
Abstract
The present study investigated psychosocial predictors for major depressive disorder (MDD), general anxiety disorder (GAD), and suicidal ideation (SI) of Latino American men identified in the first national mental health epidemiological survey of Latinos. Three separate sets of logistic regression analyses were performed for 1,127 Latinos, following preplanned two steps (Model 1—Known Demographic and Acculturation Predictors as controls, Model 2—Psychosocial Risk and Protective Factors). Results show that Negative Interactions with family members significantly predicted the likelihood of both MDD and SI, while SI was also associated with Discrimination. Acculturation Stress was associated with that of GAD (alongside more Income, Education of 12 years, and Years in the United States for less than 11 years). Other potential protective factors (social support, racial/ethnic identity, religious involvement) were not influential. The differential predictors for mental health issues among Latino men imply that assessment and intervention for them may need certain gender-specific foci in order to improve mental health disparities in this population.
As one of the two fastest growing minority groups in the United States, Latino Americans are expected to comprise an estimated 30% of the national population in 2050 (U.S. Census Bureau, 2010). Research on Latinos’ mental health has incurred considerable growth over the past 8 years, since the population-based National Latino and Asian American Study (NLAAS) was made public (Alegria et al., 2004; Alegría et al., 2008). According to the NLAAS investigators, novel aims of the national survey were presented in data on (a) 12-month and lifetime prevalence of psychiatric disorders and the rates of mental health services utilization for Latino and Asian American populations; (b) associations among social position, environmental context, and psychosocial factors with the prevalence of psychiatric disorders and service utilization; and (c) comparison of 12-month and lifetime prevalence of psychiatric disorders, and utilization of Latinos and Asian Americans with representative samples of non-Latino White Americans (from the National Comorbidity Study–Replication [NCS-R]) and African Americans (from the National Survey of American Life [NSAL]). Despite the increased number of publications on the NLAAS, few studies have specifically focused on male Latinos (Ai, Noël, Appel, Huang, & Hefley, 2013).
In a descriptive analysis on the overall health of Latino men in the NLAAS, Ai et al. (2013) reported a 6.4% incidence of major depressive disorder (MDD) over the past 12 months with no subethnic group differences. MDD is characterized by a group of disorders occurring in discrete episodes of at least 2 weeks’ duration, or longer, and involving clear-cut changes in affect, cognition, and neurovegetative functions and interepisode remissions (American Psychiatric Association, 2013). The authors recommended further investigation with multivariate analyses to explore the impact of contributing factors to this psychiatric diagnosis and other health conditions. Expanding that study and also using the NLAAS database (Ai et al., 2013), the current analysis investigated the predictive value of psychosocial protective and risk factors for MDD, generalized anxiety disorder (GAD), and suicidal ideation (SI), above and beyond the role of predictors in the literature. GAD is characterized by excessive anxiety and worry (apprehensive expectation), occurring more days than not for at least 6 months, about a number of events or activities, associated with at least three of six symptoms (e.g., restlessness, difficulty concentrating, irritability; American Psychiatric Association, 2013). SI involves thoughts about suicide.
Given the paucity of male-specific studies on Latinos nationwide, we begin with the significance of the study with previous findings on informed mental health disparity issues and key predictive factors (e.g., sociodemographics and acculturation variables) among all Latinos in the United States. We then present emerging evidence on psychosocial protective factors, mostly evident in the non–gender-specific studies. Finally, we delineate the study aims. The significance of this study may lie in the implications for the integrated health care for minorities. To date, mounting evidence suggests that comorbid mental health disorders play a critical role in chronic ailments and affect the efficiency of health care services in the United States. For example, research has consistently associated MDD and GAD with short- and long-term poor health outcomes, such as cardiovascular diseases (Ai, Rollman, & Berger, 2010; Pan, Sun, Okereke, Rexrode, & Hu, 2011; Whooley et al., 2008). As for the Latino population, Ortega, Feldman, Canino, Steinman, and Alegría (2006) related depression and cooccurring anxiety and depression both to a history of asthma. In addition, anxiety was linked with suffering from diabetes and cardiovascular disease, after controlling for demographics and immigration status or number of years in the United States.
Addressing these mental health issues in the Latino men, primarily in the low-wage job market, may, thus, bear a considerable influence on their health disparities and health care service utilization in the future. Using Collaborative Psychiatric Epidemiology Studies (CPES), epidemiological research has documented mental health disparities among Latinos and other racial/ethnic minorities in the United States. Nicklett and Burgard (2009) linked Latino ethnicity, the female sex, a longer residency in the United States, and being a U.S. citizen with greater odds of major depressive episodes among immigrants to the United States in the national database. González, Tarraf, Whitfield, and Vega (2010) showed that Mexicans, alongside African Americans, reported significantly higher depression chronicity and lower depression care use compared with European Americans. However, Asnaani, Richey, Dimaite, Hinton, and Hofmann (2010) found that Latinos overall were less likely to meet the diagnoses for GAD and posttraumatic stress disorder than European and African Americans, respectively. An earlier analysis revealed varied lifetime prevalence of SIs and suicidal attempts, ranging from 4.4% to 10.2% across Latino subgroups (Fortuna, Perez, Canino, Sribney, & Alegria, 2007). Borges, Orozco, Rafful, Miller, and Breslau (2012) found that non-Hispanic White Americans ranked the highest on SI, followed by Hispanics, non-Hispanic Blacks and Asian Americans. The difference in rates of suicide attempt, however, was equally common among Latino, non-Hispanic Black, and non-Hispanic White Americans.
