
Abstract
The objective of this study was to identify the association between gender norms and family planning practices among men in Western Jamaica. A cross-sectional survey of 549 men aged 19 to 54 years attending or visiting four government-operated hospitals was conducted in 2011. Logistic regression models were used to identify factors associated with taking steps to prevent unwanted pregnancy, intention to have a large family size (three or more children), and fathering children with multiple women. Adjusted odds ratios (AORs) and 95% confidence intervals (CIs) were calculated from the models. Reduced odds for taking steps to prevent unwanted pregnancy among men with moderate (AOR = 0.5; 95% CI = 0.3-0.8) and high (AOR = 0.3; 95% CI = 0.1-0.6) support for inequitable gender norms was observed. Desiring large family size was associated with moderate (AOR = 2.0; 95% CI = 1.3-2.5) and high (AOR = 2.6; 95% CI = 1.5-4.3) support for macho scores. For men with two or more children (41%), there were increased odds of fathering children with multiple women among those who had moderate (AOR = 2.1; 95% CI = 1.0-4.4) and high (AOR = 2.4; 95% CI = 1.1-5.6) support for masculinity norms. Support for inequitable gender norms was associated with reduced odds of taking steps to prevent unwanted pregnancy, while support for masculinity norms was associated with desiring a large family size and fathering children with multiple women. These findings highlight the importance of including men and gender norms in family planning programs in Jamaica.
Introduction
The importance of integrating gender transformative approachesinto sexual and reproductive health programs is well documented in the literature (Collumbien & Hawkes, 2000; Dworkin, Treves-Kagan, & Lippman, 2013; Hawkes & Hart, 2000(Adams, Salazar, & Lundgren, 2013)). However, much of the work in this area has primarily focused on sexual health, especially in HIV prevention and intimate partner violence, rather than on family planning (Nanda, Schuler, & Lenzi, 2013(Dworkin, Treves-Kagan, & Lippman, 2013)). Masculinity and inequitable gender norms have been reported to influence family planning practices such as involvement in contraception use, responsible fatherhood, desired family size, gender preference for children, and socialization of male children (Onyango, Owoko, & Oguttu, 2010). Gender norms, as defined by the World Health Organization, are social expectations of appropriate roles and behaviors for males and females, as well as the social reproduction of these norms in institutions and cultural practices (Pulerwitz & Barker, 2008; World Health Organization, 2007). These socially constructed roles of expected behaviors for males and females (Zhu et al., 2012), which vary in different societies, can negatively affect family planning programs and health outcomes among women and children (Gutierrez, Bertozzi, Conde-Glez, & Sanchez-Aleman, 2006; Kabagenyi, Ndugga, Wandera, & Kwagala, 2014; Mantell et al., 2009). In many patriarchal societies, women are expected to be naive about sex, which limits their ability to be informed about sex and increase their vulnerability to unwanted pregnancies (Ampofo, 2001). Additionally, these societies support men’s dominance and authority over economic resources in the family (Ampofo, 2001). This further challenges women’s ability to negotiate safer sex and take measures to prevent unwanted pregnancy due to high dependence on men for economic support. Thus, the common practice of focusing solely on women in matters pertaining to sexual and reproductive health is often ineffective as men often control the resources and decision making in relationships (Sternberg & Hubley, 2004; Zhu et al., 2012). Involving men as partners in family planning programs is critical to reducing unwanted pregnancies, improving parenting skills, and increasing knowledge on sexual and reproductive health among men (Ali, Rizwan, & Ushijima, 2004; Berhane et al., 2011; Mistik, Nacar, Mazicioglu, & Cetinkaya, 2003; Ndong, Steele, & Mahony, 1998). However, integrating men and gender norms in family planning programs have proven to be challenging as it is difficult to motivate men to participate in health programs that are traditionally designed for women and children. Furthermore, support for masculinity norms is associated with reduced likelihood of using health care facilities among men.
