
Abstract
Recent findings suggest that men have higher mortality rates than women after a hip fracture. Although the risk of osteoporotic fractures in men is increasing, male osteoporosis still remains underdiagnosed and undertreated. In general, male osteoporosis is given low priority by policy makers in public health initiatives. The purpose of this study is to examine the patterns of use and gender distribution of DXA (dual-energy X-ray absorptiometry) scan usage at a university medical center in the United States. The total number of DXA scans increased during the study period while the percentage of men studied actually declined. The results of this study may lead to heightened awareness among providers who are caring for male patients at risk for osteoporosis.
Osteoporosis is a disease that is characterized by low bone mass with an increase in bone fragility and fracture risk (NIH Osteoporosis and Related Bone Diseases National Resource Center, 2011). An underlying cause can be identified in up to 50% of osteoporotic men (Gielen, Vanderschueren, Callewaert, & Boonen, 2011). Common causes of secondary osteoporosis are glucocorticoid excess, hypogonadism, excessive alcohol consumption, gastrointestinal malabsorption syndromes, renal insufficiency, chronic respiratory disorders, rheumatoid arthritis, ankylosing spondylitis, malignancy, anemia, hyperthyroidism or excess thyroxine, hyperparathyroidism, anticonvulsants, smoking, and immobilization (Campion & Maricic, 2003; Ebeling, 2008; Gielen et al., 2011; Nguyen, Bakshi, & Borum, 2010).
Approximately one third of all hip fractures worldwide occur in men (Gullberg, Johnell, & Kanis, 1997). Recent studies suggest that men have higher mortality rates than women after a hip fracture and those men may experience fractures at higher bone mineral density (BMD) values than women (Diamond, Thornley, Sekel, & Smerdely, 1997; Haney & Bliziotes, 2008). More men than women die in the year after a hip fracture, with a mortality rate in men of up to 37.5% versus 28.2% in women (Jiang et al., 2005). The number of hip fractures is predicted to increase markedly over the next 35 years, and the most conservative estimate is an increase of 135% in men and 100% in women (Gullberg et al., 1997).
Male osteoporosis is increasingly being recognized as a major public health problem in the United States and around the world (Kaufman & Goemaere, 2008). And although it is a serious threat to the health and well-being of affected men, it is largely underdiagnosed and undertreated (Haas & Moore, 2007; Kaufman & Goemaere, 2008). The International Society for Clinical Densitometry and the American College of Physicians both have published guidelines that recommend BMD testing for men older than 70 years or men younger than 70 years who have risk factors for secondary osteoporosis (Lewiecki et al., 2008; NIH Osteoporosis and Related Bone Diseases National Resource Center, 2011; Qaseem et al., 2008).
Although the risk of osteoporotic fractures among men is increasing due to aging of the population, there is still a perception among lay public and policy makers that osteoporosis is a disease of women (Marx & Quinn, 2009). This perception contributes to the policy gaps in the prevention, diagnosis, and treatment of male osteoporosis (Marx & Quinn, 2009). Multiple published guidelines recommend that male patients should get screened with DXA (dual-energy X-ray absorptiometry) scan (Hochberg & Adler, 2008; Lewiecki et al., 2008; National Osteoporosis Foundation, 2011; NIH Osteoporosis and Related Bone Diseases National Resource Center, 2011; Qaseem et al., 2008). It is unclear, however, whether this has resulted in increased DXA screening in males. This study examines the patterns of use and gender distribution of DXA scan usage at the University of Missouri (MU) over a 5-year period.
Materials and Methods
All DXA scans performed on male patients from January 1, 2005, to December 31, 2009, in the MU health care system were identified. We reviewed electronic and paper chart medical records of all male patients who had DXA scans for age, body mass index, ethnicity, and common risk factors for osteoporosis. In addition, data were collected on the gender distribution of all outpatients aged 18 years and older who attended MU clinics during the same time period. The study was approved by our facility’s institutional review board.
Results
The total number of outpatient visits at MU during the same period was 195,025, of which men made up 42% of visits (Table 1). Of 3,820 patients who had DXA scans during the study period, 411 (10.76%) were male. The average age of the male group was 58 years, and the total number of men ≥70 years was 104. Of the 411 male patients, weight and height data were available for 404. The average body mass index of these patients was 28. Caucasians made up 90% of male DXA recipients followed by African Americans at 8.3% (Table 2). Rheumatologists, nephrologists, endocrinologists, and primary care physicians commonly ordered the DXA screening exam.
All Outpatient Visits at MU and DXA Scan Gender Distribution

Note. MU = University of Missouri; DXA = dual-energy X-ray absorptiometry.