To date, NLAAS publications have exhibited certain known predictors for Latinos’ mental health, which must be controlled for in the present study. An unemployed status was associated with MDD among all Latinos (Gavin et al., 2010) and, in particular, with psychiatric disorders among men of all minority subgroups (Chatterji, Alegria, & Takeuchi, 2009). U.S.-born and more acculturated Latinos (e.g., better English proficiency, third generation) had greater likelihood of being diagnosed with MDD and other psychiatric disorders (e.g., bipolar disorders, posttraumatic stress disorder) than immigrant Latinos (Alegría, Mulvaney-Day, Woo, & Torres, 2007; Alegría et al., 2008; Grant et al., 2005; Vega, Canino, Cao, & Alegria, 2009; Vega et al., 1998; Ortega, Canino, & Alegría, 2008). Odds of lifetime GAD were more prevalent in the bilingual group assigned to English than in the group interviewed in Spanish (Shrout et al., 2008). For Latino and other minorities, risk for suicide including ideations prior to migration was low among immigrants than the U.S.-born but was equalized over time after migration (Borges et al., 2012). Differences of SI across Latino subgroups were linked with or moderated by their lifetime Diagnostic and statistical manual of mental disorders, fourth edition (DSM-IV) diagnoses (Fortuna et al., 2007). Zhang, Hong, Takeuchi, and Mossakowski (2012), however, displayed a stronger connection of sociodemographic variables and discrimination (an important acculturation factor for Latinos) with psychological distress than English proficiency in Latino and Asian Americans. Despite the recent evidence regarding known predictors and psychiatric disorders, there is still an insufficient understanding of Latinos’ m7ental health. Additional efforts should be made on culturally relevant psychosocial factors.
One of the important goals of the NLAAS survey was attaining cultural relevance in contextual differences of Latinos as compared with the mainstream population. Emerging evidence suggests that the lower rate of anxiety disorders in Latinos, compared with those in European and African Americans, may partly be attributed to protective influences of certain psychosocial factors (e.g., racial/ethnic identity, social support, and religious involvement, operationalized as religious attendance and coping). Mulvaney-Day, Alegría, and Sribney (2007) demonstrated the benefit of a strong social network and social support for their physical and mental health. Robinson, Bolton, Rasic, and Sareen (2012) found that religious attendance contributed to the low odds of both anxiety and SI. Pérez, Fortuna, and Alegria (2008) indicated that Latinos holding greater racial/ethnic identity perceive less discrimination, compared with their counterparts who identified themselves less with Latinos. In another report, such identity significantly contributed to Latinos’ self-rated mental health and self-rated physical health, above and beyond the predictive value of known predictors (e.g., discrimination; Ai, Aisenberg, & Weiss, 2014). This study also replicated Robinson et al.’s (2012) finding concerning an optimal role of attendance in mental health.
Among all psychosocial predictors, family-relevant factors may stand out as one most uniquely relevant to the Latino culture. Predominantly Catholics, the Latino population is characterized by the influence of collectivism in which family values play a central role in their ethnic identity and mental health (Ai, et al., 2014). Earlier reports found family discord to alleviate self-reported mental health and to accelerate the risk of mood disorders (Alegria, Shrout, et al., 2007; Mulvaney-Day et al., 2007). Those authors suggested that maintenance of family harmony, integration in advantageous U.S. neighborhoods, and positive perceptions of social standing are critical to successful adaptation into the United States. Indeed, Lorenzo-Blanco and Cortina (2013) associated acculturated Latinos with a pattern of frequently perceived discrimination, family conflict, and a lack of shared family values and cohesion. Family cohesion was identified as a protector against GAD in Latinos, in addition to the damage of family discord concerning all anxiety disorders (Priest & Denton, 2012). As a part of the acculturation process, family problems and discrimination, in turn, contributed to the greater likelihood for MDD.
Currently, however, there is limited research evidence concerning the role of family factors (negative interaction and family coherence) among Latino men, alongside other potential protective factors (racial/ethnic identity, social support, and religious involvement). Latino male immigrants who assumed a culturally inherent role for their families (chief breadwinners) may face more distress within the personal autonomy-oriented culture in the United States (Arbona et al., 2010). As such, cultural-transmutation-based stressors may exert particular pressure on Latino men. In an earlier study, Canino, Vega, Sribney, Warner, and Alegría (2008) found that substance use disorders increased with problematic family relations for Latino men but not for Latin women. Based on the limited evidence, more gender-specific studies are required to better inform assessment and intervention for this growing prominent blue-collar workforce and the largest immigration group in the United States.
