
Abstract
Background. Hepatitis C virus (HCV) infection is associated with clinical depression,a condition that is aggravated on interferon-based therapy. In HCV infection, men often appear more resilient to depression than women. However, men are subject to depression in diseases that tend to be comorbid in HCV-infected. Aim. This study examined whether HCV-infected men with baseline comorbidities were more or less susceptible to depression prior to and on treatment. Methods. Patients with chronic HCV infection preparing to begin treatment participated (n = 37). The presence of baseline comorbidities was determined by pretreatment medication regimes. Depression was measured by the Beck Depression Inventory prior to and following 2, 4, 8, and 12 weeks of interferon therapy. Results. At baseline, cohorts with (n = 16) and without (n = 21) comorbidities had equivocal demographics and infection characteristics. Comorbidities did not associate with baseline depression. However, on treatment, men with baseline comorbidities demonstrated an elevated risk for the onset of de novo depression (odds ratio = 19.25; confidence interval = 1.41, 582.14; p = .008). This was not observed for women. Baseline comorbidities did not alter the need for treatment discontinuations or the ability to achieve a sustained viral response. Conclusion. The results of this study suggest that baseline comorbidities render men more susceptible to interferon treatment–induced depression.
Keywords
Introduction
Hepatitis C virus (HCV) infection is a serious health problem with an estimated 170 million individuals chronically infected worldwide (Mohd Hanafiah, Groeger, Flaxman, & Wiersma, 2013; Perz, Armstrong, Farrington, Hutin, & Bell, 2006). Chronic HCV infection can progress to end-stage liver disease in 5% to 20% of cases (Thomas, 2013; Thomas & Seeff, 2005). However, in the absence of overt liver disease or interferon (IFN) treatment, 2% to 29% of chronically HCV-infected patients experience neuropsychiatric disorders such as depression (Dieperink, Willenbring, & Ho, 2000; Yamini et al., 2011). The etiology of depression in HCV infection is not well understood, though it may involve HCV infection of the brain (Bolay, Soylemezoglu, Nurlu, Tuncer, &Varli, 1996; Weissenborn et al., 2009). In addition, tryptophan depletion has been observed in HCV infection implicating a reduced availability of serotonin (Cozzi et al., 2006).
The impact of neuropsychiatric disorders in HCV infection can be further exacerbated by IFN therapy, the backbone of HCV infection treatment (Fried, 2002; Manns et al., 2001; Myint, Schwarz, Steinbusch, & Leonard, 2009). On IFN administration, de novo depression and other neuropsychiatric problems can occur in up to 40% of treated patients (Dienstag & McHutchison, 2006; Dieperink, Ho, Thuras, & Willenbring, 2003; McHutchison et al., 1998). Patient susceptibility to IFN-induced depression may reflect reduced baseline serotonin levels (Loftis et al., 2013). In addition, IFN activates indolamine 2,3-dioxygenase, which redirects tryptophan conversion from serotonin to kynurenine (Taylor & Feng, 1991). Clinical depression generally emerges within the first 12 weeks of treatment, often resulting in modification or discontinuation of the treatment regimen (Dienstag & McHutchison, 2006; Dieperink et al., 2003; McHutchison et al., 1998).
The occurrence of neuropsychiatric events can be influenced by a number of factors including gender (Hinz, Brahler, Möde, Wirtz, & Bosse-Henck, 2012; Michal et al., 2013; Nakaya et al., 2013). Previous reports suggest that being male is protective to the development of depression in HCV infection and on IFN treatment (Ashrafi et al., 2012; Erim et al., 2010; Yamini et al., 2011). However, this has not been universally observed (Golden, O’Dwyer, & Conroy, 2005; Hauser et al., 2002; Martin-Santos et al., 2008). In addition, comorbidities common to HCV infection, including hypertension, are associated with depression in men (Fiedorowicz, He, & Merikangas, 2011). Thus, clinical acceptance that men may be less susceptible to treatment-induced depression may have ramifications for preparing men for the possibility of this therapeutic side effect.
