
Abstract
The aim of the study was to compare the effect of exercise on postural control (PC) among the elderly with lower or higher level of habitual physical activity (HPA). The study involved 17 elderly men (mean age 72.9 ± 4.79 years). Mean velocity of the center of pressure (COP) displacements was measured using a force plate both before and after cycle ergometer exercise. A significantly higher increase in mean velocity of COP displacements and its component in the sagittal plane were observed in the group with lower level of HPA in comparison with the group with higher HPA level. Simultaneously, a relatively similar reaction to the exercise in the frontal plane was observed in both groups, possibly connected to the specific type of used exercise, which mainly activated the sagittal muscles.
Introduction
Positive influence of physical activity on health and functional fitness level among the elderly has been noted numerous times (e.g., Aoyagi, Park, Watanabe, Park, & Shephard, 2009; Daly et al., 2008; Garatachea et al., 2009; Martin, Syddall, Dennison, Cooper, & Aihie Sayer, 2009). The level of functional fitness, especially when considered in view of falls and instability, is a crucial issue for the geriatric population (Isaacs, 1965). Approximately 30% to 40% of people aged 65 and older fall at least once a year (Hausdorff, Rios, & Edelber, 2001; Tinetti & Williams, 1998). Taking into account the fact that the falls often lead to serious consequences, such as fracture of the femoral neck or even death (Kannus et al., 1999; Parkkari et al., 1999), taking steps to decreasing the risk of their incidence is quite important.
Postural control (PC) is one of the fundamental elements of proper functioning of an older person in everyday life (Hassinen, Komulainen, Lakka, Väisänen, & Rauramaa, 2005; Moreland et al., 2003). Lower level of PC is usually linked to increased postural sway, which occurs at higher values of indicators of center of pressure (COP) displacements (Gribble & Hertel, 2004; Lin et al., 2009; Nardone, Tarantola, Galante, & Schieppati, 1998; Nardone, Tarantola, Giordano, & Schieppati, 1997). The positive impact of exercise programs on the improvement in PC has been noted by numerous researchers (Cyarto, Brown, Marshall, & Trost, 2008; Maciaszek, Osiński, Szeklicki, & Stemplewski, 2007; Simmons & Hansen, 1996). Less recognized is the problem of the impact of habitual physical activity (HPA) on PC level; the existing results are quite difficult to compare because of the use of various methods of HPA and PC measurement. HPA is defined as the “total data on leisure physical activity, exercise, sports, occupational work, and other chores used to assess the overall level of regular engagement in physical activity” (p. 80, Bouchard & Shephard, 1994). Therefore, HPA should be composed of each physical activity performed as part of our lifestyle habits. HPA is assessed with the use of mechanical devices such as pedometers or accelerometers (Aoyagi et al., 2009) or questionnaires (Prioli, Freitas, & Barela, 2005), whereas PC can be determined both in a laboratory setting and in a nonlaboratory setting, force plates or optokinetic instruments (Aoyagi et al., 2009; Prioli et al., 2005) or functional tests (Berg, Wood-Dauphinee, Williams, & Maki, 1992; Tinetti & Williams, 1998), respectively. The majority of evidence gathered with the above-mentioned methods indicates that HPA has a positive impact on PC (Aoyagi et al., 2009; Daly et al., 2008; Islam, Takeshima, Rogers, Koizumi, & Rogers, 2004; Prioli et al., 2005).
