
Abstract
Objective
The manifestations of sarcoidosis differ by ethnicity and region. However, the few studies that have focused on elderly sarcoidosis are only from Western countries. Therefore, we investigated elderly sarcoidosis in Japan.
Methods
We retrospectively reviewed the records of adult patients (≥18 years old) who were diagnosed with sarcoidosis from 1 April 2006 to 31 March 2020. The diagnosis was pathologically confirmed in all patients. We compared the clinical features of elderly (diagnosed at ≥65 years old) and non-elderly (diagnosed at <65 years old) patients.
Results
Thirty-five (33%) of 106 patients were elderly. The elderly group had significantly more comorbidities than the non-elderly group (median [range], 1 [0–4] vs. 0 [0–5]). The biopsy site at diagnosis included significantly more extrathoracic sites in the elderly than non-elderly group (57.1% vs. 33.8%). The elderly group had significantly more muscle lesions than the non-elderly group at the time of diagnosis (11.4% vs. 1.4%) and at any time during follow-up (17.1% vs. 1.4%).
Conclusion
In Japan, elderly patients with sarcoidosis might have more muscle involvement and comorbidities than younger patients. Because comorbidities might affect the prognosis of elderly sarcoidosis, further study is needed to clarify the effect of comorbidities on elderly sarcoidosis.
Introduction
Sarcoidosis is a systemic disease of unknown origin that is characterized by granuloma formation. With the aging global population, there is an increasing need to research elderly sarcoidosis. In fact, although age at the diagnosis of sarcoidosis is increasing globally, including in Japan,1,2 only a few previous studies have focused on elderly sarcoidosis.3–6 Elderly patients with sarcoidosis reportedly have more comorbidities and certain extrapulmonary manifestations, including subcutaneous nodules and intra-abdominal/retroperitoneal lymph node involvement. However, these reports were only from Western countries even though the manifestations of sarcoidosis differ according to ethnicity and region.7–11 For example, a higher frequency of ocular involvement, extrathoracic lymph node involvement, hypercalcemia, and cardiac involvement exists in Asian cohorts than in other ethnic groups. 10 Therefore, it is necessary to investigate elderly sarcoidosis in other regions, including Asia. The aim of this study was to reveal the clinical features of elderly sarcoidosis in Japan.
Patients and Methods
This was a retrospective observational study. We retrospectively reviewed the electronic medical records of consecutive adult patients (≥18 years old) who were diagnosed with sarcoidosis from 1 April 2006 to 31 March 2020 at Yokohama City University Hospital. The diagnosis of sarcoidosis was based on the joint statement proposed by the American Thoracic Society, the European Respiratory Society, and the World Association of Sarcoidosis and Other Granulomatous Disorders (WASOG). 12 The diagnosis was pathologically confirmed in all the patients. Organ involvement was defined by the WASOG Sarcoidosis Organ Assessment Instrument. 13 Non-Japanese patients were excluded from this study. Muscle involvement was divided into three patterns: chronic myopathy, acute myopathy, and nodular myopathy. 14 We handled these patterns as muscle involvement.
Next, we compared the clinical features of elderly patients (diagnosed at ≥65 years of age) and non-elderly patients (diagnosed at <65 years of age). The cut-off age of 65 years for inclusion in the elderly group was chosen based on previous studies.3–5 The proportion of elderly patients was analyzed by dividing the diagnosis period every 5 years.
Data are presented as median (range) unless otherwise specified. JMP Pro 16 software (SAS Institute, Cary, NC, USA) was used for the statistical analyses. Continuous variables were compared using the Mann–Whitney U test, and categorical variables were compared using Fisher’s exact test. The Cochran–Armitage test for trend was used to determine whether the proportion of elderly sarcoidosis was increasing. Statistical significance was set at a p value of <0.05, and all tests were two-tailed.
