
Abstract
Racial/ethnic differences in health are evident among men. Previous work suggests associations between mental and physical health but few studies have examined how mood/anxiety disorders and chronic physical health conditions covary by age, race, and ethnicity among men. Using data from 1,277 African American, 629 Caribbean Black, and 371 non-Hispanic White men from the National Survey of American Life, we examined associations between race/ethnicity and experiencing one or more chronic physical health conditions in logistic regression models stratified by age and 12-month mood/anxiety disorder status. Among men <45 years without mood/anxiety disorders, Caribbean Blacks had lower odds of chronic physical health conditions than Whites. Among men aged 45+ years with mood/anxiety disorders, African Americans had greater odds of chronic physical health conditions than Whites. Future studies should explore the underlying causes of such variation and how studying mental and chronic physical health problems together may help identify mechanisms that underlie racial disparities in life expectancy among men.
Research on variations in men’s health by race, ethnicity, and other social factors is limited (Young, Meryn, & Treadwell, 2008). Though racial disparities in health are substantial, persistent, and pervasive (Dressler, Oths, & Gravlee, 2005; Geiger, 2006; Griffith, Moy, Reischl, & Dayton, 2006; Griffith, Neighbors, & Johnson, 2009; Williams & Collins, 2004), these differences are exacerbated by gender (Griffith, Metzl, & Gunter, 2011; Xanthos, Treadwell, & Holden, 2010; Young, 2009). The primary focus of disparities research has been on chronic physical illnesses (Geiger, 2006; Geronimus & Thompson, 2004; Sankar et al., 2004), but mental illnesses can be just as debilitating (Hays, Wells, Sherbourne, Rogers, & Spritzer, 1995; Scott et al., 2009). In addition, evidence from both clinical (Berardi et al., 1999) and community samples (Kessler, Barker, et al., 2003; Kessler, Ormel, Demler, & Stang, 2003) suggest having either a sole physical or mental illness tends to be less debilitating than experiencing comorbid mental and physical illnesses. There is a growing need to address comorbid physical and mental illnesses, but research examining variability in the prevalence of comorbidities and how comorbidities vary by race and ethnicity among men remains limited. The purpose of this article is to examine the associations between race, ethnicity, and mental and physical illnesses among Black and White men in the United States.
Ethnic Variations in Health
Race is a sociopolitical categorical indicator that denotes a common social and political history; race captures differential access to power and resources based on arbitrary but distinctive physical characteristics and cultural criteria (LaVeist, 1996; Neighbors, Griffith, & Carty, 2008). Although aggregating ethnic groups into a single racial category of Black Americans allows for comparative analyses between racial groups (Griffith et al., 2006), examining ethnic heterogeneity among Black Americans facilitates investigation of the variation in social contexts among Black Americans, and their associations with health and disease independent of racial category (Arthur & Katkin, 2006; Bediako & Griffith, 2007; Williams, Haile, et al., 2007. More than 25 years ago, the U.S. Department of Health and Human Services Secretary’s Task Force Report on Black and Minority Health argued that the racial categories were too broad to accurately reflect the disease profiles and risk factor prevalence among subgroups of American Blacks (Nickens, 1986). Despite this call for further investigation into variation among racial groups, the implications of ethnic heterogeneity among Blacks in the United States have generally been neglected in health research (Arthur & Katkin, 2006).
