
Abstract
Voluntary Counseling and Testing (VCT) remains low among men in sub-Saharan Africa. The factors associated with previous HIV testing and knowledge of partner’s HIV status are described for 9,107 men who visited the Muhimbili University College of Health Sciences’ VCT site in Dar es Salaam, Tanzania, between 1997 and 2008. Data are from intake forms administered to clients seeking VCT services. Most of the men (64.5%) had not previously been tested and 75% were unaware of their partner’s HIV status. Multivariate logistic regression revealed that age, education, condom use, and knowledge of partner’s HIV status were significant predictors of previous HIV testing. Education, number of sexual partners, and condom use were also associated with knowledge of partner’s HIV status. The low rate of VCT use among men underscores the need for more intensive initiatives to target men and remove the barriers that prevent HIV disclosure.
Introduction
In 2009, Africa accounted for 1.8 million of the 2.6 million new HIV infections that occurred worldwide (UNAIDS, 2010). Despite the aggressive promotion of Voluntary Counseling and Testing (VCT) services, a large number of infected individuals in Africa have not had an HIV test (Bunnell, Mermin, & De Cock, 2006; Kakoko, Åstrøm, Lugoe, & Lie, 2006). Furthermore, the risk of transmission remains high even within marriages because of the prevalence of extramarital affairs (Shisana et al., 2008). In response to the risks that are driving the HIV epidemic in Africa, prevention programs have widely promoted HIV testing and encouraged HIV-infected individuals to disclose their serostatus to their partner (Bunnell et al., 2006). Several VCT services in East African countries such as Uganda, Kenya, and Tanzania have implemented these recommendations but have not been successful in substantially increasing the proportion of men who seek VCT (Bwambale, Ssali, Byaruhanga, Kalyango, & Karamagi, 2008; Kairania et al., 2010; Miller & Rubin, 2007; Msuya et al., 2008).
According to the Tanzania HIV/AIDS and Malaria Indicator Survey, 6% of adults aged 15 to 49 years were infected with HIV in 2007-2008 (Tanzania Commission for AIDS, 2008). The spread of HIV in Tanzania has been attributed to the high rate of multiple sexual partners and the low rate of HIV testing (Tanzania Commission for AIDS, 2008). In 2007-2008, only 19% of women and men aged 15 to 49 years had been both tested for HIV and were aware of the results (Tanzania Commission for AIDS, 2008). From a public health perspective, knowledge of one’s own as well as a partner’s HIV status is imperative because it can lead to a decrease in risky sexual behavior and HIV infection (Allen et al., 1992). In addition, VCT serves as the gateway for HIV-positive people to benefit from increased access to antiretroviral treatment (Wringe et al., 2008). A study conducted among HIV discordant couples to assess the impact of VCT on condom use in Zambia revealed that men who learned of their positive HIV status were more likely to report 100% condom use than HIV-negative men (Allen et al., 2003). The authors suggested that the HIV-positive men intentionally used condom after becoming aware of their status to protect their uninfected partner. The effect of knowing one’s HIV status has also been shown to be associated with a reduction in sexual risk behaviors in the United States, with HIV-positive persons aware of their HIV status reporting a lower prevalence of unprotected anal or vaginal intercourse compared with HIV-positive persons unaware of their status (Marks, Crepaz, Senterfitt, & Janssen, 2005). These findings are similar to other studies showing that HIV-positive individuals who were aware of their partner’s HIV status were more likely to use condoms than those who were unaware (Bunnell et al., 2008; Benki-Nugent et al., 2011; Conserve, Sevilla, Younge, Mbwambo, & King, 2012).