The primary aim of our study is to address this gap through revealing the joint effect of psychosocial factors on the likelihood of MDD, GAD, and SI among Latino men. To evaluate the predictive value of these factors, above and beyond the influence of existing demographic and acculturation predictors, we conducted logistic regression analyses controlling for those variables in the literature. The secondary aim was to take the study as a mirror analysis of our previous report in a Latin women-specific multivariate analysis (Ai, Weiss, & Fichman, 2014) in order to draw cross-gender comparison in Latinos nationwide. In that study, we have found the prediction of negative interactions in their families for women’s GAD and SI but not for their MDD, while family cohesion appeared to protect them against GAD. Furthermore, negative interactions in part explained the detrimental impact of perceived discrimination on Latin women’s SI. Such a comparison between Latino men and Latin women may help inform the care service providers for this rapidly growing working force in the U.S. health industry.
Method
Data Source and Procedure
The study is a secondary data analysis using the NLAAS data set. The NLAAS is the first representative household survey on the mental health of Latino and Asian Americans residing in the United States. The study was designed as a part of the CPES that includes NLAAS, the NSAL, and the NCS-R. The aggregated data of CPES are partly aimed to compare the association of immigration factors and the use of mental health services across major racial and ethnic categories (African American, Asian American, and Latino Americans) with that of European Americans. The original research design of the NLAAS was thus adapted from that of the NCS-R (Alegria et al., 2004; Kessler et al., 2004).
Available in six languages (e.g., English and Spanish), the NLAAS questionnaire provided the information on key sociodemographics, self-reported mental health diagnoses, service utilization, and acculturation variables for Latinos. The data were collected from May 2002 to December 2003 at various sittings by trained bilingual interviewers and aggregated at the University of Michigan. The total sample size in the NLAAS was 4,649, including 2,554 Latinos (aged 18 years or older) in three major subgroups (i.e., Cubans, Mexicans, and Puerto Ricans) and “Other” Latinos (e.g., Costa Ricans, Ecuadorans, Guatemalans, and Hondurans), all aged 18 years and older. This research project involved all 1,127 Latino men identified in the NLAAS.
The NLAAS consists of primary sampling units selected with probabilities proportional to size with three stages of sampling that were described extensively elsewhere (Alegria et al., 2004; Heeringa et al., 2004). Weights were developed to correct for sampling bias for the total sample, using the interval estimates from other CPES studies. Specifically, the NLAAS employs Bayesian methods to produce weighted estimates (Heeringa et al., 2004). The public version of the NLAAS was released in 2004. Institutional review board approvals were gained and informed consent was received from all study participants in the initial NLAAS and also for this secondary analysis at the Florida State University. All computations were conducted using Stata 10 (StataCorp LP, College Station, TX). The weights created for the data are presented in the results, based on demographics social and economic variables to correct for sampling bias, including age.
Measures
Dependent Variables as Criteria
Mental health disorders
In the NLAAS, a diagnosis of MDD, GAD, or SI was recorded, based on the World Mental Health Survey Initiative version of the WMH-CIDI, equivalent to the criteria from the DSM-IV (American Psychiatric Association, 1994; Kessler, Andrews, Mroczek, Ustun, & Wittchen, 1998). Participants were asked whether they had had these diagnoses in their lives and over the past 12 months by interviewers, which were recorded as dichotomy variables (0 = no, 1 = yes). We used the 1-year rate in order to not introduce bias concerning the extent of life span toward younger respondents.
Known Predictive Factors as Controls
Sociodemographic predictors
In the Step-I multivariate analysis, we entered a set of four variables: Age (measured by years), Education (four levels: 1 = 0-11 years, 2 = 12 years, 3 = 13-15 years, and 4 = ≥16 years with 0-11 years served as the reference category), Income (ranging from 0 to 17; measured using an index as the ratio to poverty threshold—the U.S. Census’ Year 2000 poverty line), and Employment (two levels: 0 = unemployed or not in the labor force, 1 = employed).
Acculturation predictors
Step I of the multivariate analysis also evaluated a set of five such variables. First, English Proficiency was based on an average of three items regarding levels of one’s ability to speak, read, and write English (α = 0.97). Second, U.S.-born was dichotomized (0 = foreign-born, 1 = U.S.-born). Third, Years in the United States was categorical (four levels: 0-10, 11-20, ≥21 years or more, and U.S.-born with 0-10 years in the United States served as the reference category). Fourth, Acculturation Stress (an averaged scale based on nine items with dichotomized answers; 0 = no, 1 = yes) assessed social and emotional strains pertaining to culture change resultant from migration (Vega et al., 1998; α = 0.69). Finally, Discrimination (an average of nine questions on a 6-point scale for each; 1 = never, 6 = almost every day) measured daily perception of perceived discrimination (Gee, Spencer, Chen, Yip, & Takeuchi, 2007; α = 0.908).
Independent Variables of Major Interests
Risk and protective factors of major interests
The Step-II analysis included a set of five psychosocial variables of major interest in this study: (a) Religious Involvement (Attendance or Coping; one item for each measure, respectively; for example, Attendance was measured on a 4-point scale, 1 = never, 2 = once a month, 3 = 1-3 times a month, and 4 = once a week or more with never served as the reference category); (b) Social Support (composed of eight variables measuring emotional support through spouses/partners, family, and friends; an averaged 4-point scale,1 = not at all; 4 = a lot; α = 0.783); (c) Negative Interactions (based on two items asking about past conflict with the respondent’s family; an averaged 4-point scale, 1 = never, 4 = often; α = 0.598); (d) Family Cohesiveness (consisting of three variables measuring the feeling of closeness to the respondent’s family; an averaged 4-point scale,1 = strongly disagree, 4 = strongly agree; α = 0.845); and (e) Racial and Ethnic Identity (based on three items measuring perceived closeness to the respondent’s ethnic group; an averaged 4-point scale; α = 0.749).