The present study was designed to enable clinicians to more effectively assess the risk of treatment-induced depression in men by determining whether baseline comorbidities served as a potential predisposing factor.
Method
Study Participants
This study was approved by the -University of Manitoba Research Ethics Board. In accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments, patients provided informed consent. Participants were recruited from the Viral Hepatitis Investigation Unit in -Winnipeg, MB. Adult patients with chronic HCV infection preparing to undergo IFN-based treatment were invited to participate in the study on a consecutive basis. In addition to standard exclusion criteria for treatment, participants had to be negative for serologic evidence of HIV and HBV infections. Ten individuals declined participation. One individual was excluded from analysis due to being actively medicated for depression at baseline.
Baseline patient demographics, liver enzymes serum aspartate and alanine aminotransferase levels, -viral loads and viral genotype were recorded. The presence of baseline comorbidities with HCV infection was defined as (a) having a drug prescription for another health condition as indicated in clinical charts (n = 13) or as (b) evidence for the presence of cirrhosis based on biopsy or ultrasound results (n = 3).
Treatment Protocol
Study participants were treated with 1.5 µg kg−1 day−1 of peg-IFN-α2b (67%, Schering-Plough Canada, Kirkland, Quebec, Canada) or 180 µg/day of peg-IFN-α2a (33%, Roche Canada, Mississauga, Ontario, Canada) plus ribavirin (800-1200 mg day−1) according to standard of care. Sustained viral responses were assessed 6 months after the end of treatment.
Report on Psychometrics of Instrument
Participants were evaluated for depression by one research nurse using the Beck Depression Inventory (BDI), a widely used and standardized instrument (Krueger et al., 2011; Loftis, Huckans, Ruimy, Hinrichs, & Hauser, 2008). The shorter 13-item questionnaire version was chosen because the reduced somatic symptom content is considered less influenced by concurrent medical illness (Reynolds & Gould, 1981). A diagnosis of depression was assigned to patients with BDI scores of ≥10. This score has been demonstrated to be highly reliable for the detection of moderate to severe depression under many conditions (Furlanetto, Mendlowicz, & Romildo Bueno, 2005; Leahy, 1992; Scogin, Beutler, Corbishley, & Hamblin, 1988).
In addition to the baseline visit, the questionnaire was administered during regularly scheduled clinical appointments on weeks 2, 4, 8, and 12 of therapy.
Data Analyses
Differences in categorical data were determined by Fisher’s exact test. The interaction of depression and comorbidities was examined by the Mantel–Haenszel test. Differences in the medians of a parameter were evaluated using the nonparametric Mann–Whitney U test. Odds ratios with 95% confidence intervals were calculated for selected outcomes. P < .05 was considered significant.
Results
Study Population
Thirty seven individuals with chronic HCV infection were included in this study (Table 1). Based on medication records, 16 patients demonstrated baseline comorbidities as detailed in Table 2, with hypertension being the most prominent. Patients with and without comorbidities had similar percent males and other characteristics (Table 1).
Patient Demographics and Disease Characteristics Based on Baseline Comorbidities.

Note. ALT = alanine aminotransferase (normal values: <26 U/L); AST = aspartate aminotransferase (normal values: 10-32 u/L); IU = international units; SVR = sustained viral responses.
Categorical differences were assessed by Fisher’s exact test. No statistically significant differences were observed.
Continuous differences were analyzed by the Mann–Whitney test. No statistically significant differences were observed. Shown are median (ranges).
Baseline Comorbidities.

Note. CVD = cardiovascular disease.
Percentage of specific disease within the group of 16 individuals with comorbidities.
Number of individuals that scored positive for treatment-induced depression.
