
Abstract
Men infected with HIV are often faced with caregiving responsibilities of aging, ill parents, while simultaneously looking for support from their parents in dealing with their own health problems. Unfortunately, the reciprocal roles of HIV-positive adult sons and aging mothers as caregivers have not been examined. To address this gap in the literature, HIV-positive men (n = 118) answered open-ended questions about the support they exchanged with their mothers, completed the Depth of Relationships Inventory, and rated the importance of health-related assistance between themselves and their mothers. The men viewed themselves as important providers of both instrumental and emotional support to their mothers. Men perceived their mothers to be significant providers of emotional support but only moderately important in providing instrumental support. About a third of the men responded that the help they provided and received from the mothers in managing each other’s health and staying healthy was extremely important. Men regarded their relationships with their mothers as one of their most important social relationships. Non-White men rated the quality of their mother–son relationships more highly, exchanged more instrumental support, and provided more emotional support to their mothers than White men. Men who disclosed their HIV-positive status to their mothers rated the importance of the help they received from their mothers in managing their illnesses higher than men who had not disclosed.
Keywords
Introduction
More than 1.1 million persons in the United States are living with HIV/AIDS. Men comprise about 73% of the HIV/AIDS population (Centers for Disease Control and Prevention, 2009). Although HIV/AIDS affects all race/ethnicities, the impact has been more serious among minorities. Blacks/African Americans account for about half of the HIV diagnoses even though they comprise only about 13.6% of the U.S. population (Centers for Disease Control and Prevention, 2011). Hispanics/Latinos are also disproportionally affected. The rate of new HIV infections among Hispanic/Latino men is more than twice that of White men (Centers for Disease Control and Prevention, 2010).
HIV infection has been referred to as a family disease, not only because multiple members of a family may be infected but also because unaffected members can become intensely involved in the disease experience as providers of social support (DeMatteo, Wells, Salter Goldie, & King, 2002). Partners, parents, and siblings of HIV positive individuals often experience psychological pain and trauma unlike that caused by any other crises they have had to face (Siegl & Morse, 1994). Family members may be thought of as emotionally co-infected because they share similar psychological symptoms (Flaskerud, 1995).
In addition to the psychological ramifications of HIV infection, the family faces other challenges. Although HIV infection is no longer considered a terminal disease, persons living with the infection often suffer from debilitating symptoms that can interfere with activities of daily living. Management of the disease is often difficult with frequent health care visits, laboratory tests, and adherence to complicated medication regimens (Sacajiu, Raveis, & Selwyn, 2009). To maintain healthy immune systems, persons with HIV infection must be vigilant about good nutrition, regular exercise, and avoidance of common infections (Swendeman, Ingram, & Rotheram-Borus, 2009). The psychological ramifications combined with the challenges of maintaining a healthy lifestyle make HIV infection a unique disease that affects family members who may be called on to provide assistance.
The age of persons living with HIV/AIDS has increased. HIV/AIDS has become a chronic rather than a terminal disease. Americans aged 40 to 49 years now constitute the largest proportional group of persons living with HIV/AIDS (27% of the total), followed by
As the age distribution of persons living with HIV/AIDS has shifted over the years, the implications for family members have changed as well. Adults living with this chronic disease may be forced to look to aging parents for emotional and instrumental support (Johnston, Stall, & Smith, 1995). Persons living with HIV/AIDS may be unpartnered or have partners who are also ill and cannot provide care. Relying on parents may conflict with the expectation that adult children should be independent, especially if aging parents have difficulty adjusting to the caregiving strains associated with the illness. Of all family members of origin, mothers tend to provide more support (Kadushin, 1999) and are most often engaged by community agencies to assume support roles for their adult HIV-infected children (Thompson, 2000). Adult sons’ relationships with mothers are closer than relationships with their fathers (Barnett, Marshall, & Pleck, 1992).
In this article, HIV-positive men’s perceptions of their relationships with their mothers were examined. The article focused on the exchange of emotional and instrumental support and the quality of mother–son relationships. Important factors (e.g., race/ethnicity and disclosure of HIV-positive status to mothers) were also examined to determine their impact on the sons’ perceptions of their mother–son relationships.
Background Literature and Guiding Concepts
Filial Responsibility
A major concept in the social science research on families and aging is filial responsibility, which is conceptualized as a societal attitude toward adult children’s duty to meet the needs of aging parents (Lee, Netzer, & Coward, 1994; Stein et al., 1998). Both parents and adult children acknowledge the existence of filial responsibility as a societal expectation. Filial responsibility is a useful concept on the sociocultural level but it does not focus on expected specific behavior that adults develop in their ongoing relationships with their parents. Intergenerational aid actually flows in two directions—from parents to children as well as from children to parents. Exchange patterns typically reflect a reciprocity effect—aid provided by one generation may be reciprocated by the other. Previous researchers found that older parents who received more aid from their adult children typically provided more aid to their children as they were growing up (Lee et al., 1994; Stein et al., 1998).
