
Abstract
This article sought to determine whether racial disparities exist in psychotropic drug use and expenditures in a nationally representative sample of men in the United States. Data were extracted from the 2000-2009 Medical Expenditure Panel Survey, a longitudinal survey that covers the U.S. civilian noninstitutionalized population. Full-Year Consolidated, Medical Conditions, and Prescribed Medicines data files were merged across 10 years of data. The sample of interest was limited to adult males aged 18 to 64 years, who reported their race as White, Black, Hispanic, or Asian. This study employed a pooled cross-sectional design and a two-part probit generalized linear model for analyses. Minority men reported a lower probability of psychotropic drug use (Black = −4.3%, 95% confidence interval [CI] = [−5.5, −3.0]; Hispanic = −3.8%, 95% CI = [−5.1, −2.6]; Asian = −4.5%, 95% CI = [−6.2, −2.7]) compared with White men. After controlling for demographic, socioeconomic, and health status variables, there were no statistically significant race differences in drug expenditures. Consistent with previous literature, racial and ethnic disparities in the use of psychotropic drugs present problems of access to mental health care and services.
Background
A supplement to the Surgeon General’s Report (1999) revealed disparities in mental health between racial and ethnic minorities and Whites across measures of access to care and diagnosis (U.S. Department of Health and Human Services, Office of the Surgeon General, SAMHSA, 1999). Among the findings were that African Americans were more likely to experience a mental disorder compared with Whites, yet less likely to seek treatment (Agency for Healthcare Research and Quality, 2010; Centers for Disease Control and Prevention, 2011; Office of Minority Health, 2012). African Americans were also more likely to use the emergency room for mental health care when seeking treatment (U.S. Department of Health and Human Services, Office of the Surgeon General, SAMHSA). While Hispanics displayed rates of mental illness comparable with those of Whites, Asians were less likely to receive inpatient care than Whites and more likely to be misdiagnosed as “problem-free” when seeking treatment (U.S. Department of Health and Human Services, Office of the Surgeon General, SAMHSA, 1999).
A study by Wells, Klap, Koike, and Sherbourne (2001) reported that when compared with Whites, African Americans were less likely to have access to mental health care, and Hispanics were more likely to have less care than needed, or delayed care. McGuire, Alegria, Cook, Wells, and Zaslavsky (2006) indicated that Blacks have a significantly lower likelihood of any health care expenditure when compared with Whites. Blacks were more likely to have mania, psychosis, and panic disorder, and along with Hispanics, were less likely to have mental health coverage compared with Whites (McGuire et al., 2006).
Racial disparities in controlled drug prescribing for mental health have also been revealed. A study by Kuno and Rothbard (2002) uncovered disparities in schizophrenia drug prescribing patterns between African Americans and Whites. In addition, Han and Lui (2006) reported significant disparities in psychotropic drug use for mental illness between Whites, Blacks, Hispanics, and Asian Indians. In the same study, disparities were also revealed in expenditures on prescription drugs for specified mental illnesses between racial minorities and Whites, even after adjusting for the difference in likelihood of using those prescription drugs. Recent studies examining trends in mental health care reveal little to no progress toward eliminating disparities in mental health care in primary care or psychiatric settings (Cook, McGuire, & Miranda, 2007; Stockdale, Lagomasino, Siddique, McGuire, & Miranda, 2008).
In 2009, psychotropic drugs were the fourth most commonly prescribed drug in the country, costing adults $20.9 billion. Almost 18% of adults who use any prescription drug experienced psychotropic drug expenses in 2009, with an average cost of $119 per prescription (Agency for Healthcare Research and Quality, 2009a, 2009b). While previous research has uncovered significant mental health disparities between Whites and racial minorities, racial and ethnic disparities in terms of drug use and expenditures are underresearched, particularly among American men. Widespread research has documented that men report poorer health than women across a broad range of measures, including infant mortality, accidents, suicides, hypertension, cancer, and homicide (Williams, 2003). It is also well known that African American men report poorer health measures than the rest of the U.S. population (Williams, 2003). These measures include greater age-adjusted death rates over the past decade, lower life expectancy, and greater mortality from conditions such as prostate cancer, diabetes, and cardiovascular disease (Xu, Kochanek, Murphy, & Tejada-Vera, 2010). Given the economic burden that both mental health and racial and ethnic disparities have on society, this article will uncover whether race is a significant predictor of drug use and expenditures, which serve as a proxy for measuring adequate access to mental health care and services. The growing national use of psychotropic drugs coupled with increasing racial and gender health disparities makes this project an important and necessary contribution to the literature. This study seeks to determine whether racial disparities exist in psychotropic drug use and expenditures in a nationally representative sample of men in the United States, aged 18 to 64 years.