This study was approved by the institutional review board of Yokohama City University Hospital (No. 200600007). The need for written informed consent from the patients was waived because of the retrospective nature of the study. We de-identified all patient details. The reporting of this study followed the STROBE guideline. 15
Results
One hundred seven patients had pathologically confirmed sarcoidosis, among whom one patient was excluded because of Caucasian ethnicity. Thus, data from 106 patients were analyzed (Figure 1). Thirty-five of the 106 patients were ≥65 years old (elderly group) (Figure 1).

Flowchart of patient inclusion.
Table 1 shows the clinical features of the patients. The elderly group had significantly more comorbidities than the non-elderly group (1 [0–4] vs. 0 [0–5], p = 0.001). The biopsy site at diagnosis differed significantly between the elderly and non-elderly groups. Significantly more extrathoracic sites (e.g., cutaneous and muscle lesions) were biopsied in the elderly group than in the non-elderly group (57.1% vs. 33.8%, p = 0.04). The follow-up period was 4.4 [0.04–12] years in the elderly group and 4.9 [0.03–14] years in the non-elderly group. Table 2 shows the details of the biopsy site. Lung biopsy was less frequent in the elderly than non-elderly group.
Comparison of clinical features.
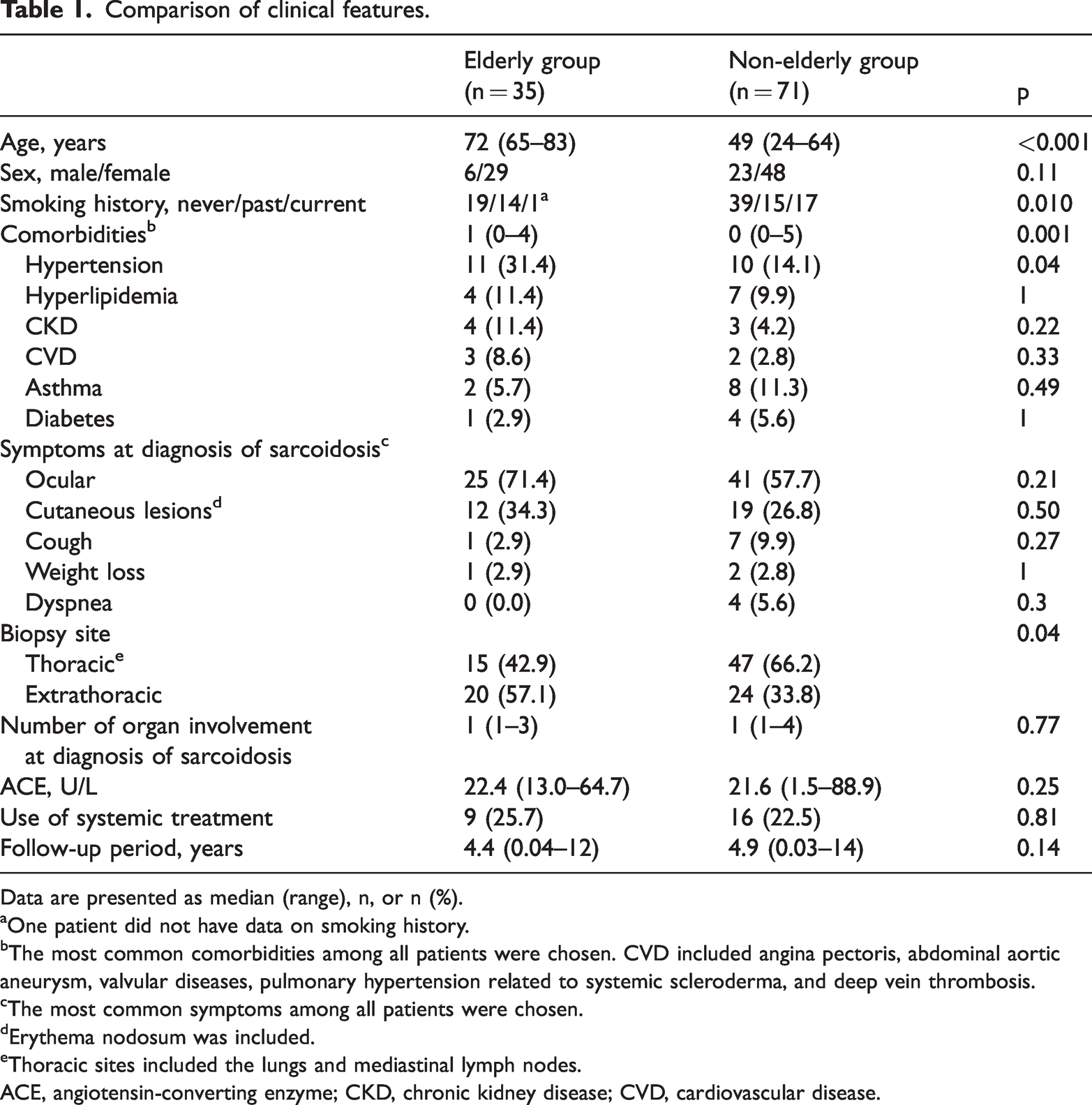
Data are presented as median (range), n, or n (%).
