
Abstract
Purpose
This study investigated the effects of an interactive multitouch game-based cognitive intervention (ICI) on cognitive function in community-dwelling older adults.
Methods
Thirty-two older adults (19 women) between 65 and 84 years of age (mean age, 74.47 ± 4.30 years) without a history of neurological disease participated. They were randomized into two groups: intervention and control. The intervention group took part in ICI sessions using HAPPYTABLE® (Spring Soft Co. Ltd, Seoul, Korea) (ICI group), and the control group underwent a traditional paper-and-pencil-based cognitive intervention (TCI group). Both groups completed 10 intervention sessions over four consecutive weeks. Cognitive function was assessed before (pre-intervention) and after (post-intervention) intervention. Executive function was evaluated through the Color-Word Stroop Test (CWST) and Controlled Oral Word Association Test (COWAT). Memory was assessed through the Verbal Learning Test (VLT) and Rey Complex Figure Test (RCFT).
Results
The ICI and TCI groups showed significant improvements in some cognitive functions after the intervention. Both groups showed substantial improvements in VLT and RCFT (P < 0.05), reflecting memory function. Regarding the executive role, the ICI group showed significant post-intervention improvements in the conditions of the CWST incongruent (ICI 76.31 ± 23.82; P = 0.004) compared to the pre-intervention scores. ANCOVA with pre-intervention scores and gender as covariates revealed improved results in the ICI group compared with the VLT delayed (ICI 9.18 ± 1.68, TCI 7.56 ± 2.13; P = 0.015) and VLT recognition task (ICI 22.81 ± 1.22, TCI 21.38 ± 1.09; P = 0.035).
Conclusions
These findings revealed that both ICI and TCI helped increase cognitive performance in community-dwelling older persons; nevertheless, ICI showed better improvement in memory function than TCI. Thus, the ICI can be used to improve cognitive performance among older adults living in the community.
Keywords
Introduction
An increasing older adult population from extended life expectancy is a global phenomenon. 1 The average percentage of the world's population aged 65 years or older is expected to be 11.7% by 2030, surpassing 16% by 2050. 1 With age, degenerative changes in the brain reduce memory and other cognitive functions. Therefore, as the older adult population grows, so does the number of older adults with cognitive impairment. A previous study found that the older the population, the higher the rate of decrease in cognitive function. 2 Cognitive functions can be divided into four basic categories: memory, including retention, storage, and recall of information, is highly associated with dementia in the case of older people. 3 Executive function is a multi-faceted construct including attention, organizing, abstract thinking and problem-solving, self-regulation, and motor control and relates to a range of higher-level cognitive processes. 4 Executive function is the essential cognitive ability to adapt to novel situations and solve problems by combining knowledge. Attention, a fundamental building block of cognition and crucial to many mental tasks, refers to the ability to process information rapidly, which becomes increasingly limited with age.5,6 Visuospatial function is the ability to perceive visual and spatial connections among things in daily tasks such as driving, using a map, and playing sports.7,8
There is a range of cognitive decline between healthy cognition and dementia. Mild cognitive impairment (MCI) is the most common condition on this spectrum and is defined as cognitive decline greater than predicted for an individual's age and education level but does not significantly interfere with everyday activities. 9 At this stage, impaired memory and executive function deficiencies are common, including those of working memory and cognitive flexibility. 9 Older persons with pre-MCI might perceive minor cognitive changes that cannot be detected clinically, resulting in a subjective sense of cognitive decline, which may be one of the first indications of MCI. 10
Consequently, the social burden of supporting the older adult population continues to increase as the capacity of older adults to manage the physical, mental, and daily aspects of life deteriorates. 11 Early recognition of cognitive decline and early management to prevent dementia are critical social issues for the well-being of older adults and the minimization of social costs. Alzheimer's disease affects over 50 million people globally, with roughly 10 million new cases diagnosed each year. It is the most prevalent dementia, accounting for 60–70% of all such cases. 12 A previous meta-analysis 8 looked at the impact of cognitive-based training on healthy-aged people. It indicated that cognitive training could modulate the general cognitive function and executive function while having little effect on memory, attention, or visuospatial skills in older individuals. Therefore, cognitive intervention is a form of rehabilitation that combines personalized life skill interventions with drills and practice to strengthen the cognitive skills required to perform various daily tasks.13–15