Method
Data Source
Demographic, medical conditions, and prescribed medicines data files were merged across 10 years (2000-2009) of the Medical Expenditure Panel Survey (MEPS). Since 1996, MEPS has been conducted by the Agency for Healthcare Research and Quality in an effort to determine the relationships between social, demographic, medical characteristics, and health service utilization, including access to care and quality of care in the U.S. civilian noninstitutionalized population. Each annual survey is a nationally representative subsample of households, based on the sampling frame of the prior year’s National Health Interview Survey, which uses a stratified, multistate sampling design. MEPS is unique in its ability to link data on individuals and households to information on health services use. This information includes sources of payment for specific medical services, health insurance status, and details on health insurance plans. Additional information regarding MEPS has been described elsewhere (Agency for Healthcare Research and Quality, 2009a).
Study Sample
The study sample was restricted to non-Hispanic White, non-Hispanic Black, Hispanic, and Asian men, aged 18 to 64 years, for a total of 45,198. Men who did not respond to medical conditions and/or prescription drug use questions were excluded from the sample. Given the widespread use of psychotropic drugs for Alzheimer’s disease and other dementias, those aged 65 years and older were excluded from the sample because of their higher propensity to seek these medications. The outcome variables of interest are likelihood of psychotropic drug use and psychotropic drug spending. The independent variable of interest is race. Covariates in our analyses were age, marital status, insurance status, education, family poverty status, physical health, and metropolitan statistical area (MSA) residence. Several mental health status indicators were controlled for in the analysis, specifically mental health component score from the SF-12 (Mental Component Summary [MCS]), number of mental health diagnoses, and severity of disease. With the exception of MCS, the covariates were measured categorically. The categories for age were defined as 18 to 24 years, 25 to 34 years, 35 to 44 years, 45 to 54 years, and 55 to 64 years. Marital status was measured dichotomously, with individuals categorized as being married or not married. Insurance status categories were private, public, and uninsured. Education was measured in six categories: Grade 8 or below, some high school, GED/high school completion, some college, bachelor’s degree, and advanced degree. Family poverty status was categorized as poor or near poor, low income, middle income, or high income. Physical health categories were excellent, good or very good, fair, and poor. MSA was measured dichotomously as yes (residing in MSA) or no (residing outside of an MSA).
Mental health diagnoses were identified using the International Classification of Diseases–Ninth Revision classification codes used in the medical conditions file of MEPS. A categorical indicator of diagnosis was created, where an individual was classified as having no diagnosis, 1 diagnosis, 2 diagnoses, 3 diagnoses, or 4+ diagnoses. A new measure of severity was developed using the number of inpatient hospital admissions and emergency room (ER) visits related to a psychotropic condition. Individuals with no ER or inpatient admissions were classified as having low severity mental health. Individuals with 1 inpatient admission or 1-2 ER visits related to a psychotropic condition were classified as having moderate severity mental health. An individual with 2+ inpatient admissions or 3+ ER visits related to a psychotropic condition were classified as having high severity mental health issues. Drug class categories were identified in MEPS based on Multum Lexicon drug classifications (see Table 1).
Medical Expenditure Panel Survey Psychotropic Drug Class Categories.

Note. Categories developed by Cerner Multum, Inc.
Statistical Analyses
To develop descriptive statistics, Pearson chi-squared tests were used. Correlation matrices were produced to examine collinearity among the predictors; however, minimal evidence was found (Tabachnick & Fidell, 2001). Two-part probit generalized linear model (GLM) models were used for analysis. The first part of this model was estimated using a probit model to assess the association between race and the likelihood of any psychotropic drug use. In the second part of the model, differences by race in expenditures were calculated among individuals who used at least one psychotropic drug using GLM. Results from the Park test suggest that the Gaussian family be used in the GLM analysis. In both parts of the model, four heuristic models were conducted, first looking at race alone, followed by race and mental health indicators. Model 3 was run with race, demographic covariates, as well as mental health indicators. In Model 4, physical health status was added. Appropriate survey weighting techniques were applied according to MEPS survey documentation. All data were analyzed using Stata/IC 11.2.