In Jamaica, perception of manhood has been reported to be associated with having multiple sexual partners and fathering children with multiple women (Figueroa et al., 2008). These behaviors among men which are intended to validate manhood and demonstrate to society that they are not homosexuals (P. Anderson, 2012; Chevannes, 2002; Chevannes & Mitchell-Kernan, 1992; Gibbison, 2007; Wyss, 2000) can undermine family planning programs. Forty percent of Jamaican women have been pregnant at least once by age 20 years (Crawford, McGrowder, & Crawford, 2009) and approximately 45% of Jamaican households are headed by females (Dreher & Hudgins, 2010). Furthermore, about 85% of Jamaican children are born out of wedlock (Dreher & Hudgins, 2010). This is higher than the estimated 70% premarital births in the Caribbean overall (Gray, Parkin, & Samms-Vaughan, 2007). In Jamaica, multiple sexual partners especially among males is very common (Crawford et al., 2009; Walcott et al., 2014(Figueroa et al., 2008; Morgan et al., 2012)), and the expressions “baby mother” and “baby father” are commonly used in the Jamaican society to refer to unmarried parents.
The purpose of this study was to determine the association between masculinity and inequitable gender norms and men family planning behaviors (involvement in contraception use, desire to have a large family [more than three children], and fathering children with multiple women).
Materials and Method
Study Design and Setting
A cross-sectional study was conducted among 549 men aged 19 to 54 years in Western Jamaica, during June to August 2011. The participants were recruited from the four government-operated hospitals within the Western Regional Health Authority (WRHA), as described elsewhere (Walcott et al., 2013). The WRHA has an estimated population of approximately 474,944 and consists of 4 parishes (St. James, Trelawny, Hanover, and Westmoreland). One hospital is located in each parish, each serving a wide cross-section of the population.
To estimate the potential effect of selection bias in recruiting from hospitals, a sample of 51 men was recruited from the community in the parish of St. James. The hospital sample was compared to the community sample with respect to attitude toward gender norms (Gender Equitable Men [GEM] and Macho scores), outcome variables (involvement in contraception use, fathering children with multiple women, and desire a large family), and key sociodemographic variables (age, income, and education). Men in the community sample tended to be older and desire larger families.
Ethical approval for the study was obtained from the institutional review board of the University of Alabama at Birmingham, the Advisory Panel of Ethics and Medico-Legal Affairs in the Jamaican Ministry of Health, and the WRHA.
Participants
To be eligible for participation in this study, men had to be 19 to 54 years old, live in the western region of Jamaica, and present at one of the four government-operated hospitals in the WRHA for outpatient care or as a visitor. Each study participant was given a phone card valued at $215 Jamaican dollars (equivalent to US$2.50) at the end of the interview. Men who worked at the hospitals or who were employed by the WRHA were not eligible to participate in this study.
Data Collection
Men who consented to participate in this study were interviewed by a member of the interview team (all females), at the participating hospitals. All members of the interview team were trained to reduce the effect of introducing bias into the study. Data were collected using a 143-item questionnaire, which was developed based on an extensive search of the literature. The parameters that were assessed included sexual behaviors, reproductive health practices, male circumcision, health-seeking behaviors, attitude toward gender norms, and sociodemographic factors. Two validated scales were included in the questionnaire: GEM and Macho. While there is some overlap between the constructs of the two scales, they measure distinct dimensions of gender norms. The GEM scale is mainly designed to evaluate men’s beliefs about the level of equality and inequality between men and women in relationships (Pulerwitz & Barker, 2008), whereas the Macho scale primarily measures men’s beliefs about ideals of manhood (how men define themselves as men) (Anderson, 2012).