In Tanzania, several studies have examined factors associated with VCT and HIV serostatus disclosure, but most of them have focused only on women (Antelman et al., 2001; de Paoli, Manongi, & Klepp, 2004; Kominami, Kawata, Ali, Meena, & Ushijima, 2007; Maman et al., 2002). A study of men attending a VCT clinic in Dar es Salaam indicates that some men view HIV testing as a cue to action to take precautionary preventive measures (Maman, Mbwambo, Hogan, Kilonzo, & Sweat, 2001). In another study carried out in the northern region of Tanzania, pregnant women (n = 2,654) were encouraged to invite their partners for VCT and only 12.5% of the men agreed to receive VCT (Msuya et al., 2008). The men were more likely to respond to their partner’s invitation if they had an older partner, lived with their partner or if their partner had a high monthly income, a history of treatment for STI symptoms, and intended to share their HIV results.
The low rate of VCT participation among men in Tanzania is alarming because previous studies have indicated that many men in Africa engage in risky sexual behaviors that place themselves and their partner at risk. For example, it has been reported that men in Tanzania and Nigeria seek extramarital sexual partners to increase their sense of masculinity and self-esteem when faced with situations, such as unemployment, that prevent them from fulfilling the role of provider and meeting the needs of their family (Oyediran, Isiugo-Abanihe, Feyisetan, & Ishola, 2010; Silberschmidt, 2001; Smith, 2007). In another study conducted among 584 married men in Mbeya, one of the regions with the highest HIV prevalence in Tanzania, 39% of the participants reported to have had sex with women other than their wives (Mbago & Sichona, 2011). A recent study revealed that that the only risky behavior associated with HIV among men in Tanzania was the number of sexual partners in the last 3 years (Ghebremichael & Paintsil, 2011).
Increasing the number of men who receive VCT services is crucial in curbing the AIDS epidemic in Africa. Some of the factors underlying the risky sexual behaviors of men are related to gender role norms that encourage men to be sexually active and to have multiple partners as a rite of passage to adulthood (Barker & Ricardo, 2005). Furthermore, the well-documented gender power imbalance in sexual relations that exists in many African countries also reduces a woman’s ability to negotiate safer sex as many men refuse to use condoms despite having multiple sexual partners (Langen, 2007). These contemporary gender roles also influence women’s ability to seek VCT services and prevent some women from sharing their serostatus with their partners (Peacock & Levack, 2004). In Dar es Salaam, it was reported that women’s fear of their partners’ reactions was the most common barrier to HIV testing and that the men needed to give the women permission prior to attending the VCT clinic (Maman et al., 2001).
Considering the low rate of VCT participation, the high rate of risky behaviors reported among males, and the important role men play in their households, it is crucial to investigate HIV testing behaviors of men. The present study examines the association between sociodemographic factors, number of sexual partners, condom use, and previous HIV testing as well as knowledge of partner’s HIV status among men who had sex in the past 6 months.
Method
Procedures
Data for this analysis were collected from clients seeking HIV testing between 1997 and 2008 at the Muhimbili University College of Health Sciences’ Voluntary Counseling and Testing clinic in Dar es Salaam, Tanzania. A total of 45,071 men and women were selected through convenience sampling to complete the intake form that was self-administered in Kiswahili and translated into English. To ensure that people who had multiple visits were only included once in the data set, the client ID was used to sort individuals by date of clinic attendance and the first observation (earliest date) was kept. Of the 45,071 clients, 22,808 were excluded because they were females, 8,716 were not included because they were less than 15 years old and had not engaged in sexual intercourse in the past 6 months. The remaining 4,440 were excluded due to missing data, leaving a total of 9,107 men who met all the criteria and completed all the questions for the variables used in this analysis. The form inquired about sociodemographic characteristics, HIV testing history and serostatus of the clients and their sexual partner, sexual practices, and condom use in the previous 6 months. Although some men had multiple permanent sexual partners, they only needed to know at least one of their permanent partner’s HIV status to be included in this analysis. In addition, men were also questioned about casual sexual partners; however, the majority (6,986) of the men reported that they did not have a casual partner. Therefore, there were not enough men with casual sexual partners to include in the analysis. The HIV status of the men was confirmed with the results of a Capillus HIV test.