The importance of filial responsibility varies across the life course. By definition, filial responsibility assumes that kin duties are important to adults when their parents are aged, infirm, and in need of assistance. Thus, parental obligation is likely to become an important issue for adult children as they approach middle age and anticipate the needs of their aging parents. Previous researchers found, in general, that the bonds between parents and their adult children are remarkably resilient across the life course (Blieszner & Mancini, 1987; Connidis & McMullin, 1994; Rossi & Rossi, 1990). However, when an adult child is living with a serious illness such as HIV/AIDS, parents’ feelings of obligation to provide assistance to them may extend well past the “conventional” age of children’s independence.
Although norms of filial responsibility are nearly universal in the United States, research has suggested that they may vary by cultural background. Attachment to these norms is stronger among Latinos and African Americans than among non-Latino Whites. Older African Americans, for instance, expect more help from their adult children than similarly aged White elders (Burr & Mutchler, 1999). Older members of minority groups generally report a stronger attachment to social norms of filial responsibility than older Whites.
Living with a stigmatized disease, such as HIV/AIDS, may also affect the flow of social support between adult children and their parents in other ways. Persons living with the disease are often reluctant to disclose their HIV-positive status to their closest family members for fears of criticism, rejection, and even abandonment (Kalichman, DiMarco, Austin, Luke, & DiFonzo, 2003). Failure of adult children to tell their parents about their infections may block important intergenerational sources of support.
Mothers as Caregivers of Adult Sons Living With HIV/AIDS
As Nelms (2000) has observed, “One invisible and silent phenomenon associated with the AIDS epidemic is the return of mothers to care for their adult sons who are dying of the disease” (p. 46). Much attention has been given to children whose parents have died of AIDS. Almost no attention has been paid to the roles of parents of persons living with HIV/AIDS other than recognition of their responsibility as grandparents caring for children orphaned by AIDS.
The most extensive research on parents’ role in caregiving for adult sons and daughters living with HIV/AIDS has been conducted in countries outside the United States. Findings from studies in Thailand indicate that parents, usually the mother, provide at least some care for almost two thirds of Thai adults who have died of AIDS and acted as primary caregivers in half of the cases (Knodel & Saengtienchai, 2005; Knodel, Watkins, Van Landingham, 2002; Saengtienchai & Knodel, 2001). In a study conducted in Cambodia, researchers found that parents were intimately involved in many facets of their adult children’s experiences with HIV/AIDS, including serving as a link to the health care system and the community at large. Older aged parents encouraged their adult children to attend medical appointments and support groups. The parents served as general caregivers of their adult children by supporting medication adherence and encouraging positive health behaviors, such as obtaining adequate nutrition and maintaining good hygiene (Williams, Knodel, Kim, Puch, & Saengtienchai, 2008).
However, there is little research that has focused specifically on the instrumental and emotional support that older parents and mothers in the United States provide to their sons who have HIV infection. In a qualitative study involving in-depth interviews with nine women, including three mothers of adult children with HIV/AIDS, Bunting (2001) found that women played important caregiving roles, including helping their adult family members manage the health consequences of their HIV infection. Interestingly, in this study, the female caregivers recognized the value of reciprocal support and acknowledged that their family members living with HIV/AIDS benefitted from providing help to others.
Sons as Caregivers: The Gendered Nature of Men’s Caregiving
Research on filial caregiving has typically focused on the care provided to elderly family members by adult daughters or daughters-in-law. Adult sons also provide care to older parents, of course, but their contributions are often overlooked in research (Kramer & Thompson, 2004). When sons provide care for aging parents, they tend to perform tasks consistent with traditional or normative roles for men, such as home maintenance chores and financial or managerial assistance (Campbell & Martin-Matthews, 2003). Thus, “the depth and complexity of men’s caregiving is influenced not just by the gendered context of caregiving per se but also by the gendered nature of individual tasks” (Campbell & Martin-Matthews, 2003 p. S357).
In this article, emotional and instrumental social support exchanges between sons and aging mothers and the quality of the mother–son relationships in the context of HIV infection were explored. Data for the analysis reported in the article were obtained from sons’ responses to open-ended and survey questions. Additionally, factors (e.g., race/ethnicity and disclosure of HIV-positive status to mothers) that potentially could affect the mother–son relationship and the social support were examined.