Computerized cognitive training (CCT) is commonly used for cognitive interventions and is adjunct to other protocols designed to improve everyday functioning. 16 Traditional paper-and-pencil tasks require face-to-face contact, which involves setting a meeting location, coordinating schedules, and travel time. 6 Compared with traditional cognitive training, computerized cognitive interventions positively affect cognitive function through attractive and repeated exercises that can be accessed anywhere without time constraints or the need for a skilled instructor. 17 Moreover, CCTs with domain-specific gamified tasks can produce a sense of immersion through visual and auditory effects. 6 Participants can enjoy various games according to their skill level, and their performance can be monitored in real time. Participants receive instant feedback and auditory rewards, and their skills can be recorded and represented with graphical charts to increase participation and immersion.6,18
Previous research has demonstrated that training older individuals in certain working memory tasks for a short period of time (e.g., 10 days, 5 weeks, or 3 months) can significantly enhance behavioral performance in trained or untrained working memory tasks.19,20 Recent research has found that multi-domain cognitive training such as an aging education program or lecture or watching a DVD can improve memory function relative to no intervention and executive functions relative to healthy older adults.21,22
Although emerging data suggest that digital game playing can improve cognitive function in older adults,23,24 the results are inconclusive. Whether computerized cognitive intervention is more effective than traditional paper-and-pencil tasks is controversial. A Cochran review 25 did not determine whether CCT with gamified tasks affects global cognitive function, episodic memory, processing speed, executive function, or working memory more than the active control of watching educational videos or playing computer games without a training component. The author of that review suggests that the short 3-month intervention may be a limitation of previous studies. A systematic review study that evaluates the effectiveness of randomized controlled trials of CCT on cognitive outcomes suggested that gamified tasks can slightly improve episodic memory but might have little or no effect on executive function, working memory, and verbal fluency.6,14 A meta-analysis showed that gamified CCT tasks improved motivation and engagement compared to non-gamified tasks. However, no effects were related to the training domain. 26 Study results have been diverse due to different design characteristics (group-based training or home-based training14,27) and types of training (gamified or non-gamified task, 26 CCT or active control6,28), making it difficult to draw definite conclusions.
In this study, we examined the impact of an interactive multitouch game-based cognitive intervention (ICI), a gamified computerized cognitive intervention, on cognitive function in older persons living in the community. Paper-and-pencil tasks were employed to compare the outcomes of a traditional cognitive intervention (TCI). We hypothesized that both ICI and TCI would help the participants but that the ICI group would have more significant gains in memory and executive function.
Materials and methods
Participants
Thirty-two older adults between 65 and 84 years of age with no history of neurological diseases participated. The exclusion criteria were (1) fewer than 10 points on the Korean Mini-Mental State Examination (K-MMSE), (2) severe mental illness, (3) impairment of vision, and (4) limitations in upper extremity ranges of motion that could affect task performance. The Institutional Review Board (IRB) of Samsung Medical Center, Seoul, Korea, approved this study procedure (IRB no. 2020-08-147; clinical trial no. NCT04873843), and all participants provided a signed informed consent before participating in the study.
Sample size estimation
We calculated the sample size using Lehr's formula. 29 According to a previous study, we set a clinically significant difference of 4.5 points for the CWST. 30 We used a two-sample, two-sided t-test of mean difference, a power of 80%, and a significance level of 5%. As a result, 32 subjects (16 experimental and 16 control) were identified as an appropriate minimum sample size. To allow for a dropout rate of 20%, a total of 38 participants were included.