Variables
The first outcome variable measured the men’s history of HIV testing prior to visiting the clinic. To determine testing history, clients were asked whether they had been tested for HIV. The variable was coded as follows: (1) no; (2) yes, it was negative; and (3) yes, it was positive. The second outcome variable inquired if the men’s partner had been tested for HIV and was coded as follows: (0) no; (1) yes, it was negative; (2) yes, it was positive; (3) yes, but the result was unknown; and (4) I do not know. Clients were categorized as having had an HIV test if they reported both that they had been tested and knew their HIV status. Men whose partner had been tested and knew their partner’s test result were categorized as being aware of their partner’s HIV status, whereas those whose partner had not been tested or did not know their partner’s HIV status were considered unaware.
The independent variables included sociodemographic characteristics, number of sexual partners, and condom use in the past 6 months. Individuals reported their gender (male/female). The age variable was categorized (15-25 years, 26-36 years, 37-47 years, and 48 years and older) to explore how certain stages of the life cycle such as adolescence, young adult, and adults influence previous HIV testing. This categorization was also based on the evidence that Tanzanian men in the 25 to 29 and 30 to 39 age ranges are more likely to know where to get an HIV test (Tanzania Commission for AIDS, 2008). The education variable was divided into five ascending education categories: no education, primary education, secondary, postsecondary, and university. In Tanzania, the official school attending age ranges from 7 to 13 years for primary, 14 to 19 years for secondary, and 20 to 24 years for postsecondary education (Ministry of Education and Vocational Training, 2010). Respondents reported their marital status to the enumerator; however, because of the limited number of individuals in certain categories, this variable was recoded accordingly: single, married, or divorced. Based on the reported number of children, a binary variable was created to designate the presence or absence of dependents. Responses to the question about the number of permanent sexual partners were categorized as one partner and two or more partners. Condom use was assessed by the following question: Did you use a condom during sex in the past 6 months? Responses for condom use were no, sometimes, always, and not applicable. Respondents who reported not using or sometimes using condoms in the past 6 months were combined as neither group reported consistently using condoms, and thus the risk of infecting their HIV-negative partners was high in both groups.
Statistical Analysis
The analyses consisted of univariate, bivariate, and multivariate analyses. Basic frequencies were used to describe the distribution of the sociodemographic variables, history of HIV testing, knowledge of partner’s HIV status, and behavioral variables. Due to the small percentage of HIV-positive men and those with an HIV-positive partner, the recoded versions of the two outcome variables, HIV testing (no vs. yes) and knowledge of partner’s HIV status (unaware vs. aware), were used in the bivariate and multivariate analyses. Cross-tabulation analysis between HIV testing, knowledge of partner’s HIV status, and sociodemographic and behavioral variables was performed. Last, the variables that were significant in the bivariate analyses were included in the multivariate logistic regression models to examine predictors of HIV testing and knowledge of partner’s HIV status. Separate analyses for years 1997-2002 and 2003-2008 were run to investigate if the same variables predicted the two outcomes. The majority of the significant variables for the different time frame were similar to the variables for the combined years. Therefore, only the findings for the combined years were reported. All analyses were performed using SPSS for Windows, Version 20 (IBM SPSS Inc., Chicago, IL).