Results
Table 2 presents data on the 45,198 men with complete demographic, medical conditions, and prescription medicine data. Sixteen percent of these men reported psychotropic drug use, with mean expenditures of $696.1. Whites report 17.6% drug use, the highest among all the racial and ethnic groups. Blacks report the highest overall mean psychotropic drug expenditure at $1038. Across the entire sample, the mean characteristics are age-group between 45 and 54 years, privately insured, completed high school, high income relative to the poverty line (greater than or equal to 400% of the poverty line), good or very good mental health, no mental health diagnoses, low disease severity, married, a mental health component score of 50.8, and resides in an MSA.
Distribution of Demographic Characteristics, Drug Use, and Expenditures of Adult Men; Medical Expenditure Panel Survey 2000-2009.

Source. Medical Expenditure Panel Survey 2000-2009.
The first analysis (Table 3) examines the likelihood of minority men using psychotropic drugs, compared with Whites. Significant racial disparities exist in likelihood of drug use before controlling for confounding factors. Black, Hispanic, and Asian men reported a 6%, 5.8%, and 9% lower likelihood of drug use compared with Whites, respectively. After controlling for mental health diagnoses, MCS score, disease severity, age, marital status, insurance status, education, poverty, and physical health, disparities persisted. In Model 4, it is shown that Black, Hispanic, and Asian men were less likely to use psychotropic drugs compared with White men by 4.3, 3.8, and 4.5 percentage points, respectively. From Model 4, men who reported good or very good, fair, or poor health also had a greater likelihood of psychotropic drug use than those who reported excellent health (1.8, 6.1, and 9.6 percentage points, respectfully). Every 1 point increase in mental health component score was associated with a 0.2 percentage point decrease in use of psychotropic drugs (MCS score range is 0-100, where 50 represents the population mean). A greater number of mental health diagnoses were associated with an increased likelihood of drug use. In addition, residence in an MSA was associated with a 1.7 percentage point lower likelihood of psychotropic drug use.
Part 1: Marginal Effect of Demographic Characteristics and Health Status Indicators on Likelihood of Drug Use Among Adult Males; Medical Expenditure Panel Survey 2000-2009.
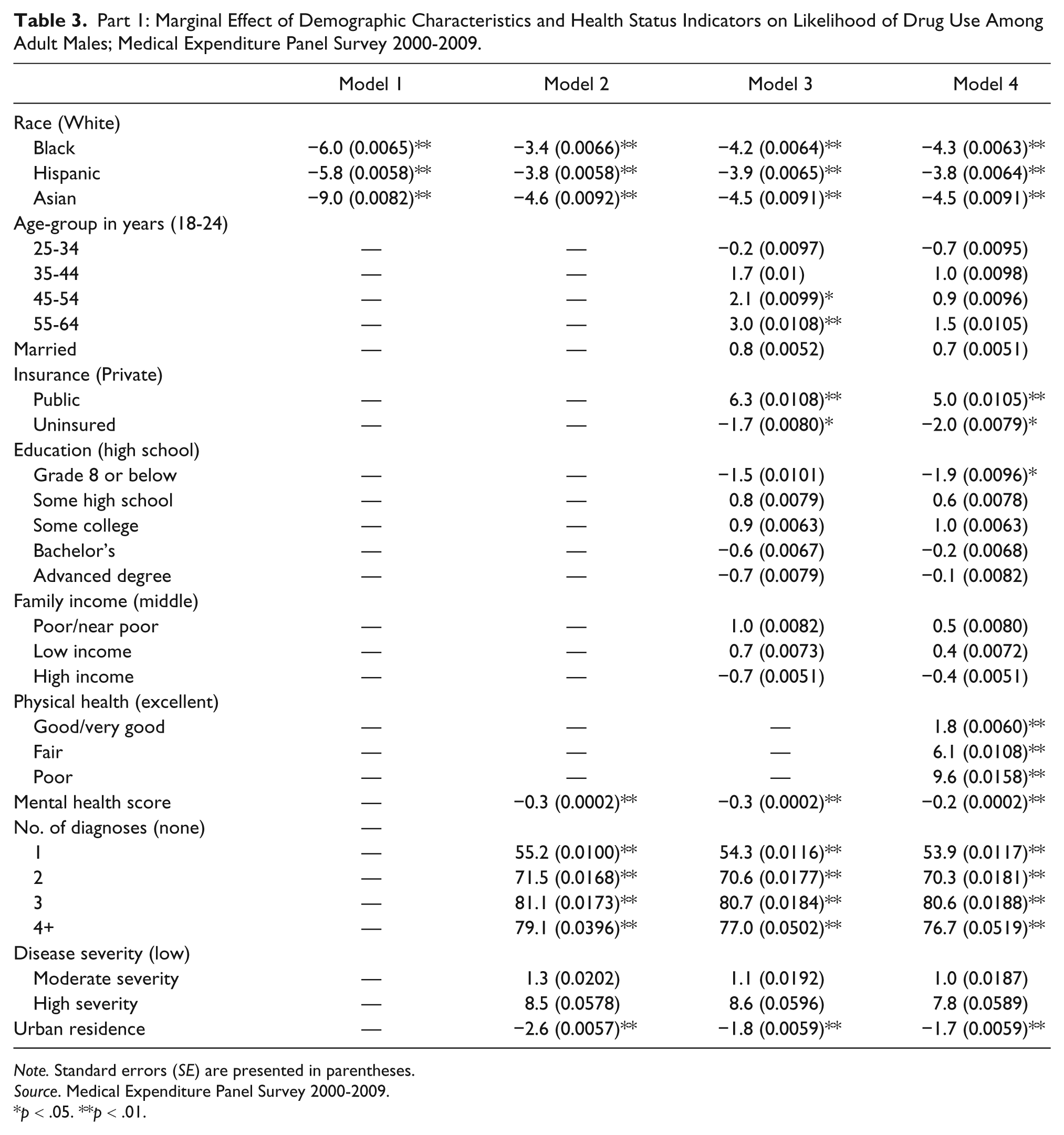
Note. Standard errors (SE) are presented in parentheses.
Source. Medical Expenditure Panel Survey 2000-2009.
p < .05. **p < .01.
Results of the GLM regression revealed that expenditures on psychotropic drugs were not statistically significant for any racial/ethnic group, compared with Whites (Table 4). In Models 1 and 2, Blacks experienced $381 and $345 in greater drug spending than Whites, respectively. This difference is eliminated once additional covariates are added to the model. There were no significant differences in the expenditures of Hispanic and Asian men compared with White men in any of the models. Variables that were statistically significant in predicting drug expenditures were being married ($84.5 lower expenditures), having public insurance and being uninsured ($477.7 greater expenditures, $139.6 lower expenditures, respectively), mental health component score ($4.1 greater expenditures for every 1 point increase in score), and MSA ($140.90 greater expenditures). As expected, mental health diagnoses were also positively correlated with expenditures, after controlling for confounding factors. Having four or more diagnoses increased expenditures by an average of $1600.