The GEM scale (Pulerwitz & Barker, 2008) has been reported to be a culturally sensitive tool for measuring gender norms and has been used in a number of countries such as India, Kenya, Ethiopia, and Nicaragua (Pulerwitz, Michaelis, Verma, & Weiss, 2010). The scale measures dimensions of gender norms related to sexual behaviors (multiple sex partners and homosexuality), reproductive health, and violence against women (Pulerwitz & Barker, 2008; Pulerwitz et al., 2010). It consists of 24 items scored on a 3-point Likert-type scale (1 = agree, 2 = partially agree, 3 = disagree). Items 1 to 17 measure gender inequitable norms, whereas Items 18 to 24 measure gender equitable norms. Scores for the inequitable norms (maximum score 51) and equitable norms (maximum score 21) subscales were calculated separately. The Cronbach alpha for the “inequitable” and equitable subscales are .85 and .77, respectively (Pulerwitz & Barker, 2008). Scores were classified as “high,” “moderate,” and “low” by dividing the sum of the range of answers on the two subscales into three equal and separate parts as recommended by the author of the scale. For example, support for inequitable gender norms was classified as high (41-51), moderate (29-40), and low (17-28) (Pulerwitz & Barker, 2008).
The Macho scale was recently developed among fathers (18-59 years of age) residing in Jamaica, and it is designed to measure sexual dominance and virility and the primordial need to beget children (Anderson, 2012). The scale consists of 13 items (Cronbach’s α = .82) measuring three dimensions of masculinity: (1) primordial need to produce children, (2) sexual dominance (virility), and (3) domestic freedom. Items are scored using a Likert-type scale ranging from 1 to 5, resulting in a minimum score of 13 and a maximum of 65. Higher scores are indicative of higher levels of machismo (Anderson, 2012). As recommended by Anderson, scores were classified as “high,” “moderate,” and “low” by dividing the frequency distribution of the sample into tertiles.
In our sample, internal reliability as measured by Cronbach’s alpha for the inequitable GEM, equitable GEM, and Macho scales were 0.74, 0.32, and 0.74, respectively. Due to low reliability of the equitable GEM subscale, it was not used in any of the analyses.
The dependent variables used in this study were (1) involvement in contraception use, (2) desire to have a large family, and (3) fathering children with multiple women. Involvement in contraception use was determined by asking “Do you take any steps/measures to prevent your sexual partner (s) from getting pregnant? The responses were dichotomized as “yes” or “no.” Desire to have large family size was assessed by asking “How many children do you intend to have?” Men who expressed their intention to have a family size greater than the median desired number of children (three children) in our sample were classified as desiring a large family size. To determine the number of men who fathered children with multiple women, the participants were asked, “How many baby mothers do you have?” Men who reported more than one “baby mother” were classified as fathering children with multiple women. This analysis was restricted to the 224 men who had at least two children (all were aged 25 or older).
Other variables that were assessed in this study included sociodemographic factors, use of health care facilities, preferred gender for health care provider, and family planning knowledge.
Data Analysis
Bivariate and multivariable analyses were performed to obtain crude and adjusted estimates (odds ratios) of the association between gender normsand family planning practices (involvement in contraception use, desire to have large family, and “fathering children with multiple women”). Separate logistic regression models were used for each of the three family planning practices studied. Backward selection modeling was used in each. All predictive variables resulting in p < .10 in the crude analyses were entered in the adjusted models and retained if p < .05. The final models were adjusted for age, education, income, and religion, regardless of significance, as these characteristics are known to be associated, in general, with the outcomes. Data analysis was performed using SAS software version 9.2 (SAS Institute, Cary, NC).
Results
The mean age (± SD) of the 549 participants was 32.4 (±10.1) years. Most (64%) of the men fathered at least one biological child; 41% fathered two or more children. Of the latter, 64 % reported fathering children with multiple women. The mean age of fathering a first child was 23.4 ± 5.7 years. Almost 35% of the men desired a large family (more than 3 children). Most of the men were classified as having moderate or high support for masculinity (71%) and inequitable (74%) gender norms (Table 1).
Selected Characteristics of the Participants.

Note. SD = standard deviation.
Among 351 with men biological children.
Among 224 men with at least two biologic children.
Most (75%) of the men reported taking steps to prevent unwanted pregnancy. The steps taken to prevent unwanted pregnancy included consistent (40%) and inconsistent (22%) condom use, supporting a partner to use contraception (15%), and using the withdrawal method (13.7%). None reported ever having had a vasectomy. The median number of children the men desired to have was three, and 35% of the men desired to have a large family (more than 3 children). Among men with two or more children, 64% had fathered children with multiple women.
