
Abstract
Sexual violence is a serious public health problem that has been associated with negative mental and physical health outcomes. Few existing studies have examined the prevalence and patterns of adverse mental health among victims of sexual violence using data from nationally representative samples of U.S. adults. The main objectives of this study were to identify patterns in the associations between sexual violence victimization and depression and anxiety (DA) symptoms using data from the sexual violence and DA Behavioral Risk Factor Surveillance System (BRFSS) modules. Stratified multivariate logistic regression models were conducted to test the associations between sexual violence victimization and DA controlling for demographic characteristics. Multiple stratified MANOVA models were used to detect the effect of sexual violence victimization on DA symptoms while controlling for key demographic characteristics. Among all 61,187 participants, more than 5% (n = 3,240) were victims of sexual violence, out of which 18.82% reported being diagnosed with depression, 8.37% reported an anxiety disorder, and 28.28% reported being diagnosed with DA disorder. Victims of sexual violence reported significantly higher number of days when they had trouble concentrating, sleep difficulties, poor appetite, little interest or pleasure in activities, blamed themselves for personal failure, felt depressed, and had little energy. The present study highlights the importance of collecting nationally representative data from victims of sexual violence and extends previous findings from clinically based studies. This study also serves as an example of an analytic approach that addresses a public health priority area by drawing on data from multiple topic-specific BRFSS modules.
Introduction
Sexual violence is a serious public health problem that has been associated with long-lasting negative mental and physical health outcomes (Choudhary, Coben, & Bossarte, 2008; Norris & Feldman-Summers, 1981; Resick, 1993; Walker, Archer, & Davies, 2005a). In 2007, the last year for which data are available, results from the National Crime Victimization Survey indicate that an estimated 248,300 women and men were victims of rape or other forms of sexual assault (Rand, 2008). Estimates from a nationally representative sample of U.S. adults suggest that as many as 1 in 6 females and 1 in 33 males experience some form of sexual violence during their lifetime (Tjaden & Thoennes, 2006). However, studies that have estimated the prevalence of male sexual violence victimization have produced conflicting results, with estimates ranging from 0.6% to 22.2% depending on the study sample, notably lower than estimates of female victimization calculated using comparable data (Tewksbury, 2007; Tjaden & Thoennes, 2006).
An emerging body of research is establishing a strong association between sexual violence victimization and poor mental health (Hedtke et al., 2008; Kaminer, Grimsrud, Myer, Stein, & Williams, 2008; Mechanic, Weaver, & Resick, 2008; Rentoul & Appleboom, 1997; Ullman, Filipas, Townsend, & Starzynski, 2007; Walker, Archer, & Davies, 2005b) that may differ for women and men (Afifi et al., 2009; Reid et al., 2008), and results from previous studies have suggested that sexual violence victimization can affect mental and physical health across the life course (Leserman, 2005; Messman-Moore, Brown, & Koelsch, 2005; Santiago, McCall-Perez, Gorcey, & Beigel, 1985). For example, victims of sexual assault have been shown to be at an increased risk for posttraumatic stress disorder (PTSD), depression, and anxiety disorders (Messman-Moore et al., 2005; Santiago et al., 1985). Results from a nationally representative sample of U.S. adults indicated that 33% of female and 24.2% of male victims of sexual violence received counseling for adverse mental health outcomes as a result of their most recent victimization (Tjaden & Thoennes, 2006). However, research among female victims of rape suggests that as much as 40% of all victims may never seek professional help for mental health problems (Amstadter, McCauley, Ruggiero, Resnick, & Kilpatrick, 2008). Despite lower than expected levels of mental health service utilization, existing studies have suggested that symptoms of depression and anxiety disorders are prevalent among both men and women who were victims of sexual violence (Fergusson, Swain-Campbell, & Horwood, 2002; Norris & Feldman-Summers, 1981).
Results from studies examining symptom severity and clinical presentation using samples of females obtained from clinical settings have suggested that symptom severity, for diagnoses such as depression or PTSD, are strongly associated with sexual violence victimization (Cortina & Kubiak, 2006; Schwartz, 1991) and may be more pronounced than similar symptoms among victimized males. However, findings from studies of male victims of sexual violence suggest that 97% of male victims reported experiencing feelings of depression and 92% reported feelings of anxiety (Walker et al., 2005a). Population-based studies have also suggested a strong association between recent (within the last 12 months) and distant (lifetime) sexual violence victimization and adverse mental health indicators among both males and females (Choudhary et al., 2008).