Method
Sample
The findings reported in this article involve responses from participants (i.e., sons) who had living mothers and had answered questions at the 12-month time point in a larger study that has been described previously (Uphold, Rane, Reid, & Tomar, 2005). The larger study is a 24-month prospective cohort investigation to determine the biopsychosocial predictors of health-related quality of life and immune and virologic outcomes of men who had been diagnosed with HIV/AIDS. Clinicians at three infectious disease clinics in the southeastern United States (i.e., a Veterans Affairs medical center, a university hospital, and a public health department) referred patients to the principal investigator. After a detailed explanation of the study, patients who agreed to participate were enrolled if they met inclusion criteria.
Participants were enrolled until a target sample size of 226 (as determined by a power analysis) was achieved. Participants, in the larger study, had to be at least 18 years old, male, and English speaking. They also had to have positive enzyme-linked immunosorbent assay (ELISA) screening and Western blot tests for HIV. Those who were currently taking corticosteroids and testosterone replacement therapy, had symptoms of acute bacterial and viral infections, had been diagnosed with HIV infection less than 3 months, had a recent (i.e., within 30 days) change in antiretroviral medications, and/or were demented or moribund were excluded from participation. Participants were interviewed at three time points (i.e., baseline, 12 months, and 24 months). The analysis reported in this article focuses only on men who participated in data collected at the 12-month time point and who had living mothers. At the 12-month follow-up, a total of 197 participated. Attrition was due to incapacitation associated with the progression of the disease, death, or geographic mobility. Of the 197 men, 118 had living mothers. These 118 men comprise the sample for the analysis in this article.
Data Collection
Participants were interviewed by a member of the research team and completed self-report questionnaires. Veni-punctures were performed to obtain blood samples for analyses of CD4+ T cells. Members of the research team reviewed the patients’ medical records to validate demographic and clinical data obtained during the interviews. Detailed demographic, medical, and social psychological information was obtained for each participant.
Measures
Sociodemographic and health-related characteristics
Age (in years), education level (less than a high school education vs. high school or beyond) and marital/partnered status (married or partnered vs. not married or partnered) were measured using 12-month self-reports. Racial/ethnic categories included Caucasian/White, African American/Black, Hispanic/Latino, and Asian/Pacific Islander. Because of the small number of Latinos and Asians/Pacific Islanders, we recoded race/ethnicity as Whites versus all non-Whites.
Multiple health-related characteristics were measured by self-report. Participants were asked which antiretroviral medications they were currently taking to combat their HIV infections. Participants were asked how many years they had been living with HIV/AIDS from time of diagnosis. Participants were asked to indicate their likely mode of exposure to HIV (i.e., blood transfusion, exchange of blood or intravenous drug use, intimate heterosexual contact, intimate homosexual contact, other, or unknown). Symptom frequency was measured with a modified instrument that was originally developed by Whalen, Antani, Carey, and Landefeld (1994). Participants rated the frequency they experienced 21 symptoms (e.g., fatigue, fever, diarrhea, weight loss, and skin problems), on a scale from never (0) to every day (3). Total scores on the symptom scale ranged from 0 to 63. To measure disclosure of HIV-positive status, participants were asked if they had disclosed their HIV-positive status to their mothers (yes or no).
Types of social support exchanged
At the 12-month time point, participants were interviewed and answered open-ended questions about their mother–son exchange of social support. The participants responded to the following open-ended items to measure the support they received from their mothers: “Please tell me what your mother does to take care of you?” “Please tell me how or why your mother has an impact on your future health.” They also responded to the following two items to measure the support they provided to their mothers: “Please tell me what you do to take care of your mother?” “Please tell me how or why you think you have an impact on your mother’s health.”
Importance of help exchanged in managing sons’ and mothers’ illnesses and health
To obtain quantitative information on the care and assistance that was exchanged between mothers and their adult sons, the participants answered two questions that were developed for this study. Participants rated how important their mothers were in helping them to manage their illnesses and/or to stay healthy on a scale from 1 (not at all important) to 10 (extremely important). In addition, they rated how important they were in helping their mothers manage their illnesses or stay healthy on a scale from 1 (not at all important) to 10 (extremely important).
Quality of the mother–son relationship
All the participants also completed one part of the Quality of Relationship Inventory (QRI) questionnaire at the 12-month follow-up. The QRI is a 39-item measure that assesses individuals’ perceptions of interpersonal conflict and relationship depth for each of several significant relationships (Pierce, Sarason, & Sarason, 1991). In this study, participants answered eight items from the Depth of Relationship subscale of the QRI with regard to their relationships with their mothers. This subscale measures the individuals’ beliefs about the commitment, security, and strength of the interpersonal bond between the individual and his mother. (The actual statements and mean scores on each item are presented in a table later in the text.) All items were rated on a 4-point scale (i.e., 1 = not at all, 2 = a little, 3 = fairly, 4 = very). The participants’ total scores were obtained by computing the mean of their responses across all items in the subscale. In this study, the standardized Cronbach’s alpha coefficient for the Depth of Relationship Inventory subscale for men’s perceptions of their relationship with their mothers was .93.