The primary sources of reproductive health knowledge among the men were schools (25%), media (17%), and parents (16%). Other sources of knowledge included “the streets” and health care facilities. Fifty-one percent of the men reported that withdrawing the penis before climaxing during sex could result in unwanted pregnancy (Table 2). Most (66.2%) of the men reported no preference for the gender of their health care provider, and 53% had had a routine health check in the past year.
Frequency of Family Planning Practices/Beliefs Among Men in Western Jamaica.

Steps taken include the following: consistent condom use 40%, inconsistent condom use 22.0%, withdrawal 13.7%, support partner to take contraception 15.4%, and vasectomy 0%.
There were reduced odds of taking steps to prevent unwanted pregnancy for men who had moderate (adjusted odds ratio [AOR] = 0.5; 95% confidence interval [CI] = 0.3-0.8) or high (AOR = 0.3; 95% CI = 0.1-0.6) support for inequitable gender norms compared with those with low support (Table 3). A similar association was observed for younger men, and men ages 25 to 34 years compared with men who were ≥35 years, and for men who seldom or never sought routine check-ups compare to those who did (Table 3).
Associations of Select Characteristics With Involvement in Contraception Use Among Men in Western Jamaica.

Note. OR = odds ratio; AOR = adjusted odds ratio; CI = confidence interval.
Adjusted for age, education, religion, and income, regardless of significance level; Bold =p<.05.
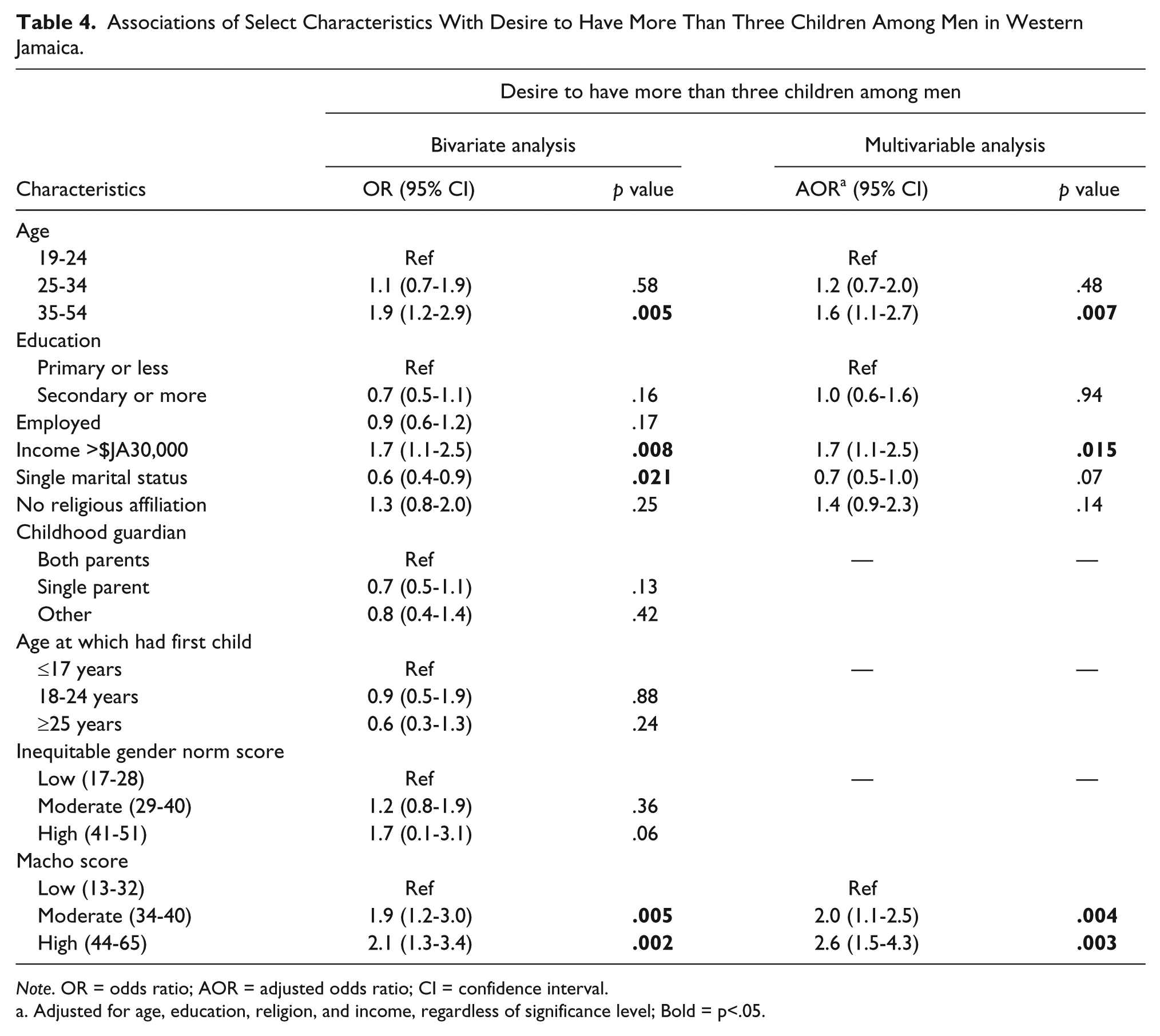
In the bivariate analysis, desire to have a large family (>3 children) was associated with older age, higher income, single status, and moderate and high support for masculinity norms (Table 4). The associations with moderate (AOR = 2.0; 95% CI = 1.3-2.5) and high (AOR = 2.6; 95% CI = 1.5-4.3) support for masculinity norms remained significant in the adjusted analysis.
Associations of Select Characteristics With Desire to Have More Than Three Children Among Men in Western Jamaica.
Note. OR = odds ratio; AOR = adjusted odds ratio; CI = confidence interval.
Adjusted for age, education, religion, and income, regardless of significance level; Bold = p<.05.
