
Abstract
This study was designed to replicate the study of Levant, Wimer, and Williams (2011), which reported complex relationships between masculinity and health behaviors using a more diverse sample and updated measures. A sample of 589 college and community-dwelling men responded to an online survey consisting of five scales. Levant et al.’s (2011) study was partially replicated—some masculinity constructs were identified as protective buffers for some health behaviors and others as risk factors. The vast majority of the findings that were replicated were risk factors, suggesting that traditional masculinity is more of risk than a buffer, and occurred in the analyses involving Avoiding Anger and Stress and Avoiding Substance Use subscales, suggesting that these health behaviors are most closely associated with masculinity. The results are discussed in terms of limitations, suggestions for future research, and implications for health care practice.
Recent research estimates that risky behavior accounts for half of all morbidity and mortality (Mokdad, Marks, Stroup, & Gerberding, 2004). American men tend to engage in more than 30 controllable behaviors that increase their risk for disease, injury, and death (Courtenay, 2000a, 2000b), which may at least partly explain why American men live an average of 5.2 years less than American women (Minino, Heron, Murphy, & Kocharek, 2007). Men spend less time with their physicians; have poorer diets, sleep hygiene, physical activity, and weight management; engage in fewer preventive health behaviors; consume more alcohol; and use more tobacco products than women (Centers for Disease Control, 2004; Galuska, Serdula, Pamuk, Siegal, & Byers, 1996; Garfield, Isacco, & Rogers, 2008; Kandrack, Grant, & Segall, 1991; Shi, 1998). Research on the variables that influence men’s health behaviors is thus of considerable importance (Addis et al., 2007; Baker, 2001; Bonhomme, 2007).
Masculinity has long been thought to be implicated in men’s health risk behaviors. For example, the title of an influential article in the late 1970s was “Warning: The male sex role may be dangerous to your health” (Harrison, 1978). This thinking has stimulated research (Courtenay, 2000a). However, recent studies indicate that the relationships between masculinity and men’s health behaviors appear to be more complex than had previously been assumed, in that, in addition to masculinity being associated with health risk behaviors, some aspects of masculinity were found to be associated with health promotion behaviors and could be considered protective health buffers.
An investigation of the relationships between three multidimensional masculinity constructs and five dimensions of health promotion behaviors found that the relationship between health behavior and masculinity depends on which dimension of health behavior one is interested in predicting, and which facets of masculinity one is using as predictors (Levant, Wimer, & Williams, 2011). The masculinity constructs were the endorsement of traditional masculinity ideology, measured by the Male Role Norms Inventory–Revised (MRNI-R; Levant, Rankin, Williams, Hasan, & Smalley, 2007), conformity to masculine norms, measured by the Conformity to Masculine Norms Inventory (CMNI; Mahalik et al., 2003), and gender role conflict as measured by the Gender Role Conflict Scale (GRCS; O’Neil, Helms, Gable, David, & Wrightsman, 1986). The five dimensions of health promotion behaviors were measured by the Health Behavior Inventory–20 (HBI-20; Levant et al., 2011), and included Diet, Preventive Self-Care (PSC), Proper Use of Health Care Resources (Including Medications; PUHCR), Avoidance of Anger and Stress, and Avoidance of Substance Use.
The investigators reported that when looking at the total scores for the masculinity and health behavior measures, only the CMNI predicted overall health promotion behaviors (Levant et al., 2011), and, as it was negatively associated with health promotion behaviors, was viewed as a risk factor, replicating two prior results (Hamilton & Mahalik, 2009; Mahalik et al., 2003). When looking at the subscale scores for the masculinity and health behavior measures, Levant et al. (2011) reported that scores on the CMNI Pursuit of Status, Playboy, Risk-Taking, and Self-Reliance scales and the GRCS Restrictive Emotionality scale were negatively related (and thus may be health risk factors), whereas scores on the CMNI Winning, Primacy of Work, and Emotional Control scales were positively related (and thus may be health protective factors), to one or more scores on HBI-20 subscales. In addition, scores on the MRNI-R were negatively related to one HBI-20 subscale and positively related to another, and scores on the CMNI Dominance scale were negatively related to two HBI-20 subscales and positively related to a third. Thus, while some masculinity scales were associated with health risk, others were associated with positive health behaviors, and some were associated with both health risk and with positive health behaviors. There is no obvious explanation for this complex pattern of relationships between masculinity constructs and health behaviors, which therefore demands further investigation.
The Present Study
We hypothesized that the findings of Levant et al. (2011), which were based on a study of college men that used the full scales for the CMNI and GRCS and also included the Attitudes Toward Seeking Professional Psychological Help (ATSPPH) as one of the predictors, would be at least partially replicated in a broader sample that included both college and community-dwelling men. Moreover, the partial replication would also use updated short scales for the CMNI (CMNI-46) and the GRCS (GRC-SF), but would not use the ATSPPH. The exploratory part of the study was to determine which findings were replicated under somewhat different conditions in order to determine any underlying order in the findings.
Method
Power Analysis
Levant et al. (2011) reported adjusted R2s from five multiple regression analyses ranging from .04 to .23, with an average of .12; hence, we estimated a small effect size for the present study. For multiple regression with up to 28 predictors, an f2 = .15, power of .95, and an alpha error probability = .05, and using two-tailed tests, the necessary sample size is 90 participants, which our N (589) exceeds.
