he finds the token inside each one; the token moves from one box to another and never appears in any box twice. Elimination by the subject is required until the token is found in each box.
Statistical Analysis
Statistical analysis was conducted using the Statistical Package for Social Sciences (SPSS for Windows, version 21.0). Independent t-test was used to compare the differences in the mean values of the two quantitative variables. The effect size was measured using Cohen’s d formula, and statistical significance was set at p < .05.
Results
In School 1, students were exposed to RF-EMF produced by MPBSTs at 2.010 µW/cm2 at a frequency of 925 MHz for 6 hr a day, 5 days a week. Although in School 2, students were exposed to RF-EMF of 10.021 µW/cm2 at a frequency of 925 MHz for 6 hr a day, 5 days a week for a total period of 2 years (Table 2). In School 1 group, students’ age range was 13–16 years (mean age 14.25 ± 0.98), while in School 2, it was 13–16 years (14.10 ± 1.01; Table 1) .
Anthropometric Variables of Students in Both Schools.

Note. Values are expressed in mean ± SD. RF-EMF = radio frequency electromagnetic field; SD = standard deviation.
MOT and SWM tasks were recorded; the MOT results are expressed as the standard score of mean latency (MOT ML). There was a statistically significant impairment in the MOT ML (806.99 ± 136.28 vs. 849.53 ± 160.14; p = .036) and SWM task (37.29 ± 3.14 vs. 36.40 ± 3.22; p = .043) among students who were exposed to high RF-EMFR generated by MPBSTs (School 2) compared to students who were exposed to low levels of RF-EMFR (School 1; Table 2). Cohen’s d for MOT ML was 0.28 and for SWM strategy was .27; it shows small effect of RF-EMF produced by MPBSTs on cognitive function impairment.
Comparison of the Cognitive Function Between Students Who Were Exposed to RF-EMF at 2.010 µW/cm2 Versus Students Who Were Exposed to RF-EMF Generated by MPBSTs at 10.021 µW/cm2.
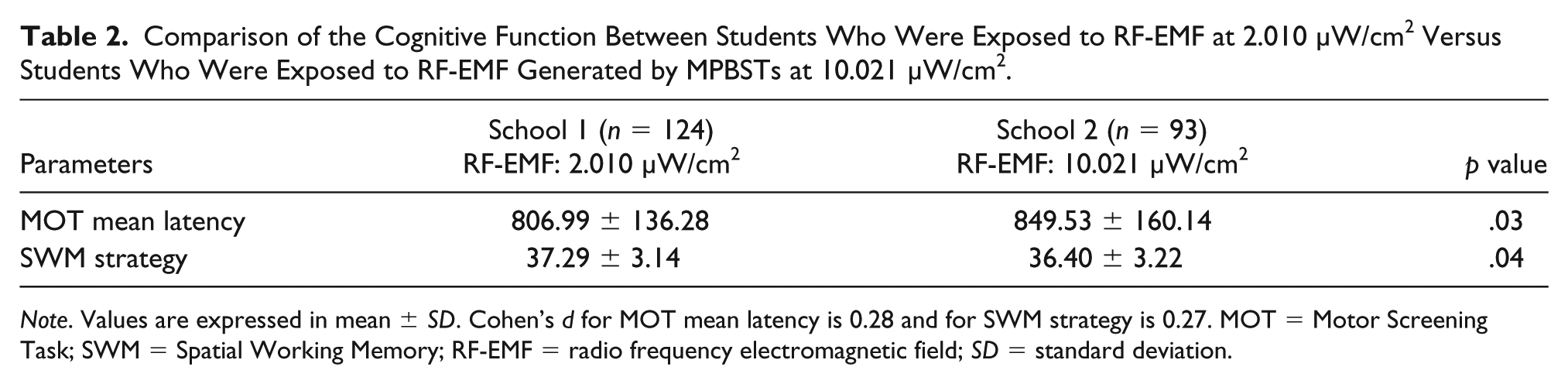
Note. Values are expressed in mean ± SD. Cohen’s d for MOT mean latency is 0.28 and for SWM strategy is 0.27. MOT = Motor Screening Task; SWM = Spatial Working Memory; RF-EMF = radio frequency electromagnetic field; SD = standard deviation.
Discussion
The RF-EMF radiations are the waves emitted from MPBSTs. The occurrence of RF-EMFR changes rapidly with distance and they scattered in different directions toward the ground (Buckus et al., 2017). The RF-EMFR carry non-ionizing radiations, known to have biological effects on human health (Hardell, Carlberg, & Hedendahl, 2018). The present study identified a decrease in fine and gross motor skills, spatial working memory, and attention among school children who had been exposed to high RF-EMF compared to students who had been exposed to low RF-EMF.