Demographics of Men Who Had DXA Scan
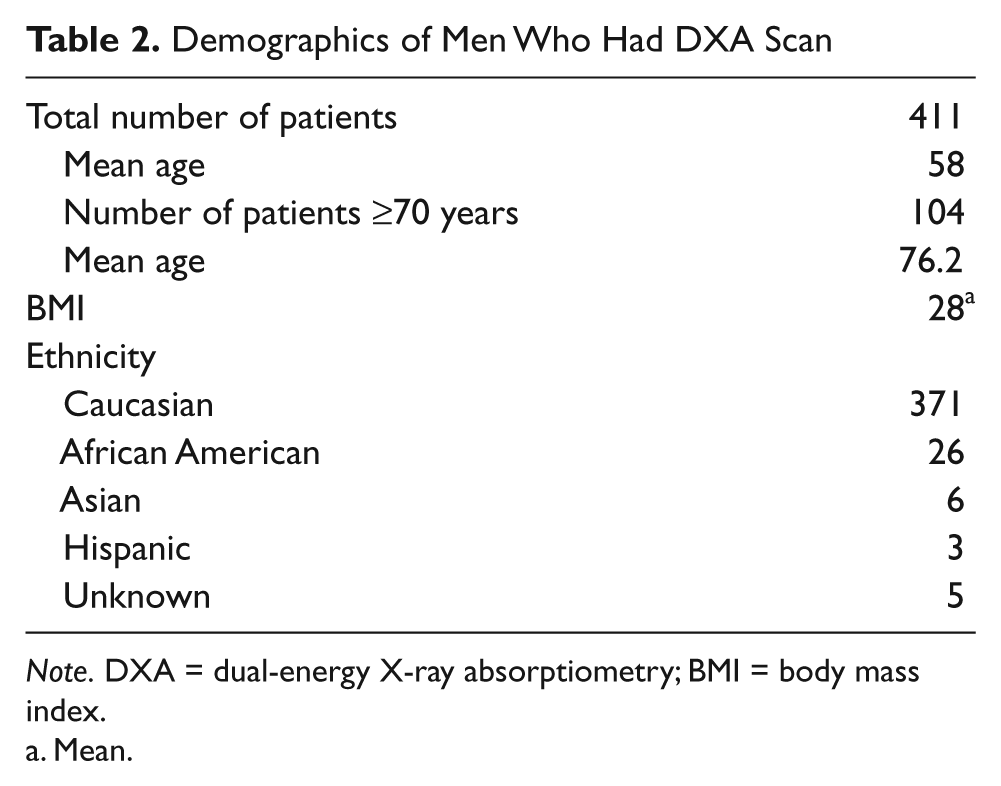
Note. DXA = dual-energy X-ray absorptiometry; BMI = body mass index.
Mean.
Indications for DXA screening in male patients included chronic corticosteroid use, vertebral and other fractures, androgen deficiency, smoking, age >70 years, excessive alcohol usage, monitoring osteoporosis therapy, primary hyperparathyroidism, anticonvulsant treatment, and low body weight. The majority of male patients had a single risk factor as the reason for DXA screening (n = 393, 67.68%). Corticosteroid usage was the most common indication for screening (41.98% of patients), followed by age over 70 years (15.11%; Table 3). A total of 213 patients had DXA scans diagnostic of osteoporosis (BMD T score −2.5 or less). Osteopenia (T score between −1.0 and −2.4) was seen in 102 patients and 96 patients had normal DXA scans.
Clinical Indications Among Men Who Had DXA Screening
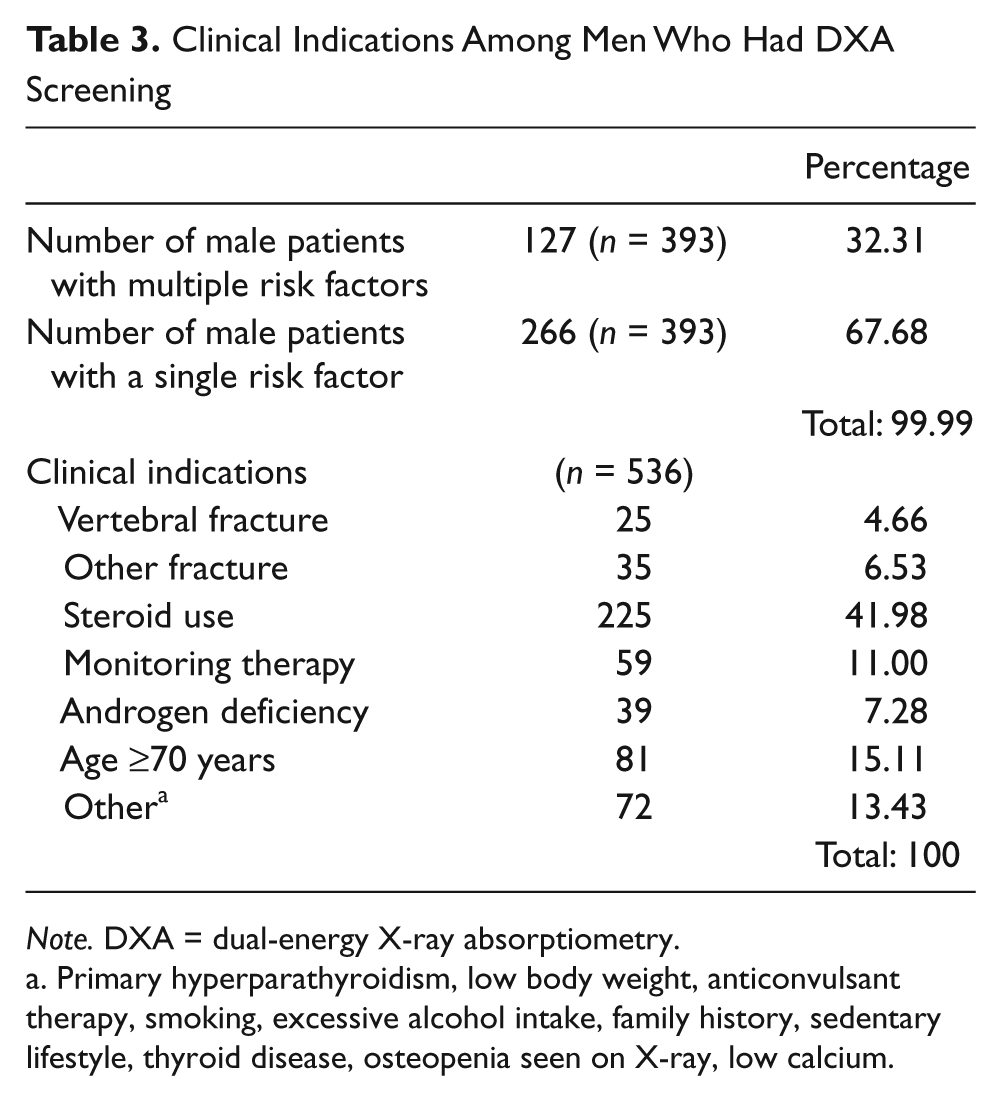
Note. DXA = dual-energy X-ray absorptiometry.
Primary hyperparathyroidism, low body weight, anticonvulsant therapy, smoking, excessive alcohol intake, family history, sedentary lifestyle, thyroid disease, osteopenia seen on X-ray, low calcium.
The total number of DXA scans (males and females) rose by approximately 66% between 2005 and 2009. However, the percentage of male patients screened for osteoporosis in our study group decreased by 5.36% between 2005 and 2009 (Table 4).
DXA scan by year

Note. DXA = dual-energy X-ray absorptiometry.
Discussion
Comparison data from the National Health and Nutrition Examination Survey (NHANES) 2005–2006 and the NHANES III showed that 30% of older U.S. men had osteopenia at the femur neck and 2% of men had osteoporosis (Looker, Melton, Harris, Borrud, & Shepherd, 2010). This study, using a cohort from an academic center, illustrates that males accounted for 46% of the outpatient clinic population but accounted for only around 10% of DXA recipients. In this study, 51.8% of men screened with DXA scans had osteoporosis and 24.8% had osteopenia, making a total of 76.6% diagnosed with either osteoporosis or osteopenia, which demonstrates that a significant number of men screened at our facility have low BMD. It could, however, be argued that if 76.6% of the men scanned had low bone density, then the prescreening process was successful and DXA was being used appropriately.