Participants
A total of 589 men participated in the study. Most participants identified as White/European American (452, 76.7%), whereas 46 (7.8%) identified as Asian/Asian American, 33 (5.6%) as Black/African American, 27 (4.6%) as Latino/Hispanic, and 24 (4.1%) identified as American Indian, Middle Eastern, or Bi/Multiracial. The remainder checked “Other” or did not respond. Ages ranged from 18 to 63 years, with a mean of 23.01 years (SD = 1.13). Most participants indicated that they were either not currently dating anyone (230, 39.0%) or dating one person exclusively (162, 27.5%), whereas 113 (19.2%) were engaged in casual nonexclusive dating, 73 (12.4%) were married/partnered/engaged, and 10 (1.7%) were divorced, separated, or widowed. The remainder did not respond. In response to the question “Whether or not you are sexually active, would your preferred partner be . . .?” most participants (521, 88.5%) selected “always female,” 48 (8.1%) selected “always male,” and 19 (3.1%) selected either “usually female but sometimes male,” “equally likely to be either,” or “usually male but sometimes female.” The remainder did not respond. Most participants reported that the highest degree that they completed was high school/GED (512, 86.9%), 54 (9.2%) reported bachelor’s degree, and 21 (3.5%) reported either a master’s or a doctoral degree. The remainder did not respond. In terms of self-identified socioeconomic status, most (276, 46.9%) identified as middle class, whereas 30 (5.1%) identified as lower class, 117 (19.9%) as lower middle class, 145 (24.6%) as upper middle class, and 16 (2.7%) as upper class. The remainder did not respond. In terms of family/household income, 160 (27.1%) reported earning $40,000 or less, 194 (33%) reported earning from $40,001 to $80,000, and 225 (38.2%) reported earning more than $80,000. The remainder did not respond. Finally, in regard to religion, most participants identified as Christian (340, 57.7%), but 66 (11.2%) identified as Atheist, 54 (9.2%) as Agnostic, 20 (3.4%) as Jewish, and 95 (16.1%) identified as Muslim, Hindu, Buddhist, Pagan, or other. The remainder did not respond.
Procedure
The present study was part of a larger data collection effort that also resulted in the publication of Wimer and Levant (2013), which analyzed the relationships between the consumption of energy drinks, three masculinity constructs, jock identity, and fraternity membership, and in an article under review (Levant & Wimer, 2013) that tested a multiple mediation model of the links between these three masculinity constructs and general health behaviors. The study was approved by the University of Akron and the Pennsylvania State University Institutional Review Boards. Participants were recruited through undergraduate courses at the two universities and Internet websites and listservs of interest to men. For the University of Akron, undergraduate student participants were solicited from psychology courses and offered an incentive of 2 extra credit points for their participation in the study. Students who wished to participate provided their e-mail address to the research assistant who had visited their classroom, and were subsequently e-mailed the link to the online survey site, which is supported by a commercial survey utility licensed to the University of Akron. For the Pennsylvania State University, students from Introduction to Psychology courses chose to participate in the study in order to partially fulfill the research participation aspect of the course, and they entered the online survey site via the university’s subject pool website. Community participants were solicited by contacting a number of websites and listservs of potential interest to men (e.g., sports, motorcycles, hunting, and fishing), and posting a description of the study, request for participants, and link to the online survey site.
The first page of the survey site provided the informed consent information, and participants who consented clicked “yes” and were taken to the survey. On completion of the survey, participants were provided with an educational briefing on the study, including the rationale and hypotheses, and references with more information on the topic. Once they clicked “done,” they were directed to the incentive fulfillment page, which first asked how they had been recruited for the study, either from one of the two universities or from an Internet website. If they responded that they had been recruited from a university, they were directed to the extra credit or research participation credit pages (which asked for their name, e-mail, course for which they wanted extra credit, and the professor of that course). If they responded that they had been recruited from an Internet website, they were then directed to the raffle page (which asked for their name, e-mail, and address). About 20% of the participants were recruited from the community via the Internet. The incentive fulfillment, extra credit, and raffle pages were not linked to participants’ answers on the survey, thus keeping their answers to the survey completely anonymous.
The survey consisted of 5 scales with 144 questions and took approximately 25 to 35 minutes to complete. It was presented in the following order: Demographic Form, MRNI-R, CMNI-46, GRCS-SF, and HBI-20.
Measures
Demographic Questionnaire
This questionnaire inquired about gender, age, race/ethnicity, relationship status, sexual orientation, highest degree completed, family/household income, socioeconomic status, and religion.
Male Role Norms Inventory–Revised
The MRNI-R is a 53-item measure of traditional masculinity ideology, with items (e.g., “A man should be able to perform his job even if he is physically ill or hurt) rated on a 7-point Likert-type scale (1 = strongly disagree, 7 = strongly agree), and with higher scores indicating higher levels of endorsement of traditional masculinity ideology (Levant, Rankin, Williams, Hasan, & Smalley, 2010). None of the items are reverse-scored. Seven subscales assess individuals’ endorsement of different dimensions of traditional masculinity ideology, but, as noted below, these were not used in the study due to multicollinearity. A total scale score may also be obtained through the averaging of scores on all items (α = .97). Levant et al. (2010) found evidence for the factor structure, reliability of the subscales, and convergent, divergent, and concurrent validity.
