
Abstract
Background:
Shifting demographics and shortages of care staff place increasing pressure on healthcare systems and highlight the need for sustainable informal care. Although informal care alleviates pressure on healthcare systems, it comes with significant burden, primarily for caregivers. Minimizing burden through adequate support systems is essential. This review maps the evidence landscape on (a) educational, (b) social/emotional, (c) practical, (d) financial, and (e) legal support interventions for informal caregivers.
Methods:
A scoping review of literature published between 2019 and 2025 and indexed in medline, Web of Science, and CINAHL. Screening was conducted in duplicate. Data extraction was conducted using elicit and quality checked manually. Synthesis followed a 4-step, iterative, and thematic approach.
Results:
About 2665 articles were screened and 67 included. The most common support types were educational (n = 63) and social or emotional (n = 45), often combined. Educational support improved caregivers’ knowledge, skills, preparedness, and self-efficacy, often linked to improved burden and quality of life. Social and emotional support was linked to lower isolation, anxiety, and depression while enhancing well-being, and emotional connections. Overall, studies reported improved caregiver burden, self-efficacy, preparedness, quality of life, as well as mental and physical health. Financial and legal interventions were marginally addressed. We identified (1) caregiver-related, (2) intervention-related, and (3) system-level barriers and facilitators.
Conclusions:
The literature primarily focuses on educational and social-emotional interventions with reported benefits across caregiver outcomes, including caregiver burden and overall well-being. Financial and legal support remain inadequately addressed despite broader evidence that financial burden is a key driver of caregiver burden.
Keywords
Background
Globally, shifting demographics and a growing prevalence of multi-morbid patients are placing increasing pressure on public health and healthcare systems. 1 At the same time, persistent shortages of qualified care staff further exacerbate these challenges and highlight the need for additional support structures, such as stronger informal care networks. 1 Informal care forms the backbone of global long-term care (LTC) and broadly refers to support provided to a relative, friend, or acquaintance without a formal contractual agreement. 2 A 2023 OECD report with data across 25 countries found that 1 in 8 individuals aged 50 and above receive informal care, while 1 in 12 reported providing informal care on a daily basis. 3 In the U.S alone, it is estimated that about 100 million adults provided informal care for a dependent relative, a 40 million increase from 2015. 4 Most informal care takes place at home, where caregivers deliver a wide range of care tasks as well as support with activities of daily living. 5
Although informal care alleviates pressure on healthcare systems, it comes with financial, physical, and mental health burden, primarily for caregivers. 6 Intense provision of informal care is associated with anxiety, depression, social isolation, reduction or loss of employment, early retirement, and reduced quality of life.3,7-9 Caregiver burden is shaped not only by the intensity and duration of care and the patient’s cognitive and functional state, but also by contextual factors such as social support networks, access to information, and societal embedding, which can significantly influence carers’ ability to better cope with these challenges.9,10 Caregivers often report the need for more professional/clinical guidance, better communication, as well as financial and other resources to help them navigate the complexity of daily care and healthcare systems.8,11,12 Addressing these needs through external support systems is more urgent than ever. Equally crucial is improving our understanding of how different support measures affect informal care, including patients and caregivers.
Externally provided informal care support refers to interventions, resources, and services provided by actors outside the immediate informal care context (e.g., NGOs, private agencies, public institutions, healthcare professionals) to assist informal caregivers and improve informal care. Support can be educational, such as training and skill development programs; social and emotional such as peer-support interventions; practical, such as assistance with daily care tasks; financial, such as payments, subsidies, and other economic benefits; as well as legal, such as legal assistance around rights and insurance issues. Understanding how different types of support are implemented and affect informal caregivers and their patients is key to fostering a more efficient, sustainable, and less burdensome informal care ecosystem. Therefore, this scoping review provides an up-to-date synthesis of the scientific literature on externally provided informal care support. We have focused on physical, educational, social/emotional, financial, and legal support.
Aims
Our scoping review aims to map the evidence landscape on supported informal care to provide a holistic understanding of how different support interventions are currently addressed in the scientific literature. Additionally, it aims to provide a broad understanding of how support interventions are implemented, what barriers and facilitators they face and how they impact informal caregiving. Overall, we aim to inform best practices, further research, shape policy discussions, and ultimately contribute to a more equitable and sustainable caregiving system.
Methods
We conducted a scoping review of published randomized controlled trials (RCTs), quasi-experiments, as well as cohort-, case-control-, and qualitative studies.
Scoping reviews are particularly suited to examine and map the breadth, scope, and nature of literature, especially if large and heterogenous.13,14 In contrast to systematic reviews and meta-analyses, scoping reviews are less focused on assessing intervention effectiveness and study quality and more focused on the iterative mapping and summarizing of findings and research gaps.13,14 Our methodology was guided by Arksey and O’Malley’s framework, as well as Levac, Colquhoun, and O’Brien’s conceptual extensions, emphasizing a systematic and thorough study selection, an iterative yet transparent data charting, as well as thematic synthesis and reporting 13,14 A protocol was registered prospectively. 15
Search Strategy, Selection Criteria, and Screening
A search strategy was designed and tailored to 3 electronic databases: Medline, Web of Science, and CINAHL. We used multiple term variations (and synonyms) of the following search terms: informal care, family care, physical support, education, training, emotional support, social support, community support, peer support, financial assistance, and legal counseling. Our full search strategy (Medline) is provided in Supplemental File 1. All eligibility criteria are provided in Textbox 1. Interventions addressing purely digital support were excluded as we addressed those in a separate scoping review.