Despite an extensive history of research on the prevalence and correlates of sexual violence, few studies have compared gender differences in the prevalence and consequences of sexual violence victimization among members of the general U.S. adult population. The main objectives of the present study were to compare the prevalence of poor mental health among male and female victims of sexual violence and to identify patterns in the associations between victimization and symptoms of depression and anxiety.
Method
Data were obtained from the 2006 Behavioral Risk Factor Surveillance System (BRFSS) survey, an ongoing data collection program designed to collect data on risk factors and health behaviors using a nationally representative sample of U.S. adults. Detailed information about the questionnaire and data collection process can be obtained from the BRFSS website (http://www.cdc.gov/brfss/; Centers for Disease Control and Prevention [CDC], 2006). Briefly, BRFSS is cross-sectional telephone survey conducted by state health departments. The questionnaire has three parts including a core component used by all states, topic-specific optional modules, and state-added questions. The topic-specific optional modules are supported by the CDC and chosen by the participating state. This study uses data from respondents who responded to the core questionnaire and two optional modules, sexual violence and depression and anxiety modules, which were administered in 11 U.S. states and territories in year 2006. The response rate among participating states ranged from 31.8% to 58.4% in 2006.
Variable Recoding
Sexual violence victimization was identified using a single question in the BRFSS sexual violence module asking about unwanted sexual intercourse experienced at any point in the respondent’s lifetime. The question asked, “Has anyone EVER had sex with you after you said or showed that you didn’t want them to or without your consent.” The reference group for all analyses was respondents reporting no victimization. Correlates of sexual violence victimization included eight depression and anxiety symptom questions and self-reported diagnosis from a health care professional of a depression and/or anxiety disorder. The eight symptom questions in the depression and anxiety module were similar to those routinely asked as part of the nine-item Patient Health Questionnaire and measured the number of days with symptoms of depression and anxiety over the past 2 weeks (Kroenke, Spitzer, & Williams, 2001). These symptoms included loss of pleasure, depressed mood, sleep problems, lack of energy, change in appetite, feelings of failure, difficulty concentrating, and feeling slow or agitated. Questions asking about a diagnosis of depression and/or anxiety included the following: (a) “Has a doctor or other health care provider EVER told you that you have a depressive disorder (including depression, major depression, dysthymia, or minor depression)?” (b) “Has a doctor or other health care provider EVER told you that you had an anxiety disorder (including acute stress disorder, anxiety, generalized anxiety disorder, obsessive–compulsive disorder, panic disorder, phobia, PTSD, or social anxiety disorder?” Response options included yes and no. Based on responses to these diagnosis questions, three mutually exclusive outcome categories were created. The first category, “depression only,” included those respondents who answered “Yes” to the question asking about a diagnosis of a depressive disorder and answered “No” to the question asking about a diagnosis of an anxiety disorder. The second category, “anxiety only,” defined those respondents who answered “Yes” to the question asking about a diagnosis of an anxiety disorder and answered “No” to the question asking about a diagnosis of a depression disorder. The third category “both depression and anxiety” included respondents who answered “Yes” to the diagnosis of both depression and anxiety disorders.
Controls for each regression model included age, gender, marital status, race/ethnicity, income, and education. Age was divided into six categories (18-24, 24-34, 35-44, 45-54, 55-64, and 65+ years). All participants were divided into four main racial/ethnic categories including White, African American, Hispanic, and Others. Marital status included married, unmarried, and divorced or separated categories. Educational attainment was dichotomized into “attended high school or less” and “more than high school education.” Annual household income groups were divided into less than $25,000, $25,000-$50,000, and above $50,000 categories.
Data Analysis
Stratified multivariate logistic regression models were conducted to test the associations between depression and anxiety disorder diagnoses and sexual violence victimization while controlling for demographic measures and other potential confounders (age, gender, marital status, race/ethnicity, income, and education). To identify gender-based differences in symptoms, all analyses were conducted for the overall sample and stratified by gender. Multivariate analysis of variance (MANOVA) was used to estimate the influence of sexual violence victimization and key demographic variables (age, gender, race/ethnicity, marital status, and education) on depression and anxiety symptoms reflected by the eight symptom questions. Chi-square test of homogeneity was used to identify significant differences between frequencies. All frequencies and regression models were calculated using SAS (Version 9.1) and SUDAAN (Version 9.01).