aOne patient did not have data on smoking history.
bThe most common comorbidities among all patients were chosen. CVD included angina pectoris, abdominal aortic aneurysm, valvular diseases, pulmonary hypertension related to systemic scleroderma, and deep vein thrombosis.
cThe most common symptoms among all patients were chosen.
dErythema nodosum was included.
eThoracic sites included the lungs and mediastinal lymph nodes.
ACE, angiotensin-converting enzyme; CKD, chronic kidney disease; CVD, cardiovascular disease.
Biopsy sites for diagnosis of sarcoidosis.

Data are presented as n (%).
aErythema nodosum was included.
bOthers included eyelid mass, subcutaneous mass, liver, and gastric lesions.
eTable 1 shows the involved organs at the time of diagnosis. Among sarcoidosis lesions, ocular and cutaneous lesions were frequently observed in both groups. The elderly group had significantly more muscle lesions than the non-elderly group at the time of diagnosis (11.4% vs. 1.4%, p = 0.04).
Table 3 shows the involved organs at diagnosis and any time during follow-up in the two groups. Muscle lesions developed in two elderly patients during follow-up (the time from the diagnosis of sarcoidosis to the development of muscle lesions was 5 months and 18 months, respectively). As a result, the elderly group had significantly more muscle lesions than the non-elderly group at the time of diagnosis and during follow-up (17.1% vs. 1.4%, p = 0.005). In five of the seven patients with muscle involvement, the muscle involvement was confirmed by muscle biopsy. Two patients had a clinical diagnosis of muscle involvement. However, both were diagnosed with gallium scintigraphy and magnetic resonance imaging, which is adequate for clinical diagnosis of muscle involvement of sarcoidosis. 13 In addition, orthopedists made the diagnosis. When we only considered patients with biopsy-confirmed muscle involvement, the elderly group still had significantly more muscle lesions than the non-elderly group (11.4% vs. 1.4%, p = 0.04).
Organ involvement at diagnosis and/or anytime during follow-up.