Ethnic groups consist of people who have common cultural (and often similar physical) traits that distinguish them from other ethnic groups, including primary language, nativity, history, traditions, values, and dietary habits (C. L. Ford & Harawa, 2010; Smedley & Smedley, 2005). Ethnicity encompasses aspects of social life (culture) and personal identity that people within some socially defined group (choose to) share (C. L. Ford & Harawa, 2010). Ethnicity comprises two dimensions: an attributional dimension that highlights unique sociocultural characteristics (e.g., culture, diet) of groups and a relational dimension that captures characteristics of the relationship between an ethnically defined group and the society in which it is situated (C. L. Ford & Harawa, 2010). Within countries, ethnic groups are diverse subcultures maintaining certain patterns of behaviors, beliefs, and values that distinguish them from other cultural groups (Marger, 1997). The two largest ethnic groups of Black Americans are African Americans and Caribbean Blacks (e.g., Haitian, Jamaican, etc.; Schmedley, 2001). The vast majority of Black Americans include those born in or with ancestral roots linked to the United States, Canada, South America, the Caribbean, and Africa. For the purposes of this study, the term Black Americans refers to all people of African descent (including African Americans), whether they are originally from the United States or not (e.g., Jamaicans, Haitians, West Indians, etc.). The term African American is used to refer to respondents who self-identified as Black but did not identify ancestral ties to the Caribbean. Caribbean Blacks are respondents who self-identified as Black and indicated (a) that they were of West Indian or Caribbean descent, (b) that they were from a country included on a list of Caribbean countries presented by the interviewers, or (c) that their parents or grandparents were born in a Caribbean country.
The persistence of poor mental and physical health outcomes for men of color suggests within and between ethnic group variations may be important determinants of comorbid physical and mental illnesses among men of color. Evidence suggests that Caribbean Blacks (Nazroo, Jackson, Karlsen, & Torres, 2007), and particularly Caribbean Black men, have better self-rated health and longer life expectancies when compared with African Americans (Kaba, 2009). Other studies have found Caribbean Black men to have greater odds of hypertension than White Americans (Nazroo et al., 2007), and greater odds of any mood/anxiety disorders than African American men (Williams, Gonzalez, et al., 2007). These findings provide evidence of both ethnic and racial differences in mental and physical health.
Although old age is generally associated with poorer health in the United States, research on ethnic differences in poor health among older groups is limited. Research has demonstrated racial differences in chronic disease prevalence at younger ages; however, only one report has examined ethnic differences in chronic disease prevalence across age groups among Black Americans. This report found that self-reports of “fair” or “bad/poor” health were more frequent among African Americans (referred to as “Black Americans” in the report) compared with White American adults ages 55 years and older (Nazroo et al., 2007). Caribbean Blacks had the lowest prevalence of fair/bad/poor self-rated health at ages 45 to 54 years, which subsequently increased to levels consistent with the levels of Black Americans (African Americans) and White Americans (Nazroo et al., 2007). Consistent with the immigrant health paradox often articulated in reference to the health of Americans from Latin America, variations in health by time and generations that Caribbean Blacks have been in the United States suggest that there may be physiological consequences of assuming the American lifestyle (Griffith, Johnson, Zhang, Neighbors, & Jackson, 2011). Ethnic differences across age groups are apparent, as well as increased prevalence of chronic disease among these groups. This raises the question of whether the effect of cumulative long-term exposure of ethnic groups to cultural experiences in the United States negatively affects their health.
Social Determinants of Health for Black and White Men
In large, epidemiologic community surveys, the prevalence of depression symptoms is lower in Black men compared with both White men and Black women (Blazer, Kessler, McGonagle, & Swartz, 1994; B. C. Ford et al., 2007; Watkins, Walker, & Griffith, 2010). Across racial groups, women tend to have higher rates of diagnosed depression and anxiety disorders than men (Addis, 2008; Cochran & Rabinowitz, 2003; Kessler, Brown, & Broman, 1981; Oliffe & Phillips, 2008), but men have higher rates of diagnosed substance abuse, antisocial behavior, and suicide, suggesting that depression in Black and White men may be underdiagnosed (Addis, 2008; Cochran & Rabinowitz, 2003; Williams, 2003). Although Black men typically have a decreased prevalence of depressive and mood disorders compared with White men, and suicide rates among older White men are disproportionately higher compared with Black men (Centers for Disease Control and Prevention, 2012), the increased prevalence of depressive symptoms among Black men compared with White men (Skarupski et al., 2005) is consistent with racial patterns of poorer health among racial/ethnic minorities.