Statistical Analysis
Descriptive analyses were computed for all variables among Latino men in this analysis. Kendall’s Tau statistics were conducted to illustrate the zero-order correlations between all variables in the multivariate analyses. Logistic regression analyses were conducted with dichotomous diagnostics as the criterion for three outcomes, respectively, involving two preplanned steps. Under each diagnosis, the first model included covariates (existing sociodemographics and acculturation predictors in the literature. The second included the investigation of psychosocial risk and protective factors in addition to the existing predictors in the first model. Religious Attendance and Coping were evaluated in two separate equations, following previous analyses; Ai, et al., 2014), and were presented in two models. In logistic regression, the odds ratios (ORs) indicate the likelihood that one group had the likelihood of occurrence in any diagnosis than another group. An OR >1 represents a positive relationship, and OR <1 represents a negative relationship. Differences in chi-squares in Steps I and II showed whether the newly added variables increase the power of the original sets of predictors. For all tests, we used an alpha level of .05 to establish statistical significance.
Results
Descriptive Analyses and Bivariate Correlations
Table 1 displays all descriptive information for Latino men. Average age was 39.94 years (SD = 15.5; range = 18-92 years), and average income was 4 (SD = 3.97), based on the 2001 Census household income/needs ratio (range = 0-17). Around 64% of them have some level of education up to high school (Levels 1-2, ≤12 years), with nearly 26% of that group graduating the 12th grade (Table 1). Although only slightly over one third of the sample was U.S.-born, 80% of Latinos have stayed in the United States at least 11 years during the interview. Bivariate correlations show a positive and significant relationship between all three dependent variables for Latino men.
Descriptive Analyses.

The reference category in multivariate analyses.
Other correlations among all independent variables are shown in Table 2. In particular, positive correlates of Negative Interactions, Religious Coping, and Discrimination included three acculturation factors (U.S.-born, Length in the United States, and English Proficiency). These acculturation factors were also negatively correlated with three other factors of major interests (Family Cohesion, Social Support, and Racial/Ethnic Identity). In contrast, Acculturation Stress was correlated inversely with Negative Interactions but positively with Social Support and Racial/Ethnic Identity. Discrimination was also negatively correlated with Family Cohesion, Social Support, and Racial/Ethnic Identity. Correlations between all independent variables and all dependent variables are presented in Table 3. Positively related to MDD was Negative Interactions, alongside Discrimination, three acculturation factors, unemployment, and younger age. The pattern was the same to SI, except Negative Interactions. However, there was no significant correlate with GAD.
Kendall’s Tau–B Correlations.

p ≤ .05. **p ≤ .01.
Correlations for All Independent and Dependent Variables for Latino Men (N = 733).

Note. MDD = major deopressive disorder; GAD = general anxiety disorder; SI = suicidal ideation.
p ≤ .05. **p ≤ .01. ***p ≤ .001.
Furthermore, a post hoc gender-comparison analysis found that, concerning demographic and acculturation factors, there were no differences for Age, Education, Length in the United States, U.S.-born, English Proficiency, and Acculturation Stress across male and female subgroups (data not shown). Conversely, Latino male respondents perceived greater discrimination against them, even though they reported relatively higher levels of Incomes and better Employment status, compared with their women counterparts. Regarding psychosocial variables, Latino men indicated fewer Negative Interactions and greater Social Support while involving in less Religious Attendance or Coping to deal with their problems, compared with Latin women. No difference was shown in Family Cohesion and Racial/ethnic Identity.
Multivariate Analyses Using Religious Attendance to Indicate Religious Involvement
Major Depressive Disorder
Model 1 (MDD, Table 4) shows the likelihood of being diagnosed with MDD for Latino men. Employment was the only factor linked with 52.3% less likelihood of MDD. This effect, however, was nullified in Model 2, while Negative Interactions occurred as a single significant predictor for MDD among Step II psychosocial factors. Every increased level of such interactions added the likelihood of a MDD diagnosis by 94.2%. However, entry of Negative Interactions did not mediate the initial effect of Employment (Model 1, Table 4), given that the two independent variables were not correlated (Table 2). The new predictive factors as a group entered in Model 2 resulted in a significantly better model fit. Therefore, Latino men who reported greater family conflicts were more likely to be diagnosed with MDD.
Logistic Regression Predicting MDD, GAD, and SI in the Past 12 Months (Religious Attendance Used).