Results
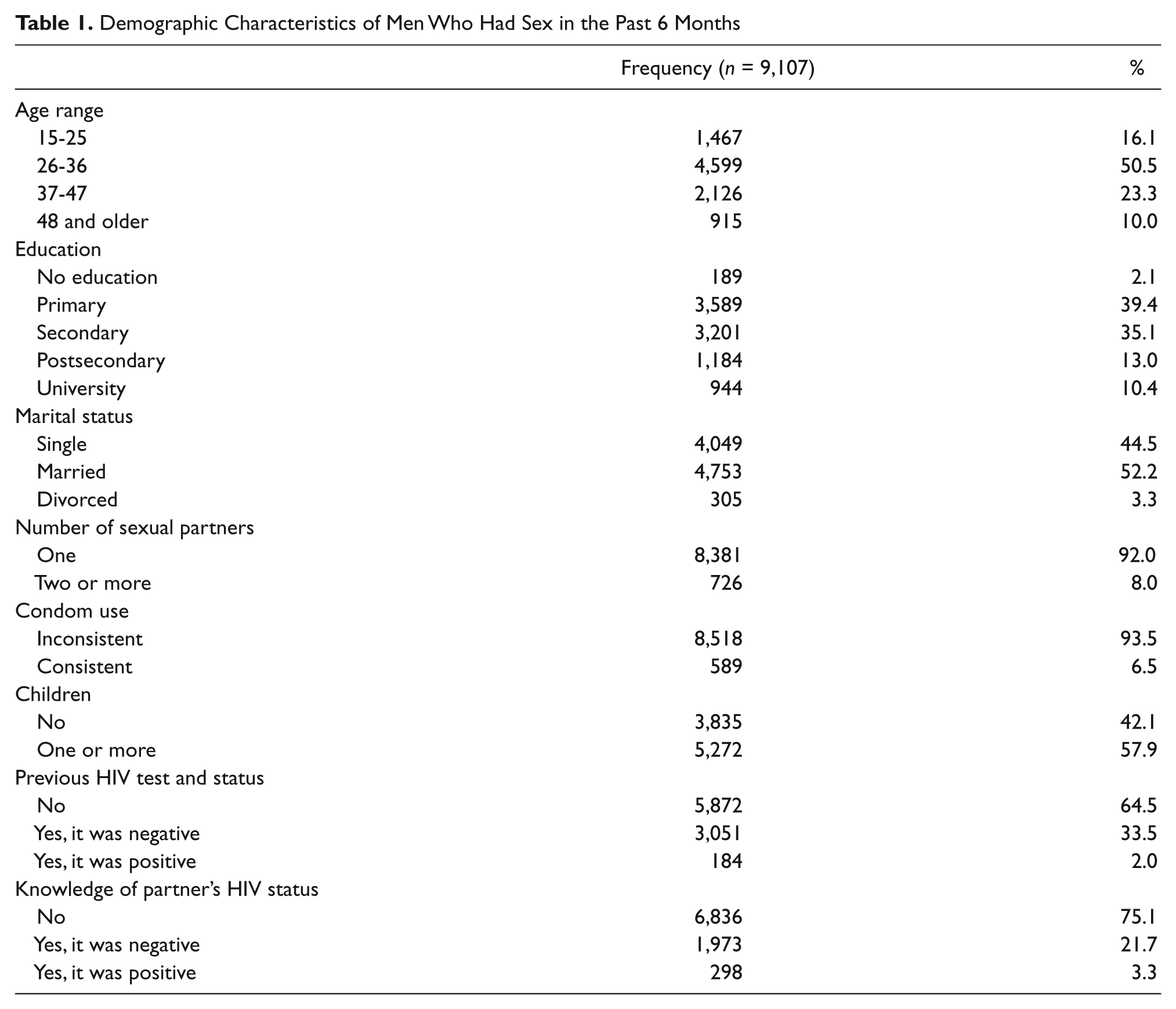
The sample consisted of 9,107 men with an average age of 34.3 years, and 3,201 (35%) of the men had a secondary education (Table 1). Approximately 4,700 (52%) reported being married and 5,272 (57.9%) had a child. Consistent condom use was low (n = 589; 6.5%), and 5,872 (64.5%) of the men had not previously been tested before visiting the clinic. Among those who had been tested, 3,051 (33.5%) reported they were HIV negative and 184 (2%) were HIV positive. Similarly, three quarters (n = 6,836; 75.1%) of the men were unaware of their partner’s HIV status, and 1,973 (21.7%) had an HIV-negative partner whereas 298 (3.3%) had an HIV-positive partner.