Previous reports that document social patterning of physical health suggest that Black Americans experience higher rates of mental illness than White Americans, including depression and anxiety, as a result of exposure to chronic stress (Mezuk et al., 2010). Community studies, however, have found that in comparison with White Americans, Black Americans have similar or lower rates of mood disorders, particularly major depression (Kessler, Barker, et al., 2003; Kessler, Ormel, et al., 2003). Analyses based on respondents aged 54 to 65 years from the Health and Retirement Survey have also reported lower rates of major depression among Blacks relative to Whites in adjusted models (Dunlop, Song, Lyons, Manheim, & Chang, 2003). The extent to which cultural variation is associated with health in epidemiologic community surveys is not well understood (Neighbors, Trierweiler, Ford, & Muroff, 2003). The lower prevalence of mental health disorders among Black compared with White Americans may appear counterintuitive (Mezuk et al., 2010), yet this finding has been consistently reported over the past two decades (Blazer et al., 1994; Riolo, Nguyen, Greden, & King, 2005; Somervell, Leaf, Weissman, Blazer, & Bruce, 1989; Compton, Conway, Stinson, & Grant, 2006), despite Black Americans’ social and economic disadvantage when compared with their White counterparts.
Jackson and colleagues have offered a testable, theory-driven model to disentangle the racial differences in mental and physical illnesses (Jackson & Knight, 2006). The goal of this model is to explain the rationale behind why Black Americans tend to have lower rates of mood/anxiety disorders and other psychiatric diagnoses than White Americans, and also why Black Americans tend to have higher rates of chronic physical health conditions than White Americans. Jackson and Knight (2006) propose that individuals experiencing significant stress engage in negative health behaviors (e.g., smoking or overeating) that provide short-term relief from the psychological and physiological experience of stress. Although these behaviors are “protective” of one’s mental health, their use to cope with chronic stress can lead to negative physical health consequences. Initial empirical tests have found support for this model (Jackson, Knight, & Rafferty, 2010; Mezuk et al., 2010), but none of these studies reported specific analyses by sex or examined ethnicity. These findings, however, highlight that more research is needed to explain patterns of comorbid mental health conditions and chronic physical health conditions.
In this study, we use a nationally representative sample to explore racial/ethnic differences in experiencing one or more chronic physical health conditions, by age and mood/anxiety disorder status among African American, Caribbean Black, and non-Hispanic White American men. We hypothesize the following:
Regardless of race or ethnicity, men with mood/anxiety disorders will be more likely to also experience chronic physical health conditions.
With or without a mood/ anxiety disorder, African American and Caribbean Black men will be more likely to have chronic physical health conditions than White men.
Among men with a mood/anxiety disorder, African American and Caribbean Black men will be more likely to have chronic physical health conditions than White men.
Among men younger than 45, Caribbean Black men will be less likely than White and African American men to have a chronic physical health condition.
Among men 45 and older, Caribbean Black men and African American men will be more likely than White men to have a chronic physical health condition.
Method
Participants
All men from the National Survey of American Life (NSAL), which was conducted between February 2, 2001, and June 30, 2003, were eligible for inclusion in these analyses (Jackson, Neighbors, Nesse, Trierweiler, & Torres, 2004). The majority of interviews (86%) were completed face-to-face using a computer-assisted instrument and lasted an average of 2 hours and 20 minutes. The remaining interviews were either partially or entirely conducted by telephone. The adult sample (aged 18+) of the NSAL was a national household probability sample of 6,082 persons, of which 5,191 were Black Americans (which may have included Hispanic Blacks) or Blacks of Caribbean descent and 891 were non-Hispanic Whites. The Black American sample was drawn to be nationally representative of the 48 contiguous states with at least one Black adult 18 years of age or older. The sample of non-Hispanic Whites, representing 14% of the Whites population of the United States, was a stratified, disproportionate sample of White American adults from households selected from census tracts and blocks with a Black American population of 10% or more. The response rates for the survey were 72.3% overall, 70.7% for African Americans, 77.7% for Caribbean Blacks, and 69.7% for non-Hispanic Whites. The NSAL included 2,286 men, of which 2,277 self-reported their main race as Black or non-Hispanic White. A total of 629 of the 2,277 men were Blacks of Caribbean or West Indian descent; 1,277 reported being Black and not of Caribbean or West Indian descent; and 371 reported being White (four of which were of Caribbean or West Indian descent).