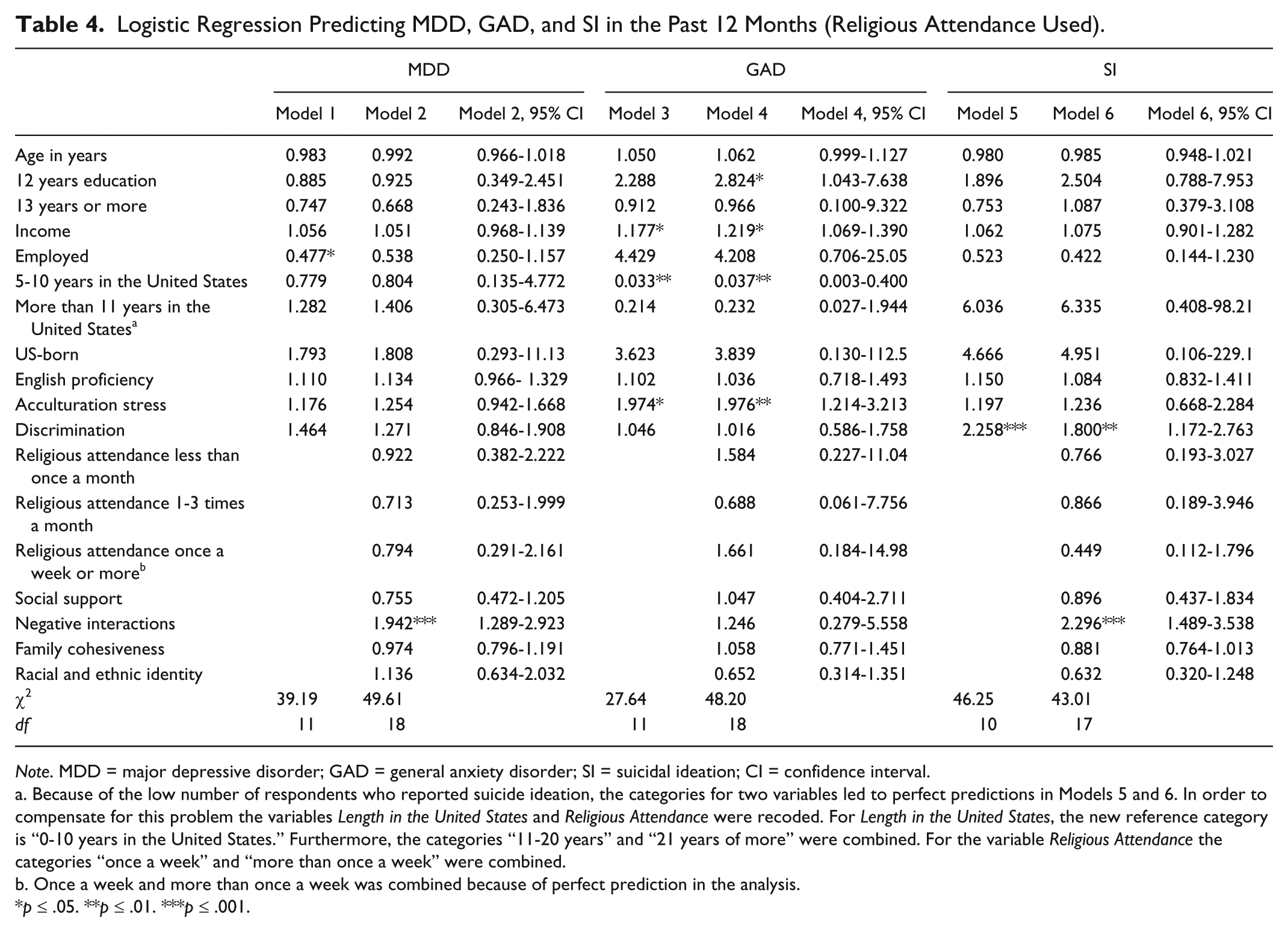
Note. MDD = major depressive disorder; GAD = general anxiety disorder; SI = suicidal ideation; CI = confidence interval.
Because of the low number of respondents who reported suicide ideation, the categories for two variables led to perfect predictions in Models 5 and 6. In order to compensate for this problem the variables Length in the United States and Religious Attendance were recoded. For Length in the United States, the new reference category is “0-10 years in the United States.” Furthermore, the categories “11-20 years” and “21 years of more” were combined. For the variable Religious Attendance the categories “once a week” and “more than once a week” were combined.
Once a week and more than once a week was combined because of perfect prediction in the analysis.
p ≤ .05. **p ≤ .01. ***p ≤ .001.
General Anxiety Disorder
Model 3 (GAD, Table 4) presents the odds of being diagnosed with GAD for Latino men. As noted, every one unit increase in Income raised the odds by 17.7. Length in the United States less than 11 years was associated with the 96.7% less likelihood of GAD, while each unit increase of Acculturation Stress increased the odds by 97.4%. These patterns were sustained in Model 4. The magnitude in the role of Income increased to 21.9%, while effects of Acculturation Stress and Length in the United States were slightly altered. However, Education of 12 years emerged as significant predictor. New factors as a group entered in Model 4 yielded a significantly better model fit, though none of the Step II factors presented as a significant predictor. As such, Latino men who had higher income, perceived more acculturation stress, and those who reported high school education, but not college education, were more likely to be diagnosed with GAD. On the other hand, having been in the United States less than 12 years had a lower chance.