Inclusion criteria.
Screening was conducted in duplicate across 2 stages. First, 2 reviewers (EM, AB) screened titles and abstracts in duplicate. Second, all potentially eligible studies were screened by both reviewers in full text. Those studies not meeting all the above criteria (Textbox 1) were excluded. Any disagreements were resolved by a third reviewer (VN). All screening stages were conducted in Rayyan. 16
Data Extraction
Data extraction was conducted with Elicit based on a pre-defined data extraction sheet, developed by the study team. 17 For each data extraction item, we drafted a detailed prompt which was entered into Elicits automatic data extraction tool (https://elicit.com/). Prompts were carefully formulated to extract data accurately and keep redundancies low. They were initially tested in a sample of 10 studies and then corrected and adjusted. This process was conducted iteratively until the accuracy and consistency of extracted data was satisfactory. Extractions were manually quality-checked by 1 reviewer (AB). The data extraction sheet and corresponding Elicit prompts are provided Supplemental File 2.
Data Synthesis and Reporting
We synthesized data following a 4-step qualitative and iterative thematic approach, conducted by 1 reviewer (VN) and quality-checked by a second reviewer (EM). 14 First, we familiarized ourselves with the data and generated initial themes. Second, we mapped and clustered themes, generating conceptual maps that provided an overall picture of our findings. Third, outlier findings were noted and highlighted separately. Fourth, findings were synthesized and reported. Our reporting was guided by the Preferred Reporting Items Extension for Scoping Reviews (PRISMA-ScR) statement. 18
Results
We identified and screened the titles and abstracts of 2665 articles. We excluded 2469 studies and screened 196 in full text. Finally, 67 studies fulfilled all eligibility criteria and were included in our analysis. Informal care was primarily provided at home (n = 48, 72%), followed by care in a clinical/institutional setting (n = 19, 28%; e.g., outpatient clinics, care homes) and community-based care settings. The PRISMA flow chart (Figure 1) shows all screening stages in detail.
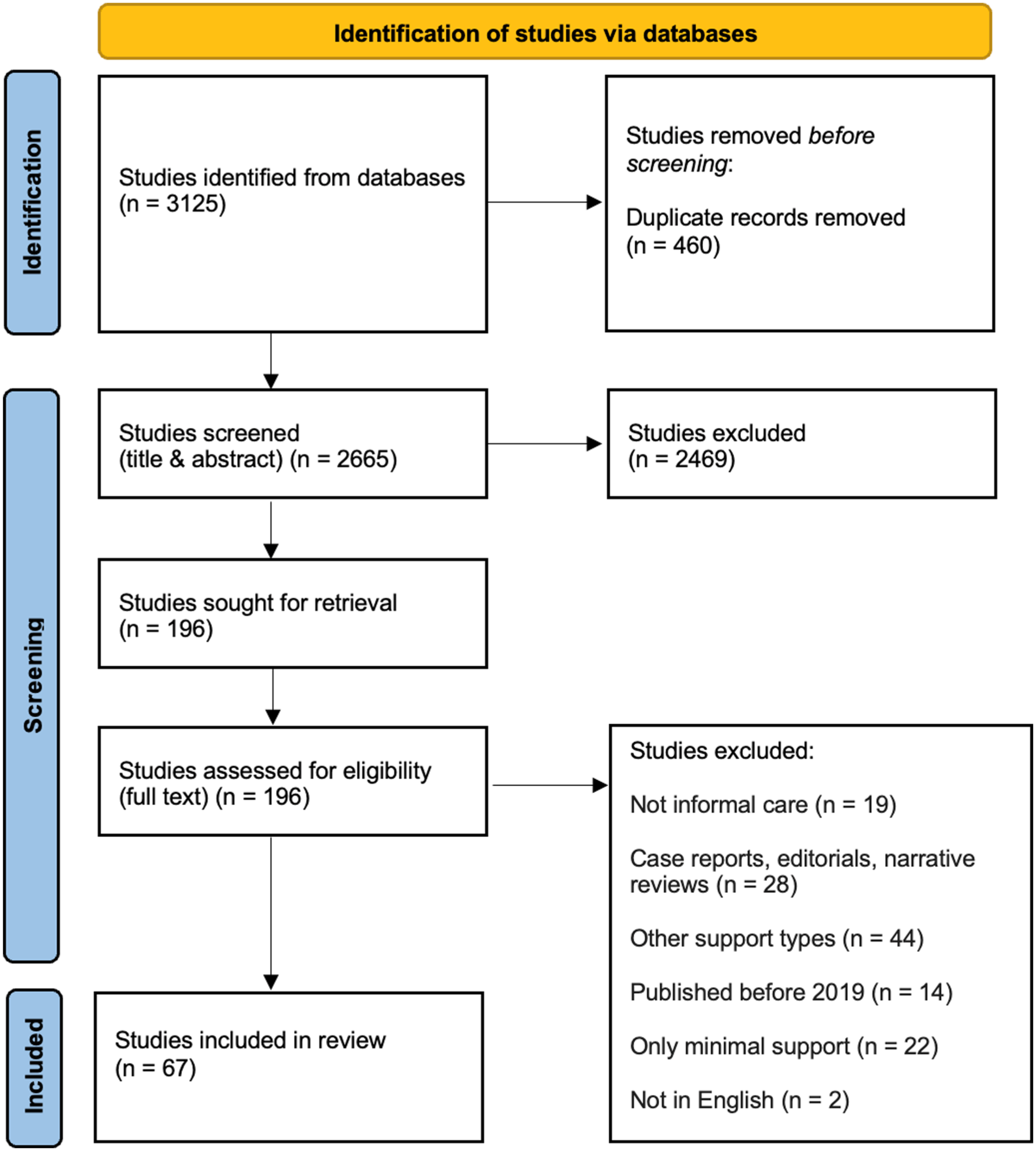
Prisma flow chart. 18
Scope and Aims of Literature
The number of publications on support interventions for informal caregivers has been gradually increasing over the last 6 years. We identified 3 eligible studies in 2019, six in 2020, 12 in 2021, 14 in 2022 and 2023, 16 in 2024, and 2 in early 2025. Most studies were conducted in Asia (n = 29, 43%), followed by North and Central America (n = 17, 25%), Europe (n = 14, 21%), Oceania (n = 3, 5%), Africa (n = 2, 3%), and South America (n = 2, 3%). Most identified studies were RCTs (n = 25, 37%), followed by quasi-experimental methodologies (n = 23, 34%), mixed method designs (n = 14, 21%), and then qualitative (n = 3, 5%) and observational methodologies (n = 2, 3%). Most studies were primarily targeted toward informal caregivers (n = 44, 65%), followed by studies including caregiver and patient participants (n = 20, 30%) and studies primarily focusing on patients receiving informal care (n = 3, 5%).