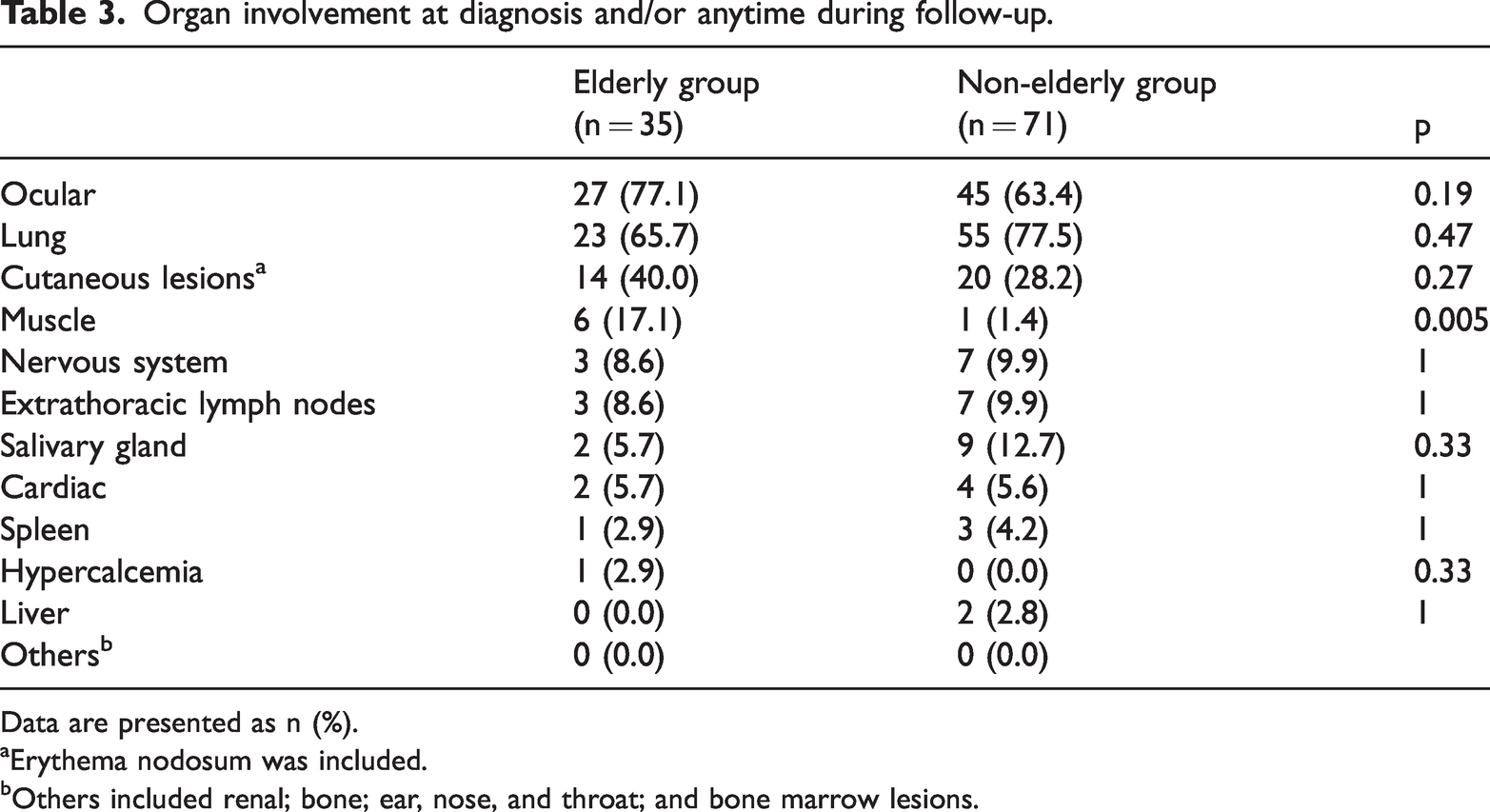
Data are presented as n (%).
aErythema nodosum was included.
bOthers included renal; bone; ear, nose, and throat; and bone marrow lesions.
Figure 2 shows the proportion of elderly patients by diagnosis period. The proportion of elderly patients increased as the diagnosis period progressed, but this trend was not statistically significant.

Proportion of elderly patients by diagnosis period. These data were analyzed using the Cochran–Armitage test of trend. There were no significant differences in the proportions of elderly patients among the three diagnostic periods (p = 0.22).
Discussion
This study was performed to evaluate the clinical features of elderly patients with sarcoidosis in Japan. The results showed that the number of comorbidities was higher among elderly than non-elderly patients, biopsies were performed more frequently at extrathoracic sites in elderly than non-elderly patients, and elderly patients had more muscle involvement than non-elderly patients.
