
Abstract
The image of male nurses is closely related to the development of a female-driven nursing occupation. As a minority group in the nursing industry, male nursing students may have a negative self-image in their learning and clinical practicum. This may affect their psychological health and mental status. This study explored the positive and negative self-image of male nursing students. Eighteen participants were recruited from a local nurse-training institute. The participants were undergraduate bachelor’s and master’s students of nursing. The experience and opinions of the participants were collected by multiple methods. The participants’ drawings and audio diaries representing their self-image as nurses were collected in advance of a discussion of ideas raised in the focus group interview. The findings were categorized into three themes: (a) self-roles, functions, and identities; (b) awareness of gender differences; and (c) the future of professional development. The findings of this study provide information on the nurse role, identity, gender differences, and professional development of male nursing students, which will drive the direction of the development of a positive image for male nurses in the future.
The shortage of nurses has become a serious problem in many countries. In Hong Kong, nurses have excessive workloads in the clinical setting, putting them under enormous pressure. Up to the end of 2012, a total of 27,205 registered nurses (general) were female, but only 3,465 were male (The Nursing Council of Hong Kong, 2012). The problem of a shortage of nurses would be alleviated if more people went into nursing. Thus, the challenges faced by males who are preparing to join the profession are worthy of study. Here, we focus on the issue of self-perception.
Self-perception is defined as “a process whereby people observe their external behaviors or experience significant events so as to understand and evaluate themselves” (Bem, 1972; Hattie, 1992; Myers, 2009). During the process of self-perception, their attitudes, emotions, and inner thoughts may be altered, because when people encounter similar events again, they may handle them in different ways. Understanding the self-perceptions of newly graduated nurses or nursing students may help reveal their concerns about entering this female-dominated industry, which can affect the development of this industry in various ways.
The self-perception of male nursing students is different from the self-perception of female nursing students. Although male nurses enter into a nursing career voluntarily, and initially feel competent about performing nursing duties (Holroyd, Bond, & Chan, 2002; Loughrey, 2008; Meadus, 2000; Nilsson & Sätterlund Larsson, 2005; Price, 2009), some studies have found that male nurses feel embarrassed about providing intimate nursing care to female patients (Keogh & Gleeson, 2006; Lodge, Mallet, Blake, & Fryatt, 1997). When male nursing students are discriminated against and badly treated during their lessons and clinical placement, they feel inferior, isolated, or angry (Shen-Miller, Olson, & Boling, 2011). Such feelings adversely affect their perceptions of themselves, their work performance, and future career plans (Shen-Miller et al., 2011; Wyatt & Harrison, 2010). Promoting nursing education responding to the needs of male students could boost the image that they have of themselves (Bolan & Grainger, 2009; Sasat et al., 2002), making it more likely that they will develop a career in nursing.
According to the above-mentioned studies, the self-perception of male nurses has an effect on their feelings, performance, and future plans. This may in turn affect their psychological health and mental status. However, the perspectives of male nursing students on their self-image, whether positive or negative, have yet to be explored. This study examined the images of male nurses and undergraduate male nursing students, to shed light on the future development of a positive image for male nurses.
Method
This study was part of a larger research endeavor of a master research project about male nursing students’ self-perception and their relationships with female patients. A qualitative research design was adopted in our study, which focused on revealing multiple truths about a phenomenon (Holloway & Wheeler, 2010). Our research aimed to explore the experiences and feelings of male students, which are unique to each individual. Ethical approval was granted by the research ethics committee of a local university.
The narrative approach was chosen because it uncovers the hidden story of marginalized people in society (Dyson & Norrie, 2010); and male nurses are a minority group in nursing and the stories of male nursing students have yet to be told. The approaches of drawing and autobiography were keys to encouraging the participants to review their learning and practicum experience, especially with regard to sensitive topics (Guenette & Marshall, 2009; Hesse-Biber & Leavy, 2011; Staude, 2005). This approach does not rely on a list of structured questions and, consequently, offers great flexibility in data collection and more freedom for the participants.