Data Analyses
Qualitative data analyses
Responses to the open-ended interview questions were content-analyzed. The principal investigator read all the responses and identified broad categories of responses. The research team then discussed and refined the categorization. A trained research assistant coded all the responses into the identified categories. A second coder, who was well acquainted with the data, reviewed the categorization of the data. The two coders agreed on more than 90% of the coding decisions. When differences in coding arose, the coders discussed the disagreements and consensus was reached. In the final step, the frequency of responses within each of the categories was calculated. Key quotations from participants were tracked to illustrate common response patterns.
Quantitative data analysis
Descriptive statistics were used to delineate the men’s sociodemographic, health-related characteristics, quality of the mother–son relationship, and the importance of the help exchanged in managing sons’ and mothers’ illnesses and health. Pearson product–moment correlations and t tests were conducted to test for associations between the men’s sociodemographic and health-related characteristics (i.e., age, race/ethnicity, education, mode of exposure to HIV, marital/partnered status, disclosure of HIV-positive status to mothers) and the quality of the mother–son relationships. t Tests were conducted to determine if there were differences between non-White and White men and between men who had disclosed their HIV-positive status and those who had not disclosed in terms of the help exchanged in managing the sons’ and mothers’ illnesses and health.
Results
Background Characteristics of the Sample
The mean age of participants was 44.4 years (SD = 7.6). The majority of the participants (n = 90, 76%) were not married or partnered. A total of 60% (n = 71) of the participants had greater than a high school education. Overall, 42% (n = 50) of the sample was non-White and included 45 African American, 4 Hispanic/Latino American, and 1 Asian/Pacific Islander men.
Approximately 45% of the participants (n = 53) in the sample reported that they were exposed to HIV through intimate sexual contact with other men. Nearly all the study participants (n = 106, 90%) were taking highly active antiretroviral therapy or a combination of three or more medications to combat the HIV infection. The mean years of living with HIV/AIDS from time of diagnosis was 7.9 years (SD = 5.3). The mean number of symptoms reported by the men in our subsample was 7.8 symptoms (SD = 5.85). The majority of men (80%) in this sample reported that they had disclosed their HIV-positive status to their mothers.
Types of Social Support Exchanged
Our team-based coding of responses to open-ended questions concerning the types of social support provided to and received by HIV-positive men and their mothers produced two similar sets of categories. Table 1 summarizes the frequency with which major categories of social support were exchanged between sons and their mothers. The middle column of the table presents the percentage of sons who reported that they provided the type of help to their mothers, whereas the third column presents the percentage of sons who reported that they received the type of help from their mothers. As shown in Table 1, emotional support emerged as the most common type of assistance provided by sons to their mothers and mothers to their sons. Nearly two fifths of the participants (39%) reported that they provided and received emotional support to/from their mothers. One son, aged 54 years, non-White, and unmarried/unpartnered said, regarding the types of help he received from his mother, “She is my rock.” Another son, aged 62 years, White, and married, responded that “without her, there would be a vacancy in my life. I need her support.” A 41-year-old, non-White, unmarried man said, “She provides me with good spiritual and mental health. Home is always home. I wouldn’t be here without her support.” Two men stated that their mothers provided them with moral or values background. A 57-year-old, married non-White son said, “(She) taught me a way of life. She gave me a spiritual background. Without her, I would be nothing.” A related type of support—instigating social interaction, which included calling, visiting, and sending cards or letters—also emerged in our open-ended coding. Sons were more likely to mention that they initiated interaction with their mothers than to mention that their mothers initiated interactions with them (18% and 13%, respectively). A 41-year old, non-White, unmarried/unpartnered son said, “I’m there for her. We communicate. She calls on me for advice and direction and support.”
Types of Social Support Exchanged Between HIV-Positive Adult Sons and Their Mothers (N = 109)

Note. Nine participants did not respond to interview questions concerning their social support exchange with mothers because of fatigue or time constraints.