Conformity to Masculine Norms Inventory–46
The CMNI-46 (Parent & Moradi, 2009) is a short version of the CMNI (Mahalik et al., 2003). The CMNI assesses “the extent to which an individual male conforms or does not conform to the actions, thoughts and feelings that reflect masculinity norms in the dominant culture in U.S. society” (Mahalik et al., 2003, p. 5). The CMNI-46 assesses conformity to nine masculine norms: Winning (6 items, α = .86), Emotional Control (6 items, α = .87), Primacy of Work (5 items, α = .78), Risk-Taking (5 items, α = .80), Violence (6 items, α = .82), Heterosexual Self-Presentation (6 items, α = .90), Playboy (4 items, α = .80), Self-Reliance (5 items, α = .84), and Power Over Women (4 items, α = .85). Responses to items (e.g., “In general, I will do anything to win”) are made on a 4-point scale (0 = strongly disagree, 3 = strongly agree). Eighteen items are reverse-scored. A total scale score may also be obtained through the averaging of scores on all items (α = .90). CMNI-46 subscales yielded large positive correlations with their parent CMNI subscale (r range = .89-.98; Parent & Moradi, 2009).
Gender Role Conflict Scale–Short Form
The GRCS-SF (Wester, Vogel, O’Neil, & Danforth, 2012), derived from the GRCS (O’Neil et al., 1986) is a 16-item instrument that assesses the degree to which “rigid, sexist, or restrictive gender roles result in personal restriction, devaluation, or violation of others or self” (O’Neil, Good, & Holmes, 1995, p. 167). The GRCS-SF, like the GRCS, has four subscales, supported by numerous factor analyses (O’Neil et al., 1995; O’Neil et al., 2011): Success/Power/Competition (4 items, α = .76), Restrictive Emotionality (4 items, α = .84), Restrictive Affectionate Behavior Between Men (4 items, α = .84), and Conflict Between Work and Family Relations (4 items, α = .82). Participants used a 6-point Likert-type scale (1 = strongly disagree, 6 = strongly agree) to rate their level of agreement or disagreement with statements intended to measure instances of male gender role conflict (e.g., “Affection with other men makes me tense”), with higher scores indicating higher levels of conflict. None of the items are reverse-scored. A total scale score may also be obtained through the averaging of scores on all items (α = .86). O’Neil et al. (1986) reported 4-week test–retest reliabilities for the GRCS subscales ranging from .72 to .86, and O’Neil et al. (1995) reported αs ranging from .75 to .90 and evidence for construct validity. O’Neil et al. (2011) reported that the GRCS-SF subscales had large positive correlations with their parent GRCS subscale (r range = .90-.96).
Health Behavior Inventory–20
To assess health behaviors we used the HBI-20, which resulted from modifications to the Health Risks Inventory (Courtenay, 1998; Courtenay, McCreary, & Merighi, 2002). Exploratory factor analysis found a 20-item, 5-factor instrument (Levant et al., 2011). Three factors reflect health-promoting behaviors: Diet (5 items, α = .86), PSC (3 items, α = .57), and PUHCR (Including Medications; 6 items, α = .84). Two factors are reverse-scored to reflect the avoidance of health risk behaviors: Avoidance of Anger and Stress (3 items, α = .77), and Avoidance of Substance Use (3 items, α = .65). Participants are asked to rate the extent to which each item (e.g., “I fill my medicine prescriptions immediately”) was self-descriptive, using a scale from 1 = always to 7 = never. Subscale scores are obtained by summing participants’ responses (after reverse-coding the risk items) and dividing by the number of items. A total scale score may also be obtained through the averaging of scores on all items (α = .78). Levant et al. (2011) reported αs for the subscales and the full scale ranging from .68 to .79, and evidence for concurrent validity of the HBI-20.
Results
Data Cleaning and Descriptive Statistics
The data were thoroughly screened before conducting statistical analyses to ensure the accuracy of the data file. A total of 743 participants began the survey. After eliminating those who did not complete it and those who identified as female or transgender, the final sample included 589 men, for a completion rate of 80.2%. There were missing data as some participants did not respond to every item. A small amount of missing data was observed (0.29% of the responses), with the number of missing responses per item ranging from 0 to 7. No discernible patterns were found by visually inspecting the missing data, which suggested that they were missing at random. With a small percentage of data points missing in a random pattern from a large data set, the problem is less serious, according to Tabachnick and Fidell (2007). Nonetheless, we took a conservative approach, and replaced missing values using SPSS-19’s Linear Trend at Point method. This is a regression-based imputation method, in which other variables are used as independent variables to write regression equations for the variable with missing data serving as the dependent variable. Cases with complete data generate the regression equation. The equation is then used to predict the missing values for the incomplete cases. Missing values are replaced with their predicted values. Descriptive statistics and bivariate correlations of study variables are presented in Table 1.
Means, Standard Deviations, Cronbach’s Alphas, and Bivariate Correlations of Study Variables.

Note. N = 589. HBI-20 = Health Behavior Inventory–20; MRNI-R = Male Role Norms Inventory–Revised; CMNI-46 = Conformity to Masculine Norms Inventory–46; GRC-SF = Gender Role Conflict–Short Form. Scores for the HBI-20 and the MRNI-R range from 1 to 7, with higher scores indicating greater health promotion behavior and greater endorsement of traditional masculinity ideology, respectively. Scores for the CMNI-46 range from 0 to 3, with higher scores indicating greater conformity to traditional masculine norms. Scores for the GRC-SF range from 1 to 6, with higher scores indicating greater gender role conflict.
p < .05 (two-tailed). **p < .01 (two-tailed).
Replication of Levant et al. (2011)
We conducted multiple regression analyses (using the Enter method) to examine the association of the three measures of masculinity constructs (MRNI-R, CMNI-46, GRC-SF) with the HBI-20. Given the potential for overlap between the three masculinity measures, we examined the data for multicollinearity, or high levels of common variance using the variance inflation factor (VIF). In the regression analysis using total scale scores of the three masculinity measures, the predictors had VIF values ranging from 1.02 to 2.39; hence none reached 2.50, the most conservative threshold (Miles & Shevlin, 2000). Similarly, the bivariate correlations, which can indicate multicollinearity if values are greater than .70, revealed no issues (see Table 1).