Recruitment of Participants
A snowball sampling method was employed to select current full-time male students studying for their bachelor’s or master’s degree in nursing in a local university. Eighteen participants aged 22 to 31 years were interviewed in two focus groups, divided according to their programs (see Table 1). To facilitate method triangulation, the students were recruited for the drawing section before the focus group interview was held. In addition, after the focus group interview, eight master’s students voluntarily participated in the autobiographical research.
Demographic Data of the Participants.
Drawings and Focus Group Interviews
Before the interview, the participants were asked to sketch their own image. They were instructed to draw an image of themselves in a clinical setting inside a boxed area of a sheet of A4-sized paper, with the box taking up about half of the sheet. Afterwards, in the focus group interview, they described the meaning of the sketch. The focus group interviews lasted 1.5 to 2 hours. Two researchers moderated the group interaction, while the remaining three researchers acted as facilitators. The data from the bachelor’s students were collected in a discussion room in a university, while the data from the master’s students were collected in a private hospital. The data collection process was implemented during the end of the clinical practice, to ensure that the students had enough time to reflect on their experiences.
Audio Diary
After the interview, all the participants were invited to take part in the audio diary research. Participation was voluntary, and only eight master’s students consented to participate. These participants were welcome to share any related ideas in the diary. Significant events during their clinical placement were recorded. The collecting of the audio diaries took 6 months during the clinical practicum. Participants were encouraged to produce at least one recording per week.
Data Analysis
Three types of data were collected: drawings, recordings of focus group interviews, and audio diaries. The approach to analyzing the drawings was adopted from Guillemin (2004), who provided a systematic description of applying drawing in research on adults. To avoid bias in the interpretation of the drawings, the description of each drawing was extracted from the dialog of the participant who drew it. The drawings and descriptions provided by the participants were analyzed together.
A modified content analysis approach by Chenail (2012a, 2012b) was adopted to analyze the transcript. This approach guided the researchers to adjust the focus of the analysis from a line-by-line examination of the text to the metaphorical expression of entire meaningful entities. Thorough data immersion was performed during and after the transcription process via repetitive listening and reading. Descriptive coding was performed for meaningful units.
Peer checking was conducted among the research team. Discrepancies and missed information were discussed in meetings, and a consensus was reached when three out of four researchers agreed with a point. In addition, member checking was achieved by returning the focus group interview and audio transcripts to two participants to verify the correctness of the interpretation. One of the main goals of the focus group interview was to conduct member checking on the interpretation of the drawings.
Short summaries were made of each participant’s audio diaries. The summaries describe the actual events entered in the diaries, the emotions of the participants, and the ideas they shared. Content analysis was performed for all summaries using the same method as that described above.
Results
The findings were categorized into three major themes: (a) self-roles, functions, and identities; (b) awareness of gender differences; and (c) the future of professional development. Each participant whose is responsible for a quote used in this article is identified by his nursing program (i.e., bachelor’s degree, B, or master’s degree, M).
Theme 1: Self-Roles, Functions, and Identities
This theme highlighted how our participants regarded themselves as nurses. Three subthemes were included under this theme: (a) confusion about nursing roles and identities, (b) self-deprecation, and (c) instrumentalization. The first subtheme “confusion about nursing roles and identities,” describes how participants were confused about their identities and roles as nurses.
Actually, anyone can do these things: I can do them, an HCA can do them too, so why . . . I mean they don’t make you feel like you are a nurse. (M2)
The above narrative might describe the common concerns of both female and male students. However, the popular view of a nurse is of someone who is female, and this may cause male nursing students to construct a different image of themselves from that of the female students. Some participants shared the belief that the image of nurses as female was common among patients and other health care staff and that a clear image for male nurses was still lacking (see Figure 1).