The elderly group had more comorbidities than the non-elderly group in this study. This is consistent with the results of studies from Western countries.4,6 In general, elderly people have more comorbidities than younger people. However, clinicians should be cautious when treating elderly patients with sarcoidosis because some comorbidities might worsen with systemic steroids, which are widely used in the treatment of sarcoidosis. In fact, adverse events with steroid treatment are more frequent in elderly patients with sarcoidosis. 6 In addition, one study showed that the number of comorbidities affected the prognosis in patients with sarcoidosis. 16 In that study, however, causes of death other than sarcoidosis were more common. 16 Therefore, comorbidities themselves rather than sarcoidosis might have a great impact on the prognosis. Nevertheless, one report described an increase in sarcoidosis-related deaths among elderly patients. 17 Further studies are needed to clarify the effect of comorbidities on the prognosis in elderly patients with sarcoidosis.
In a previous report in Japan, ocular, dermal, and cardiac sarcoidosis were common types of extrathoracic involvement. 7 The number of patients with cardiac involvement in this study seemed low. This might have been due to the small number of patients, short observation period, and retrospective study design. However, another study in Japan by Sawahata et al. 1 showed that the incidence of cardiac involvement was 2.4% (14 of 588 patients), similar to the results of our study.
Extrathoracic biopsies were performed more frequently in elderly than in younger patients with sarcoidosis in our study. The involved organs usually differ between elderly and non-elderly patients. In this study, however, the sites of involvement were not significantly different between the two groups with the exception of muscle involvement. Therefore, the reason for the higher number of extrathoracic biopsies in the elderly patients in this study was probably that clinicians avoided invasive intrathoracic biopsy procedures (e.g., surgical lung biopsy) in the elderly patients. This is supported by a previous study showing that the salivary glands and skin are frequent biopsy sites in elderly patients with sarcoidosis. 4
The elderly group had more muscle involvement in this study. The incidence of muscle involvement in this study was roughly the same as that previously reported in Japan. However, muscle involvement might be under-detected in elderly patients because many such patients have muscle weakness and/or pain.18,19 Our results suggest that clinicians must exercise caution to avoid missing muscle involvement in elderly patients with sarcoidosis who have muscle-related symptoms.
This study has some limitations. First, this was a retrospective study involving a small number of elderly patients. A larger study is needed to reveal the clinical features of elderly sarcoidosis in Japan. Second, we only included patients in whom the diagnosis of sarcoidosis had been pathologically confirmed. However, it is difficult to obtain pathological specimens in some patients with sarcoidosis. In particular, invasive procedures for obtaining biopsy samples tend to be avoided in elderly patients. Hence, we might have missed some patients with sarcoidosis. Third, our research included only Japanese patients. As we mentioned above, the manifestations of sarcoidosis differ according to ethnicity and region. Further studies from other regions are therefore needed to elucidate the diverse features of elderly sarcoidosis.
In conclusion, elderly patients with sarcoidosis might have more muscle involvement and comorbidities than younger patients. Clinicians must be cautious about comorbidities and should not overlook muscle involvement in elderly patients with sarcoidosis.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605221142705 - Supplemental material for Elderly sarcoidosis in Japan
Supplemental material, sj-pdf-1-imr-10.1177_03000605221142705 for Elderly sarcoidosis in Japan by Nami Masumoto, Keisuke Watanabe, Nobuyuki Horita, Yu Hara, Nobuaki Kobayashi and Takeshi Kaneko in Journal of International Medical Research
Footnotes
Author contributions
NM and KW contributed to the conception and design of the study, collection of the patients’ data, analysis and interpretation of the data, and drafting and finalizing of the manuscript. NH, YH, NK, and TK contributed to the interpretation of the data and to finalizing of the manuscript. All authors have read and approved the final manuscript.
Data availability statement
The data supporting the findings of this study are available on request from the corresponding author. This study was partially presented at the 25th Congress of the Asian Pacific Society of Respirology, 20–21 November 2021, Kyoto, Japan.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.