In a trial run of the regression analyses using subscale scores of the three masculinity measures, we found that all the subscales of the MRNI-R, two subscales of the CMNI-46 (Power Over Women, Heterosexual Self-Presentation), and one subscale of the GRCS (Restrictive Affectionate Behavior Between Men) had VIF values greater than 2.50. An additional analysis of correlations indicated that the subscales of the MRNI-R were strongly correlated with each other, ranging from .46 to .89, with 14 out of 28 correlations greater than .70, whereas the correlations of the subscales of the CMNI-46 and the GRC-SF were less than .70. Hence, for these analyses, we omitted all the MRNI-R subscales (substituting the total scale score of the MRNI-R), two subscales of the CMNI-46 (Power Over Women, Heterosexual Self-Presentation), and one subscale of the GRCS (Restrictive Affectionate Behavior Between Men). The remaining 11 masculinity scales were used as predictors in the subscale analyses.
We first assessed the relative strength of the total scores of the MRNI-R, CMNI-46, and GRC-SF in predicting HBI-20 total scores. Four demographic variables were significantly correlated with the HBI-20: age, family income, sexual preference, and highest degree completed. Hence we treated these as control variables, and entered them in the first model in the multiple linear regression analysis, which resulted in an adjusted R2 of .045, R2 change of .051, F(4, 573) = 7.77; p < .001. For the second model, we entered the total scale scores for the MRNI-R, CMNI-46, and GRC-SF, which resulted in an adjusted R2 of .136, R2 change of .095, F(3, 570) = 21.23; p < .001. The results are presented in Table 2, where one can see that in the final model scores on family income were positively related to HBI-20 scores (and, thus, a potential protective buffer), whereas scores on the CMNI were negatively related to HBI-20 scores (and thus a potential risk factor).
Regression Analyses of the Prediction of HBI-20 Scores (Total Scale and Subscale Scores) Using Demographic Variables and the MRNI-R, CMNI-46, and GRC-SF (Total Scale and Subscale Scores) as Predictors.

Note. Only the significant results and trends in the final model (Step 2) are reported from these analyses. For the analysis Prediction of HBI-20 Total, predictors were the demographic variables associated with the HBI-20 Total Scale and Total scales of the MRNI-R, GRC-SF, and CMNI-46. For all the other analyses, predictors were the demographic variables associated with the HBI-20 subscale used as the outcome variable, and the 11 masculinity scales (all but two subscales of the CMNI-46, Power Over Women, Heterosexual Self-Presentation, all but one subscale of the GRCS, Restrictive Affectionate Behavior Between Men, and the MRNI-R Total Scale). Outcome variables were all subscales of the HBI-20: AAS = Avoiding Anger and Stress; ASU = Avoiding Substance Use; PSC = Preventive Self-Care; PUHCR = Proper Use of Health Care Resources (Including Medications); Diet = Diet. Predictors: MRNI-R = MRNI-R total scale; C-Win = CMNI-46 Winning subscale; C-EmoCon = CMNI-46 Emotional Control subscale; C-Risk = CMNI-46 Risk-Taking subscale; C-Play = CMNI-46 Playboy subscale; C-SelfRel = CMNI-46 Self-reliance subscale; C-Viol = CMNI-46 Violence subscale; G-RE = GRC-SF Restrictive Emotionality subscale; G-WFC = GRC-SF Conflict Between Work and Family Relations subscale.
We next assessed the relative roles of the subscales of the CMNI-46 and GRC-SF and the total scale for the MRNI-R in predicting each of the five HBI-20 subscale scores. For this we entered as control variables in Model 1 of the regression analyses those demographic variables that correlated with the particular criterion. For Model 2 in the regression analysis, we entered the 11 masculinity scales delineated above.
For the subscale Avoiding Anger and Stress (AAS), age and highest degree completed were entered as control variables in Model 1, which resulted in an adjusted R2 of .019, R2 change of .023, F(2, 584) = 6.72; p = .001. In Model 2, the 11 masculinity scales were entered, which resulted in an adjusted R2 of .23, R2 change of .224, F(11, 573) = 15.53; p < .001. The results are presented in Table 2, where one can see that in the final model scores on the CMNI-46 Emotional Control subscale were positively related to scores on AAS, and scores on the MRNI-R, the CMNI-46 Winning subscale, and GRC-SF Restrictive Emotionality, Conflict Between Work and Family Relations, and Success/Power/Competition subscales were negatively related to scores on AAS. There was also a trend (p = .06) for the CMNI-46 Risk-Taking subscale to be positively related to scores on AAS.
For the subscale ASU, sexual preference was entered as the control variable in Model 1, which resulted in an adjusted R2 of .009, R2 change of .011, F(1, 586) = 6.51; p = .011. In Model 2, the 11 masculinity scales were entered, which resulted in an adjusted R2 of .18, R2 change of .186, F(11, 575) = 12.08; p < .001. The results are presented in Table 2, where one can see that in the final model, scores on the CMNI-46 Winning and Emotional Control subscales and the GRC-SF Success/Power/Competition subscales were positively related to scores on ASU, and scores on the MRNI-R, CMNI Risk-Taking and Playboy scales and the GRC-SF Restrictive Emotionality Scale were negatively related to scores on ASU. There were also trends for the CMNI-46 Winning subscale to be positively related (p = .056) and for CMNI-46 Self-reliance subscale to be negatively related (p = .087) to scores on ASU.