Suicidal Ideation
Model 5 (SI, Table 4) shows the likelihood of experiencing SI with Discrimination as the single predictor. Each increased level of perceived discrimination raised the likelihood of a SI diagnosis by 125.8%. In Model 6, the magnitude reduced to 80%, while Discrimination remained to be a significant predictor. Once again, Negative Interactions occurred as a single significant predictor for SI among Step II psychosocial factors. Every increased level of such interactions added the likelihood of a SI diagnosis by 129.6%. Because of the correlation between Discrimination and Negative Interactions (Table 2), and Discrimination and SI (Table 3), the reduced influence of Discrimination appeared to be moderated by Negative Interactions. The set of newly entered factors as a group led to a significantly better model fit. Accordingly, Latino men who perceived greater discrimination and/or family conflict were more likely to be diagnosed with SI.
Multivariate Analyses Using Religious Coping to Indicate Religious Involvement
Models using Religious Coping, rather than Religious Attendance, presented only slight differences in the size of coefficients in Table 5, predicting MDD, GAD, and SI, respectively, with no substantive changes of signs.
Continued. Logistic Regression Predicting MDD, GAD, and SI in the past 12 Months (Religious Coping Used).
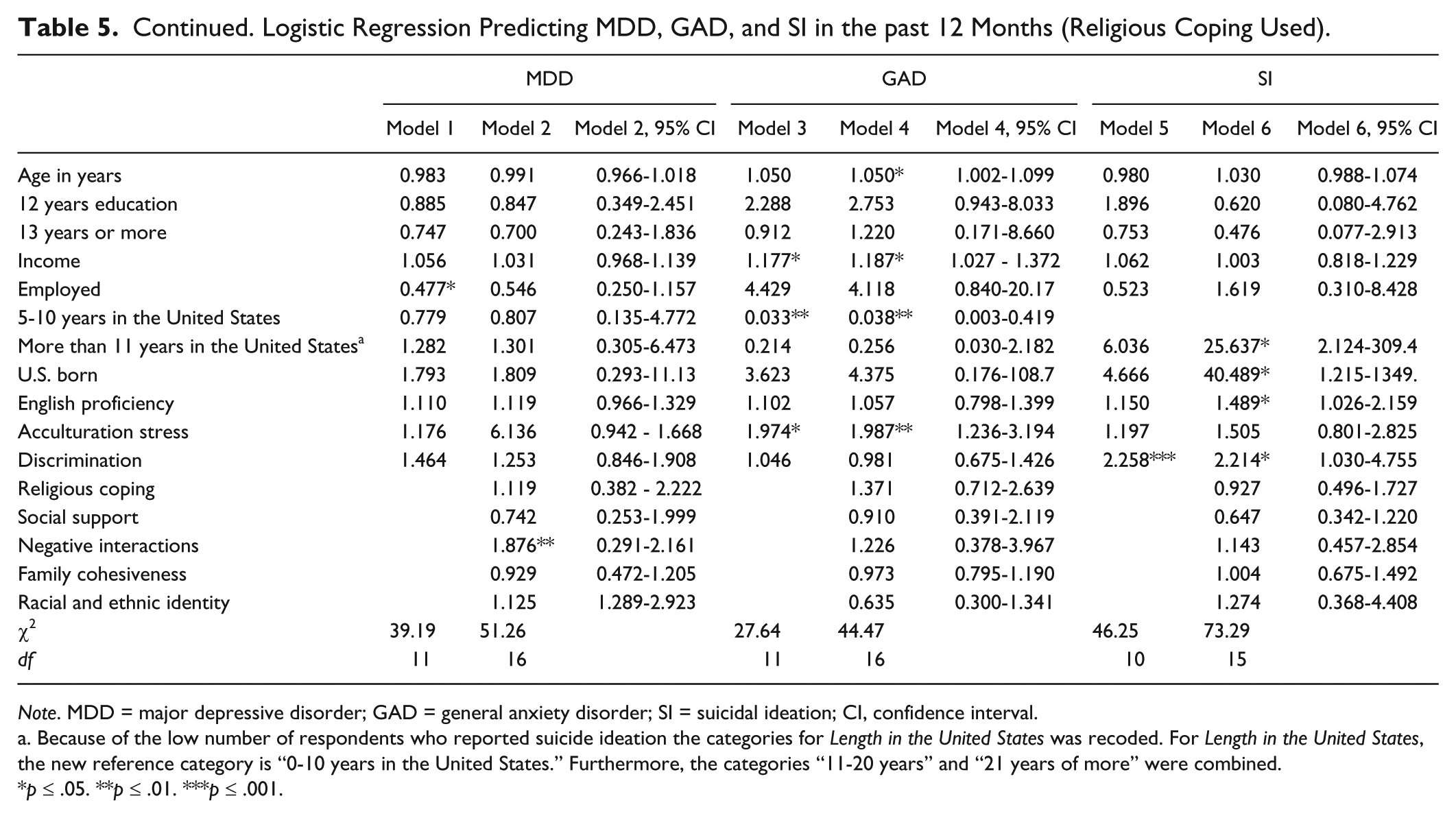
Note. MDD = major depressive disorder; GAD = general anxiety disorder; SI = suicidal ideation; CI, confidence interval.
