
Abstract
African American men are disproportionately affected by prostate cancer. This project adopted a community-based participatory approach to design and pilot test an educational outreach strategy that promotes informed decision making about screening among African American men in community settings in St. Louis, Missouri. Interviews with local subject matter experts informed the design of the strategy. The revised curriculum was pilot tested in 2009 with 63 men who completed pre- and posttest surveys that measured knowledge, norms, beliefs, decision self-efficacy, and screening intention. The intervention resulted in statistically significant improvement in prostate cancer knowledge, decreased perceived risks and barriers, and increased screening decision self-efficacy. The educational outreach strategy offered in community settings was effective in improving knowledge, beliefs, and decision self-efficacy related to prostate cancer screening. This project sought to devise a screening outreach strategy that struck a balance between the imperatives of informed decision-making goals and the pragmatics of community settings. The findings suggest the need for further research to assess the effectiveness of community-based outreach efforts in enhancing engagement of men in decision making related to screening, diagnostics, and treatment.
Introduction
Prostate cancer (PCa) is the most frequent cancer and the second leading cause of cancer deaths in men—estimated to be 32,050 in 2010 (American Cancer Society, 2010). Racial disparities are larger for PCa than for any other cancer site: incidence is 60% higher among African American than White men. Although mortality due to PCa has been declining among both African American and White men since the early 1990s, it remains more than two times greater among African Americans than Whites (American Cancer Society, 2009).
Multiple explanations for disparities include environmental, genetic, behavioral, and clinical factors. Unequal exposure to environmental contaminants (Olden & White, 2005) and genetic factors (Zeigler-Johnson et al., 2008) has been linked to PCa disparities. Earlier research among African American men has reported low levels of knowledge about PCa (A. Jones, Shipp, Thompson, & Davis, 2005). African American men are less likely to be screened for PCa than White men and, when diagnosed with PCa, are more likely to have advanced disease (B. Jones et al., 2008). Prior research in St. Louis has identified that many African American men are underserved with limited access to health care and educational outreach programs (Wray et al., 2009). Recent research has encountered a nearly fivefold risk of late-stage diagnosis for underserved men compared with national data (19% compared with 4%). D. Miller et al. (2009) conclude that “our findings suggest that for low income, uninsured men, under-detection and under-treatment remain significant concerns” (p. 582). The combined effects of low knowledge, advanced-stage diagnosis, and high rates of death underscore the need to target African Americans and other underserved groups for PCa prevention efforts (B. Jones et al., 2008).
No proven means for primary prevention of PCa currently exist. Screening in the form of the prostate-specific antigen (PSA) blood test and the digital rectal exam (DRE) are the primary available means of secondary prevention. PCa screening is contentious as there is no clear evidence that it decreases mortality. Preliminary results from two randomized trials, in the United States and Europe, released in 2009 offer a confounding picture. The U.S. study found no association of PCa-related mortality with PSA or DRE screening (Andriole et al., 2009). The European study reported that PSA screening reduced mortality from PCa by 20% but was associated with a high risk of overdiagnosis (Schroder et al., 2009).
The 5-year survival rate for cancer local to the prostate (early stage) is 100%; with metastatic disease the survival rate drops to 31% (American Cancer Society, 2007). Screening clearly results in greater percentages of men diagnosed with early-stage disease. This logic has proven persuasive to patients and physicians alike as PCa screening is common: in 2004, 50.0% of African American men older than 50 years were screened. Professional ambivalence about the recommendations is reflected by even higher screening rates (95%) among urologists older than 50 years (Barry, 2009).
Past research on PCa outreach programs has reported potential for recruiting substantial numbers of men for screening (Abernethy et al., 2005). Studies have assessed a variety of educational tools including brochures, pamphlets, and videos that have been disseminated and proven effective in increasing knowledge and awareness (Hewitson & Austoker, 2005; Partin et al., 2004). Several studies have explored informed decision making (IDM) for PCa screening (Flood et al., 1996; Frosch, Kaplan, & Felitti, 2001; Volk, Cass, & Spann, 1999). Lower screening rates have resulted among men in the IDM study arms, compared with those in the screening promotion arms, possibly an indication of success of the decision-making intervention, given a greater emphasis on screening risks and independent decisions (Volk et al., 1999). Recent research has shifted the focus in intervention outcomes from knowledge and found that interventions can increase decision self-efficacy and reduce decisional conflict (Drake, Shelton, Gilligan, & Allen, 2010; Evans et al., 2010).