In the end, there were some procedures for which he really wanted . . . someone wearing a cap and dress to come in to help him. (M7) I mean there are no signs that . . . err . . . identify us as nurses. (M2)
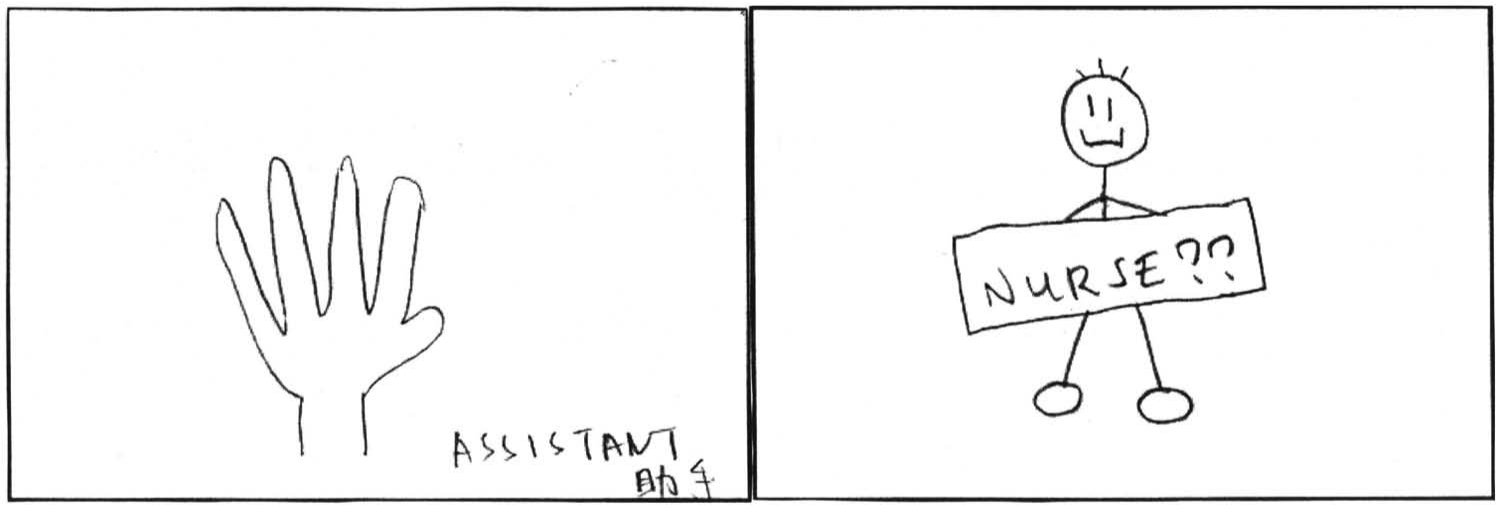
Drawings of M3 (left) and M2 (right).
Fulfilling the roles of a nurse could develop the students’ identity as nurses. Not being ignored in a ward is important for students, both male and female. The students focused their efforts on developing their nursing skills and gaining clinical experience.
After going through the A&E, I felt better because I had gained more experience and learned more, which helped to build my confidence. (M9, Audio Diary 2) Male nurses in public hospitals can do better, as they have more duties than the female nurses. They will thus have a better self-image because they feel more useful there. (M3, Audio Diary 2)
The second subtheme, “self-deprecation,” is about a sense of inferiority. The participants believed that male nurses were less competent than female nurses, especially when taking care of female patients. This supports the argument that male nursing students may have a different self-image from that of female students (see Figure 2).
There is a female nurse—actually she represents a female-dominated profession. This is me, kneeling down, representing pettiness and smallness. This profession is just like this drawing, it is female-dominated . . . and they rule, so males are really small. (B6)

Drawings of M7 (left) and B6 (right).
Regardless of their gender, the student nurses have limited experience and skills. As a result, they develop a sense of self-deprecation in clinical settings.
Yes, my drawing can be interpreted in two dimensions, as the stars in the sky, and as sand on the ground. Actually I feel just like a grain of sand, even less than a grain of sand. In the ward setting, everybody is busy; I feel like a grain of sand, and my status is very low. (B8)
Having autonomy as a nurse is believed to be important for the development of a positive self-image among male nursing students. The participants believed that having autonomy means being trusted by the hospital (see Figure 3).
Administering medication is one way to express myself . . . that is, gaining control of something. I mean, I can do my job and maintain my autonomy. (M8, Focus Group Interview 2) I am more significant in a public hospital, and [the hospital] gives me a lot of autonomy. For example, once they assign me a task, they count on me to do it. If I have any questions, they don’t make an ugly face at me. (M1, Audio Diary 1)

Drawings of B8 (left) and M8 (right).