Part 2: Drug Expenditures Among Adult Males With >0 Expenditures.

Note. Standard errors (SE) are presented in parentheses.
Source. Medical Expenditure Panel Survey 2000-2009.
p < .05. **p < .01.
Discussion
Summary
Racial and ethnic disparities uncovered in the use of psychotropic drugs present issues of adequate access to these drugs for men. Among individuals that indicated that they had a mental health problem and sought treatment, Blacks, Hispanic, and Asian men are significantly less likely to report using psychotropic drugs compared with Whites. These differences are most profound for Asian men (4.5 percentage points lower), followed by Black (4.3 percentage points lower), and Hispanic (3.8 percentage points) men. This is consistent with previous mental health literature, which revealed disparities between Whites and racial and ethnic minorities in mental health care access, and presents new, important evidence that this disparity persists for men.
There were no significant racial disparities in expenditures among American men who use at least one psychotropic drug, even when controlling for need, likelihood of use, and social and economic factors. The lack of disparities in drug expenditures implies that once minority men gain access to drugs, the spending in these racial and ethnic groups are comparable to that of Whites. Severity of disease is also a measure created for this study that is important to control for in considering disparities in expenditures and may have accounted for differences in spending between groups. These findings are inconsistent with previous research that indicate minorities have lower mental health drug expenditures than Whites (Han & Lui, 2006; McGuire et al., 2006). In those studies, the authors did not examine disparities in mental health expenditures specifically by gender. The National Alliance on Mental Illness (2009) reported that more than six million men have at least one episode of major depression each year, illustrating the need for adequate mental health care access and treatment for this population. The findings from this study underscore the importance of examining disparities in mental health expenditures by gender.
An interesting finding that is consistent in both parts of the model is that individuals with public insurance experienced a greater likelihood of drug use and high drug spending and uninsured individuals experienced lower likelihood of drug use and lower drug spending compared with individuals with private insurance, even after controlling for demographic and health status variables. More research should be done to determine whether those with public insurance do in fact experience greater access to psychotropic care than their counterparts or whether overuse may be an issue.