The ambiguous scientific evidence of the efficacy of PCa screening has compelled most major medical organizations to recommend that patients make an informed decision about screening after weighing the risks and benefits in consultation with their physicians. The U.S. Preventive Services Task Force defines an informed decision as one where an individual has (a) knowledge about risks, benefits, and limitations of screening; (b) ability to participate in decision making at a personally desired level (decision self-efficacy), and (c) made a decision that is consistent with personal preferences and values (U.S. Preventive Services Task Force, 2008).
However, community organizations are reluctant to promote IDM, arguing that straightforward screening promotion is more likely to reach audiences and contribute to cancer prevention and control. Recent reviews of the literature on IDM have called for research on how to integrate promotion of PCa decision making into community education programs (in contrast to clinical settings). Briss and colleagues identified a need for further research and conceptualization of the decision-making process among diverse groups given that cultural influences shape how individuals make decisions as well as the value of the potential outcomes of these decisions (Briss et al., 2004). The community context poses unique challenges that call for refinement of the IDM approach. In this study, a community-based participatory design approach (Neuhauser, Rothschild, Graham, Ivey, & Konishi, 2009) was used to develop and pilot test a communication strategy that promotes IDM for PCa screening among African American men. The research team sought to devise a strategy to enhance IDM about PCa screening appropriate for community-based organizations engaged in outreach.
In addition to IDM, two theoretical frameworks informed the research: the social ecological model and the integrative model of behavior. Applying the social ecological model (Stokols, 1996) the study team assessed discussions and findings through a lens that envisions how institutional structures provide the context for outreach programs, how social structures and norms provide the make-up of neighborhoods and communities, and how individual beliefs and intentions independently and interactively shape individual decisions and actions. The IDM assessment instrument was designed in terms of the integrative model of behavior (Fishbein, 2009). The study assessed the extent to which the intervention enhanced PCa knowledge; beliefs about screening benefits, risks, and barriers; subjective norms; decision self-efficacy; and screening intention.
Method
The methods are divided into two parts. The first section describes the development of the PCa outreach education curriculum and the second discusses the pilot test.
Curriculum Development
The outreach curriculum was informed by community input in three ways: (1) consultation with six content experts and health educators, (2) review of draft materials by experts, and (3) pretest with members of the intended audience—African American men older than 40 years. The curriculum was designed based on an initial consultative process and refined after the review and pretesting stages. The development team had extensive experience designing culturally appropriate and health literate materials for African American audiences.
Study Design
Formative interviews were carried out with six content experts: three clinicians (radiologist, surgeon, and urological nurse) and three PCa survivors with experience providing PCa education in community settings; five of the six were African Americans. The interview guide elicited their insights on the following dimensions: preferred outline of presentation, visual aids, communicating IDM strategies, and outreach settings.
Based on the findings from the formative research, a PowerPoint presentation was developed to be presented by PCa survivors as well as health care and public health professionals.
After the development of the presentation, the content experts again reviewed the materials. Clinicians reviewed the materials to ensure all clinical information was correct, whereas survivors reviewed the materials for cultural appropriateness and ease of understanding.
This draft curriculum was pretested using small group interviews with a convenience sample of 13 African American men who had never been diagnosed with cancer in two community settings. The men participating in the pretest were asked about the main messages of the materials, understanding of and emotional response to materials, as well as likes and dislikes. The study team recorded and analyzed audience feedback and formulated changes that were provided to the graphic design team.
Findings
Content experts recommended the following topical sequence: shape, location, and function of the prostate gland; PCa prevalence, risk factors, symptoms, and disparities; screening options; benefits of early detection; and treatment options and side effects. Other recommendations included using plain language, visuals, and graphics; allowing time for a question and answer session; and conducting outreach in community settings such as churches.
Both clinicians and survivors highlighted IDM as a strategy empowering African American men to make their own choice with regard to their health. Clinicians emphasized that the curriculum should clearly address screening risks and benefits, including false positives, independent screening decision, and PCa treatment. In contrast, survivors emphasized the importance of encouraging men to discuss important health problems among themselves and with their wives.