The other issue is the effect of single bouts of exercise on PC. Worsening of PC following exercise of local muscle groups is well recognized among young people and involves temporary and joint-related influence (Corbeil, Blouin, Begin, Nougier, & Teasdale, 2003; Gribble & Hertel, 2004; Harkins, Mattacola, Uhl, Malone, & McCrory, 2005). Poorer results following exercise of muscles of the ankle and knee joints are observed also in the case of the elderly (Bellew & Fenter, 2006). For the most part, the observed effect is believed to originate from muscle fatigue, which in turn could lead to a decline in the neuromuscular control of balance (Corbeil et al., 2003; Harkins et al., 2005). In the case of exercises of larger muscle groups, the effect is not always clear. For example, Nardone et al. observed an increase in sway path and sway area after walking on treadmill and no effect after cycling on ergometer (Nardone et al., 1997; Nardone et al., 1998). The differences were explained by the potential role of peripheral factors connected to a distinct manner of contraction during these two types of exercise (more eccentric contraction during gait). Moreover, the effect of exercise on PC may also be related to other factors. Derave, De Clercq, Bouckaert, and Pannier (1998) observed a decline in PC only after exercise without fluid ingestion. Increase in posturograhic parameters after single bouts of exercise might also be related to hyperventilation (Zemkova, 2009). There are very few studies examining the influence of exercises of large muscle groups (e.g., walking, cycling, etc.) on PC among the elderly. The problem seems to be very important taking into account that most of the activities of daily living are performed using large muscle groups. A small immediate effect of moderate physical exercise (based on activities of daily living) on body balance in frontal plane was shown by Egerton, Brauer, and Cresswell (2009). On the other hand, Stemplewski, Maciaszek, Salamon, Tomczak, and Osiński (2012) observed unequivocal detrimental effect (increase in mean velocity of COP displacements) of moderate-intensity bicycling on PC among the elderly both in the frontal and sagittal planes. The decline was associated with higher body mass index (BMI) values and blood lactate, respectively.
Gender differences in the effects of physical exercise on PC have been observed in studies among young people. Springer and Pincivero (2009) showed a decline in PC in the sagittal plane after local exercise among men and after global exercise in women. Greater postexercise decline in dynamic PC among men in comparison with women was observed by Gribble, Robinson, Hertel, and Denegar (2009). The potential decline in PC after exercise seems to be significant among elderly men considering an increase in the risk of fall.
Higher level of physical activity may delay muscle mass and strength reduction as well as improve postural reaction performance (Perrin, Gauchard, Perrot, & Jeandel, 1999). However, to our knowledge no data exist on the effect of exercise on PC among the elderly, additionally differentiated by HPA level. The aim of our study was to compare the effect of exercise on PC among the elderly with lower or higher HPA level. We hypothesized that the magnitude of changes in PC after physical exercise of moderate intensity was greater among the elderly with lower HPA.
Method
Participants
The study involved 17 elderly men (mean age 72.9 ± 4.79 years, range = 66-81 years). Persons interested in participating in the experiment gave their consent (participation was voluntary). The selection criteria were the following: the ability to live in the community independently, particularly in terms of locomotion, and the lack of neurological, muscular, or orthopedic deficits (based on subjects’ statements). The selected subjects underwent qualifying medical examinations (i.e., medical history, resting electrocardiogram, blood pressure measurement) intended to exclude subjects with contraindications for moderate physical exercise. The subjects were familiarized with the experimental procedure (objectives of the experiment and the order of tests). The study was approved by the Bioethical Committee at Poznań University of Medical Science (Decision No. 770/06).
Subjects were divided based on the level of HPA. The implemented theoretical criterion (Haskell, Montoye, & Orenstein, 1985) divided the subjects into two groups of lower (below 4 kcal/day/kg) and higher (above 4 kcal/day/kg) physical activity level.
Habitual Physical Activity Level
HPA was assessed by Caltrac (Muscle Dynamics, Inc., Tarrance, CA) accelerometer on the basis of a week-long measurement of energy expenditure connected to physical activity (Ballor, Burke, Knudson, Olson, & Montoye, 1989; Bray, Wong, Morrow, Butte, & Pivarnik, 1994). Subjects carried Caltrac for 7 days. Total results in kilocalories were divided by the number of days and body mass to obtain standardized values.
Physical Exercise
Physical exercise was performed on a Lode Excalibur Sport ergometer (Lode B.V., Groningen, Netherlands) with Lode Ergometry Manager software. Heart rate (HR) was monitored with the use of Polar S610i sport-tester (Polar Elektro Oy, Kempele, Finland). Exercise was performed under constant medical supervision. The subjects were informed to report any complaints (e.g., dyspnea, chest pains, etc.).