Results
In 2006, a total of 61,187 persons participated in the sexual violence and depression and anxiety modules. As shown in Table 1, there were 24,608 male (48.75%) and 36,579 female (51.25%) participants. A majority of participants were White (73.74%), less than the age of 54 years (67%), married (65.56%), and had more than high school education (60.26%) with an annual household income of more than $50,000 (46.59%). Among all participants, 3,240 (5.3%) reported sexual violence victimization. A majority of these participants were females (88.84%). A comparison of demographic characteristics and depression and anxiety diagnostic categories among victimized and nonvictimized groups identified several significant differences (see Table 1). Chi-square test of homogeneity results indicated that victims of sexual violence were more likely to be female (88.84%, χ2 = 502.65, p < .05) and to have been diagnosed with depression (18.82%, χ2 = 112.79, p < .05), anxiety (8.37%, χ2 = 25.47, p < .05), and both depression and anxiety (28.28%, χ2 = 192.96, p < .05).
Sample Composition a
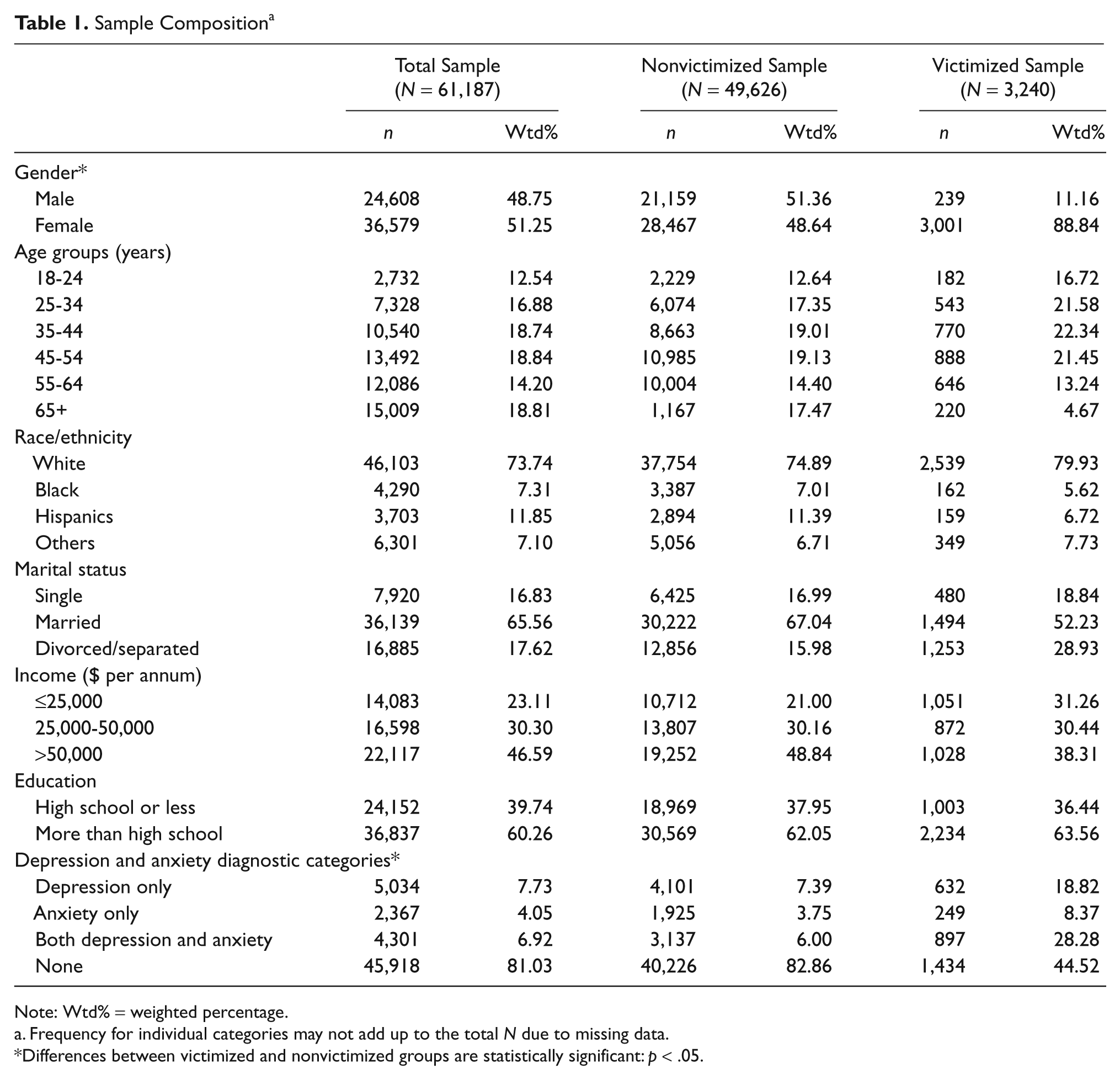
Note: Wtd% = weighted percentage.