Formatted as a PowerPoint presentation with notes for the speaker, the initial draft curriculum was revised based on content experts’ reviews. A flip chart version was designed for use in small group settings where a computer and projector were unavailable. Adopting a tagline offered by a survivor educator colleague, the presentation was titled: “Prostate Cancer: What’s Your Number?” Responding to the typically brief opportunity for presentations in many community settings, the presentation was shortened to 15 minutes or less. Reviewers concurred that the presentation should focus on screening rather than treatment and recommended providing less detailed information about symptoms, treatment options, and side effects in the slides than originally suggested (leaving these topics for question and answer sessions). With regard to IDM guidelines, the content experts agreed the presentation should convey screening risks, benefits and limitations, and decision-making self-efficacy. They noted that group presentations in community settings may not always allow for individual consultation with providers as recommended by IDM guidelines. Instead, they noted that the pressing message was to encourage screening and emphasize talking to the doctor in the event of a positive result requiring further diagnostic work and possibly treatment. Thus, the team revised the IDM component of the curriculum consistent with the reviewers’ recommended bottom line: “Get screened. If you get a positive result, talk to your doctor.”
In the pretesting phase, participants indicated understanding of major presentation themes: PCa disparities, importance of early detection, the need for both PSA and DRE, and the need to undergo diagnostic tests if the screening tests were positive. Participants indicated that the amount of information was just right and that images, content, and duration of the presentation were deemed appropriate. The participants offered minor recommendations for revision. For instance, they recommended adding a line stating that PCa can affect all men as some participants did not like the feeling of being singled out as African Americans. The outline of the presentation is presented in Table 1.
Curriculum Outline
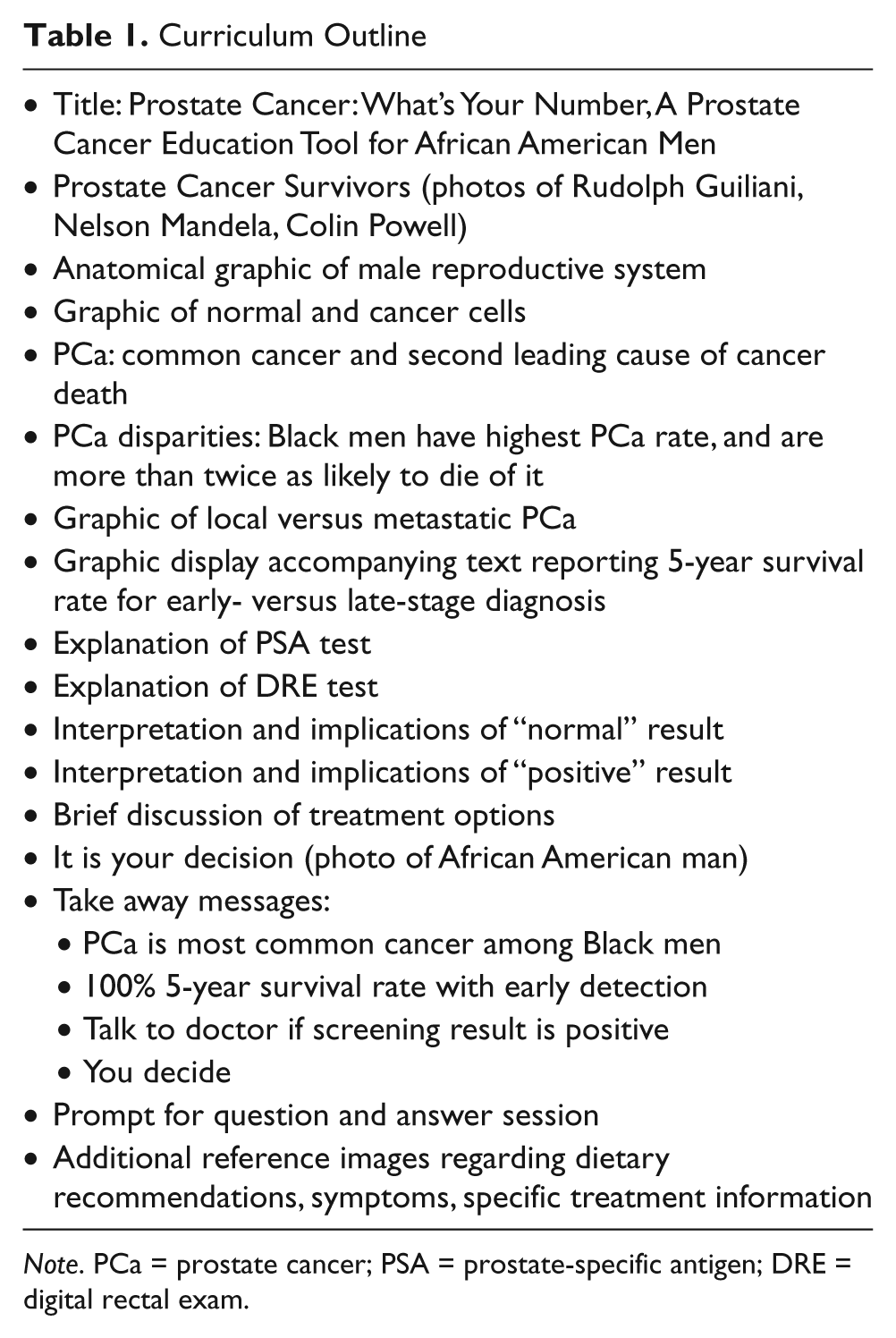
Note. PCa = prostate cancer; PSA = prostate-specific antigen; DRE = digital rectal exam.