Most of the studies aimed to assess the effects of external support on caregiver skills, such as communication and interaction skills, as well as their overall self-efficacy to provide informal care (n = 22, 33%), followed by studies that specifically and directly targeted a reduction in caregiver burden (n = 20, 30%). A significant (n = 14, 21%) proportion of literature looked at feasibility, acceptability and cultural relevance of various support types for informal caregivers. Eleven studies (16%) looked at the effects of support on the mental health of caregivers (e.g., stress, anxiety, depression), followed by studies that targeted overall quality of life and well-being (n = 10, 15%). Five studies (8%) aimed at improving caregiver lifestyles (e.g., increase in physical activity and other healthy choices) and providing financial stability respectively. Finally, 1 study (2%) assessed caregiver willingness to pay for support that reduces burden, and 1 study (2%) evaluated the cost-effectiveness of caregiver support. Support was delivered for a duration from 2 weeks up to 13 months, with 17 studies (25%) ranging between 2 and 5 months and 16 (24%) studies going beyond 5 months.
Participant Characteristics and Care Context
Most informal caregivers were spouses/partners (n = 43, 64%) or first-degree relatives (n = 30, 45%) of the patients they were caring for, followed by second degree relatives (n = 6, 9%). The focus of most studies was on middle-aged caregivers (n = 32, 48%), followed by older (n = 12, 18%) and mostly younger age groups (n = 4, 6%). In most studies, caregivers were predominantly female (n = 40, 60%), followed by balanced samples (n = 10, 15%) and 2 studies (3%) with mostly male caregivers. The employment status of caregivers was not widely reported. Among those studies (n = 51) reporting employment (n = 29, 52%), most included relatively balanced samples of both employed and unemployed caregivers (n = 16, 28%), followed mostly by unemployed (n = 6, 11%) and mostly by employed (n = 5, 9%) samples. Care was most often provided for patients with mental/cognitive conditions (n = 26, 39%) such as dementia and Alzheimer, followed by multiple chronic conditions (n = 13, 19%), cancer (n = 5, 7%), neuromuscular conditions (n = 5, 7%), cardiovascular diseases (n = 5, 7%), pulmonary conditions (n = 4, 6%), obesity (n = 3, 5%), chronic kidney disease (n = 3, 5%), and other physical disabilities (n = 3, 5%).
Types of Caregiver Support
The most common caregiver support types were educational support (n = 63, 94%) and social and emotional support (n = 45, 67%), in most studies combined. Practical support was mentioned in 12 studies (18%) and financial support in 8 studies (12%). Legal assistance was marginally mentioned in 1 study (2%). Table 1 provides all support delivery methods. Supplemental File 3 provides all included studies categorized by support types.
Caregiver Support Types and Delivery Methods.