The third subtheme, “instrumentalization,” is defined as treating people as a tool for carrying out certain tasks, and the focus is on the performance of the people rather than on their feelings. Several participants described themselves as medical instruments, such as a trolley or a stethoscope. This finding showed their unique self-image as male nursing students (see Figure 4).
I have gone through several placements. . . . There is always an idea in the mentor’s mind that males should do manual labor. There are no strict guidelines forcing you to do so, but they expect you to do it. (B7)

Drawings of M4 (left), M5 (middle), B7 (right).
For some participants, the extra tasks assigned to them increased their workload and hindered them in the performance of their personal duties. However, the majority of the participants did not oppose doing more manual labor.
Theme 2: Awareness of Gender Differences
The theme of awareness of gender differences signified the attention that they paid to the difference in their gender. Their constant comparisons of their own capabilities with those of their female colleagues magnified the gender differences between themselves and their female patients. This theme can be broken down into two subthemes: (a) inherited gender characteristics and (b) gender differences and patient caring. Regarding inherent gender characteristics, the idea that female nurses have better communication skills than male nurses was suggested.
They share the same objectives in caring but reach them in dissimilar ways . . . their voice characteristics are not alike. Females have softer voices . . . which may be more comforting . . . whereas male voices are deeper. . . . In terms of voice, females are better at providing psychological comfort, but males may be better at problem solving. (B4)
There was much discussion of the sense of circumspection exercised by male and female nurses. According to most participants, female nurses as a whole demonstrate more circumspection than male nurses. Some even suggested that a greater sense of circumspection was the instinctive talent of females:
I consider girls to be more sensitive, which means they can sense the needs of patients. . . . I think it is inherent and has nothing to do with their experience. (M5)
Regarding gender differences and patient caring, the participants recognized that male patients would prefer to be cared for by nurses of the same gender. Shared biological characteristics were reported to be a source of mutual understanding between male nurses and male patients (see Figure 5).
I think male nurses are better than female nurses at taking care of old men. . . . There is a better sense of mutuality and understanding. Male patients do not talk very much at times. If you are male too, you understand their needs and do not ask them detailed private questions. . . . From my observation in the ward, I perceive a better understanding between male nurses and male patients. Female nurses would experience communication barriers when caring for males. (B4) To cite Foley catheter insertion as an instance . . . if you ask a female nurse to perform this procedure for a male patient . . . when she inserts it . . . she may not perceive his feelings. But male nurses have a better understanding of what male patients want and feel. (B5)

Drawing of B4.
Talk of caring for patients often led to a discussion about performing nursing procedures on female patients with or without a chaperone. Some participants were “highly alert” to the gender difference between themselves and female patients and voiced their concerns about putting themselves under suspicion if caring for female patients alone:
I would worry about being under suspicion of sexual harassment. . . . It is for self-protection. . . . If someone intends to defame you . . . you should avoid getting into scrapes. . . . Why put yourself at risk? (B4)
Some participants were confident about their nursing knowledge and techniques, claiming to deliver the same quality of care to patients as female nurses do, whereas others emphasized their concern about the limited opportunities that they had to refine their nursing skills due to the barrier of approaching patients of the opposite gender.
Male nurses in Hong Kong are not allowed to provide female patients with many types of nursing care. Male nurses can only perform half of the duties that females are permitted to perform. . . . For instance, you should definitely not perform swabbing for females. . . . When you provide limited nursing care, then less communication occurs between you and your female patient, which in turn results in a limited therapeutic function from the physical or psychological aspect. (M7)
There was a belief among male nursing students that male nurses are inferior to female nurses. Male students expect female patients to not welcome male nurses, and that male nurses will be restricted to caring for male patients.
For example, when the patient is transferred back from the operating theater (OT) to our ward, we need to transfer the patient to another bed. However, if the patient is female, I have to leave, because we have to avoid [accusations of sexual harassment] and I can’t help her even if there are female nurses present. Perhaps the nurses want to avoid prosecution for inappropriate behavior and protect the privacy of the female patient. (M6, Audio Diary 1)
The gender differences were magnified by the external influences from society. The male participants kept their distance from female patients and their learning opportunities were limited because of their gender.