Several categories of instrumental support were also reported by the sons in the study, though a gendered difference emerged in the types of support sons provided as compared with the types of support they received from their mothers. Performing household chores (e.g., cooking, doing housework, cleaning, and laundry) was mentioned as a major type of support exchanged between mothers and sons. About 16% of the men said they did household chores for their mothers, but 25% said their mothers did this for them. A 40-year-old, non-White, unmarried son said, “When I get sick, she cares for me, feeds me, helps bathe me, cleans my house.” Another (41 years, non-White, unmarried) said, “She does everything for me—washes my clothes, cleans my house, makes my meals.” Several men described the reciprocity in this type of assistance. For example, one son (44 years, White, unmarried) said, “I do the same for her as she does for me: cooking . . . running errands.” However, sons were more likely to talk about providing lawn care, auto maintenance, and/or household repairs, as one 41-year old, non-White, unmarried man said, “(I do) anything she needs. I help around the house. I’m Mr. Fix-it.” A gender-typed pattern also emerged in sons’ provision and receipt of transportation: 17% said they provided transportation to their mothers but only 6% said their mothers provided transportation for them. A 47-year-old, White, unmarried son said, “I buy medications, take her grocery shopping, to appointments, and to visit family and friends.” Sons were also more likely to report providing financial help to their mothers than they were to receive it (15% vs. 2%, respectively).
A less common form of instrumental assistance reported by HIV-positive men involved health monitoring, that is, keeping track of medical appointments and medicine and sharing information about health and well-being. Nine percent of the sons reported that they performed this role for their mothers, whereas 8% said their mothers did this for them. A 36-year-old, non-White, unmarried participant replied, “She prepares my pills and helps me take them.” Another (28 years, White, unmarried) gave a similar response: “She asks me about my meds, tiredness, doctors, nutrition.” Some sons also reported performing this type of function for their mothers. A 41-year-old, non-White, unmarried participant said, “I send her information about things she’s going through—illnesses, her diet, her arthritis, and I encourage her to walk.”
Two additional codes that emerged frequently in the analysis of responses to the open-ended questions that asked about the types of social support exchange between HIV-positive sons and their mothers were “everything/anything” and “nothing.” Participants were considerably more likely to report that they would do anything and/or did everything for their mothers than they were to say that their mothers did everything for them (10% vs. 1%, respectively). One married son (38 years, White) said, “I provide financial and emotional support. I do house repairs. I help as much as I can. If I don’t, my wife does.” Nearly one quarter of the sons said they did nothing to help their mothers and roughly the same proportion said their mothers did nothing for them. The primary reason given for doing nothing to help their mothers was geographic distance and/or mothers’ unawareness of their sons’ infection with the HIV virus. In some cases, the participants indicated that their mothers were too old and/or ill to be told that their sons were HIV positive. All but one of the men who said that their mothers did nothing to help them were older than 40 years, suggesting that these mothers were elderly or approaching the later stages of their own lives and were not able to provide assistance. One 59-year-old participant said, “My mother is 86 years old. She doesn’t know about my HIV status. She doesn’t take care of me.” Another participant, somewhat younger at the age of 48 years, also said that his mother was unaware of his status. “She worries too much. (And) she lives in Ohio.”
Race Differences in Support Exchanged
We explored race difference in the types of support White and non-White sons exchanged with their mothers. The proportion of men in each race category who said that nothing or everything was exchanged was also reported. Table 2 summarizes the responses participants gave concerning the type of assistance, if any, they provided to their mothers. Emotional support was mentioned as the primary type of assistance provided by sons, regardless of race, to their mothers. A similar proportion of White and non-White men reported that they provided emotional support (40% vs. 38%, respectively). The pattern of responses pertaining to initiation of social interaction was similar: 21% of White men and 15% of non-White men gave this response.
Race Differences in Types of Social Support Provided by HIV-Positive Adult Sons to Their Mothers (N = 109)

Note. Nine participants did not respond to interview questions concerning their social support exchange with mothers because of fatigue or time constraints.
Race differences did emerge, however, with regard to provision of instrumental assistance. Non-White men were considerably more likely than White participants to report providing household chores (34% vs. 18%), to providing transportation (30% vs. 8%), and to providing financial assistance (21% vs. 10%) to mothers. Non-White men were considerably more likely than White participants to say they do everything for their mothers (19% vs. 1%) and considerably less likely to say they did nothing to help their mothers (11% vs. 32%).
Table 3 summarizes race differences in sons’ perceptions of the types of support their mothers provided to them. Differences emerged with regard to emotional support provided by mothers to adult sons (49% of non-White participants vs. 32% of White participants) and in specific types of instrumental support. Non-White participants were more likely to report that their mothers assisted them by doing household chores (40% vs. 13%) and providing transportation (11% vs. 2%). Non-White participants were also substantially less likely to say that their mothers did nothing to help them manage their illness (21% vs. 32%).