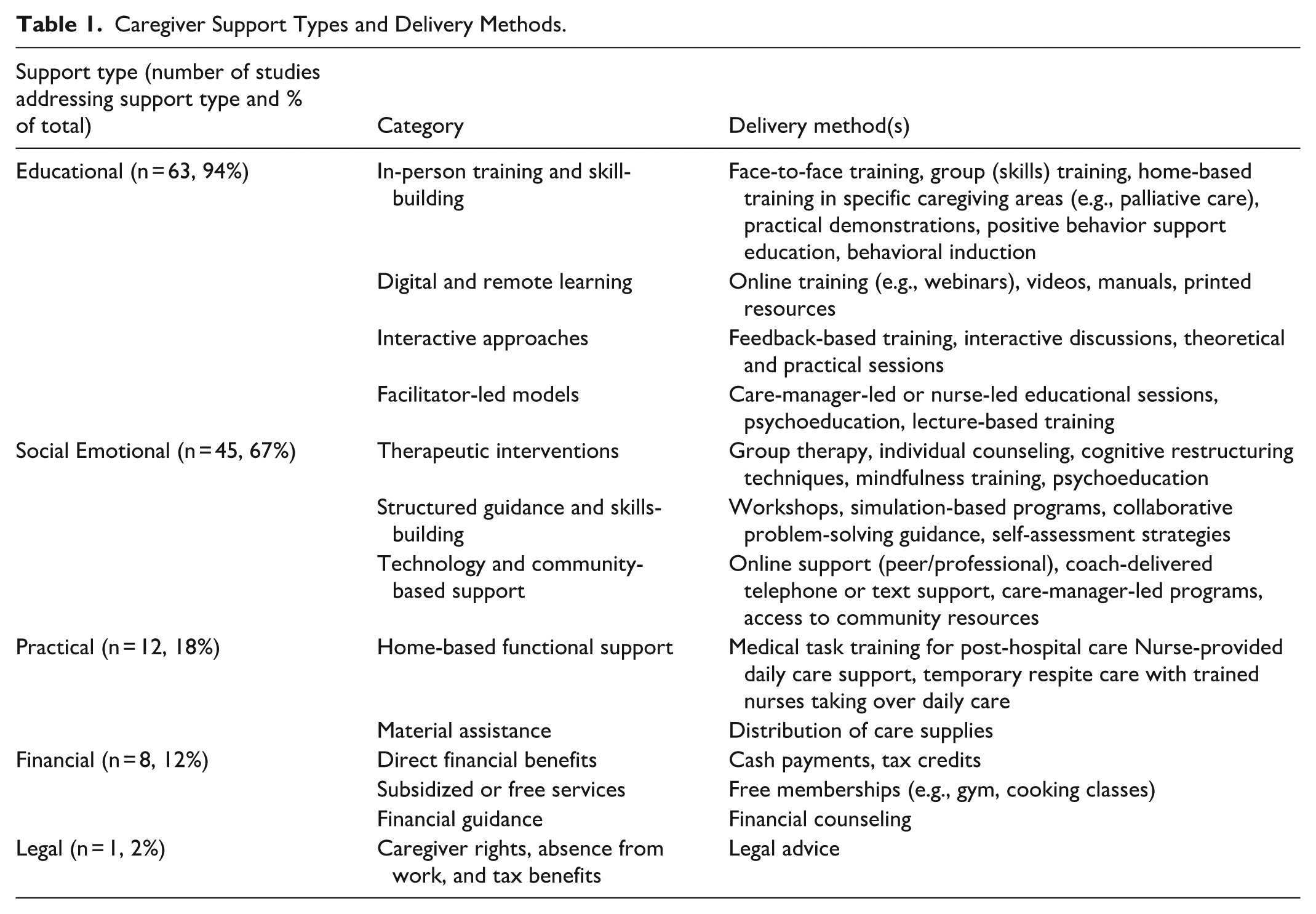
Educational support primarily targeted transferrable (e.g., problem-solving and management skills during crises, communication skills) and care-specific caregiver skills (e.g., caregiving techniques, care strategies and care coordination, and rehabilitation skills) to reduce caregiver burden.19-21 Health literacy was at the core of educational support, including knowledge on health behaviors (e.g., nutrition, physical activity), how to manage and prevent various conditions, health system navigation skills, and medication management skills. Other educational support components included helping caregivers gain knowledge on how to access resources, seek for support and managing financial decisions.
Social and emotional support primarily targeted the emotional resilience and well-being of caregivers such as through coping strategies, relaxation stress management techniques as well as activities that promote self-awareness, self-esteem, resilience, emotional adjustment and engagement, self-compassion, empowerment, and motivation.22-24 Many support interventions also targeted the reduction of psychological outcomes such as exhaustion, depersonalization, fear, and perceived burden. They also aimed to fostering social and peer connection to reduce isolation, increase empathy and build hope.
Practical support primarily included strategies to support physical functioning at home and practical help with daily care activities, often led by nurses and regular in-home visits.25,26 One study looked at relieving caregiver burden by giving them a few days off and instead letting nurses take over care. Other interventions provided medical task training for post-hospital care as well as the distribution of care supplies.
Financial support was marginally addressed and included benefits that help facilitate healthy behaviors (e.g., free gym memberships), financial counseling, cash payments for provided care activities and other benefits such as Medicaid waivers and tax credits.27,28 Findings show that there are large differences in the availability and adequacy of financial support measures. Legal support was less commonly addressed but included provisions such as caregiver rights to absence from work and tax benefits. 29
Outcomes Measured and Main Findings
Six outcomes were most frequently reported. Caregiver burden, including physical, mental, social, and financial burden, as well as caregiver self-efficacy, including preparedness, and skills were the 2 most common outcomes, reported in 27 studies (40%) each. Quality of life domains for caregivers and patients were addressed in 18 studies (27%), followed by overall psychological well-being, stress, and emotional exhaustion (n = 16, 24%), outcomes related to depression and anxiety (n = 15, 22%), as well physical functioning and health, including strength, function, and activity levels (n = 15, 22%). Other commonly reported outcomes were quality of care, including the relationship and communication between informal caregivers and patients (n = 8, 12%), costs (n = 6, 9%), as well caregiver coping skills and resilience (n = 4, 6%). Table 2 summarizes the main findings across the 6 most reported outcomes. Patient reported outcomes were reported in 27% of studies (n = 18). Supplemental File 4 provides all included studies categorized by the most common outcomes.
Main Findings Across 6 Most Common Outcomes.