Demographic Characteristics of Men Who Had Sex in the Past 6 Months
As reported in Table 2, men in older age categories were significantly more likely to have been tested than the men in the 15- to 25-year-old category (χ2 = 85.8, p < .001). A previous HIV test was positively associated with education, as it was lowest (n = 49; 25.9%) among men without any formal education and highest (n = 537; 56.9%) among university educated men (χ2 = 337.5, p < .001). Compared with men with one sexual partner, men with two or more sexual partners were significantly less likely to have been tested (χ2 = 22, p < .001). Differences by condom use were relatively large, with 323 (54.8%) consistent condom users reporting a previous HIV test compared with 2,912 (34.2%) inconsistent condom users (χ2 = 102.6, p < .001). The largest difference in HIV testing was between men who were aware (n = 1,447; 63.7%) and men who were unaware (n = 1,788; 26.2%) of their partner’s HIV status (χ2 = 1,050, p < .001).
Characteristics of Men Who Had Sex in the Past 6 Months by Previous HIV Test and Knowledge of Partner’s HIV Status

Note. Only men who had been tested for HIV and those who are aware of their partner’s HIV status are reported in this table.
p < .001.
Similarly, men in older age categories were more likely to be aware of their partner’s HIV status than men in the 15- to 25-year-old category (χ2 = 68.5, p < .001). As education increased, awareness of partner’s HIV status also increased (χ2 = 156.0, p < .001). Men with one sexual partner were significantly more likely (n = 2,166; 25.8%) to be aware of their partner’s HIV status than men with two or more sexual partners (n = 105; 14.5%; χ2 = 46.2, p < .001). Awareness of a partner’s HIV status was more common among consistent condom users (n = 197; 33.4%) than inconsistent condom users (n = 2,074; 24.3%; χ2 = 24.4, p < .001) and men with children (n = 1,425; 27%) than men without children (n = 846; 22.1%; χ2 = 29.3, p < .001). The proportion of men who were aware of their partner’s HIV status was significantly higher (n = 1,447; 44.7%) among men who reported a history of HIV testing than men who had not been tested (n = 824; 14%; χ2 = 1050, p < .001).
Multivariate logistic regression model indicated that men in the 26 to 36, 37 to 47, and 48 and older age categories were significantly more likely to have been tested compared with those younger than 26 years old: odds ratio (OR) = 1.58, 95% confidence interval (CI) = 1.37, 1.81; OR = 1.53, 95% CI = 1.31, 1.80; and OR = 1.80, 95% CI = 1.48, 2.17, respectively (Table 3). Men with a secondary, postsecondary, and university education were more likely to have been tested compared with men with no formal education: OR = 1.47, 95% CI = 1.04, 2.09; OR = 1.85, 95% CI = 1.28, 2.66; OR = 2.82, 95% CI = 1.95, 4.07, respectively. Consistent condom use and knowledge of partner’s HIV status were also significant predictors of HIV testing, with adjusted ORs of 2.12 (95% CI = 1.77, 2.55) and 4.53 (95% CI = 4.08, 5.03), respectively. Surprisingly, men with two or more sexual partners were no more likely to have been tested than men with one sexual partner.
Multiple Logistic Regression Analysis of HIV Test Prior to Visiting VCT Clinic (Lower and Upper 95% CI Limits)

Note. VCT = Voluntary Counseling and Testing; OR = odds ratio; CI = confidence interval.
p < .001.
The multivariate logistic regression model for knowledge of partner’s HIV status showed that the adjusted ORs were statistically significant for university-educated men (OR = 2.84, 95% CI = 1.81, 4.45) compared with men with no formal education and for married men (OR = 1.81, 95% CI = 1.55, 2.10) versus single men (Table 4). Men who had two or more sexual partners were significantly less likely (OR = 0.54, 95% CI = 0.43, 0.67) to be aware of their partner’s HIV status than men with one sexual partner. Consistent condom users had a greater likelihood (OR = 1.27, 95% CI = 1.04, 1.54) of being aware of their partner’s HIV status compared with inconsistent condom users. As expected, men who had been tested were far more likely (OR = 4.57, 95% CI = 4.12, 5.08) to be aware of their partner’s HIV status than men with no history of HIV testing.
Multiple Logistic Regression Analysis of Knowledge of Partner’s HIV Status (Lower and Upper 95% CI Limits)

Note. OR = odds ratio; CI = confidence interval.
p < .05. ***p < .001.