Race Differences in Types of Social Support Provided by Mothers to HIV-Positive Adult Sons (N = 109)
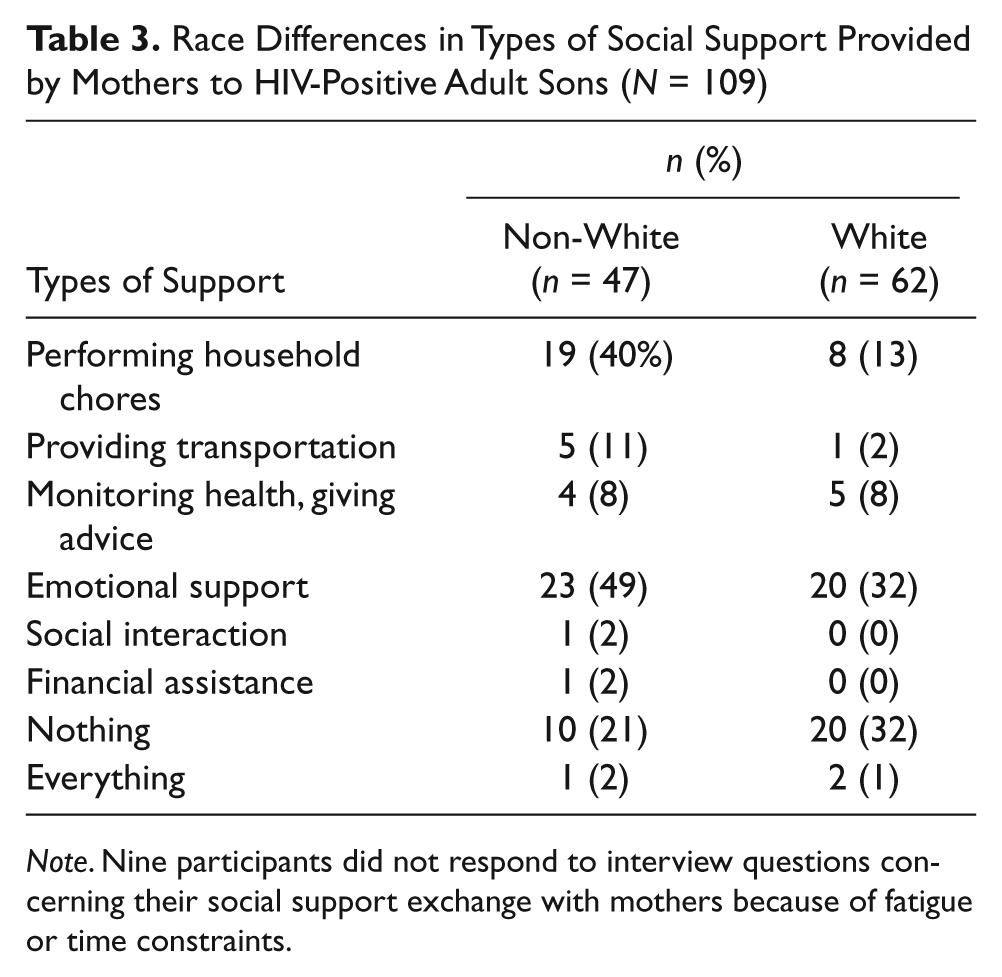
Note. Nine participants did not respond to interview questions concerning their social support exchange with mothers because of fatigue or time constraints.
Importance of Help Exchanged in Managing Sons’ and Mothers’ Illnesses and Health
Information regarding sons’ perceptions of the role they and their mothers played in helping each other manage their illnesses and health was collected. The mean rating of the importance of the mothers in helping the participants (i.e., sons) manage their illness or stay healthy was 5.2 (SD = 3.9). In all, 29% of the sons (n = 34) responded that their mothers were not at all important (response of “1” on the 10-point item). Almost an equal number of men (n = 33, 28%), however, stated that their mothers were extremely important. On the other hand, 40 sons (34%) reported they were extremely important in helping their mothers manage their illness or staying healthy. Additionally, 21% of the sons (n = 25) said they were not at all important in this regard. The mean rating of the importance of the sons in helping their mothers manage their illness or staying healthy was 6.1 (SD = 3.7).
There were significant differences between non-White and White participants in ratings of the importance of their mothers in helping them maintain their own health, t(116) = 3.45, p ≤ .001, as well as their importance in helping their mothers manage their illnesses and stay healthy, t(116) = 3.453, p ≤ .001. Mean scores on the first question (“How important is your mother in managing your illness . . .”) were 6.56 (SD = 3.9) and 4.22 (SD = 3.6), for non-White and White participants, respectively. Mean scores on the second question (“How important are you in managing your mothers’ illness . . .”) were 7.38 (SD = 3.5) and 5.06 (SD = 3.6), for non-White and White participants, respectively.