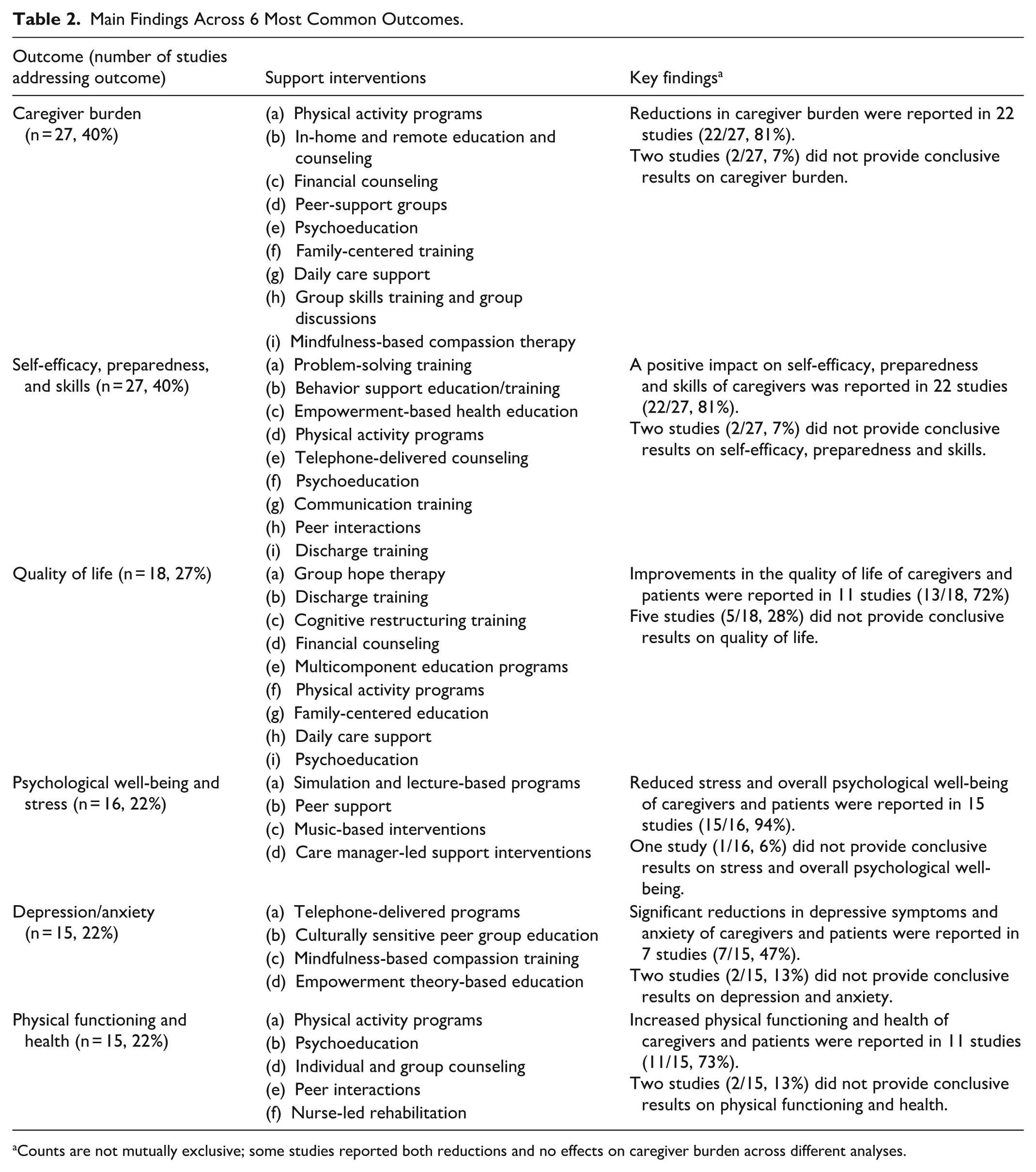
Counts are not mutually exclusive; some studies reported both reductions and no effects on caregiver burden across different analyses.
Main Findings by Type of Support
In 22 studies (33%), educational support improved caregivers’ knowledge, skills preparedness, and self-efficacy which was often linked to reduced caregiver burden and enhanced quality of life. Various educational approaches such as face-to-face training sessions, remote (e.g., online, telephone) counseling, online toolkits (e.g., webinars), psychoeducation, and other multi-component tailored programs often showed effectiveness in mitigating caregiving challenges, improving communication, coping strategies, as well as caregiving techniques across different conditions including dementia, cancer, stroke, and other chronic illnesses. In 21 studies (31%) social and emotional support interventions were linked to lower caregiver isolation, distress, anxiety, and depression while enhancing overall psychological well-being, hope, and emotional connections. Social and emotional support was often (n = 45, 67%) combined with educational components and to improve caregivers’ mood, coping styles, and social connectedness, contributing to better caregiving experiences
In 18 studies (27%) that included practical support, such as for activities of daily living and care, respite care, rehabilitation of patients, and physical activity, improved caregivers’ physical function, reduced their burden, and often provided temporary relief, which in turn contributed to improved quality of life and overall care quality. Practical support was often (n = 16, 24%) integrated with educational and social/emotional components for holistic caregiver assistance. Financial support was provided indirectly (e.g., free gym memberships) or directly (e.g., caregiver payments). Although public policies for financial aid exist, they are often insufficient as well as incompatible with actual caregiver needs. Reimbursing informal caregivers can mitigate workforce shortages and reduce caregiver burden, yet comprehensive, needs-based and well-integrated financial support systems still lack. Financial assistance was noted as a critical complement to other support types to sustain caregiving. Findings on legal support were not found, highlighting a need for more research on legal protections and support frameworks for informal caregivers.