Because of the low number of respondents who reported suicide ideation the categories for Length in the United States was recoded. For Length in the United States, the new reference category is “0-10 years in the United States.” Furthermore, the categories “11-20 years” and “21 years of more” were combined.
p ≤ .05. **p ≤ .01. ***p ≤ .001.
Major Depressive Disorder and General Anxiety Disorder
The coefficient for Negative Interactions on MDD in Model 2, Table 5, was quite similar to that in Table 4. In Model 3, Table 5, predicting GAD, entry of psychosocial factors only yielded a statistically significant effect of Age in Model 4. However, this change is mostly because of a small change in the standard error, which leads significance levels to shift from p = .051 (Table 4) to p = .040 (Table 5). The coefficient of Age in Model 4 had no substantive change from that in Model 3, Table 4. Using Religious Coping did not primarily alter the predictive role of Income and Length in the United States less than 11 years between Tables 4 and 5. The coefficient for Acculturation Stress remained about the same between Tables 4 and 5.
Suicidal Ideation
Finally, using Religious Coping in the models for SI led U.S.-Born, Length in the United States over 11 years, and English Proficiency become significant positive predictors for SI (Model 6, SI, Table 5) compared with Model 6, Table 4. The direct effect of Discrimination persisted in Model 6, Table 5, which, however, was not moderated by the entry of psychosocial factors. None of the variables entered in Model 6 emerged as a significant predictor for SI in Table 5.
Discussion
Regarding our primary aim, the present study fills a gap in Latino men’s research with respect to influences of their psychosocial risk and protective factors on three major psychiatric disorders with significant public health impacts. Expanding the previous understanding of Latino men’s overall health (Ai et al., 2013; Canino et al., 2008), our principal finding suggests that family conflicts may negatively affect the mental health diagnoses of Latino men nationwide. Consistent with the literature as mentioned, our bivariate analyses have correlated greater acculturation with poor mental health, especially MDD and/or SI, in Latino men (Alegría, Mulvaney-Day, Torres, et al., 2007; Alegría et al., 2008; Grant et al., 2005; Ortega et al., 2008; Pilver, Kasl, Desai, & Levy, 2011; Shrout et al., 2008; Vega et al., 1998; Vega et al., 2009; J. Zhang, Fang, Wu, & Wieczorek., 2013). The significance of some correlates, however, altered or vanished in multivariate analyses, supporting the need for using the latter analytical tool in studying this gender-specific subgroup (Ai et al., 2013). Indeed, whether psychosocial factors add predictive value for these diagnoses, above and beyond the role of known predictors, should be elaborated on multivariate analysis.
Specifically, this study identifies negative interactions within Latino families as a psychosocial risk factor for both MDD and SI, but not that of GAD, after controlling for existing predictors, such as socioeconomic status and acculturation factors. Importantly, the reduced impact of discrimination on SI in Model 6, Table 4, is moderated by entry of psychosocial factors, especially family conflict. Conversely, this alteration implies that improving family relationships might help mitigate the negative impact of perceived discrimination on Latino men’s SI in the future. In Model 1, Table 4, we also find that unemployed Latino men are more likely to be diagnosed with MDD, consistent with the literature on MDD among all Latinos (Gavin et al., 2010) and on psychiatric disorders in all minority male groups (Chatterji et al., 2009). The vanished effect on the entry of psychosocial factors underscores the importance of investigating these culturally relevant factors in Latino men. Social scientists suggested that, for immigrants from non-Western traditions, encountering an individualistic Western society can increase stressors because of the conflict between the latter’s individualistic social norm with the collectivist cultural norms brought with them (Fischer, Ai, Aydin, Haslam, & Frey, 2010; Lorenzo-Blanco, & Cortina, 2013; Pilver, et al., 2011). Our key finding on family conflicts thus echoes this theoretical assumption with empirical evidence concerning the value of studying all these aspects together that could jointly impose detrimental impacts on mental health.
Regarding our secondary aim, the link of family discord with MDD and, especially its strong association with SI in Latino men should further be investigated based on a comparison with findings in Latin women (Ai et al., 2014). For these women, negative interactions predicted GAD and, to a lesser degree, SI, rather than MDD. Variant correlations between the different psychiatric responses and gender with similar stressors in the United States may be interpreted with respect to their cultural roles. As Canino et al. (2008) speculated, cultural transition-based mental health issues can differ in considerable ways between these two Latino subgroups. In the previous study (Ai et al., 2014), we concluded that Latin women may be expected to attend their families more than men (Galanti, 2003) through a sustained harmonic relationship with children, spouse, and friends (Gilligan, 1993) in their family-centered culture. Disrupting family harmony for any reason may then become a major stressor for Latin women to experience anxiety that could lead to the extreme notion of SI.