Frequency for individual categories may not add up to the total N due to missing data.
Differences between victimized and nonvictimized groups are statistically significant: p < .05.
Comparisons of bivariate associations between sexual violence victimization and diagnosis with depression and anxiety disorder are shown in Table 2. Overall, the pattern of associations between sexual violence victimization and categories of depression and anxiety disorder were similar among males and females. When compared with participants who reported no victimization, those who reported victimization were more likely to report being diagnosed with depression (adjusted odds ratio [ORadj] = 3.42, 95% confidence interval [CI] = 2.80, 4.17), anxiety (ORadj = 3.18, 95% CI = 2.28, 4.43), and both depression and anxiety disorders (ORadj = 5.40, 95% CI = 4.45, 6.56). Males who reported sexual violence victimization, when compared with males who did not report victimization, were more likely to report being diagnosed with depression (ORadj = 3.11, 95% CI = 1.39, 6.94), anxiety (ORadj = 4.75, 95% CI = 1.78, 12.69), and both depression and anxiety disorders (ORadj = 4.29, 95% CI = 2.09, 8.82). Similarly, females who reported sexual violence victimization had higher odds of being diagnosed with depression (ORadj = 3.49, 95% CI = 2.85, 4.28), anxiety (ORadj = 3.03, 95% CI = 1.39, 6.94), and both depression and anxiety (ORadj = 5.69, 95% CI = 4.66, 6.94) when compared with females who reported no victimization.
Associations Between Sexual Violence Victimization and Diagnostic Categories of Depression and Anxiety

Note: ORadj = adjusted odds ratio, that is, adjusted for gender (for “Total” population only), age, race/ethnicity, marital status, education, and income level; CI = confidence interval; PAF = population attributable fraction. Analysis = multinomial logistic regression.
p ≤ .05. **p ≤ .001. ***p ≤ .0001.
Results from MANOVA analyses suggest that sexual violence victimization, demographic variables, and their interactions had a statistically significant effect on the symptom profile of depression and anxiety (see Table 3). Sexual violence victimization along with other demographic variables was associated with changes in the mean number of days with depression and anxiety symptoms among the victimized population when compared with those who reported no victimization. Significant association in sexual violence victimization and gender of the victim was observed. However, the effect size of the demographic measures and their interactions with sexual violence victimization was relatively small (Table 3). Comparisons of the reported mean number of days with symptoms of depression and anxiety by both victimized and nonvictimized males and females are shown in Figure 1. Post hoc Scheffe’s tests also indicated significant differences in the mean number of days with symptoms of depression and anxiety when victimized males and females were compared with nonvictimized males and females, respectively.

Depression and anxiety symptom profile of victimized and nonvictimized males and females
Effect of Sexual Violence Victimization and Key Demographic Variables on Depression and Anxiety Symptom Profile

Note: Analysis = multivariate analysis of variance (MANOVA).
Discussion
The current study examined the associations between depression and anxiety symptom profiles among victims of sexual violence using data from two BRFSS topic-specific modules. This study estimated the prevalence of depression and anxiety disorders among victimized and nonvictimized adult populations. Overall, our results identify that the prevalence of depression and anxiety disorders among victims of sexual violence is significantly higher when compared with the nonvictimized population. Additionally, strong associations between depression and anxiety disorder and sexual violence victimization were observed when controlling for demographic variables and other potential confounders. The prevalence of depression and anxiety disorders among the victimized and nonvictimized samples was comparable with those reported in previous studies (Fergusson et al., 2002; Walker et al., 2005a).
Depression and anxiety disorders are among the most prevalent psychological disorders in the general population. In a nationally representative sample of U.S. adults, 28.8% reported experiencing significant anxiety symptoms and 20.8% of U.S. adults reported experiencing significant symptoms of depression (Kessler, Berglund, Demler, Jin, & Walters, 2005). Our results identified higher prevalence of depression and anxiety disorder among both males and females who experienced sexual violence victimization when compared with nonvictimized participants. Consistent with previous findings, a higher prevalence of self-reported diagnosis and average number of days with symptoms of depression and anxiety among victimized females suggest an association between poor mental health and sexual violence victimization (Cortina & Kubiak, 2006; Fergusson et al., 2002; Walker et al., 2005a). The current study identified a similar relationship between depression and anxiety symptoms among victimized males using population based data.