Who’s Often Excluded from Studies?
The most common reasons for caregiver exclusion in the included studies were mental illnesses and cognitive disabilities (n = 13, 19%), as well as past or current chronic or life-limiting conditions/disabilities (n = 13, 19%), and communication and language deficits or barriers (n = 12, 18%). Being too young (e.g., below 21) or underage was also reported frequently (n = 11, 16%) as exclusion reason. Caregivers with no family relationship to their patients and/or not living with them were also frequently excluded (n = 7, 10%), as well as non-primary caregivers (n = 5, 8%). Finally, paid informal caregivers (n = 3, 5%), with low literacy levels (n = 3, 5%) and no or unreliable access to telephone, email or computer (n = 3, 5%) were also mentioned as exclusion reasons.
Barriers and Facilitators of Caregiver Support
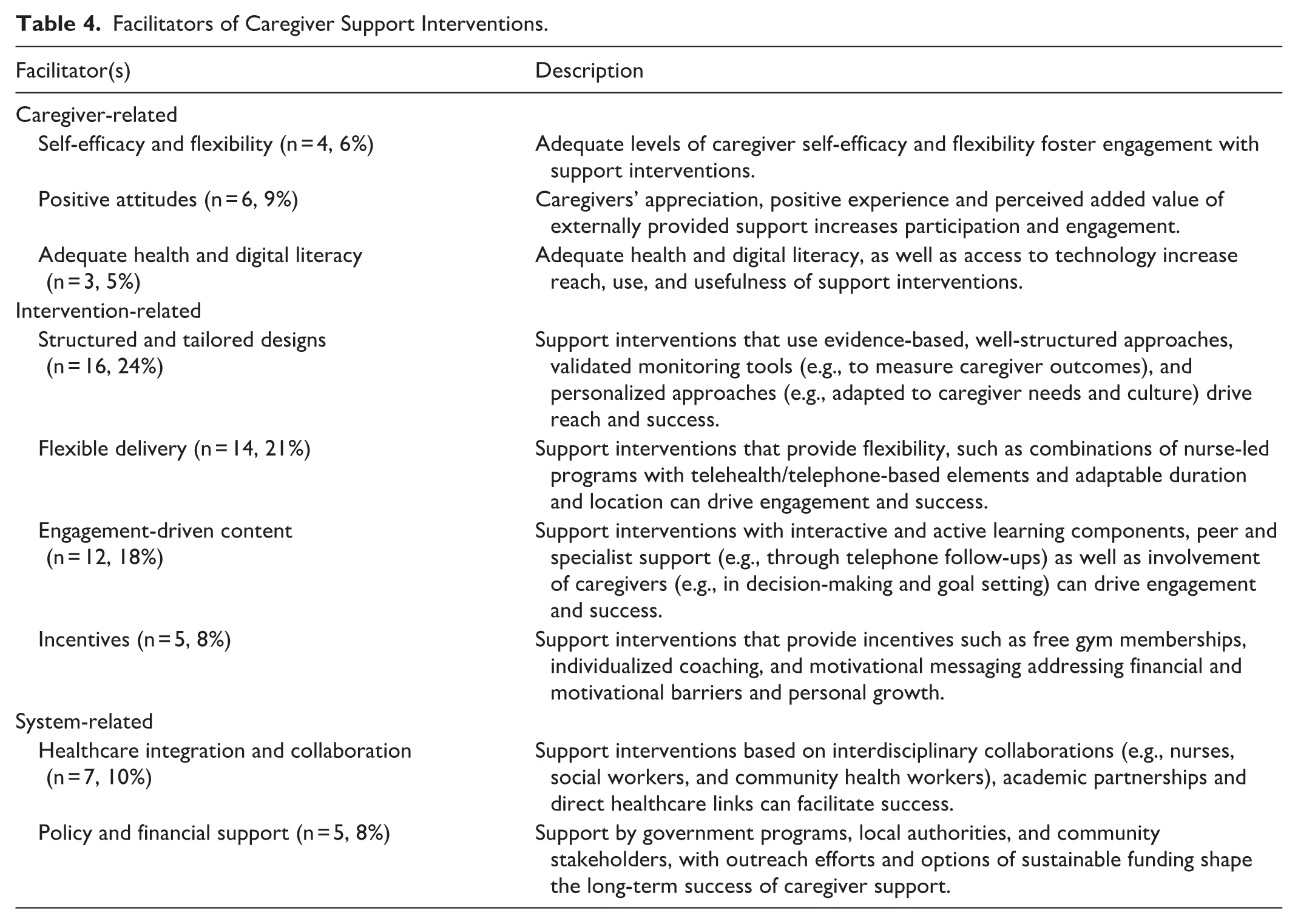
All studies mentioned at least 1 barrier (challenge) or facilitator. We categorized barriers and facilitators of informal caregiver support into 3 overarching themes: (1) caregiver-related barriers/facilitators, (2) intervention-related barriers/facilitators, and (3) system-level barriers/facilitators. Tables 3 and 4 provide a detailed summary of reported barriers and facilitators. Supplemental File 5 provides studies categorized by barriers and facilitators.
Barriers of Caregiver Support Interventions.

Facilitators of Caregiver Support Interventions.