There was a significant difference in sons’ ratings of the importance of mothers in managing their illnesses and health between sons who had disclosed their HIV status and sons who had not disclosed, t(114) = −4.44, p < .0001. Sons who disclosed their sero-status rated their mothers’ importance in health matters (M = 5.9, SD = 3.7) higher than those who had not disclosed (M = 2.2, SD = 3.0). On the other hand, there were no differences in the sons’ ratings of their importance in managing their mothers illnesses between sons who disclosed their HIV status (M = 6.2, SD = 3.6) and those who had not disclosed (M = 6.0, SD = 3.8).
Quality of the Mother–Son Relationship
Responses to the Depth of Relationships Inventory are summarized in Table 4. An examination of responses to individual items on the inventory suggests that sons perceived their relationships as primarily positive. The mean response to Item 1, which asked participants to rate the significance of their relationship with their mother, was 3.55 (on a scale of 1, low, to 4, high). Similarly, when asked to rate how much they would miss their mothers if they could not see or talk to each other for a month (Item 6), the majority (60%) said they would miss them very much (M = 3.22). The same proportion said that if they could only have a small number of relationships (Item 7) they would want to include their relationships with their mothers (M = 3.36). Item 2, which asked sons how much they depended on their mothers (which can refer to instrumental rather than emotional support) had the lowest mean score (M = 2.38).
Mean Scores on Items in the Depth of Relationship Inventory (N = 118)

Note. Response alternatives are 1 (not at all) through 4 (very).
Most of the sons’ sociodemographic (e.g., age, married/partnered status) and health-related characteristics (e.g., number of symptoms, duration of HIV infection, disclosure of HIV positive status) were unrelated to the quality of their mother–son relationships. However, there was a significant relationship between race and quality of mother–son relationship, t(116) = 3.33, p = .0012. Non-White men rated the quality of their relationships higher than White men.
Discussion
Our data support theorists and previous researchers who observed that the bonds of parents and adult children are resilient across the life course (Blieszner & Mancini, 1987; Connidis & McMullin, 1994; Lee et al., 1994; Stein et al., 1998). The significance of the mother–son relationship during life-threatening illnesses is highlighted by both the qualitative and quantitative findings in this study. Answers to the open-ended questions revealed that many men regarded themselves and their mothers as primary sources of support for one another. The importance of the mother–son relationship is underscored by quotes, such as “she [mother] is my rock” and “without her, there would be a vacancy in my life.” Quantitative findings revealed that the majority of men rated the quality of the mother–son relationship as high and stated they if they could only have a small number of relationships they would want to include their relationships with their mothers.
The findings also support the theory that exchange of intergenerational support is typically reciprocal, with a positive association between aid given and received from parent to child (Lee et al., 1994; Stein et al., 1998). The percentage of men who reported providing emotional support to mothers was similar to the percentage of men who reported receiving emotional support. A similar percentage of men responded that the help they provided to, and received from, their mothers in managing each other’s health and staying healthy was extremely important. Nonetheless, there were some differences in reciprocity of the flow of social support. For example, sons mentioned providing more transportation services and financial assistance to mothers than they received.
The findings also support Campbell and Martin-Matthews’s (2003) research that men and women provide support that is consistent with the traditional or normative, gender roles. Men reported providing mothers help with lawn care, auto maintenance, and home repairs. On the other hand, mothers provided more support doing household chores, such as cooking and cleaning.
Interestingly, most of the son’s demographic and health-related characteristics did not have an impact on the sons’ perceptions of the mother–son relationship. For example, the expectation that increased age would exacerbate the complications of living with HIV/AIDS, and consequently increase dependence on mothers was not supported. A similar expectation—that married or partnered men would have alternative sources of support other than their mothers and, as a result, report less reliance on or closeness to their mothers—was not supported. Findings regarding the stigma associated with HIV/AIDS acquired through sexual contact with other men (Dowshen, Binns, & Garofalo, 2009) led to an expectation that mode of exposure to HIV (e.g., homosexual contact vs. other exposures) would be significantly correlated with sons’ relationship with their mothers. This expectation was not supported by the findings. The expectation that men who had more HIV-related symptoms and concomitantly more compromised health would need to rely on their mothers for more support than other men was also not supported.
In contrast, the sons’ race did have an impact on the mother–son relationships. Non-White participants rated the quality of their mother–son relationships higher than White participants. The types of support sons exchanged with mothers also varied by race. Non-White participants were more likely to report providing and receiving more instrumental support than White participants. Whereas a similar proportion of White and non-White men reported they provided emotional support to their mothers, a higher proportion of non-White sons reported they received emotional support from their mothers. These findings support previous researchers who have found that norms of filial responsibility are stronger among members of minority groups as compared with White groups (Burr & Mutchler, 1999).