The adopted target level of exercise intensity was 60% of maximum intensity. It was established on the basis of changes in HR. Target HRE (value during exercise) was calculated using Karvonen’s formula (Karvonen & Vuorimaa, 1988) taking into account HRR (value in rest), the subject’s age, and the assumed level of exercise intensity:

where %Intensity is the target level of exercise intensity expressed as percentage.
Exercise lasted for 10 minutes after HR stabilization on target level. The mean HRE value during the exercise was 112.1 ± 8.4 bpm and the mean load was 96.2 ± 16.0 W and 1.2 ± 0.2 W/kg of body mass. During the last minute of exercise, subjects were asked to estimate their subjective perception of fatigue on the basis of Borg’s RPE scale (Rating of Perceived Exertion; Borg, 1970). The scale ranged between 6 points (No exertion at all) and 20 points (Maximal exertion). Subject indicated 11.4 ± 2.9 points on average (light). This subjective estimation was adequate to the moderate intensity of performed exercise.
Measurement
To estimate PC —COP data were collected using the AccuGait™ System force plate (AMTI PJB-101 model, AMTI, Waterdown, MA). The sampling frequency was 50 Hz, and the plate was connected to a computer with Balance Trainer software provided by the manufacturer. High test–retest reliability was observed in previous work. Intraclass correlation coefficients for mean velocity of COP displacements were .84 and .96 for single and average measures, respectively (Stemplewski, Maciaszek, Osiński, & Szeklicki, 2011).
Subjects took part in PC measurements during two sessions (with a 1-week interval between the sessions). The first session, following medical qualification, contained two trials, which were used as a control measurement for both groups (no differences were observed between trials and groups). During the second session, trials took place before and directly after physical exercise (pre- and posttest) to check the effect of physical exercise on PC. Before testing procedures participants rested in a sitting position for 5 minutes (only before exercise). During testing, only the examiner and the testee were present in the room. The force plate was placed on a flat, stable surface directly next to the ergometer. The subjects stood on the plane barefoot (comfortable position of feet—about 30° in relation to each other and about 5 cm between heels), with their arms held down the side of their body. Each subject was given the task of standing as still as possible with eyes open. Each test was 30 seconds long. It has been shown previously that capturing COP movement for 30 seconds during static stance is an appropriate duration to record a reliable COP measure (Pinsault & Vuillerme, 2009). Force plate was placed 4 meters in front of the white wall and subjects were asked to look straight at the wall.
COP signals were filtered with the fourth-order low-pass Chebyshev II filter (Błaszczyk, 2008) with 10-Hz cutoff frequency (Ruhe, Fejer, & Walker, 2010). Mean velocity (V) of COP displacements and its components in anterior-posterior (AP) and medio-lateral (ML) directions (VAP and VML, respectively) were taken into account. Mean velocity is a total distance covered by COP divided by the duration of trial. It is commonly used as an indicator of PC state where increasing values of V are interpreted as a decline in PC (Bizid et al., 2009; Gribble & Hertel, 2004; Vuillerme, Forestier, & Nougier, 2002).
Statistical Analysis
Statistical analyses were computed using STATISTICA 10.0 software (StatSoft Inc., Tulsa, OK). Statistical significance was defined as p ≤ .05. The differences between the groups for age, BMI, and level of HPA were calculated with use of t test. Two-way ANOVA (analysis of variance) was employed to compare the differences between the values for the parameters of COP displacements. The analysis with two levels of the first factor (within-subject factor: “fatigue”—pretest, posttest) and two levels of second factor (between-subject factor: “group”—lower and higher level of energy expenditure related to HPA) was used. For interaction effects, the eta-squared (η2) effect size was calculated. The effect size indicates the percent of variance explained by the particular effects of the dependent variable. It was also used to calculate the power of significant effects. To compare the average values of mean velocity of COP displacement (both pretest–posttest within and between groups) Scheffe detailed post hoc comparisons were conducted. The difference between values before and after exercise was calculated (range of change—presented as percent of pre-exercise value)—in the case of experimental session for individuals with lower and higher energy expenditure.