Discussion
To our knowledge, this is the first study to use data collected over 11 years to assess predictors of HIV testing and knowledge of partner’s HIV status among Tanzanian men. Overall, there was a low rate of previous HIV testing and 2% of the men reported being HIV positive before visiting the clinic. Only 35% of the men had been tested at least once prior to visiting the clinic. Our finding supports studies that have reported a relatively low rate of male VCT participation in other African countries (deGraft-Johnson, Paz-Soldan, Kasote, & Tsui, 2005). In one study conducted in a South African province, the authors examined HIV testing records in 282 VCT sites and identified that 72.7% of those tested for HIV from 1998 to 006 were females (Snow, Madalane, & Poulsen, 2010). Similarly, a study conducted among 780 men in Uganda revealed that only 23.3% of the men had completed the process of pretest counseling, HIV testing, posttest counseling, and receiving their HIV test results (Bwambale et al., 2008). The lower proportion of men who had been tested after nearly three decades of the HIV epidemic indicates the need for prevention efforts in Africa to aggressively target men.
Compared with younger men, older men were more likely to have been tested. The greater likelihood of older men to have been tested differs from previous studies (Gage & Ali, 2005; Kranzer et al., 2011). One explanation for young men being less likely to have been tested may be the fact that they are also less likely to know where to get tested (Tanzania HIV/AIDS and Malaria Indicator Survey, 2008). It can also be that older men have higher HIV-related knowledge and have had more time to get tested than younger men (Jean, Anglaret, Moh, Lert, & Dray-Spira, 2012). Previous HIV testing was also more common among men with an increasing level of education. Other studies have reported similar results in Bostwana and South Africa (Kalichman & Simbayi, 2003; Weiser et al., 2006). The higher rate of HIV testing among the most educated may be a result of their prolonged exposure to HIV prevention messages, which are more readily available in the school system than in the community (Hargreaves et al., 2008). Previous research indicates that more educated men are more likely to engage in risky sexual behavior (Kongnyuy, Wiysonge, Mbu, Nana, & Kouam, 2006). Therefore, the authors suggest the finding which reveals that more educated men are more likely to seek HIV testing may also be a result of their greater concern regarding the risk of HIV due to their sexual behavior. In addition, a person’s educational level can determine knowledge and interest in health issues and increase their access to health care and utilization of care, which in turn would influence the likelihood of having been tested for HIV (Bond, Lauby, & Batson, 2005). Education was also positively correlated with knowledge of partner’s HIV status. It is plausible that since men with more years of education are more likely to get tested, their partners are also more likely to seek VCT and disclose their HIV status.
Knowledge of partner’s HIV status among men can be influenced by an array of individual, relational, and environmental factors such as their attitudes toward HIV testing, decision making and communication patterns with their partners, and most importantly whether their partner has been tested (Maman et al., 2001). Many of the men in this study were not aware (75.1%) of their partner’s HIV status. The lack of awareness of partner’s HIV status reflects the possibility that a majority of the men’s partners may also be unaware of their own status because they have not been tested. It may also be the case that some of the women have been tested for HIV without informing the men. It was reported that in Dar es Salaam whereas men who participated in VCT had no fear disclosing their results, the situation was different for women, some of whom risked being abandoned or verbally and physically abused by their partner (Maman et al., 2001).
Our finding confirms the low rate (20% to 40%) of disclosure that was reported among 1,078 HIV-positive pregnant women who participated in a randomized controlled study in Dar es Salaam (Antelman et al., 2001). To increase knowledge of partner’s HIV status among men in Tanzania, prevention programs that provide VCT services need to provide women with adequate support that can assist them with the disclosure process and protect them from any violence that may ensue (Maman et al., 2002). Culturally sanctioned gender roles have been associated with sexual violence against women, reducing their ability to protect themselves from STI/HIV, and personal control over their use of health services (Carey et al., 2011; Dunkle et al., 2004; Kalichman et al., 2005; Peacock & Levack, 2004; Susser & Stein, 2000). VCT clinics should promote couples voluntary counseling and testing because it has been shown to be more cost-effective in helping couples learn about their and their partner’s HIV status with the assistance of a professional and lead to greater protected sexual intercourse when compared with individual HIV voluntary counseling and testing (Becker, Mlay, Schwandt, & Lyamuya, 2010; Coates, 2000; Desgrées-du-Loû & Orne-Gliemann, 2008; Sweat et al., 2000).