Disclosure of HIV-positive status to mothers was another variable that affected the mother–son relationship. As expected, sons who had disclosed their HIV status rated the importance of the help they received from their mothers in managing their illnesses as more important than sons who had not disclosed their HIV-positive status. This finding is consistent with other studies (Kalichman et al., 2003; Smith, Rossetto, & Peterson, 2008) that there is a close association between disclosure and perceived social support. Disclosure of HIV positive status is probably a prerequisite for receiving help and care with HIV-related symptoms and treatments from mothers. Surprisingly, however, disclosure of HIV status to mothers was unrelated to ratings of the quality of the mother–son relationships and the importance of the sons’ help in managing the mother’s illness. This finding underscores the complexity of the association of disclosure and emotional bonds within families. As noted by Derlega, Winstead, and Folk-Barron (2000) disclosure of HIV positive status has unexpected consequences and can disrupt personal relationships. Men’s acknowledgment that they have a stigmatizing disease, such as HIV infection, potentially can lead to criticism and rejection by their mothers.
For health care professionals, the study findings have important implications. Professionals need to be aware that adult sons and their aging mothers often have special relationships. Both are potentially available sources of support to the other when illness or disability occurs. The study findings provide support for the growing body of research about men’s roles as caregivers. However, it is also important to remember that every family is different and that some mother–son relationships are not supportive. For example, in this study, about one fourth of the men stated that they provided and received no support from their mothers. Health professionals should keep in mind that other social networks such as friends and health care workers may need to be accessed for meeting physical and emotional needs of family members in unsupportive relationships.
The finding that adult sons living with HIV/AIDS believed they provided more instrumental support in terms of financial support and help in transportation than they received from their mothers raises other issues for health professionals to consider. Older parents, particularly mothers, may be willing but not able to help sons who are living with HIV/AIDS. Aging mothers may have limited economic resources as well as difficulty performing activities of daily living, such as driving, which limits their ability to assist their sons cope with serious illnesses. However, physical illness and disability from either HIV infection or aging, in the case of mothers, may not be important factors in the exchange of emotional support and help in monitoring illness. Thus, health professionals need to be cognizant of the importance of both sons and mothers in helping each other maintain a positive outlook as well as helping mange their illnesses.
Health professionals caring for and counseling men with HIV infection should be aware that certain factors, such as race and disclosure of HIV-positive status, may affect the mother–son relationship. In this study, non-White men rated the quality of their mother–son relationships more positively and had a higher reciprocity of support exchange than White men, which is consistent with Burr and Mutchler’s (1999) statement that minority groups have stronger attachment to the social norms of filial responsibility than Whites. In addition, men who disclosed their HIV-positive status to mothers rated the importance of help received from mothers in managing their illnesses higher than men who had not disclosed. Health professionals must remember that sons who do not disclose their HIV status to their mothers block an important source of support if their health deteriorates or they need assistance in managing their symptoms or medications (Shehan et al., 2005).
The results must be interpreted cautiously because of limitations in the study. One limitation is that data were collected only from the son. Thus, only the son’s perception of the mother–son relationship was studied. In future studies it will be important to explore the mother’s perception of the relationship and to determine the similarities and differences between mothers’ and sons’ perceptions of the mother–son relationship. In addition, the participants were responding spontaneously about their perceptions of the support they gave and received from their mothers. Inferences about what sons and mothers actually do for one another cannot be made. Last, obtaining demographic, economic, or health-related status information about mothers is recommended for future research studies.
Conclusion
HIV/AIDS has been referred to as a family disease because unaffected members often become intensely involved as providers of support and caregivers of the individual infected with the virus. HIV infection is no longer considered a terminal disease, which has important consequences for family members. The life expectancy of persons living with HIV/AIDS has been increasing over the past two decades. People who once would not have been expected to live long enough to see their parents reach old age are now themselves living into middle age and beyond. At these ages and life stages, they may encounter their older parents’ physical and mental health decline. Thus, just as their own need for health-related assistance may start to increase, they may be called on to provide help to their parents. As this study’s findings suggest, there is reciprocity in the support exchanged between men who are living with HIV/AIDS and their mothers. Throughout the lifespan, many men have a strong sense of filial responsibility and will engage in providing care for their aging mothers. Conversely, mothers continue to play important roles in their lives even when they are old and chronically ill. The findings indicate the utility of using a life-course framework in understanding long-term family relationships of persons living with the now chronic HIV/AIDS.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
This research was based on work supported by the Health Services Research & Development, Department of Veterans Affairs (NRI98182, RCD99011).