Procedure
To assess the effects of the ICI on older adult subjects, we used a single-blind, randomized, and controlled intervention. Subjects were randomly assigned to the ICI or TCI group (https://www.randomization.com). The groups underwent cognitive training for 40 min per day, three times per week, for four consecutive weeks, for 12 full sessions. Participants were asked to attend two or three sessions a week for each group, each of which involved four exercises. Each task combination lasted around 40 min, with 10 min per game. An overview of the structure of both interventions, with examples of the exercises, is given in Table 1. To assess the effectiveness of each cognitive intervention, we administered comprehensive neuropsychological tests to both the intervention and control groups at baseline before the intervention (pre) and after the intervention (post). Adherence was calculated as the percentage of intervention sessions attended.
Description of interactive multitouch game-based cognitive intervention (ICI) and traditional paper-and-pencil-based cognitive intervention (TCI) components.

Abbreviations: ICI, interactive multitouch game-based cognitive intervention; TCI, traditional paper-and-pencil-based cognitive intervention.
Interventions
The types of interventions used for the experimental and control groups were cognitive training. The ICI group played 12 games during the cognitive intervention sessions. Each task was designed to train in one or more cognitive areas (attention, visuospatial skills, memory, language, and executive function). Tasks were organized from low to high levels in each intervention session. The ICI used HAPPYTABLE®, designed by Spring Soft Co. Ltd (Seoul, Korea), to deliver interactive, computerized, cognitive intervention with gamified tasks to community-dwelling older adults. This system is operable on a multitouch screen over a rectangular table, and four subjects can play together (shown in Figure 1). The playful exercise tasks involve basic information processing parameters and memory and require various types of decision-making. We chose 12 games that target the major cognitive domains of attention, visuospatial skills, memory, language, and executive function (Table 1). Each game had different difficulty levels, and all participants in a group of 4 played at the same difficulty level due to the game's characteristics, where several players can be co-located and collaborative.
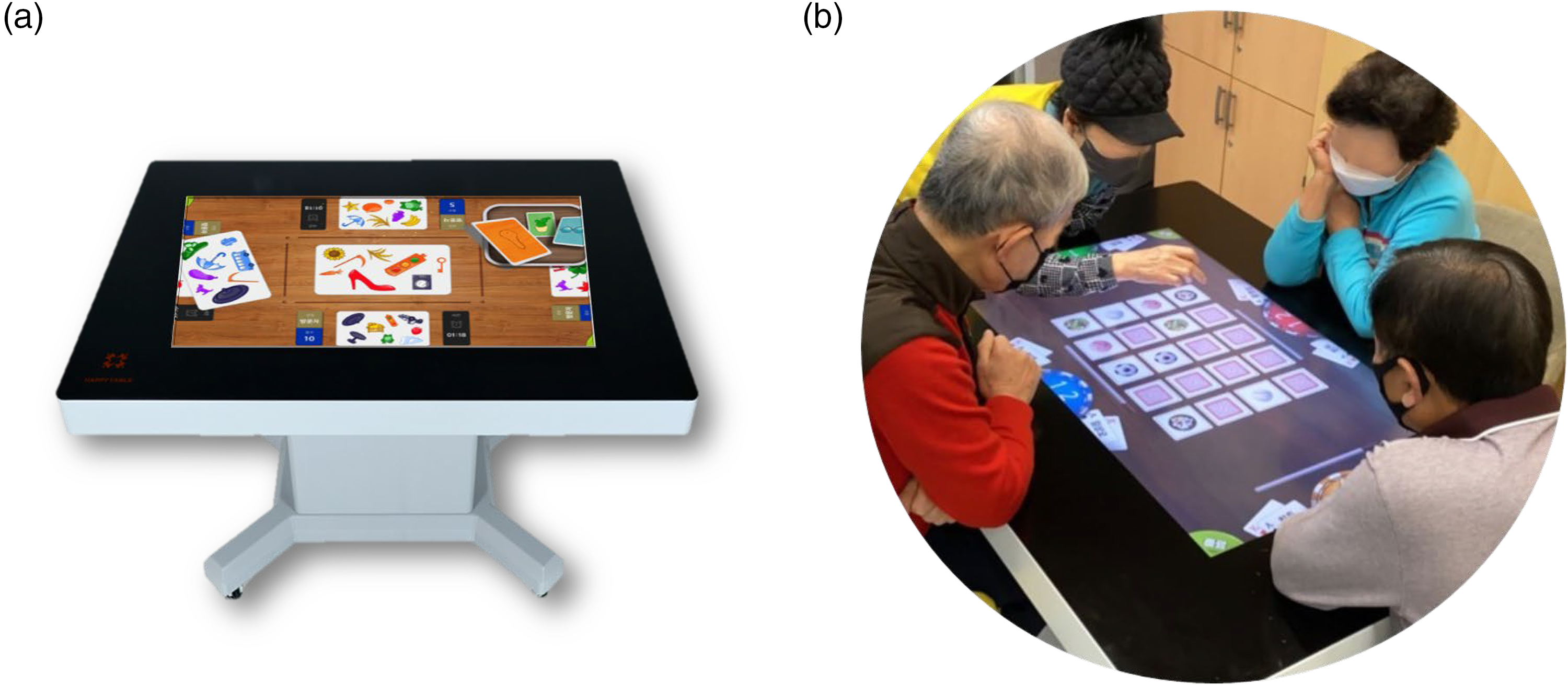
(a) HAPPYTABLE®, an interactive multitouch table with gamified tasks designed by Spring Soft Co. Ltd. (Seoul, Korea) and (b) interactive multitouch game-based cognitive intervention sessions.