Finally, HIV testing and awareness of partner’s HIV status was more common among men who had consistently used a condom in the past 6 months. One possible explanation for this finding is that the counseling that went along with testing may have led to an increase in condom use and partner communication regarding HIV serostatus (Bentley et al., 1998). Alternatively, this finding may be related to a greater concern about health among those who have tested, which would motivate them to use condoms and learn about their partner’s HIV status. The increase in condom use among those who were aware of their partner’s HIV status support previous studies from Tanzania, Uganda, and South Africa, which reported that adults who used condoms were more likely to be aware of their partner’s HIV status than individuals who did not use condoms (Bunnell et al., 2008; Conserve et al., 2012; King et al., 2008; Olley, Seedat, Gxamza, Reuter, & Stein, 2005).
Contrary to what may be expected, men with two or more sexual partners were both less likely to have been tested and to be aware of their partners’ HIV status. Although only one of these findings was significant, it does indicate that men with the riskiest behaviors are least likely to seek VCT. Our results, however, are consistent with a recent study that reveals that although men with multiple sexual partners understand their behavior increases their likelihood of HIV infection, those who perceive themselves at high risk of HIV do not seek testing (Johnston et al., 2010). Men with multiple sexual partners may associate their behavior with risk taking, which is often endorsed as a characteristic of masculinity (Towsend et al., 2011, Shai, Jewkes, Nduna, & Dunkle, 2012).
The strengths of our study include the large sample size collected over a period of 11 years, inclusion of men residing in the region with the second highest HIV prevalence rate, and ability to compare VCT attendance among inconsistent condom users to consistent condom users and men aware of their partner’s HIV serostatus to those unaware. Considering the analysis only included men already seeking VCT services, the results of this study may not be generalizable to all men in Tanzania, as they may different from the men who seek VCT services. Data were collected only in Dar es Salaam and the intake form did not inquire about sexual orientation. VCT practices could vary if examined among men in other regions and those who have sex with men (Nyoni & Ross, 2012; Wringe et al., 2008). The use of client’s self-report for their previous HIV test history, knowledge of their partner’s HIV status, and the number of sexual partners may have led to social desirability and recall bias. An underreporting of VCT attendance may also have occurred due to item nonresponse. Although much research have been conducted to examine the effects of awareness of one’s own and partner’s HIV status on sexual behavior, fewer studies have investigated the concordance between individual’s perceived and actual partners’ HIV status (Brown et al., 2011; Niccolai, Farley, Ayoub, Magnus, & Kissinger, 2002; Witte, El-Bassel, Gilbert, Wu, & Chang, 2010). Future research should include males’ sexual partners and measurement of the accuracy of knowledge of partner’s HIV status, and sexual behaviors.
In conclusion, these findings suggest the need for the Tanzanian government as well as other African countries to ensure that the HIV/AIDS testing campaign increasingly direct their efforts toward men who are younger, less educated, and have multiple sexual partners. These efforts could not only increase the number of men who seek VCT but also encourage men to protect themselves and in turn reduce the number of new infections in Africa. In addition, increasing the number of men who uses VCT services is crucial in curbing the HIV epidemic in Tanzania because men are the heads of households and can influence whether their partner has access to HIV prevention and care resources (Bwambale et al., 2008).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received following financial support for the research, authorship, and/or publication of this article: This research was supported by the Minority Health and Health Disparities International Research Training Program of National Institute of Minority Health and Health Disparities # 5 T 37 TW00113-08 and National Institute of Mental Health-COR Grant # MH-16573.