For the factor PSC, socioeconomic status and family income were entered as the control variables in Model 1, which resulted in an adjusted R2 of .009, R2 change of .012, F(2, 575) = 3.62; p = .027. In Model 2, the 11 masculinity scales were entered, which resulted in an adjusted R2 of .04, R2 change of .049, F(11, 564) = 2.69; p = .002. The results are presented in Table 2, where one can see that in the final model there were trends for the MRNI (p = .054) and GRC-SF Success/Power/Competition subscale (p = .061) to be positively related, and for CMNI-46 Self-Reliance subscale (p = .054) to be negatively related to scores on PSC.
For the factor PUHCR (Including Medications), family/household income and sexual preference were entered as the control variables in Model 1, which resulted in an adjusted R2 of .026, R2 change of .029, F(2, 576) = 8.70; p < .001. In Model 2, the 11 masculinity scales were entered, which resulted in an adjusted R2 of .088, R2 change of .079, F(11, 565) = 4.56; p < .001. The results are presented in Table 2, where one can see that in the final model scores on the GRC-SF Success/Power/Competition subscale were positively related, and scores on the CMNI-46 Winning and Risk-Taking subscales were negatively related, to scores on PUHCR. There was also a trend for the CMNI-46 Emotional Control subscale (p = .059) to be negatively related to scores on PUHCR.
For the subscale Diet, age, highest degree completed, and sexual preference were entered as control variables in Model 1, which resulted in an adjusted R2 of .045, R2 change of .05, F(3, 583) = 10.24; p < .0001. In Model 2, the 11 masculinity scales were entered, which resulted in an adjusted R2 of .075, R2 change of .047, F(11, 572) = 2.71; p = .002. The results are presented in Table 2, where one can see that in the final model scores on age and GRC-SF Success/Power/Competition subscale were positively related to scores on Diet, and scores on the CMNI-46 Winning, Violence, and Self-Reliance subscales were negatively related to scores on Diet.
To facilitate the comparison of the results of the regression analyses from Levant et al. (2011) with those of the present study, the beta weights and p values for significant results and trends are displayed in Table 3. There were several notable differences between the two studies. First, as noted above, Levant et al. (2011) used the original scales for the CMNI and GRCS, whereas the present study used the updated short forms of these scales (CMNI-46 and GRC-SF). As a consequence the earlier study included two CMNI subscales that were eliminated from the CMNI-46—Dominance and Pursuit of Status. Hence, these results were not included in Table 3. Second, Levant et al. (2011) included the ATSPPH as one of the predictors, which was not included in the present study. Third, Levant et al. (2011) did not report an analysis with the HBI-20 Total score as outcome variable, and the 11 masculinity scales as predictors, and found no significant predictors for the HBI-20 Diet subscale; hence, these analyses are not reported in Table 3. To compile an accurate picture of the overlap between the findings in the two studies we would have to add in the findings from the present study on Diet to the total findings to have a complete count of the findings from the two studies that were directly comparable. When this is done, 14 of the 43 (32.6 %) significant findings occurred in both studies. Also of note, the percent of variance in outcome variables accounted for the predictors was stable and of moderate size for the analyses with AAS and ASU (17%-23%), stable and small for the analysis with PSC (4%), and unstable for the other three analyses (6%-18%).
Comparison of the Beta Weights (Significant Results and Trends) From Regression Analyses Results of Levant, Wimer, and Williams (2011) With Those of the Present Study.
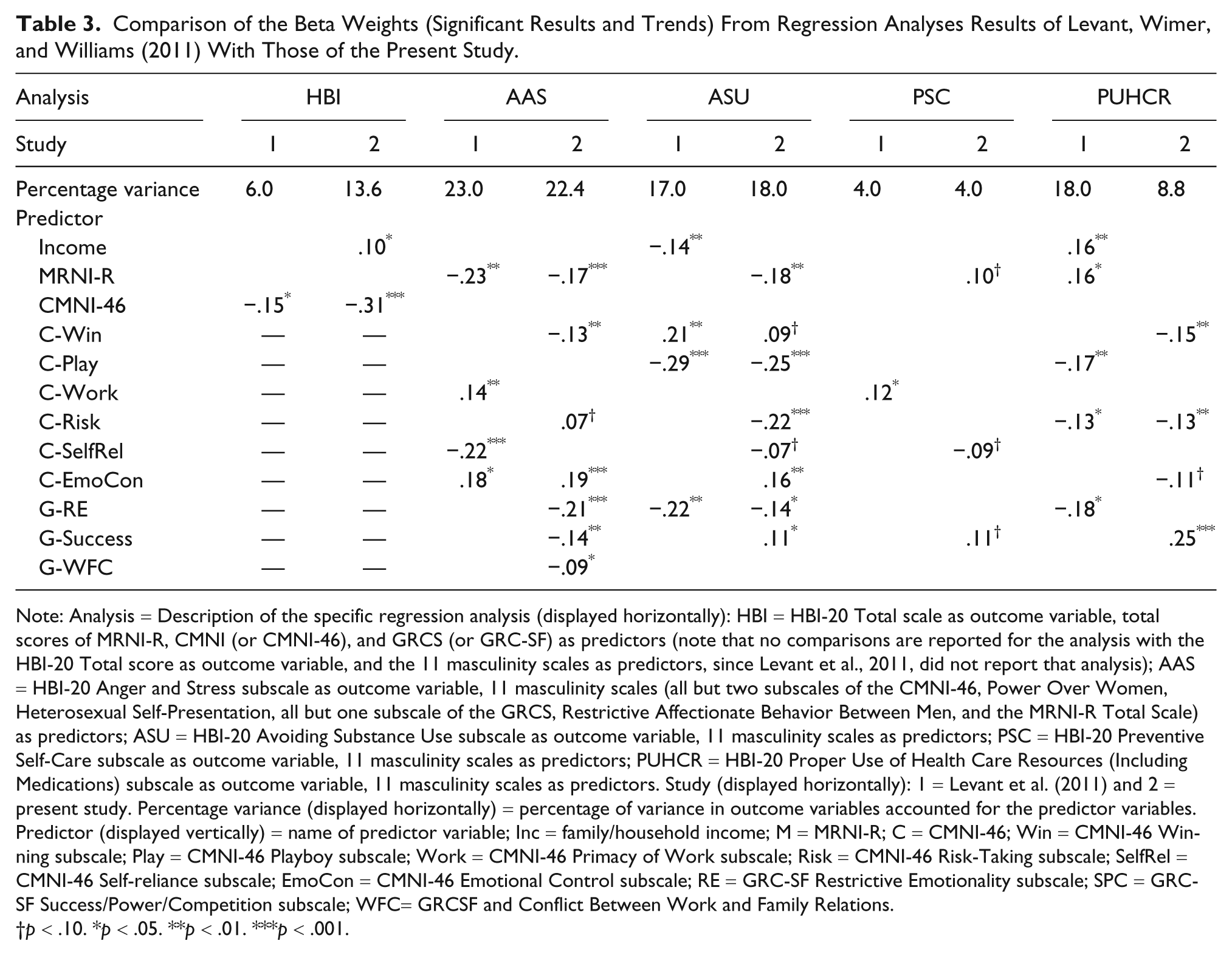