The TCI group also performed 12 cognitive intervention sessions over 4 weeks. Four people participated in each session and performed paper-and-pencil tasks. Each task included training in one or more cognitive areas organized from low to high levels in each intervention session. However, each individual performed the given tasks independently without interaction among participants. The TCI consisted of cognitive stimulation programs and leisure activities commonly used in existing facilities for older adults, such as community welfare centers. 31 Nine cognitive tasks were chosen: mosaic, maze, finding the hidden picture, origami, spotting the difference, tangram, connecting the dots, coloring, and transcribing activities targeting the major cognitive domains (Table 1).32–34
Outcome assessments
We performed the following assessments before intervention (pre) and immediately after intervention (post). During outcome measurements, the examiners were blinded to the participant group.
Attention and memory function
Digit span test forward and backward (DST)
The DST is a simple neuropsychological test that measures attention and consists of two parts, forward and backward. In the forward task, participants repeat numbers in the order that they hear them. In the backward part, they repeat the numbers in the reverse order.35,36
Verbal Learning Test (VLT)
The VLT evaluates verbal learning and memory skills. It consists of 12-word lists with four words each from the three most used semantic categories. After these words are spoken to the patient, the participants must repeat them immediately. This process is repeated three times. After that, the participants perform immediate recall twice more, delayed recall after 20 min, and recognition recall at the end of the assessment. 37
Rey Complex Figure Test (RCFT)
The participants are asked to copy a complex and nonsymmetrical geometric figure as accurately as possible, and after 3 minutes, without previous warning, the immediate recall task is implemented. The delayed recall task is performed 20 min after the copy trial and is followed by the recognition recall trial. 38
Executive function
Color-Word Stroop Test (CWST)
The CWST assesses executive processing abilities in general. There are two kinds of tasks: reading color names printed in black ink and naming the colors of words rather than reading the words. The CWST protocol was used to determine the number of correct answers and errors, as well as response times.39,40
Controlled Oral Word Association Test (COWAT)
The COWAT is an oral fluency test in which participants must make verbal associations to various letters of the alphabet (phonemic fluency test) or categories, such as animals and supermarkets (semantic fluency test), by saying all the appropriate words they can remember.41,42 The Korean version of controlled oral word association test test requires participants to create as many category-specific words as they can in 1 min. It consists of two parts: phonemic and semantic fluency (words beginning with “ㄱ,” “ㅇ,” and “ㅅ”). 42
Go/No-Go Test
The Go/No-Go test examines set-shifting ability. 43 In this test, when the examiner raises only the second finger, the patient raises the second and third fingers, and when the examiner raises the second and third fingers, the patient makes a fist (don’t raise a finger).