Strengths and Limitations
In this study, only men with complete demographic, medical conditions, and prescribed medicines data were included in the analytic sample, reducing the amount missing data in the analyses. The responses of men that were omitted may vary from those who were included in the study, but it is unlikely that this small sample would change the direction of our findings. The small sample size of men across racial and ethnic groups taking psychotropic drugs in may reduce the overall power of the study. Ten years of data were pooled in order to address this limitation and make the data more robust.
Self-reporting of information is also an issue, as individuals may differ in their perception of illness, and in their experiences throughout the year. Mental and personal health, diagnosis, and prescription drug information were all collected based on what an individual reports to survey collectors. For example, if a surveyor inquires into overall perceived health status, an individual may associate this with having a bad day or physical disability and report poor overall health, although actual indicators of health, including cardiovascular and immune function, may be okay. Nevertheless, previous research has indicated that self-reported information is a good proxy for true health status.
It is important to note that the researchers are unable to determine whether patients are not using psychotropic drugs because they were not prescribed or whether it is the patient’s conscious decision to not use drugs. It is possible that some of the differences reported, even after controlling for confounding factors, are a factor of patient preferences, culture, and/or individual beliefs. The issue of providing a sufficient amount of care and reducing the gap of disparities in care, while taking into account desire and cultural interpretation of illness can be referred to as the “Conundrum of Health Disparities” (Dilworth-Anderson, Pierre, & Hilliard, 2012). Gaskin, Briesacher, Limcangco, and Brigantti (2006) are among the many researchers who have indicated that disparities are often linked to not only injustices in the health care delivery system but also to differences in cultural perception (Gaskin et al., 2006). In this case, cultural perception may have resulted in thoughts of stigmatization against mental illness and reluctance in seeking care by minority populations (Gary, 2005). Dilworth-Anderson and Gibson (2002) reported that normalization of symptoms as being associated with aging were more prevalent among African Americans than Whites, leading them to delay or put off seeking care for mental health issues (Dilworth-Anderson & Gibson, 2002).
This study has several strengths. MEPS data represent a large nationally representative sample, which makes the results of the two-part study generalizable to the greater population. The use of a large, pooled sample is also a strength for this research. Next, this study appropriately measures mental health disparities based on actual need and confounding factors. It reveals more than just differences between populations; social injustices in access to psychotropic medications are exposed and open the door for new research related to a vulnerable population that has been shown to be underresearched (Williams, 2003). Finally, this is among the first studies to comprehensively explore the issue of psychotropic drug spending specifically for men.
Directions for Future Research
The Institute of Medicine suggests a comprehensive, multi-level strategy as the only way to eradicate disparities among racial/ethnic minorities. This strategy would incorporate better educational programs surrounding mental illness diagnosis and drug use for both the patient and his or her family. Specialized programs in predominately minority communities can inform individuals of the issues related to diagnosis and treatment of mental disorders and facilitate better access to mental health care drugs and facilities. Health plans, Accountable Care Organizations, and health care providers must ensure that their patients are receiving the proper care. Finally, policy makers should also use the outcomes of this and similar research to consider addressing patient preferences and needs. This can be done through cultural competency training for providers in order to not only ensure baseline equity in prescribing for individuals with the same diagnosis and need, but to also address what patients want and how it correlates to improving their mental health outcomes. Educational initiatives for the patients and their family around the importance of mental health care and the need to not ignore or normalize symptoms is crucial, as normalization can affect patient preferences and decisions and lead to underutilization of needed mental health services by minority men.
The development of tiered public policy has also been suggested as an important way to eliminate mental health disparities (Miranda, McGuire, Williams, & Wang, 2008). These policies would address health disparities by first targeting social disparities in sectors, such as education, housing, and employment. Policies to increase the number of minorities in the health care workforce are also important in addressing provider–patient communication issues that contribute to mental health disparities. The Affordable Care Act includes provisions to do just this (Joint Center for Political and Economic Studies, 2010). Secondly, policies designed to improve overall quality of care, particularly by making interventions appropriate for minorities, have the potential to better health outcomes, improve unmet need for care, and reduce health disparities for minority populations. Last, increasing the amount of research conducted to decrease disparities could better address the protective role of cultural factors as well as help in understanding the role that environmental and social factors play on mental health among males. Learned information could lead to interventions and projects to directly benefit minority men where they need it the most.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grant #P60MD000214 from the National Center on Minority Health and Health Disparities (NCMHD) of the National Institutes of Health (NIH).