Existing Evidence Gaps
Finally, we extracted reported evidence gaps and future developments. The following 4 themes emerged: (1) Need for robust evidence on how support interventions work, (2) need for stronger personalization and adaptability of support, (3) need for holistic and collaborative approaches, and (4) need for stronger emphasis on the financial support of informal caregivers. First, studies underlined the need for robust evidence on how support interventions work.30,31 Studies reported that this requires larger-scale and multi-center studies across caregiver groups, diseases and cultural contexts, with an emphasis on long-term and sustained effects.24,32,33 Needs-based research that explores cultural, ethnic, gender, and regional differences in caregiver burden, experiences and preferences should be prioritized.34-36 Second, studies reported that future caregiver-support interventions should be personalized adaptable to remote, online or hybrid delivery, to reach harder-to-reach caregiver subgroups (e.g., rural residents) and ensure a better fit into daily caregiving schedules.37,38
Third, some authors highlighted that future support should be holistic and ensure that those involved (e.g., nurses, healthcare providers) are well-trained and equally supported. That will require measure to address workforce shortages, standardized training curricula, stronger partnerships between healthcare organizations and community networks, and the incorporation of caregiver support into larger care models.19,39 Fourth, a stronger focus on the financial support of caregivers is required. That requires better assessment of financial strains of informal caregivers, such as how caregiving impacts income and career development. Build on economic analyses, future support should be backed up by innovative policies that will enable financial aid and reimbursement. That includes more streams of financial support directly directed to caregivers, better access to community resources and solutions that mitigate the impact of informal caregiving on employment and career.37,40-42
Discussion
Our findings reveal a substantial and growing body of evidence that highlights the potential positive impact of various support measures tailored toward informal caregivers, while simultaneously highlighting critical gaps and implementation challenges that must be addressed to optimize informal care caregiver support systems.
Combining Education with Social and Emotional Support
The literature suggests that educational interventions, addressed in almost all of the studies included in this review, are one of the most frequently used caregiver support measures. This finding reflects previous research which suggests that knowledge deficits, including low health literacy, constitute a fundamental barrier to effective caregiving. 43 Multiple studies reported that educational interventions improved key outcomes such as caregiver preparedness (e.g., to provide care under stress or emergencies), disease-specific knowledge, and care-related skills across diverse patient populations, from dementia care to complex medical conditions requiring technical skills. Previous reviews have reported educational effects on caregiver burden, patient outcomes, and quality of life.44,45 Education was commonly combined with social and emotional support interventions, with reported positive effects on caregiver psychological well-being, burden, anxiety, depression, and isolation. This is aligned with previous literature which suggests that education and psychological support can significantly reduce caregiver burden, coping skills, self-efficacy, and quality of life.46,47
The Neglected Role of Financial Support
Financial support interventions, while only marginally addressed, were described as essential for caregiver well-being and system sustainability. The lack of financial resources for (a) informal caregivers, (b) and support interventions were commonly reported barriers of intervention accessibility, interventions success as well as overall informal care delivery. Previous research has shown that financial difficulties not only increased stress and limited access to support services but also created “double burdens” where caregivers faced simultaneous financial and caregiving responsibilities.48,49 The limited representation of financial support interventions in our review likely reflects the complex policy landscape surrounding caregiver compensation as well as how social insurance systems are designed, rather than lack of need for financial support. While in some countries, such as Switzerland, Germany, Sweden, France, Austria, the Netherlands, and the USA there has been considerable movements toward direct informal caregiver payments, in others, financial support remains scarce. 50 This fragmented approach creates substantial inequities in caregiver support across geographic regions. Previous research suggests that the financial needs of informal caregivers and their patients often remain unmet. 51 Our findings suggest that the provision of financial incentives such as free gym memberships and individualized coaching can mitigate some financial barriers and help support caregiver well-being, however, are most likely not enough to meet the full financial needs of informal caregivers.
Emphasis on “Home”
As expected, most identified caregiver support interventions were tailored to context of home care, reflecting both the reality that most informal care occurs within domestic settings as well as the economic imperative driving this trend. 52 This emphasis on home has important implications for the design of caregiver support intervention, as it must account for the complex dynamics of family relationships, variable home environments, and conflicting private responsibilities. The focus on home-based care reflects broader healthcare policy trends toward community-based care models. 53 While receiving care at home is often framed in terms of patient preference and quality of life, the economic drivers are equally compelling. Home-based care, supported by informal caregivers, represents the most cost-effective approach to LTC delivery, with institutional care costs typically significantly higher. 54 This economic reality makes support for informal caregivers not merely beneficial but essential for healthcare system sustainability. From a home health care management perspective, our findings highlight the importance of integrating informal care and routine home-based care services, including communication and coordination with healthcare professionals (e.g., nurses, home care agencies, and other community-based providers.