Results
There were no statistically significant differences in age and BMI and significant difference in HPA between the groups (Table 1).
Descriptive Statistics (Means-Standard Deviations-and 95% Confidence Intervals) of Groups’ Age, BMI, and Energy Expenditure Related to HPA a
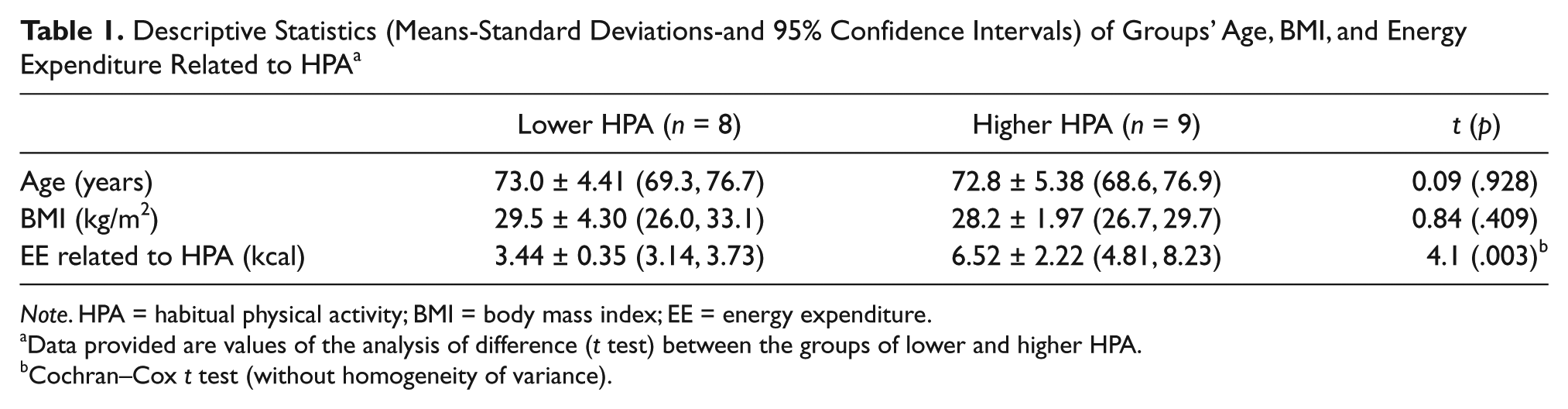
Note. HPA = habitual physical activity; BMI = body mass index; EE = energy expenditure.
Data provided are values of the analysis of difference (t test) between the groups of lower and higher HPA.
Cochran–Cox t test (without homogeneity of variance).
The two-way interaction effects “group × fatigue” were significant (V: η2 = 0.32, p < .05, power statistics = 0.70; VAP: η2 = 0.42, p < .01, power statistics = 0.86)—see Figures 1 and 2. These results indicated a significantly higher increase in the mean velocity of COP displacements after exercise for individuals with a lower level of HPA (V: pre–post Δ% = 56.79; VAP: pre–post Δ% = 60.02) than for individuals with a higher level of HPA (V: pre–post Δ% = 21.59; VAP: pre–post Δ% = 17.38).

Mean values and standard error of measurements for mean velocity of COP displacements (V) for “fatigue” factor (pre–post) in groups of lower and higher level of habitual physical activity (HPA)

Mean values and standard error of measurements for mean velocity of COP displacements in anterior–posterior direction (V AP) for “fatigue” factor (pre–post) in groups of lower and higher level of habitual physical activity (HPA)
The two way interaction effect “group × fatigue” for VML (Figure 3) was not significant (η2 = 0.01; p = .801), which indicated a relatively similar increase in the mean velocity of COP displacements after exercise for individuals with lower (pre–post Δ% = 47.75) and higher level of HPA (pre–post Δ% = 36.59).