Note: Analysis = Description of the specific regression analysis (displayed horizontally): HBI = HBI-20 Total scale as outcome variable, total scores of MRNI-R, CMNI (or CMNI-46), and GRCS (or GRC-SF) as predictors (note that no comparisons are reported for the analysis with the HBI-20 Total score as outcome variable, and the 11 masculinity scales as predictors, since Levant et al., 2011, did not report that analysis); AAS = HBI-20 Anger and Stress subscale as outcome variable, 11 masculinity scales (all but two subscales of the CMNI-46, Power Over Women, Heterosexual Self-Presentation, all but one subscale of the GRCS, Restrictive Affectionate Behavior Between Men, and the MRNI-R Total Scale) as predictors; ASU = HBI-20 Avoiding Substance Use subscale as outcome variable, 11 masculinity scales as predictors; PSC = HBI-20 Preventive Self-Care subscale as outcome variable, 11 masculinity scales as predictors; PUHCR = HBI-20 Proper Use of Health Care Resources (Including Medications) subscale as outcome variable, 11 masculinity scales as predictors. Study (displayed horizontally): 1 = Levant et al. (2011) and 2 = present study. Percentage variance (displayed horizontally) = percentage of variance in outcome variables accounted for the predictor variables. Predictor (displayed vertically) = name of predictor variable; Inc = family/household income; M = MRNI-R; C = CMNI-46; Win = CMNI-46 Winning subscale; Play = CMNI-46 Playboy subscale; Work = CMNI-46 Primacy of Work subscale; Risk = CMNI-46 Risk-Taking subscale; SelfRel = CMNI-46 Self-reliance subscale; EmoCon = CMNI-46 Emotional Control subscale; RE = GRC-SF Restrictive Emotionality subscale; SPC = GRC-SF Success/Power/Competition subscale; WFC= GRCSF and Conflict Between Work and Family Relations.
p < .10. *p < .05. **p < .01. ***p < .001.
To summarize the replicated results, first, in regard to the analysis of the relative strength of the total scores of the MRNI-R, CMNI (or CMNI-46), and GRCS (or GRC-SF) in predicting HBI-20 total scores, scores on the CMNI (or CMNI-46) were significant predictors in both studies. In both cases they were negatively related to HBI-20 total scores, and thus, may be a risk factor for total health behaviors. In regard to the analyses of the relative roles of the subscales of the CMNI (or CMNI-46) and GRCS (or GRC-SF) and the MRNI-R total score in predicting each of the five HBI-20 subscale scores, we found that in both studies: (a) AAS scores were negatively related to MRNI-R total scores, which thus may be a risk factor for avoiding anger and stress. AAS scores were also positively related to CMNI (or CMNI-46) Emotional Control scores, which thus may be a protective buffer for avoiding anger and stress. (b) ASU scores were negatively related to CMNI (or CMNI-46) Playboy scores and to GRCS (or GRC-SF) Restrictive Emotionality scores which thus may be risk factors for avoiding substance use. ASU scores were positively related to CMNI (or CMNI-46) Winning scores which thus may be a protective buffer factor for avoiding substance use. Finally, PUHCR (Including Medications) scores were negatively related to CMNI (or CMNI-46) Risk-Taking scores, which thus may be risk factors for proper use of health care resources.
Another notable difference between the two studies concerned the participants, which were college men in Levant et al. (2011) and both college and community-dwelling men in the present study. Table 4 presents a comparison of the two studies on the demographic and study variables. It can be seen that the present participants (in comparison with those in the 2011 study) are older, more frequently married, partnered, or engaged, more frequently reporting to be gay, better educated, but reporting similar income. On the study variables, the present participants report engaging in fewer positive health behaviors, but score very similarly to those in the 2011 study on the three masculinity measures.