Comorbidities Do Not Affect the Prevalence of Depression in HCV-Infected Men
Evidence of comorbidities in HCV infection was evaluated with respect to BDI scores ≥ 10 (Table 3). At baseline, comorbidities did not associate with increased levels of depression in HCV-infected patients (Table 3). Specifically, for HCV-infected men, comorbidities did not interact with BDI scores (Table 3). Indeed, none of the men with comorbidities (n = 11) displayed indications of depression. In the cohort without defined comorbidities (n = 13), one man (7.7%) demonstrated depression. Median BDI scores were also similar between the cohorts.
Baseline Comorbidities Do Not Associate With Depression in Chronic HCV Infection.
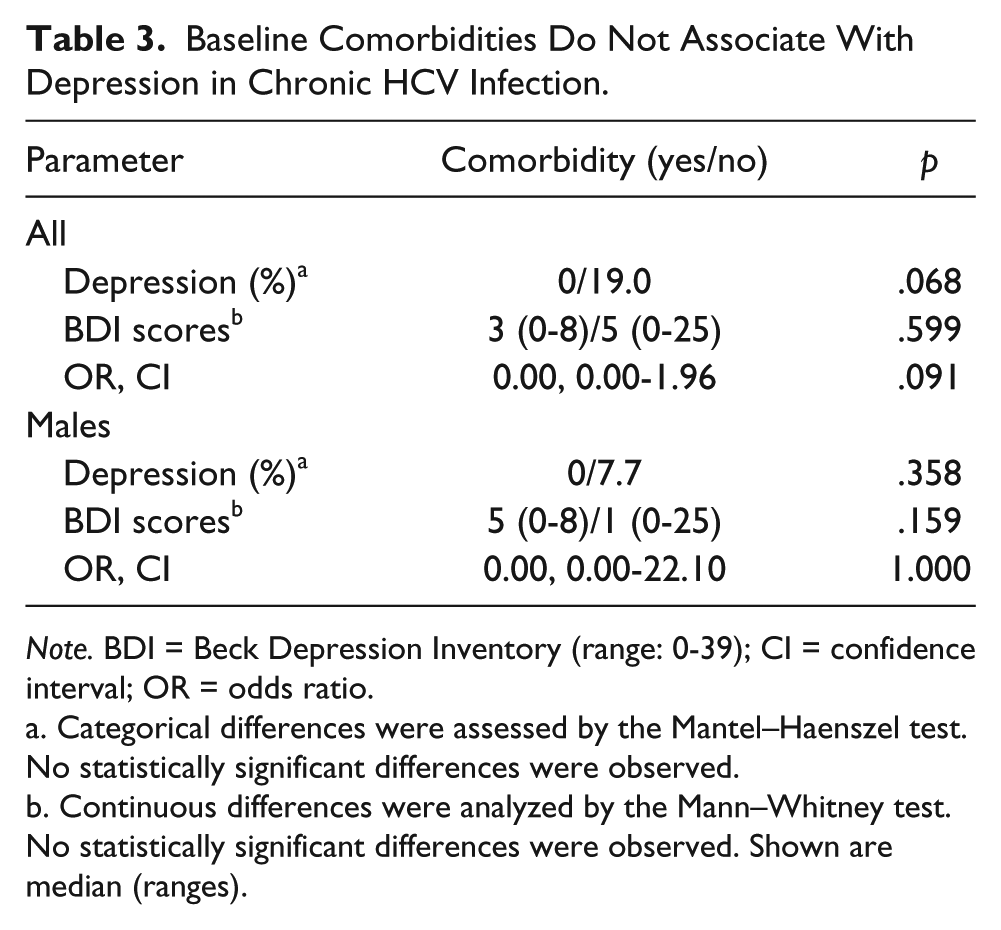
Note. BDI = Beck Depression Inventory (range: 0-39); CI = confidence interval; OR = odds ratio.
Categorical differences were assessed by the Mantel–Haenszel test. No statistically significant differences were observed.
Continuous differences were analyzed by the Mann–Whitney test. No statistically significant differences were observed. Shown are median (ranges).