A recent Veteran Affairs (VA) study in Tampa, Florida, identified 4,919 patients who had BMD scans from 2001 to 2004 (Bass, Pracht, & Foulis, 2007). In that study, Caucasian men aged 70 years and older and taking medications with potential bone-loss side effects were the most common risk factors for DXA scans performed. More than 50% of male scans were given to those aged between 60 and 79 years. This study was done outside the VA and included a more diverse population. A large number of men in our cohort who had osteopenia or osteoporosis were receiving corticosteroids for autoimmune diseases such as rheumatoid arthritis or immunosuppression for organ transplant. About 42% of male DXA recipients in our cohort were receiving steroids and age >70 years was an indication for DXA screening only in 15%. In this article, we changed the setting to an academic center and found that despite published guidelines the percentage of DXA scans in males decreased in our study.
There are limitations to this study. The data are from a single center and may not reflect the practice patterns in other settings. The majority of the study population was Caucasian with underrepresented minority populations. Data on treatment or change in medical management were not collected. The collected data do not establish a difference in the number or percentage who presented with a specific risk factor that had a DXA scan. This study may have missed DXA studies that were ordered but not performed.
Future research studies should include surveys of awareness of male osteoporosis among providers; multicenter, larger studies examining awareness of male osteoporosis and screening among providers; and sample populations that include more ethnic groups. Future studies should also address other reasons why DXA screening is not as commonly performed in male patients. Primary and specialist indications may differ in screening for male osteoporosis.
Primary care physicians, rheumatologists, endocrinologists, and other specialists who care for men at high risk for significant bone loss and fractures need to assess risk factors, educate patients, perform relevant screening, and provide appropriate therapy with vitamin D, calcium, or the addition of bisphosphonates. Regardless of all the published guidelines over the past few years promoting the need for increased male osteoporosis screening, awareness is low in this academic community. Larger studies examining DXA screening in men are needed to increase the awareness about this major public health problem.
Footnotes
Acknowledgements
The authors wish to thank Tom McCord (Computer Project Manager in the Department of Radiology) and Carla Pudenz (Administration Associate in the Division of Rheumatology) for their assistance in data collection.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
This research was supported by the University of Missouri Health Care System in Columbia, Missouri.