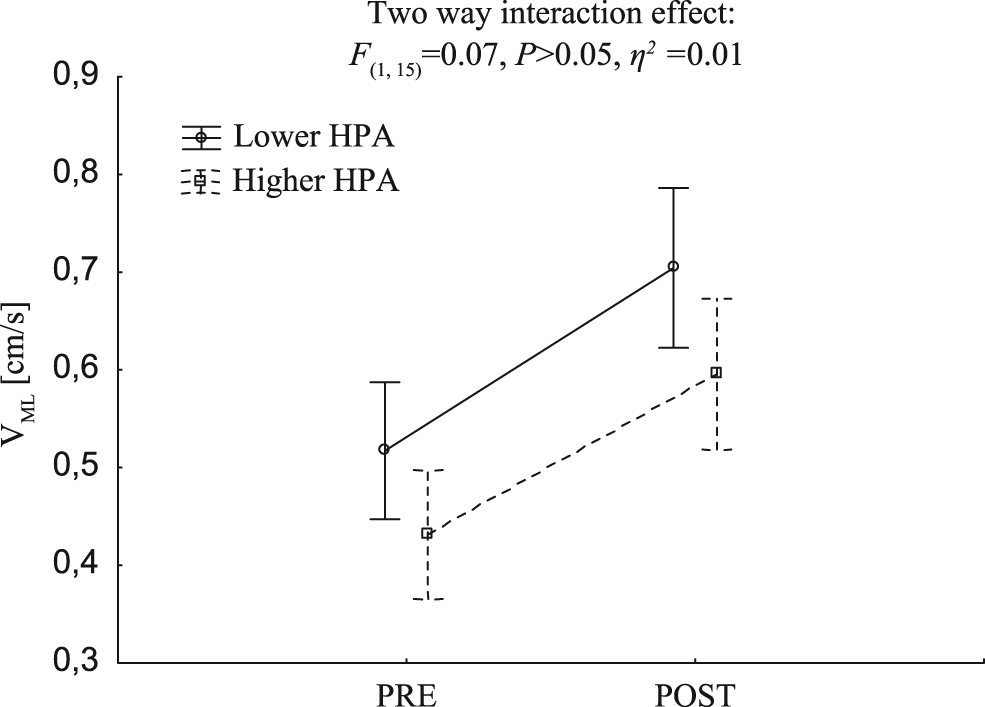
Mean values and standard error of measurements for mean velocity of COP displacements in mediolateral direction (VML) for “fatigue” factor (pre–post) in groups of lower and higher level of habitual physical activity (HPA)
Discussion
The analysis identified a significant increase in the mean velocity of COP displacements after physical exercise in comparison to pre-exercise values in the group with the lower HPA level. It might be an indicator of the decline in postural control. This effect was demonstrated repeatedly among young people (Ageberg, Roberts, Holmström, & Fridën, 2003; Bizid et al., 2009; Gribble & Hertel, 2004; Nardone et al., 1998; Zemkova & Hamar, 2005).
The studies using acute fatigue of small muscle groups indicate that observed decline in PC (e.g., increase in mean velocity of COP) in conditions of localized fatigue is joint related (Lin et al., 2009). Changes observed during the exercises that use large muscle groups are less clear. For instance, Nardone et al. (1998) reported moderate changes in body sway after 25 minutes of uphill walking with 85% of age-predicted HR but concluded that in the case of the elderly deconditioning or cardiological issues might affect body balance (Nardone et al., 1998). To the best of our knowledge only Egerton et al. (2009) studied the effect of moderate physical exercise on body balance (with the use of force plates) among the elderly and showed a small immediate effect in frontal plane. Differences between results obtained by Egerton et al. (2009) and by us (effect mainly in the sagittal plane) might be connected to different exercise protocols and standing balance assessment. In comparison to the continuous exercise used in our protocol, the authors of previously mentioned study used activities composed of various exercises (walking, stepping onto blocks in forward and sideways directions, single leg raises in standing, etc.). Additionally, a different position for balance assessment (with feet together), more challenging for control of the center of mass in frontal plane and requiring more activity by the hip abductors and adductors, was used.