Men With Baseline Comorbidities Have a Greater Incidence of Treatment-Induced Depression
On treatment, patients with baseline comorbidities relative those without comorbidities displayed a twofold increase in the onset of de novo depression (p = .058, Table 4). Moreover, men with baseline comorbidities demonstrated a 7.7-fold greater incidence of de novo depression than men without comorbidities (p = .007, Table 4). As a result, men with baseline comorbidities were subject to a markedly enhanced susceptibility to de novo depression (odds ratio [OR] = 19.25; confidence interval [CI] = 1.41, 582.14; p = .008). This was not observed for women patients (Suppl. Table 1; available online at http://ajmh.sagepub.com/content/by/supplemental-data.Patient gender as an independent variable did not influence the incidence of baseline or treatment-induced depression (Suppl. Table 2; available online at http://ajmh.sagepub.com/content/by/supplemental-data).
Baseline Comorbidities Are Associated With De Novo Treatment-Induced Depression in Men.

Note. BDI = Beck Depression Inventory (range: 0-39); CI = confidence interval; OR = odds ratio.
Categorical differences were assessed by the Mantel–Haenszel test. No statistically significant differences were observed.
Continuous differences were analyzed by the Mann–Whitney test. No statistically significant differences were observed. Shown are median (ranges).
Lastly, the presence of baseline comorbidities did not affect treatment discontinuations or the ability to achieve sustained viral responses (Table 1).
Discussion
This study raises the possibility that for HCV-infected men the presence of baseline comorbidities contributes to the onset of IFN treatment–induced depression.
HCV infection is associated with neurological disorders (Dwight et al., 2000; Fletcher & McKeating, 2012). This study observed that 10.8% (n = 4/37) of HCV-infected individuals had symptoms of depression in keeping with previous estimates of 2% to 29% (Dieperink et al., 2000; Yamini et al., 2011). Understanding the etiology of depressive disorders in this population is complicated by the high rate of comorbidity in HCV infection (El Garf et al., 2013; Louie, St Laurent, Forssen, Mundy, & Pimenta, 2012; Roed, Lebech, Kjaer, & Weis, 2012). Chronic inflammatory diseases such as hypertension and autoimmune disorders are linked with conditions of psychological distress (Hinz et al., 2012; Michal et al., 2013; Nakaya et al., 2013; Viinamaki et al., 2009). A clear association between diagnoses of cardiac disease and major depression has been established (Findley, Shen, & Sambamoorthi, 2011). In this HCV-infected cohort, 43% patients were on medications for additional health conditions at baseline, with hypertension being the dominant indication (50%, Table 2). However, the presence of comorbidities did not increase the prevalence of depression in HCV-infected male patients (Table 3). Thus, there was no indication that comorbidities in chronic HCV infection enhanced depression levels. This suggests that the potential psychological effects of comorbidities did not surpass those of chronic HCV infection.
Independent of HCV infection, pharmaceutical doses of IFN triggers the onset of depression (Asnis & De La Garza, 2006; Bonaccorso et al., 2002). Considering the influence of chronic inflammatory conditions on mood disorders, the impact of preexisting comorbidities on treatment-induced depression was examined. When comparing the effect of comorbidity, there was a twofold greater increase in de novo depression for patients with comorbidities relative to those without comorbidities (p = .058, Table 4). This observation solely reflected events within the male cohort.