Measures
Sociodemographic Factors
Age was measured in years, and marital status was categorized as married or not married. Education was categorized as <11 or 12+ years. Household income was measured in U.S. dollars and adjusted for household size by dividing the household income by the square root of household size (Figini, 2000). Respondents reported their race as either White or Black, but were also asked whether they were of Caribbean or West Indian descent.
Psychiatric Disorders
Twelve-month mood and anxiety psychiatric disorders were assessed using the World Health Organizations Composite International Diagnostic Instrument (Jackson et al., 2004; Kessler, Berglund, et al., 2003). Of the six anxiety disorders (panic disorder, agoraphobia disorder without panic disorder, social phobia, generalized anxiety disorder, obsessive compulsive disorder, and posttraumatic stress disorder) and the three mood disorders (major depressive disorder, dysthymia, and bipolar disorder) assessed in the NSAL, only a subset of these disorders was assessed in the White respondents. As a result, the 12-month assessments available for the analytic sample included four anxiety disorders (panic disorder, agoraphobia disorder [without panic disorder], social phobia, and generalized anxiety disorder) and three mood disorders (major depressive disorder, dysthymia, and any bipolar disorder). Individuals deemed to have any (one or more) of these seven disorders were categorized as having a mood/anxiety disorder.
Chronic Physical Health Conditions
The presence of one or more (1+) chronic physical health conditions was determined by a “yes” response to the question that asked if respondents had a blood circulation problem or “hardening of the arteries,” heart trouble or heart attack, hypertension or “high blood pressure,” diabetes or “sugar,” a kidney problem or “kidney trouble,” stroke, cancer, asthma, chronic bronchitis, or emphysema. The chronic physical health conditions included in these analyses were selected for consistency with previous literature (Freid, Bernstein, & Bush, 2012).
Data Analysis
Survey weighted F tests and Rao–Scott chi-square tests were used to evaluate differences in demographic variables by race and ethnicity. Logistic regression models for complex survey data were run using SAS software, Version 9.2 of the SAS system for Windows (Copyright2004. SAS Institute Inc. SAS and all other SAS Institute Inc. product or service names are registered trademarks or trademarks of SAS Institute Inc., Cary, NC). Model fit was evaluated based on the Akaike information criterion, with smaller values indicative of improved model fit. Stratified models of the associations between race/ethnicity and 1+ chronic physical health conditions were performed by age (<45 years vs. 45+ years) and mood/anxiety disorder status. Interaction effects of race and mood/anxiety disorder status within age strata were tested to maximize statistical power and were reported in log-odds ratios to avoid misinterpretation of the interaction effects (Ai, Norton, & Wang, 2004). Four strata were examined: <45 years without mood/anxiety disorders, 45+ years without mood/anxiety disorders, <45 years with mood/anxiety disorders, and 45+ years with mood/anxiety disorders. In light of previous studies highlighting the influence of socioeconomic status on men’s health (Hudson et al., 2011), models were adjusted for tertiles of household income. Weights accounting for disproportionate sampling, nonresponse, and population representation across various sociodemographic characteristics were applied (Heeringa et al., 2004).
Results
Sample Characteristics
Sample characteristics are shown in Table 1. Differences in the age distribution were detected (p < .01), suggesting a greater proportion of White men were aged 45+ years (49.4%), whereas larger proportions of Caribbean Black and African American men were aged 18 to 24 years compared with White men. A greater proportion of Caribbean Black men were married (p < .01), and the distributions of income were also varied across racial/ethnic groups (p < .01). No significant differences in the proportions of the sample with mood/anxiety disorders or chronic physical health conditions were suggested.
Sample Characteristics of the Caribbean Black, African American, and White Men From the NSAL.

Note. NSAL = National Survey of American Life.