Comparison of the Demographic and Study Variables of Levant, Wimer, and Williams (2011) With Those of the Present Study.
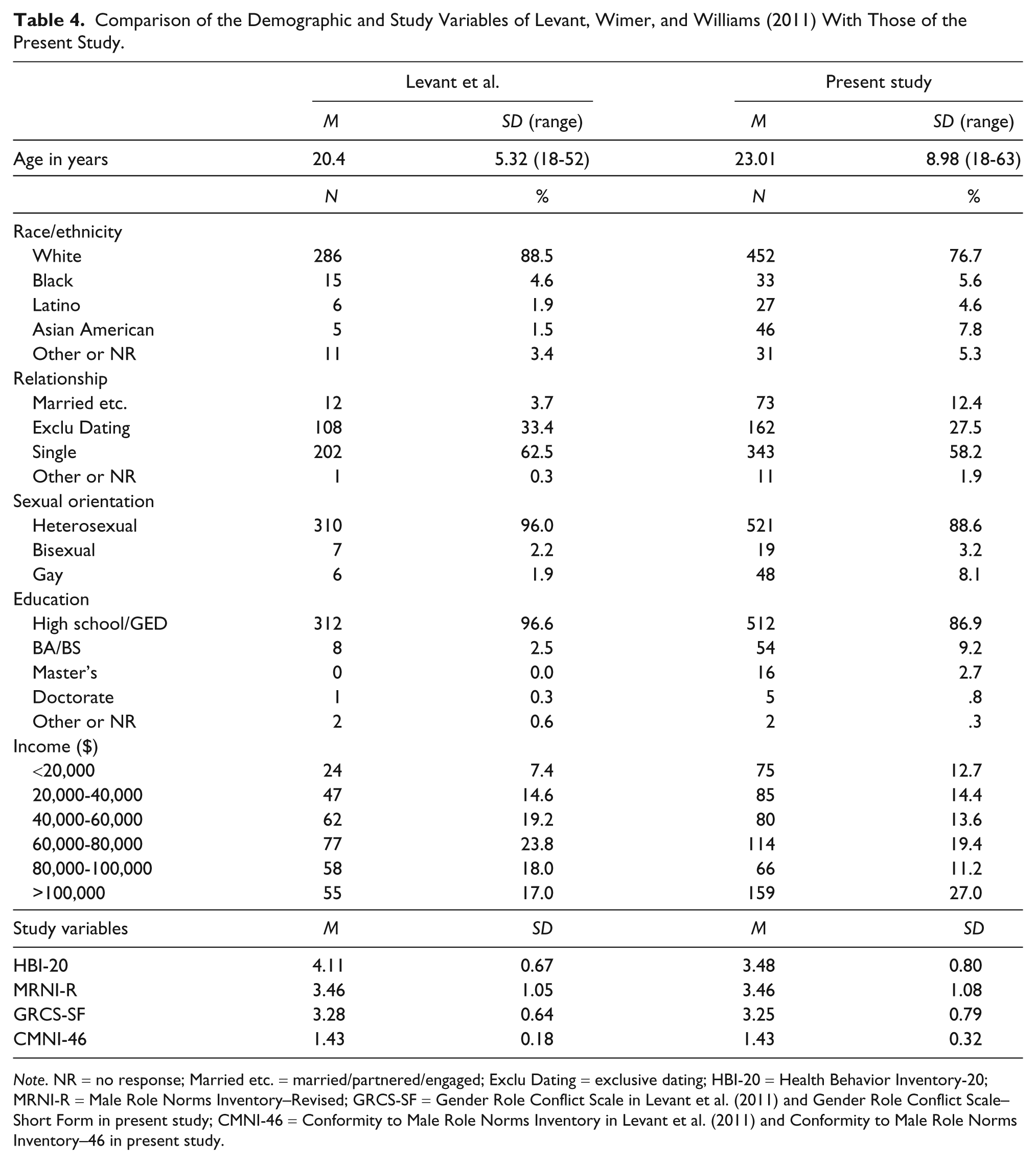
Note. NR = no response; Married etc. = married/partnered/engaged; Exclu Dating = exclusive dating; HBI-20 = Health Behavior Inventory-20; MRNI-R = Male Role Norms Inventory–Revised; GRCS-SF = Gender Role Conflict Scale in Levant et al. (2011) and Gender Role Conflict Scale–Short Form in present study; CMNI-46 = Conformity to Male Role Norms Inventory in Levant et al. (2011) and Conformity to Male Role Norms Inventory–46 in present study.
Discussion
The relationship between health behaviors and masculinity was again observed in the present study to depend on which dimension of health behavior one is interested in predicting, and which facets of masculinity one is using as predictors. Some masculinity constructs appear to be protective buffers for some health behaviors in that they are positively associated with one or more specific health promotion behaviors, whereas others appear to be risk factors for some health behaviors in that they are negatively associated with one or more specific health promotion behaviors. Furthermore, some masculinity constructs appear to be both protective buffers for some health behaviors and risk factors for others.
However, the relationships between specific masculinity constructs and specific sets of health behaviors were not stable across the two studies, as only 32.6% of the findings occurred in both. Some of the instability may be because of the fact that this was not an exact replication, as previously outlined. Some of the instability may also be because of the lower alphas of two of the outcome variables in the present study, the HBI-20 Preventive Self-Care (.57) and Avoiding Substance Use (.65) subscales. In addition, some may be because of differences in the samples, with the first sample consisting exclusively of college students, and the second largely college students but also including 20% community-dwelling adults. Future research should further investigate the reasons for the instability of these relationships between masculinity constructs and health behaviors.