In men, the presence of baseline comorbidities resulted in a sevenfold greater incidence of treatment-induced depression, with an OR equal to 19.25 (CI = 1.41, 582.14; p = 0.008; Table 4). This was not observed for women (Suppl. Table 1; available online at http://ajmh.sagepub.com/content/by/supplemental-data). This contrasts population studies where men are often cited as being less susceptible to depression than women (Howell, Brawman-Mintzer, Monnier, & Yonkers, 2001; Parker & Brotchie, 2010). Aligning with those publications, HCV-infected males have been described as having a lower prevalence of depression than their female counterparts (Ashrafi et al., 2012; Erim et al., 2010; Yamini et al., 2011). Similarly, men are reported as being less vulnerable to IFN treatment–induced depression (Baranyi et al., 2013; Shakoor et al., 2010). These observations are thought to be a consequence of biological differences in serotonin, dopamine or GABAergic pathways, as well as gender-specific environmental stressors (Parker & Brotchie, 2010; Rucci et al., 2009; Sershen, Hashim, & Lajtha, 1998). Other reports indicate that gender does not influence depression in HCV-infected populations orupon IFN treatment, as observed in this study (Suppl. Table 2; available online at http://ajmh.sagepub.com/content/by/supplemental-data) (Golden et al., 2005; Hauser et al., 2002; Martin-Santos et al., 2008). The inconsistency between these reports may reflect the extent of baseline comorbidities, which is generally not accounted for when studying depression in chronic HCV infection.
It is increasingly recognized that specific disease manifestations can differentially influence the onset of depression in men and women (Fiedorowicz et al., 2011; Gentil, Vasiliadis, Préville, Bossé, & Berbiche, 2012; Hartley et al., 2012; Mossakowski, 2009; Viinamaki et al., 2009). Hypertension and cardiovascular disease are implicated as stronger factors for neuropsychiatric disease in men than women (Fiedorowicz et al., 2011; Gentil et al., 2012; Hartley et al., 2012). Fiedorowicz et al. (2011) reported that vascular disease, defined as a self-report of stroke, cardiac disease, or heart attack, was associated with a lifetime occurrence of major depressive disorders in men (OR = 1.85; 95% CI = 1.17, 2.92) but not in women (OR = 1.52; 95% CI = 0.93, 2.49) (Fiedorowicz et al., 2011). The interaction between cardiovascular disease and depression involves multiple mechanisms including increased inflammatory, sympathetic nervous system and hypothalamic-pituitary-adrenal axis activity (Nemeroff & Goldschmidt-Clermont, 2012). The accumulated effects of altered biological pathways can further increase susceptibility to depression (Hartley et al., 2012). These sex-based physiological characteristics were not distinguishable at baseline (Table 3), perhaps being confounded by the ability of HCV infection to trigger similar pathways (Cozzi et al., 2006). However, on administration of pharmacological doses of IFN, there appeared to be a physiological shift such that for men baseline comorbidities strongly correlated with the onset of therapeutically induced depression (Table 4). Whether this shift involves genetic polymorphisms that can confer gender-specific influences is unknown. Brain-derived neurotrophic factor polymorphisms, for example, can modulate the interaction between cardiovascular disease and depression in women (Bozzini et al., 2009). Thus, yet unidentified genetic polymorphisms may link cardiovascular disease to depression in men and render them more susceptible to IFN-induced depression.
There are a number of caveats to this study that warrant emphasis. First, as with many patient-based studies, the interpretation of the data is limited by the sample size. Thus, the possibility of type I or II errors must be considered. In addition, it has been hypothesized that in studies of depression, men tend to underreport symptoms (van Noorden et al., 2010). Finally, because BDI testing was only undertaken at baseline and for 3 months following the initiation of IFN-based therapy, no comments can be made regarding the incidence or severity of late-onset depression or the reversibility of this condition following discontinuation of treatment.
In conclusion, the presence of comorbidities was not associated with a higher prevalence of depression in chronic HCV-infected male patients. However, men with baseline comorbidities had a greater risk for developing IFN treatment–induced depression.
Footnotes
Acknowledgements
The authors would like to thank Claudia Watson (R.N.) and the other nursing staff at the Viral Hepatitis Investigation Unit, Winnipeg, Manitoba for their assistance in patient recruitment, along with -research nurse Kim Hawkins (R.N.) for managing the cohorts.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Thorlakson Foundation and Manitoba Health Research Council. The author(s) would like to thank these agencies for their support.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.