Among men (all aged 25 years or older) with two or more children, those with moderate or high support for masculinity norms had twofold increased odds of having fathered children with multiple women (Table 5). Men who fathered their first child at 25 years or older had a 70% reduced odds of having fathered childeren with multiple women compared with men who fathered their first child by age 17 years (Table 5).
Factors Associated With Fathering Children With Multiple Women Among the 224 Men With Two or More Children in Western Jamaica.

Note. OR = odds ratio; AOR = adjusted odds ratio; CI = confidence interval.
Adjusted for age, education, religion, and income, regardless of significance level; Bold = p<.05.
Discussion
The findings from this cross-sectional study involving men in Western Jamaica demonstrate that masculinity and inequitable gender norms influence men’s family planning practices. Specifically, it was identified that men with higher support for inequitable gender norms were less likely to take steps to prevent unplanned pregnancies. Additionally, men with higher support for masculinity norms were more likely to report that they fathered children with multiple women and desired to have a large family (>3 children). These findings suggest that both masculinity and inequitable gender norms have important implications for family planning programs targeting men in Jamaica as these norms influence men’s family planning behaviors in different ways. This also underscores the importance of measuring gender norms to inform the design of gender transformative interventions in family planning programs.
Our findings regarding the association between inequitable gender norms and contraception use is consistent with research conducted by Pulerwitz and Barker (2008). On the contrary, it should be noted that in research conducted by Nanda and colleagues among 200 couples in Tanzania, no association was observed between husbands’ attitudes toward gender norms as measured by the GEM scale and reports of contraception use among their wives. However, more equitable gender norms among wives were positively associated with contraception use (Nanda et al., 2013), which is consistent with our findings.