Singh et al. (2016) investigated the RF-EMFR generated by MPBSTs and its impact on the public health of people who lived close to the MPBSTs. The authors reported that majority of the subjects who were living adjacent to the MPBSTs complained about cardiovascular and nervous system associated clinical symptoms including headache, sleep disturbances, dizziness, difficulties in concentration, and high blood pressure, when compared to the control subjects.
In agreement with present study findings, researchers established a link between high exposure to RF-EMF and cognitive function (Calvente et al., 2016). The study outcome demonstrates a positive link between exposure to RF-EMF and decline in cognitive function. Children who were exposed to high levels of RF-EMF had lower cognitive scores for verbal expression and comprehension in comparison to those living in areas with lower exposure. They also identified that exposure to RF-EMFR has a negative impact on cognitive and behavioral development in children. Similarly, Thomas et al. (2010) reported a significant decrease in response time in adolescents who were involved in using mobile phones for long durations.
Contradictory to present study findings, Malek, Rani, Rahim, and Omar (2015), Haarala, Björnberg, Ek, Laine, Revonsuo, and Koivisto (2003), and Riddervold et al. (2008) reported no impact of RF-EMF exposure generated from MPBSTs on human cognitive function. The most probable reason for this contradiction is the determination of acute effect in a very limited time period. However, in the current study, the students were exposed to 6 hr a day, 5 days a week for a total period of 2 years.
Abdel-Rassoul et al. (2007) performed a study on inhabitants living near the MPBSTs. The exposed people experienced a considerable increase in neuropsychiatric symptoms including headache, dizziness, sleep disturbance, depressive feelings, and memory changes compared to those in the control group. The exposed inhabitants exhibited a decreased performance in attention and short-term memory tests. Silva, Barros, Almeida, and Rêgo (2015) demonstrated an association between anxiety and depression in individuals who live 100–200 m closer to MPBSTs compared to subjects living 300 m away from MPBSTs. Augner and Hacker (2009) reported that closer the distance to the MPBSTs, greater the radiation and higher the percentage of somatization, anxiety, and phobic nervousness in individuals living near MPBSTs. Kalafatakis, Bekiaridis-Moschou, Gkioka, and Tsolaki (2017) identified that mobile phone use has a significant negative impact on the working memory performance of people. The current study findings are in agreement with the results found by Abdel-Rassoul et al. (2007) and Kalafatakis et al. (2017).
Saikhedkar et al. (2014) determined the effects of mobile phone radiation on cognitive performances mainly on learning and memory. Their study findings indicate significant changes in behavior and poor learning in the exposed group as compared to the control group. These study findings agree with the present study findings that high exposure to RF-EMF produced by MPBSTs is associated with a decline in the fine and gross motor skills and spatial working memory and attention in the school adolescents who had been exposed to high RF-EMF compared to the students who had been exposed to low RF-EMF.
The potential reasons behind cognitive functions impairment in subjects exposed to RF-EMF radiation from MPBSTs are sleep disturbances, behavioral problems (Hardell et al., 2018), reduced regional cerebral blood flow (Hossman & Herman, 2003; Huber et al., 2002), myelin sheath damage (Kim, Yu, et al., 2017), and neuronal function impairment (Kim, Kim, et al., 2017). RF-EMF radiation may result in these mechanisms associated with neurological functioning resulting in cognitive impairment.
Strengths and Limitations
We took considerable efforts to adjust the relevant confounding factors; still there might be some residual confounding. This study has a relatively reasonable sample size, well-established research methodology, exclusion criteria, reliable tools used to measure the RF-EMFR, and minimized confounding factors (Meo et al., 2015). The recruitment of the male gender only is the limitation of this study due to the rules and regulations in Saudi Arabia that do not allow co-education systems in schools or universities. Students whose residences were adjacent to high power lines or MPBSTs and students who commonly used and kept cordless phones and Wi-Fi devices in their bedrooms were excluded from the study. There may be chances of exposure to RF-EMF generated from other sources such as television, remote devices, and wireless networks.
Conclusions
Despite the limitation of this cross-sectional study, it is identified that high exposure to RF-EMF produced by MPBSTs is associated with a decrease in fine and gross motor skills and spatial working memory and attention in school adolescents compared to students who had been exposed to low RF-EMF. This study provides cognizance to society and stakeholders in health care about the health hazards of RF-EMF produced from MPBSTs. No one can deny the facilities that are being provided by the telecommunication industry, but it is believed that nothing should be compromised over health. MPBSTs must be installed away from thickly populated residential zones particularly in or near the school buildings or there must be some system to shield human beings from RF-EMFR.
Footnotes
Acknowledgements
The authors are thankful to the Deanship of Scientific Research, King Saud University, Riyadh, Saudi Arabia for supporting the work through research group project (RGP-VPP 181). We also thankful to Dr. Shahid Bashir, Department of Physiology, College of Medicine, KSU for providing cognitive function lab facilities for data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Deanship of Scientific Research, King Saud University, Riyadh, Saudi Arabia (RGP-VPP 181).