Logistic Regression Model Results
In Table 2, the preliminary logistic regression model that included age, race/ethnicity, mood/anxiety disorder status, and household income suggested men younger than 45 years of age (odds ratio [OR] = 0.25, 95% confidence interval [CI] = 0.18-0.36) were less likely than men ages 45 years and older to have 1+ chronic physical health conditions. Individuals with mood/anxiety disorders had greater odds of 1+ chronic physical health conditions than those who did not have a mood/anxiety disorder (OR = 2.09, 95% CI = 1.21-3.61). There were no significant associations between race/ethnicity and chronic physical health conditions.
Baseline Logistic Regression Model (N = 2,277).
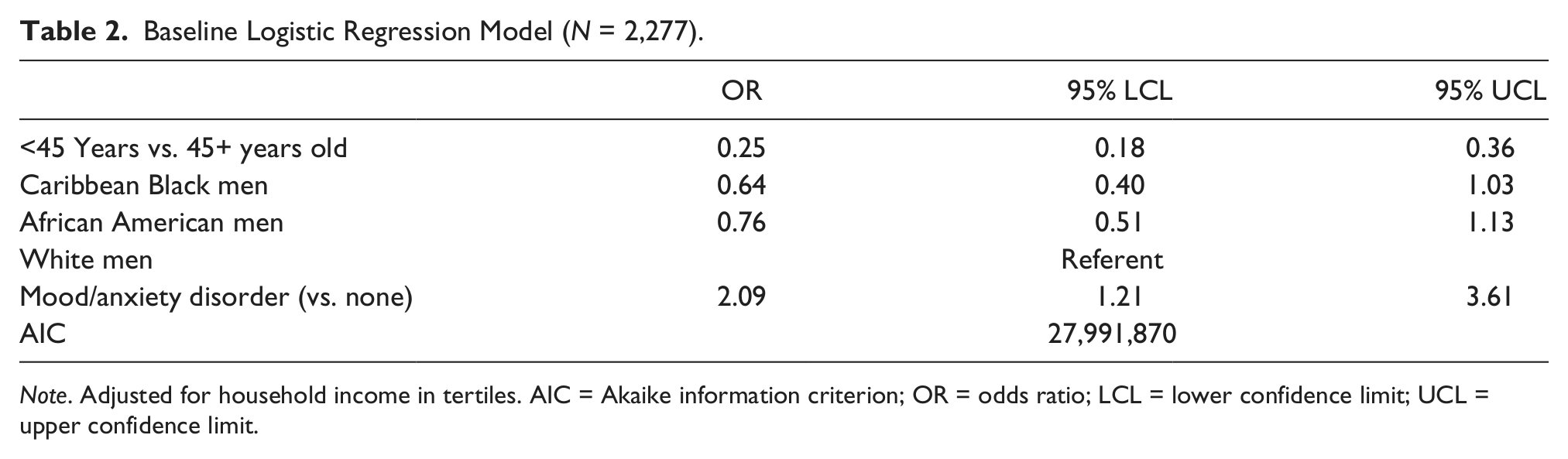
Note. Adjusted for household income in tertiles. AIC = Akaike information criterion; OR = odds ratio; LCL = lower confidence limit; UCL = upper confidence limit.
In Table 3, we show age-stratified models (<45 years, 45+ years) examining associations with having 1+ chronic physical health conditions. We found a marginally significant positive interaction term for Caribbean Black men <45 years of age without mood/anxiety disorders when compared with White men (log OR = 1.29, standard error (SE) = 0.69, p = .06), but there was no significant association for African American men <45 years of age compared with White men <45 years of age (log OR = 0.06, SE = 0.62, p = .92). In contrast, for men aged 45+ years, African American men with mood/anxiety disorders were less likely to have 1+ chronic physical health conditions than White men (log OR = −2.25, SE = 0.97, p = .02), but no significant interaction was suggested for Caribbean Black men (log OR = −0.36, SE = 1.27, p = .77).
Age Stratified Logistic Regression Models of 1+ Chronic Physical Health Conditions (N = 2,277).