There were no studies connected to the comparison of the effect of exercise on PC between men and women among the elderly. However, studies in young people showed that exercise results in greater decline in PC among men (Gribble et al., 2009; Springer & Pincivero, 2009). Gender differences might be the result of lower fatigue resistance during low-intensity exercise in men (Fulco et al., 1999) as well as a higher location of the center of gravity in men (Hageman, Leibowitz, & Blanke, 1995). Men might be more exposed to PC decline in the activities of daily living.
One of the important factors determining the observed postexercise effects may be the current level of HPA. We did not obtain a statistically significant difference in the mean velocity of COP displacements values between groups with lower and higher level of HPA in the pre-exercise trial (pretest). Most studies have found a positive relationship between HPA and PC level. Islam et al. (2004) found a positive relationship between HPA (measured with accelerometer) and static balance (measured as the time of maintaining one-leg standing balance with eyes closed). Perrin et al. (1999) found a relationship between the lifelong physical activity (participation in selected sports—running, swimming, etc.) and values of posturographic parameters during static and dynamic tests. Authors observed that the best level of control was retained by older people who were active throughout their lives, whereas the worst was found in lifelong inactive ones. Intermediate values were found in those currently active, but inactive in the past, and among those who are currently inactive. However, there are also studies that did not find any relationship between these variables (Aoyagi et al., 2009). The results obtained by us may be affected by the specificity of the research group. Even those subjects that were classified as having a lower HPA were characterized by a relatively high level of health and functionality. The absence of contraindications to exercise was necessary to participate in the study. Plausibly, there would be greater differences in the measurement under static conditions if frail elderly were included in the comparison.
The analysis identified a significantly greater increase in the average values of mean velocity of COP displacements and its component in the sagittal plane after exercise in the group with a lower level of HPA. This may indicate worse postural control as compared with those individuals with higher level of HPA. The role of HPA in maintaining functional fitness among the elderly should be taken into account for the demonstrated differences between groups in terms of V and VAP. People with a higher level of physical activity may have a higher level of functional capacity (Aoyagi et al., 2009; Brach et al., 2003; Daly et al., 2008; Garatachea et al., 2009; Martin et al., 2009). Among other things, this may be linked to a higher level of muscle strength (Garcia, Dias, Dias, Santos, & Zampa, 2011; Kozakai et al., 2005). Also, a correlation between choice stepping reaction time and leisure-time physical activity among the elderly has been noted (Tsunoda, Tsuji, Yoon, Muraki, & Okura, 2010). These factors may have a direct impact on the ability to maintain a stable posture and as a consequence might decrease the relative fall risk (Pereira, Vogelaere, & Baptysta, 2008). Higher muscle strength and shorter reaction time might allow to oppose stronger destabilizing factors and to generate faster postural adjustment.
In the case of VML, a relatively similar reaction to the exercise was observed in the groups with lower and higher levels of HPA (no interaction effect “group” × “fatigue”). It can be explained by the specificity of exercise used in the experiment. It is possible that hip abductors and adductors are not strongly activated during exercise on cycloergometer. Moreover, feet position during the assessment of postural control in our study was not challenging for control in the frontal plane in comparison with one-leg or feet together standing (Egerton et al., 2009).
Relatively low number of subjects is one possible limitation of this study. This is due to selection of group in health aspects (it was intended to exclude subjects with contraindications for moderate physical exercise). However, relatively high power statistics was observed (0.78 on average) for significant effects.
Conclusion
The level of HPA may distinguish the observed effect of decline of postural control after exercise. People with a lower level of HPA were characterized by higher increase in the mean velocity of COP displacements and its component in the sagittal plane in comparison with individuals with a higher level of HPA. Simultaneously, relatively similar changes in the postexercise values of mean velocity of COP displacements in the frontal plane were observed in both groups. It might be connected to the specific type of used exercise, which mainly activated the sagittal muscles.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from the Ministry of Science and Higher Education in Poland (No. N404 149534).