Theme 3: Future Professional Development
This theme illustrated the perceived career development of male nurses. Male nursing students are at the stage of learning. Therefore, what they perceive is closely related to their experience of their clinical education. This theme is covered by two subthemes: (a) career development and (b) clinical education.
Almost all the participants were unclear about the development of their career path. Female nurses can serve both male and female patients without embarrassment, whereas male nurses are still not accepted by the general public. This phenomenon may cause male nursing students to construct a different self-image from that of female students (see Figure 6).
Hmm . . . I also have a similar point of view. I also find it reasonable for women to become nurses, but the general public finds it special and strange when males become nurses. I am frequently asked by people: “You are male. Why are you studying nursing?” People find it a little bit strange. (B2) There are roads in my drawing. The girls are all following the same path, all becoming nurses. I am the guy here, looking at the road signs and not knowing which way to go. I believe that the traditional girls, I mean the female nurses, have a single direction to follow and they know what to do, such as how to take care of the patients. However, as for me, I am confused about whether I should follow the girls or use my own knowledge to take care of the patients, but not following the same path. (B1)

Drawing of B1.
Several participants felt restricted in their professional path. They could only show their potential in a few departments, such as the operating theater.
They [male nurses] have a greater function in the OT. There is not much difference between male and female nurses there in terms of duties. Also, male nurses have an advantage in the OT in terms of technique and professional knowledge. They feel more competent in the OT than in the ward. (M10, Audio Diary 1)
Organizational barriers place many limitations on the practice of male nurses. It was noted that private hospitals are more conservative than public ones in terms of giving learning opportunities to students.
Sometimes, there are some staff, like the mentor and HCA, who will assign you some trivial tasks. I help them, but how much does it help me? I always have this question in my heart. (B8, Focus Group Interview 1) The tasks assigned to students are repetitive and boring, so there is nothing new to learn. As a nursing student, if we have this kind of training, of course we can do better in routine work and learn a lot about this aspect. However, I doubt that this kind of repetitive training without critical thinking, without clinical judgment is really good for our students. Should nurses train like this in the future? (M10, Audio Diary Self-Perception 3)
The participants had difficulties providing nursing service to patients in their clinical practicum. This was partly due to their limited skills and experience. The nursing staff also played a role, as they were responsible for enabling the students to provide care to their patients.
After you learn some procedures and you practice a few times in the lab, you think you’re good to go. But when you go to the real setting . . . for example, like wound dressing, maybe it’s a little bit more complicated, or you haven’t done it before, and you are not familiar with the material. (B8, Focus Group Interview 1) Public hospitals pay more attention to male nurses; we can do more for our patients and make them feel secure. (M10, Audio Diary 2)
Direct nursing care is believed to be very important for students’ learning, but trivial and repetitive duties without nurse autonomy are not. Hospital staff and policies can also affect the learning opportunities of male students and the construction of a self-image that differs from that of female students.
Discussion
The discussion of the self-image of male nursing students led to a debate about nursing image. Statements and drawings revealed male students to have both positive and negative feelings about themselves. Several participants, such as M2, M7, M9, B6, and B8, stated that they lacked a clear image of themselves as male nurses, or a reasonable status. However, M9, M1, and B4 felt an enhanced sense of significance and were satisfied with their problem-solving skills and understanding of male patients. A similar study carried out in mainland China revealed a generally negative self-image of male nursing students there (Wong et al., 2011). Our findings are unlike those of previous studies, which found that male nursing students in Hong Kong are more positive about themselves than those in the other studies (Shen-Miller et al., 2011; Wong et al., 2011). Many participants believed that they had become nurses based on their own decision, and they did not regret it. They generally accepted themselves as nurses, but had difficulties in developing a positive identity from caring for other people and facilitating the recovery of patients (such as M7 and M2). The lack of a positive image of male nurses accounted for their lack of clarity about their roles and their confusion over their identity, which further aggravated their feelings of inferiority. However, not all participants blamed gender differences; the disadvantages of male nursing students were partly believed to be due to a lack of clinical experience, and some thought that their self-image would improve in the future.