Note. Adjusted for household income in tertiles. AIC = Akaike information criterion; OR = odds ratio; SE = standard error.
Logistic regression models stratified both by age and mood/anxiety disorder status (Table 4) were performed to directly assess associations of race/ethnicity and 1+ chronic physical health conditions across age and mental health status that were suggested in Table 3. Consistent with results from Table 3, the analyses suggested that Caribbean Black men <45 years of age without mood/anxiety disorders had lower odds of 1+ chronic physical health conditions than White men <45 years of age (OR = 0.49, 95% CI = 0.26-0.91), and African American men <45 years of age with mood/anxiety disorders had greater odds of 1+ chronic physical health conditions than White men in the same age group (OR = 0.08, 95% CI = 0.01-0.48).
Logistic Regression Models of 1+ Chronic Physical Health Conditions Stratified by Age and Mood/Anxiety Disorder Status (N = 2,277).

Note. Adjusted for household income in tertiles. AIC = Akaike information criterion; OR = odds ratio; LCL = lower confidence limit; UCL = upper confidence limit.
Discussion
This study sought to explore racial and ethnic differences in experiencing one or more chronic physical health conditions by age and mood/anxiety disorder status among non-Hispanic White men, African American men, and Caribbean Black men. Our findings supported our first hypothesis that men with mood/anxiety disorders would be more likely to also experience chronic physical health conditions. We did not, however, find statistical evidence to support our second hypothesis, which proposed that African Americans and Caribbean Blacks would be more likely than Whites to have chronic physical health conditions. Findings did identify trends in the odds of chronic physical health conditions for Caribbean Black and African American men compared with White men; the magnitude of associations (including nonsignificant associations) suggested Caribbean Black men had lower odds of chronic physical health conditions than African American men in comparison with White men. African American men and Caribbean Black men with mood/anxiety disorders, however, were more likely to have chronic physical health conditions than White men.
Our fourth and fifth hypotheses sought to examine the additional role of age in the relationships between race, ethnicity, and mood/anxiety disorder status in relation to chronic physical health conditions. We found that among men younger than 45 years of age without mood/anxiety disorders, Caribbean Black men were less likely to report 1+ chronic physical health conditions than White men, but there was no statistical difference in the odds of Caribbean Black and White men reporting 1+ chronic physical health conditions. In contrast, among men 45 years of age and older with mood/anxiety disorders, African American men were more likely to report 1+ chronic conditions than White men, but there was no statistical difference in the odds of Caribbean Black and White men reporting 1+ chronic physical health conditions.
The majority of previous studies that have examined ethnic differences in health outcomes among Black Americans have either examined physical health (Nazroo et al., 2007) or mental health (Williams, Gonzalez, et al., 2007; Williams, Haile, et al., 2007) independently. Of the studies that have examined ethnic differences in physical outcomes, few have assessed the role of mental health conditions. Griffith, Johnson, et al. (2011) assessed ethnic and nativity differences in self-rated health and chronic physical health conditions among Black Americans from the National Survey of American Life, and found that foreign-born Caribbean Blacks had lower odds of both self-rated health and chronic physical health conditions (which included more chronic physical health conditions than those included in our analyses) than U.S.-born Caribbean Blacks or African Americans, but they did not find any gender differences. The authors also found that Blacks with depressive symptoms determined by the Center for Epidemiologic Studies–Depression scale (CES-D) were more likely to have chronic physical health conditions than Blacks without depressive symptoms. Other studies of ethnic differences in physical health among men have found higher odds of hypertension among African Americans and Caribbean Blacks compared with White Americans, although only African Americans had increased odds of cardiovascular disease/diabetes compared with White Americans (Nazroo et al., 2007).