In regard to the exploratory part of the study, of the 14 results that were replicated, 10 (71.4%) implicated masculinity variables as risk factors whereas only 4 indicated that masculinity was a protective buffer. None found masculinity to be a risk in one instance and a buffer in another, suggesting that such a pattern of results, which occurred in each study, may have been an anomaly. In regard to risk factors, scores on the CMNI (and CMNI-46) were implicated as a risk factor for total health promotion behaviors, scores on the MRNI-R were implicated for avoiding anger and stress, scores on the CMNI (and CMNI-46) Playboy and the GRCS (and GRC-SF) Restrictive Emotionality scales were implicated for avoiding substance use, and scores on the CMNI (and CMNI-46) Risk-Taking scales were implicated for proper use of health care resources. This set of results suggests that there are many aspects of masculinity—whether measured as ideology (or views on how men ought to behave), personal conformity to traditional masculine norms, or conflict resulting from norm conformity—that are potentially detrimental to men’s positive health behaviors. This suggests that masculinity overall may be more of a risk factor than a protective buffer for positive health behavior, suggesting that Harrison (1978) may have been right in his long-ago warning that “the male sex role may be dangerous to your health.”
With regard to protective buffers, scores on the CMNI (and CMNI-46) Emotional Control scale served as a protective buffer for avoiding anger and stress. This suggests that conforming to the masculine norm of emotional control may help avoid anger and stress. However, it is puzzling that a very similar construct, namely the conflict that results from controlling one’s emotions, is a risk factor for avoiding substance use. The answer to this riddle is not clear and should be the subject of future research. Scores on the CMNI (and CMNI-46) Winning scale served as a protective buffer for avoiding substance use. This relationship might mean that men who “will do anything to win” are careful about the use of substances as that might reduce their chances of winning.
Most (10 of 14, 71.4%) of the replicated results occurred in the analyses involving two outcome variables: Avoiding Anger and Stress and Avoiding Substance Use. Relatedly, in these analyses, the percentage of variance in dependent variables that was accounted for by the independent variables was stable and of the largest size (17% to 13%). This suggests that these two subscales might constitute those aspects of health behavior that are most closely associated with masculinity constructs. This idea has face validity, as the expression of anger and drinking are associated with traditional masculine norms. Finally, it is also noteworthy that although Levant et al. (2011) did not find that any of the masculinity constructs had any relationship, positive or negative, with the health-promoting behavior of following a good diet, the present study did, suggesting that we might be on the path to better understanding the variables that promote or hinder this important set of health behaviors.
Limitations
The current study is limited by the socioeconomic and cultural characteristics of our participants (predominantly young, White/European American, Christian, middle class, and unattached heterosexual men). Additional diverse samples should be studied to explore these relationships in other groups. Also, the self-report nature of the surveys introduces the possibility of bias due to socially desirable responding. A future study using a multimethod design (perhaps including the interviewing method) would strengthen evidence for the relationships found. In addition, the questionnaires were administered to all participants in the same order, possibly creating order effects. Future studies should counterbalance the order of presentation of the instruments to control for order effects. Furthermore, the present study recruited community participants from websites that catered to traditional masculine interests, possibly allowing bias to enter into the sampling. Future researchers may want to consider also recruiting from websites that cater to less traditional masculine interests to acquire a more representative sample. Moreover, the results are limited by several subscales of the HBI-20 having low alpha coefficients (<.70). Finally, given that we drew participants from two populations (college students and members of the community) it would have been prudent to compare these two populations on the study variables. If substantial differences were found then we might have created a variable reflecting group membership that could have been included as a covariate in the model. Unfortunately, we were unable to conduct this analysis because participants were asked to indicate how they were recruited on the incentive fulfillment page, which, because of the personally identifying information requested on this page, could not be connected to participants’ responses to the questionnaires.
Implications for Health Practitioners
These results have implications for assessing and counseling men on health-related matters. First, the HBI-20 may be of use to health care providers who wish to quickly assess their patients’ engagement in health promotion behaviors and avoidance of health risk behaviors.
Second, those aspects of masculinity that are related to health protective/health promotion behaviors could perhaps be strengthened through counseling interventions. This is a new area that has not yet been investigated, but could be in a future study. Among the findings that were replicated, the positive relationships between CMNI-Emotional Control Scale and Avoidance of Anger and Stress, and between CMNI-Winning Scale and the Avoidance of Substance Use suggest that using anger management techniques to help patients avoid dwelling on anger and counseling patients to focus on defining and pursuing their goals might be helpful tools to promote positive health behaviors. Some evidence for the effectiveness of anger management interventions was provided by Deffenbacher, Oetting, and DiGiuseppe (2002). Third, in regard to those aspects of masculinity that are related to health risk behaviors, interventions aimed at modifying them might be helpful in reducing risk behaviors. Among the findings that were replicated, this was seen in the relationships between the MRNI-R Total Scale and the Avoidance of Anger and Stress, the CMNI-Playboy Scale and Avoidance of Substance Use, and the CMNI-Risk-Taking scale and PSC. Thus, it may be helpful to counsel patients to take a critical perspective on the traditional masculine norms, perhaps using techniques developed for a group counseling program (Richmond & Levant, 2003), and to not engage in nonrelational sexuality (Levant, 1997), nor take needless risks.
Footnotes
Acknowledgements
We want to acknowledge the assistance of Alyson Szlamas of Kent State University.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.