According to the World Bank, the prevalence of contraception use among Jamaican women aged 19 to 49 years was 72% in 2008 (The World Bank, 2013). Our study identified a similar percentage (75%) of men who reported that they took steps to prevent unwanted pregnancy. However, among these men only 40% reported consistent condom use and none had had a vasectomy. Similar patterns of contraception use (39% consistent and 27.7% inconsistent contraception use) among adolescents have been reported in Jamaica (Crawford et al., 2009). The male condom is the most common method of contraception in Jamaica. Therefore, it was not surprising that the majority of men reported condom use as the method of pregnancy prevention. Much of this is due to the promotion of condom use by the Ministry of Health in its HIV prevention program (Chin-Quee, Wedderburn, Otterness, Janowitz, & Chen-Mok, 2010).
The Sternberg and Hubleys’ review of interventions targeting men documented a number of strategies that have been used to improve men’s involvement in family planning (Sternberg & Hubley, 2004), and this could also be applied to men in Jamaica. These interventions include family planning clinics for men and couples, media approaches, training programs for male dominated industries such as agriculture, and community outreach (Sternberg & Hubley, 2004).
The positive association between intention to have a large family and support of masculinity norms is consistent with findings from research conducted Anderson (Anderson, 2012). In our study, income was also positively associated with desire to have a large family. This may be due to construction of masculinity related to men’s role as providers in the Jamaican family. In the Jamaican society, women are socialized to take care of the home and children, whereas men are expected to be tough, invulnerable, and provide material support (e.g., food, clothing, shelter, money) for the family (Chevannes, 2002; Dreher & Hudgins, 2010).
Although the men in this study were relatively young, a high proportion of them fathered their children with multiple women. Furthermore, higher support of masculinity norms was associated with increased odds of fathering children with multiple women. These findings suggest that intervention geared at reducing masculinity norms among men could potentially delay the onset of fatherhood in Jamaica. This could also reduce absentee fathers, as men who fathered their first child at age ≥25 years had reduced odds of fathering childern with multiple women. Our findings suggest gender ideologies can influence family structure and affect the wellbeing of children. For example the high prevalence (>50%) of multiple sex partners among men in Jamaica (Figueroa et al., 2008; Figueroa, Ward, Walters, Ashley, & Wilks, 2005; Gibbison, 2007; Ishida, Stupp, & McDonald, 2011) and beliefs about fathering a child at an early age to validate manhood and demonstrate to society that they are not homosexuals (P. Anderson, 2012; Chevannes, 2002; Chevannes & Mitchell-Kernan, 1992; Gibbison, 2007; Wyss, 2000) are more likely to result in men fathering children with multiple women.
Although our findings contribute to the understanding of the association between gender norms and family planning practices in Jamaica, this study has a number of limitations, which must be taken into consideration when interpreting the results. First, the authors were unable to demonstrate causality since this was a cross-sectional study. Second, all the assessments have relied on self-reported data collected through interviews. While the interviewers (all of whom were females) were trained the study could potentially be affected by socially desirable bias. Although participants were recruited from all the government-operated hospitals in the WRHA, which serve a wide population area, it should be noted that individuals of upper-middle to high socioeconomic status might underutilize these facilities. The inclusion of visitors (men visiting patients, not seeking health care) to the hospitals in our sample was intended to reduce the potential effect of selection bias. Additionally, the use of a community sample was employed to estimate the representativeness of the hospital sample. Since men in the community sample were more likely to father their children with multiple women, our findings may have underestimated the odds presented in this regard.
Despite these limitations, this study calls attention to the need to involve men in family planning programs in Jamaica, a country wherein approximately 85% of births are premarital and gender norms encouraging men to have multiple sexual partners are pervasive. Both masculinity and inequitable gender norms were observed to negatively affect family planning practices among men in this study. This underscores the need to use both assessment tools (Inequitable GEM and Macho scale) to measure gender norms related to family planning practices among men in Jamaica. Future research should pilot test approaches that could be used to involve men in reproductive health programs and test the effect of gender-transformative interventions on family planning practices among men. Policy changes are also required to bolster family planning programs and effectively change masculinity and inequitable gender norms in the Jamaican society.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Minority Health International Research Training (Grant No. T37-MD001448) from the National Institute on Minority Health and Health Disparities, National Institutes of Health, Bethesda, MD; and the Ministry of Health, Jamaica.