Although virtually no studies have examined the multiple roles of age, race, ethnicity, and mood/anxiety disorder status on chronic physical health conditions, Nazroo et al. (2007) reported the findings of analyses that assessed age and race–ethnic differences in physical health. Nazroo et al. (2007) reported increasing trends in self-reports of fair/poor self-rated health for Caribbean Black and African Americans from age 55+ years, and further found Caribbean Blacks aged 45 to 54 years had lower odds of self-reporting fair/poor health than at older ages and compared with African Americans or White Americans (Nazroo et al., 2007). Other studies have reported positive associations of age (measured continuously) with chronic physical health conditions across racial (Black and White) samples, finding similar associations across racial groups (Jackson et al., 2010). The variability in the odds of 1+ chronic physical health conditions in our findings across racial/ethnic groups, mood/anxiety disorder status, and age categories indicate the importance of understanding the intersection of multiple demographic factors and mental illness in relation to physical health outcomes.
From a research perspective, James Jackson’s Affordances Model (Jackson & Knight, 2006; Jackson et al., 2010), which seeks to explain the complex patterning of comorbid mental and physical health disorders by race, could be used to uncover positive coping mechanisms employed by Black and White men faced with chronic stressors. Identifying healthy behavioral strategies for men to use to cope with stress is critical because unhealthy coping behaviors, although they may protect against mental illness, often result in chronic physical health conditions such as those included in these analyses. From a practice perspective, the design, implementation, and evaluation of behavioral interventions that acknowledge unhealthy coping behaviors and work toward developing healthier behaviors will be important next steps to protect mental health while maintaining good physical health. Unique culturally grounded, gender-sensitive coping styles such as Majors’s Cool Pose (Majors, 1993) and Anderson’s Code of the Street (Anderson, 2000) have been identified as ways of deflecting negative images and coping with stress, and should be considered as coping styles that can be adapted to address cultural differences across racial and ethnic groups in future research and practice.
Limitations
Despite the contribution this study makes to the body of science on comorbid physical and mental health conditions among men, our findings should be interpreted in light of a few limitations. First, our low prevalence of mood/anxiety disorders in the sample, and particularly when further stratified by age, limited our ability to examine additional covariates that may be relevant in our analyses, including social factors such as those above. Furthermore, our limited number of respondents with mood/anxiety disorders across categorizations of race, ethnicity, and age also limits the precision of our estimates in the analyses, as evidenced by the large confidence intervals around the estimates. Another potential limitation is with regard to the self-report status of the chronic conditions. Conditions such as hypertension (Newell, Girgis, Snason-Fisher, & Savolainen, 1999) and diabetes (National Diabetes Data Group, 1995) are commonly underreported, particularly among racial/ethnic minority populations. It is most likely that respondents underreported the presence of chronic conditions, which would result in an underestimation of the associations presented in the analyses. Other limitations of the study include the cross-sectional study design, which limits any our ability to draw causal inferences from the analyses. Beyond these limitations, our approach allowed for an exploration of differences in chronic physical health conditions at the intersection of race/ethnicity, age, and mental health status, and specifically among men. Our work demonstrates the need for exploration in future studies on comorbid physical and mental health conditions among men.
Conclusion
Our study is a unique contribution to the body of research on the physical and mental health of men, because it is one of few to assess racial and ethnic differences in the prevalence of physical health conditions by mental health status across men of different age groups. Our study found that younger Caribbean Black men without mental health conditions had better physical health than younger White men without mental health conditions, but older African American men with mental health conditions had poorer physical health than older White men with mental health conditions. Our work indicates the importance of addressing the intersection of mental and physical health over the life course as we aim to understand racial/ethnic differences in health among men, and particularly among Black American men. Our study illustrates that the intersection of race and ethnicity yields a different picture than either factor alone (Read & Gorman, 2006; Warner & Brown, 2011). Future work should continue to simultaneously address mental and physical health and incorporate the role of other social factors as potential determinants of racial/ethnic differences in these outcomes. The challenge of reconciling Black men’s “better” mental health yet poorer physical health than White men highlights the critical role of stress and stressors in both mental and physical health and the opportunities for understanding the causal pathways that link social and environmental determinants of health to health disparities (Geronimus & Thompson, 2004; Jackson & Knight, 2006; Massey, 2004; Williams, Neighbors, & Jackson, 2003).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.