Conversely, Latino men from this culture may assume a male-gender role as primary financial providers and household leaders. In this case, conflicts or disputes within their families can be perceived as a personal failure, thereby resulting in a greater sense of sadness. Moreover, the present study did not replicate the protective function of family cohesion for all Latinos by Priest and Denton (2012) and for Latin women in the earlier report (Ai et al., 2014). The evident lack of protection for Latino men may reveal more risks for them regarding family issues in the face of cultural transmutation–based stressors in line with a culture-dictated male-gender role (Duke, Bourdeau, & Hovey, 2010; Edimansyah et al., 2008). In addition, our findings showed acculturation factors (English proficiency, U.S.-born, and longer stay in the United States) as risk factors for GAD and SI, while high school education (but not college education) and income may contribute to GAD in multivariate analyses. Indeed, Latino men who experienced domestic conflicts could be challenged by stress experienced both in work and at home, resulting in accumulated likelihood of suffering from mental health disorders.
Our post hoc analysis indicates that, compared with Latin women, Latino men perceived greater discrimination, while predominantly working in the low-wage job market. Furthermore, discrimination predicted Latino men’s MDD and SI in this study (Table 5) but women’s anxiety in the previous report (Ai et al., 2014). Although family factors did not predict anxiety and SI of Latino men, entry of these psychosocial factors does alter the impact of existing demographic and acculturation predictors. Future investigation must include culturally relevant psychosocial factors in examination of the mental health of Latino men, and women as well, nationwide.
The exact reason for major gender-specific differential patterns remains inconclusive, which may deserve more culturally nuanced qualitative studies and replication with prospective quantitative research. Yet the differential prediction for the mental health disorders varying with these subgroups does highlight the need for more gender-specific investigation to design better health care and psychosocial counseling for Latino men and Latin women, respectively. These variant patterns imply that the manifestation of mental health symptoms may be different in relation to the different trajectory of cultural transition for Latino descendants at the intersection of their traditional gender roles and the U.S. individualistic culture. This revealing fact underscores the importance of involving these factors in Latino studies so as to better understand the reality behind Latino men’s mental health symptomology.
To acknowledge the study’s limitations, a cross-section and correlational design in the NLAAS will only allow us to draw causal conclusions. Self-reported diagnoses may not be as reliable as those made directly by psychiatric interviews. Report bias and cultural stigma on mental health disorders could also be an influential factor, resulting in an underreported prevalence. Regarding other assessment issues in the NLAAS, Negative Interactions was scaled based on only two items that are correlated at a very modest level (α = .598). Increasing the number of items in this factor might enhance this assessment in the future. Two religious involvement factors were assessed by a single item each in the NLAAS. This approach is subject to criticism (Ai, Hall, Pargament, & Tice, 2012). While the DSM-5 (American Psychiatric Association, 2013) has just been published, those diagnostic categories identified earlier in the NLAAS have now become somewhat different from those in the DSM-IV. However, the major three outcomes in this study seem not to be affected.
Despite these limitations, the present study has employed a novel database to address an important question around acculturation (immigration related family issues and perceived discrimination) of Latino men in the United States. In particular, our findings offer the gender-specific knowledge for Latino men’s mental health based on the first national representative data. The significance of the study lies in the fact that Latino men are underrepresented in mental health services, even though all immigrant Latinos reported violence exposure and 76% described additional lifetime traumas that contribute to poor mental health (Fortuna, Porche, & Alegria, 2008). To improve their participation of health and mental health care, our findings indicate the importance of being attentive to their culturally specific factors, especially family discord and conflicts. Intervention research could also take place to evaluate the efficacy of cultural transition-based psychosocial interventions to develop effective preventive care for this population.
Furthermore, the presented patterns for three major disorders suggest that simply using psychiatric medications for Latino men, and women, may not be sufficient for preventing long-term relapse without addressing the relevant root problems. Health care providers should have cultural insight into the context of Latino men and Latin women’s mental health needs. If the findings could be replicated in longitudinal and clinical studies, our study may point to the essential role for multidisciplinary teamwork to address the needs beyond medication treatment in this male subpopulation. Professional attention should be paid to the cultural transition factors and their implications for symptoms. The process of acculturation in the United States may lead to the loss of culturally tied health beliefs, available resources, and social support networks, which can put Latinos at risk for depression, substance abuse, and other mental illnesses (Coffman, & Norton, 2010; Ellison, Jandorf, & Duhamel, 2011; Larson & McQuiston, 2008). Clinicians should involve several other providers, such as social workers, psychiatric nurses, family therapists, and clinical psychologists to account for these cultural factors and risk for disparities in mental health.
Finally, health care professionals such as social workers and public health nurses are in a unique position to provide culturally tailored and collaborative care for Latino immigrants. Cultural awareness and sensitivity are routinely included in basic assessments and health planning for both professions and are an integral part of their curricula (DeSantis & Lipson, 2007). Culture influences how patients make decisions regarding their health, communication style with providers, and coping skills during illness (Caplan et al., 2013; Halm, Evans, Wittenberg, & Wilgus, 2012). Having this knowledge gives nurses and social workers the ability to empower Latino men with mental illness while respecting their cultural backgrounds throughout the health care process. Both professionals are trained in their respective disciplines to screen for depression, manage health provider referrals for treatment, educate on coping, and find community resources for Latinos and their families (Van Voorhees, Walters, Prochaska, & Quinn, 2007). A team approach can support Latino men to meet challenges in life while proving beneficial for their mental health and acclimation into the United States.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.