Trail Making Test (TMT)
The TMT is divided into two parts, A and B. In TMT Part A, participants are given a piece of paper with randomly numbered circles on it and are asked to draw lines connecting the numbers in an ascending order. The circles in TMT Part B contain numbers and letters (1-A, 2-B, and so on). Each participant's time to complete each trial was recorded. 44
Statistical analysis
All statistical analyses were performed using the Statistical Package for Social Sciences version 22.0 (SPSS Inc., Chicago, IL, USA). Results were calculated as the mean and standard deviation (mean ± SD).
A covariance (ANCOVA) analysis with pre-intervention scores and gender as covariates was used to compare post-intervention scores between the ICI and TCI groups.
Additionally, a t-test was used to compare post-intervention scores within the ICI and TCI groups. It was also used to compare the difference between the immediate and delayed recall trials of the RCFT and between the immediate and delayed recall trials of VLT and COWAT for both groups. P < 0.05 was considered statistically significant.
Results
Participants were enrolled between 15 September 2021 and 8 December 2021, with the final follow-up completed on 3 January 2022. We screened 36 participants for eligibility, of which 34 were assessed in screening and randomized into the ICI and TCI groups. Two refused to participate before the intervention started (intervention 1, control 1) due to the difficulty of visiting three times a week. Therefore, 16 subjects in the ICI group and 16 in the TCI group completed the intervention (Figure 2). The compliance rate for this study was 100%.

Flow diagram of participant inclusion.
Demographic characteristics at baseline
Participant demographic characteristics at baseline are presented in Table 2. Among the 32 community-dwelling older adults who participated, 19 were women, and their mean age was 74.5 ± 4.3 years. Only gender differed between the ICI and TCI groups at baseline (male; ICI 62.5%, TCI 18.75%; P = 0.011). Because of this gender difference, pre-intervention and gender were used as covariates to compare post-intervention scores between the ICI and TCI groups.
Demographic characteristics of the ICI group and TCI group.

Continuous values are presented as mean (standard deviation).
Abbreviations: ICI, interactive multitouch game-based cognitive intervention; TCI, traditional paper-and-pencil-based cognitive intervention; K-MMSE, Korea Mini-Mental State Examination.
*P < .05, **P < .01.
Attention
There was no significant difference in DST forward (ICI 6.38 ± 1.67, TCI 5.25 ± 1.34; P = 0.690) or backward (ICI 4.63 ± 1.59, TCI 3.69 ± 1.01; P = 0.358) in both ICI and TCI groups (Table 3).
Effect of the interactive multitouch game-based cognitive intervention and traditional cognitive interventions on cognitive function.

Abbreviations: ICI, interactive multitouch game-based cognitive intervention; TCI, traditional paper-and-pencil-based cognitive intervention; DST, digit span test; VLT, Verbal Learning Test; RCFT, Rey Complex Figure Test; CWST, Color-Word Stroop Test; COWAT, Controlled Oral Word Association Test; TMT, Trail Making Test.
Continuous values are presented as mean (standard deviation). aP-values obtained using the paired sample t-test or Wilcoxon signed rank test. bP-values obtained using analysis of covariance (ANCOVA).
*P < .05, **P < .01.