Culturally Sensitive Caregiver Support
The international scope of included studies, spanning diverse cultural contexts from Turkey to Australia to Iran, reveals both universal caregiver support needs and culture-specific adaptation requirements. The lack of culturally sensitive support interventions, which includes language barriers and lack of content and resources that align with caregiver norms, values, and beliefs, were reported as important barriers to caregiver support. Ensuring that an intervention is culturally sensitive is not an easy task and comes with challenges and uncertainties, however, can be essential to enabling support access for vulnerable caregiver groups (e.g., elderly, ethnic minorities).55,56 The lack of cultural sensitivity is related to another common barrier, that of negative perceptions of caregivers toward support interventions and services. 57 That includes beliefs that support is irrelevant, time-consuming, or emotionally/practically difficult. Previous research has shown that caregivers with ethnic minority backgrounds are more likely to reject external support if that is not aligned with cultural values.57,58 Culturally adapted interventions have also been associated with higher satisfaction rates among caregivers who perceive them as more valuable and helpful, as well as with reduced caregiver burden and improved patient outcomes.59,60
Limitations and Methodological Considerations
This review has several limitations that should be considered when interpreting its findings. Our inclusion criteria, while comprehensive, may have excluded relevant studies published before 2019 or in languages other than English. The scoping review methodology, while appropriate for mapping the breadth of available evidence, does not permit formal quality assessment or meta-analysis of outcomes. Additionally, publication bias may have influenced our findings, particularly regarding financial interventions where policy-sensitive research may be less likely to reach publication. The predominance of studies from high-income countries may limit generalizability to low-resource settings where caregiver support needs may be most acute but financing mechanisms most constrained. We conducted data extraction with an AI tool (Elicit) which improves efficiency yet may introduce some limitations regarding data accuracy and consistency, as algorithms can misinterpret context and miss more nuanced data elements. We minimized these limitations by manually reviewing AI-extracted data.
Conclusion
Our review suggests that the scientific literature on informal caregiver support is emerging with many support interventions reporting positive impact across caregiver outcomes, including well-being, burden, resilience, and capacity. Educational and social-emotional interventions are currently the most frequently addressed support measures, with reported benefits across diverse caregiver populations and caregiving contexts. Practical support interventions were less commonly addressed yet also reported positive findings. Financial and legal interventions were only marginally addressed despite broader evidence that financial burden is a key driver of caregiver burden. This suggests that the financial and legal support needs of informal caregivers remain inadequately addressed in scientific literature. Our findings also underscore multiple caregiver-related, intervention-related and system-related barriers, including health literacy gaps, the lack of culturally sensitive interventions, as well as the insufficient funding and resources. Future research should prioritize comprehensive economic evaluations, a stronger focus on financial support, a better inclusion of vulnerable and currently underrepresented caregiver populations, while maintaining focus on rigorous evaluations as well as personalized, adaptable, and culturally sensitive caregiver support.
Supplemental Material
sj-docx-1-hhc-10.1177_10848223261428104 – Supplemental material for Supporting the Supporters. A Systematic Scoping Review of Support Interventions for Informal Caregivers
Supplemental material, sj-docx-1-hhc-10.1177_10848223261428104 for Supporting the Supporters. A Systematic Scoping Review of Support Interventions for Informal Caregivers by Vasileios Nittas, Emilie Melkestian, Alexia Bikou, Andreas Hellmann, Anja Frei, Viktor von Wyl and Milo A. Puhan in Home Health Care Management & Practice
Supplemental Material
sj-docx-2-hhc-10.1177_10848223261428104 – Supplemental material for Supporting the Supporters. A Systematic Scoping Review of Support Interventions for Informal Caregivers
Supplemental material, sj-docx-2-hhc-10.1177_10848223261428104 for Supporting the Supporters. A Systematic Scoping Review of Support Interventions for Informal Caregivers by Vasileios Nittas, Emilie Melkestian, Alexia Bikou, Andreas Hellmann, Anja Frei, Viktor von Wyl and Milo A. Puhan in Home Health Care Management & Practice
Supplemental Material
sj-docx-3-hhc-10.1177_10848223261428104 – Supplemental material for Supporting the Supporters. A Systematic Scoping Review of Support Interventions for Informal Caregivers
Supplemental material, sj-docx-3-hhc-10.1177_10848223261428104 for Supporting the Supporters. A Systematic Scoping Review of Support Interventions for Informal Caregivers by Vasileios Nittas, Emilie Melkestian, Alexia Bikou, Andreas Hellmann, Anja Frei, Viktor von Wyl and Milo A. Puhan in Home Health Care Management & Practice
Supplemental Material
sj-docx-4-hhc-10.1177_10848223261428104 – Supplemental material for Supporting the Supporters. A Systematic Scoping Review of Support Interventions for Informal Caregivers
Supplemental material, sj-docx-4-hhc-10.1177_10848223261428104 for Supporting the Supporters. A Systematic Scoping Review of Support Interventions for Informal Caregivers by Vasileios Nittas, Emilie Melkestian, Alexia Bikou, Andreas Hellmann, Anja Frei, Viktor von Wyl and Milo A. Puhan in Home Health Care Management & Practice
Supplemental Material
sj-docx-5-hhc-10.1177_10848223261428104 – Supplemental material for Supporting the Supporters. A Systematic Scoping Review of Support Interventions for Informal Caregivers
Supplemental material, sj-docx-5-hhc-10.1177_10848223261428104 for Supporting the Supporters. A Systematic Scoping Review of Support Interventions for Informal Caregivers by Vasileios Nittas, Emilie Melkestian, Alexia Bikou, Andreas Hellmann, Anja Frei, Viktor von Wyl and Milo A. Puhan in Home Health Care Management & Practice
Footnotes
Acknowledgements
Not applicable.
Ethical Considerations
This article does not contain any studies with human or animal participants.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Author Contributions
VN, MAP, AH and EM conceptualized the study. VN, EM, and AB conducted all screening stages. VN and EM wrote the manuscript. MAP, AF, AH, VvW and AB reviewed and edited the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially supported by Pflegewegweiser GmbH. The funder had no involvement in the design, data collection or publication of this manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Only publicly available data from previously published studies was used for this scoping review.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.