The participants also reported that they were strongly aware of their gender. They constantly emphasized their differences from female colleagues. Females were believed to have inherited gender characteristics such as maternal instincts, which could give them an advantage when taking care of patients. Also, the participants stated that females are better at caring than males because they have more comforting voices and are more sensitive to people’s needs. When considering caring for male patients, male nursing students perceive they have a better rapport. For example, male patients do not feel embarrassed when they perform swabbing or dressing of the genital area. On the other hand, the male nursing students tried to keep their distance from female patients. The gender barrier faced by male nurses has been discussed in previous studies (Keogh & Gleeson, 2006; Lodge et al., 1997). A chaperone and a sense of humor could improve nurse–patient relationships (Milligan, 2001). Our study also explored the chaperone issue. The participants generally agreed that the policy of requiring a female chaperone helps improve nurse–patient relationships. However, the lack of manpower is a major issue, which frequently prevents the chaperone policy from being applied to male nurses.
According to the participating male nursing students, their career development will be more restricted than that of female students. In particular, male nurses have limited access to some traditionally female-dominated specialties, such as obstetrics and gynecology. Our findings also revealed the concerns that male nursing students have when taking care of female patients. Although the medical sciences are relatively advanced in Hong Kong, Hong Kong society is still greatly influenced by the traditional Chinese cultural norm that males should have limited contact with females. This concept prevented male nurses from taking care of female patients. If it is a cultural norm for male students not to look after female patients, then the issues of concern are that they will lack clinical practice and chances to develop the ability to provide intimate care. In Western countries, male nurses are offered more opportunities and autonomy to take care of female patients, whereas male nurses in Chinese cultures are greatly oppressed by traditional norms. Interestingly, female patients generally accept assessment and care from male doctors. The professionalism of physicians can account for this attitude, and male nursing students should be given a mandate to cross cultural barriers as male doctors have done. Moreover, students should be given the opportunities to engage in more multidisciplinary health learning at university and in practice. This would help the male nursing students to be seen as part of a team rather than marginalized and allow patients to see them more closely aligned to other professionals such as doctors. Therefore, the development of professionalism in nursing could lead to greater acceptance of male nurses by female patients.
The limitation of our study is that only one nurse training institute was selected to participate in this study. The small sample size affects the transferability of the findings to the whole region. In a future study, participants could be recruited from several institutions in Hong Kong. The study only focused on male student nurses, and staff nurses were not recruited. As a result, the findings do not reveal the differences in self-image, if any, between male registered nurses and male nursing students. A comparison of their self-images may more deeply reveal the influence of clinical practice on male nurses. A similar cross-sectional study on male nurses was performed in Taiwan, covering multiple groups of male nurses at different stages of their professional and career development (Yang, Gau, Shiau, Hu, & Shih, 2004). However, this study focused on the professional development of male nurses. In the future, a longitudinal study could be performed to investigate changes in self-image during the entire course of the nursing program, so as to understand the implications of the students’ images on their education. Comparative studies in the future should involve the opinions of patients and female nurses to offer an extra dimension for the researcher to understand the image of male nurses in nursing practice. These approaches will help in the effort to develop a positive role model of the male nurse.
To help male nursing students develop a positive self-image, the nursing education curriculum must give opportunities for students to construct a more positive self-image and to get a feeling for how a nurse makes a difference in patients’ lives. The students should get a more comprehensive experience of providing care for patients and not be restricted to certain wards. Nursing education curriculum should consider male nursing students self-images related to patients and clinical contexts.
Conclusions
The aim of this article was to explore the positive and negative self-images of male nursing students in Hong Kong. Our study applied a mixture of data collection methods, which yielded descriptions of the participants’ experiences and opinions. Our findings focused on the role and identity of nurses, gender differences, and the professional development of male nurses. Some participants had a negative self-identity, whereas the others were aware of their gender differences and found advantages in being a male nursing student in clinical settings. Nevertheless, organizational barriers may restrict male nursing students in their pursuit of their career goals. The findings of our study pave the way for the future development of a positive role model of the male nurse, through a nursing education program tailor-made for male students, so as to improve their self-image and thus their mental outlook on their future career.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.