Memory
In the within-group comparisons from pre- to post-intervention shown in Table 3, both groups showed significant improvements in VLT immediate (ICI pre 22.13 ± 5.20, post 27.94 ± 4.36; P = 0.000, TCI pre 20.75 ± 5.32, post 25.56 ± 2.78; P = 0.001), VLT delayed recall (ICI pre 7.44 ± 2.50, post 9.81 ± 1.68; P = 0.001, TCI pre 5.50 ± 2.68, post 7.56 ± 2.13; P = 0.005), RCFT immediate (ICI pre 13.84 ± 5.72, post 16.59 ± 6.33; P = 0.013, TCI pre 7.13 ± 4.93, post 10.44 ± 4.83; P = 0.001), and RCFT delayed recall (ICI pre 13.91 ± 5.49, post 17.25 ± 5.87; P = 0.001, TCI pre 7.31 ± 4.70, post 11.06 ± 4.78; P = 0.001) tasks.
The ANCOVA was performed controlling for gender and pre-intervention scores as covariates to determine the between-group difference. The ICI group showed significant results on memory function in the VLT delayed task (ICI 9.18 ± 1.68, TCI post 7.56 ± 2.13; P = 0.015) and VLT recognition task (ICI 22.81 ± 1.22, TCI 21.38 ± 1.09; P = 0.035). No significant difference was found in executive function or attention between groups (Table 3).
Executive function
In the within-group comparisons from pre- to post-intervention shown in Table 3, the ICI group showed enhanced training benefits on incongruent CWST (ICI 76.31 ± 23.82, 89.06 ± 19.81; P = 0.003) and phonemic words on COWAT (ICI 23.44 ± 8.91, 28.88 ± 7.67; P = 0.004). The TCI group showed improvement on the Go/No-Go (TCI 16.06 ± 3.51, 17.88 ± 2.06; P = 0.03) and TMT Part A tasks (TCI 26.17 ± 5.98, 22.75 ± 5.62; P = 0.02). The CWST showed the most promising results between groups. The ICI group scored significantly higher in the incongruent (ICI 76.31 ± 23.82; P = 0.004) but not congruent trials of the CWST task, with an effect size of d = 0.44 (Table 3). Although no significant between-group differences were found in other working memory and executive function tasks, ANCOVA was performed to adjust for pre-intervention scores of DST, CWST, and TMT Part A as covariates.
Discussion
In this study, we investigated the effect of ICI on cognitive function in community-dwelling older adult subjects and compared the results with those of the TCI group. After 10 training sessions, both groups demonstrated improvements in some cognitive domains, indicating that both interventions were effective in older adults. Compared to the TCI group, the ICI group showed better memory function.
Cognitive function, or the ability to conduct mental processes related to problem-solving and learning, is a necessary component of independent living. 45 Memory loss is one of the most prevalent neurological symptoms among older adults. The results of this study are consistent with previous research on the impact of CCT with gamified tasks on the memory capacity of older adults.26,46,47 According to meta-analyses, cognitive training, particularly memory training, may be an effective intervention method for maintaining or increasing cognitive abilities in older persons.26,46,48 The ICI's more significant impact on memory function in older individuals appears to be attributable to its capacity to provide multisensory stimulation, social engagement, and the opportunity to reference the rules of the game regularly.
Cognitive and multisensory stimulation is a dementia intervention that offers a variety of activities to provide general stimulation of thinking, concentration, and memory and often is performed in a social setting, such as a small group. Multisensory cognitive interventions have been implemented in older adults with and without dementia, and the findings have shown benefits on anxiety, overall dementia severity, and neuropsychiatric symptoms. 49 These findings highlight the potential of multimodal treatments for cognitive training, particularly in older adults, and support for ICI as a strategy.
Previous research has suggested a connection between social interaction and cognitive function. In a meta-analysis of memory training in older adults, group-based administration was revealed to be a moderating effect. 50 Frequent social interactions are also associated with improved memory function.51,52 As part of group-based training, participants recall and manage their memories and specify the memories they want to share with others. They debate against the memory displayed by other members and agree on the remembered data. 53 Unlike the ICI group, the TCI group completed activities without interacting with others. Their interest in the exercise was not stimulated by repeated feedback from other participants, as in the ICI group.