Sexual violence victimization has been associated with a variety of adverse mental health consequences in previous studies (Choudhary et al., 2008; Santiago et al., 1985; Walker et al., 2005a). The prevalence of a diagnosis of depression, anxiety, and both depression and anxiety disorders was higher among victimized males and females when compared with those reporting no victimization. A higher prevalence of internalizing behaviors, such as those associated with depression and anxiety disorders, have been previously reported among female victims of sexual violence (Cortina & Kubiak, 2006; Fergusson et al., 2002), and our findings support these observations. However, in previous studies the prevalence of adverse mental health experiences among male victims of sexual violence has not been extensively studied or compared with the prevalence of mental health indicators among similarly victimized females. Results from this study identified a greater prevalence of depression and anxiety disorders among victimized males when compared with nonvictimized males. Although the overall prevalence was lower among male victims when compared with females, the prevalence of depression and anxiety disorders among victimized males suggests that adverse life experience, like sexual violence, may be associated with an increase in internalizing behaviors regardless of gender (Norris & Feldman-Summers, 1981; Resick, 1993).
An association between sexual violence and a combined symptom profile of depression and anxiety among both males and females that is consistent with previous studies (Schwartz, 1991; Street, Gradus, Stafford, & Kelly, 2007) were observed. Symptoms like insomnia or excessive sleeping, change in appetite, depressed mood, little energy, and feelings of failure are standard diagnostic criteria used to assess the presence of depression and anxiety disorders (Gilbody, Richards, Brealey, & Hewitt, 2007). Overall, the self-reported average number of days with symptoms of depression and anxiety disorders was higher among both male and female victims when compared with those reporting no victimization. Existing research suggests that both male (Tewksbury, 2007) and female (Davies, Pollard, & Archer, 2006) victims of sexual assault are significantly more likely to report poor mental health, including lack of sleep, loss of appetite, feelings of failure, and aggressive behavior.
In addition to the higher prevalence of symptoms of depression and anxiety disorders, self-reported physician or health care professional diagnoses of depression and anxiety disorders were also strongly associated with sexual violence victimization independent of gender. Similar findings were reported by studies using clinical samples of sexual violence victims (King & Woollett, 1997; Walker et al., 2005a). The identification of consistent findings in a population-based sample strengthens support for the hypothesis that depression and anxiety disorders are more prevalent among victims of sexual violence and highlights the importance of population-based analysis to supplement and extend clinically-based studies.
The results of present study provide important insight into sexual violence victimization and associations with depression and anxiety but are subject to several limitations. Despite weighting to adjust for sampling design and survey nonresponse, estimates calculated as part of this study used data obtained from a subsample of states may not be representative of total U.S. population. Also, questions in the BRFSS modules assessing depression and anxiety differ from other commonly used measures of anxiety (Beck, Epstein, Brown, & Steer, 1988). These differences may affect item response and may have influenced comparisons with results from other studies. Reports of victimization are based on self-reports and have not been corroborated using external data sources. Furthermore, the eight-symptom BRFSS module assessed a limited number of anxiety-related phenomena and did not address outcomes that have previously been associated with trauma, such as hyperarousal, nightmares, or avoidance of trauma-related stimuli (Beck et al., 1988; Breslau & Anthony, 2007). Finally, our results are based on cross-sectional data testing associations between self-reported victimization and poor mental health indicators and cannot determine causality.
Nationally representative survey data can be used to provide a broader understanding of mental health consequences that may be associated with sexual violence victimization. These results expand the current literature by providing support of the mental health problems associated with sexual victimization in a nationally representative population. This study is an example of an analytic approach that addresses a public health priority area like sexual violence by drawing on data from multiple topic-specific BRFSS modules. The use of publicly available population-based data sources such as BRFSS can help estimate the prevalence of potentially underreported and stigmatizing public health problems like sexual violence and can be used to enhance understanding of associated poor physical and mental health.
The findings of this study highlight the need for a better understanding of male sexual assault. Priorities for future studies might include the epidemiology of male sexual assault; more nuanced understandings of the emotional, physical, and psychological consequences of sexual violence victimization; and the development of targeted interventions informed by understanding of gender differences in definitions of sexual assault. Future studies are urged to use available data sources from multiple sources to enhance understanding of comparatively rare events such as male sexual assault.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported, in part, by grant #5R49CE001170 from the National Center for Injury Prevention and Control, CDC, to the West Virginia University Injury Control Research Center. Contents are solely the responsibility of the authors and do not represent official views of the CDC.