Executive function drives the capacity to plan and carry out an action, inhibit an inappropriate activity or thought, organize thoughts, and encode and retrieve information. 4 In this study, we chose executive function (e.g., CWST) as a primary outcome to analyze ICI task characteristics, which encouraged personal interaction and problem-solving. As a result, the CWST incongruent score changed significantly in the within-group comparisons but did not differ in the between-group comparisons. The significant within-group intervention effect on the CWST in the ICI group reflected accurate CWST incongruent and COWAT phonemic scores. Still, the effect size was insufficient to produce a between-group difference.
Previous research has shown executive function benefits of multi-domain cognitive training with active controls (education program or lecture, exercise intervention) for healthy older adults.21,22 Another study with computerized cognitive intervention showed stronger effects on executive function after long-term CCT. 54 Because our research compared only the short-term effects of group-based interactive computerized and traditional cognitive interventions, an extended intervention period might verify the effect of ICI on executive function.
High heterogeneity may have influenced several aggregated outcomes, particularly for executive function. The primary reason was that numerous computerized activities were used in eligible research. We used 12 games for ICI and nine paper-and-pencil tasks for TCI during the 12 sessions of 40-min training three times a week for 4 weeks. The exercises included simple coloring activities and complex logical thinking requiring multisensory and nonverbal reasoning. Thus, providing enough time to gain experience and become familiar with tasks seems necessary to experience the benefits of a computerized gamified task.
Recently, a survey indicated that 61% of those 65 and older own a digital device and 44% of respondents aged 60 and older play games regularly.45,46 However, a previous study showed that even when games are adapted to accommodate common age-related changes, players can experience difficulties engaging with game activities. 47 According to the principles of andragogy, older adults must have a self-concept and experience with the platform used to experience immersion in a digital game. 48 In this study, the time available for older adults to become familiar with the game's rules was relatively short.
This study had several other limitations. First, our participants had high average MMSE scores (27.4 ± 1.9); therefore, the ceiling effect on general cognitive function cannot be ruled out. Second, although corrections were made, the randomization number was small; therefore, the results do not represent the general older adult population. Third, since the ICI uses computers to deliver the intervention with more complex visual and auditory stimulation than TCI, which usually incorporates face-to-face contact with paper-and-pencil-based tasks, assessment indicators related to the characteristics of each intervention should be added in future studies.
Conclusion
These findings revealed that both ICI and TCI helped increase cognitive performance in community-dwelling older persons, although the benefits of ICI on cognitive and memory function were more significant than those of TCI. Thus, the ICI can be recommended to improve cognitive performance among older adults living in the community. Future studies should examine the differential effectiveness of the ICI on older adults with lower cognitive function or those with mild cognitive impairment (MCI).
Footnotes
Acknowledgments
We would like to thank the Neuroplasticity, Neurorehabilitation, and Imaging laboratory members for their assistance. We would also like to thank all participants for their time, dedication, and enthusiasm.
Contributorship
Y-HK and JL contributed to the design and conceptualization of the study. DR and GL contributed to the data collection and data analysis. DR contributed to the drafting of the manuscript. JL, SS, and GL contributed to the revisions of the manuscript. DR, JL, SS, GL, and Y-HK contributed to the interpretation of data, critical revision of the manuscript for important intellectual content, and final approval of the version of the manuscript to be submitted.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The Institutional Review Board (IRB) of Samsung Medical Center, Seoul, Korea, approved this study procedure (IRB no. 2020-08-147; clinical trial no. NCT04873843).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Samsung Medical Center (PHO021185) and the Ministry of Science and ICT, Korea, under the ICT Creative Consilience program (IITP-2021-2020-0-01821) supervised by the Institute for Information & Communications Technology Planning & Evaluation, and the Korea Medical Device Development Fund grant funded by the Korean government (the Ministry of Science and ICT; the Ministry of Trade, Industry and Energy; the Ministry of Health & Welfare; the Ministry of Food and Drug Safety) (KMDF-RS-2022-00140478).
Guarantor
DR.