Pilot Test
The pilot test used a single group design with pre- and posttest measurement of criterion outcomes. Data were collected with convenience samples of men recruited by community partners from January to May 2009. These men signed an informed consent form, completed a pretest, observed the educational presentation, and then completed the posttest questionnaire. Participants were given a $10.00 gift card as a participation incentive. The Saint Louis University Institutional Review Board approved the study.
The educational presentation was provided by health educators or survivor peer educators who presented the final 15-minute version of the curriculum through a flipchart or a PowerPoint slideshow, both with the same content, depending on the setting. These presentations were made in community centers, workplaces, churches, or health fairs.
Sampling Recruitment
Inclusion criteria for the study called for English-speaking African American men 40 years of age or older. Recruitment methods depended on the setting. In some instances, such as during churches’ health ministry meetings, community collaborators and two research assistants from the study team invited attendees to participate. In other settings, such as health fairs, research assistants approached and recruited individuals attending the fairs.
Measurement
Prior to the presentation, participants completed a pretest questionnaire with the following measures. Demographic characteristics included age, income, education, employment, health insurance, and family history. Outcome measures asked on both the pre- and posttests included PCa knowledge, subjective norms, behavioral beliefs (screening benefits and risks and barriers), decision-making self-efficacy, and screening intention. Measures on PCa knowledge were based on Radosevich et al.’s (2004) 10-item knowledge index. Decision-making self-efficacy questions were adapted from Holmes-Rovner et al.’s (1996) Satisfaction with Decisions Scale. Other measures were designed to match the specific content of the outreach curriculum. Belief items were scored on a 5-point Likert-type scale with 1 being Strongly disagree and 5 being Strongly agree. Specific items for each construct are presented later in the text.
Analysis
Descriptive statistics using frequencies and corresponding percentages were conducted to examine sample characteristics and distribution. T tests were used to examine differences in pre- and posttest results for individual items and aggregated scales for all outcome variables. Reliability of scales was measured using Cronbach’s α: knowledge (α = .78), subjective norms (α = .79), behavioral beliefs—benefits (α = .81), behavioral beliefs—risks and barriers (α = .81), and decision self-efficacy (α = .62). For analysis the pre–post knowledge items were recoded into incorrect and don’t know as 0 and correct as 1, and we conducted paired samples t tests for all items. The t tests allowed us to examine differences in overall scores for each knowledge item from pre to post. All analyses were conducted using SPSS Version 16.
Findings
The sample comprised a total of 63 participants, two thirds of whom were between 40 and 60 years (the recommendation to not screen men older than 70 years was released during the study period). Almost half of the participants were high school graduates, and one third had completed college. More than half were married. Two thirds of the participants were employed, though little more than half reported having employee-covered health insurance. The sample comprised almost an equal number of participants who had or had not previously received information about PCa. One in four of the participants reported a family history of prostate cancer (see Table 2).
Demographic Description of Participants in the Prostate Cancer Education Sessions (N = 63)

Note. PCa = prostate cancer.
The analysis of aggregated scores (presented in Table 3) shows that knowledge overall increased at a statistically significant level (p < .01). Subjective norms and beliefs about screening benefits remained constant among participants. A statistically significant decrease was noted in perceived barriers and a statistically significant increase in decision-making self-efficacy. Minimal increases were noted for both items capturing intention to screen.
Overall Mean Differences in Knowledge, Beliefs, and Intention to Screen

The correlation and t cannot be computed because the standard error of the difference is 0.
p ≤ .05.
Among knowledge items, the analysis showed a consistent reduction in the “Don’t Know” response and a consistent increase in correct responses to all seven items. At the same time, the analysis also shows marginal increases in incorrect responses for two questions (see Table 4).
Responses to Knowledge Items Among Study Participants Before and After the Education Session

Note. T = true; F = false; PSA = prostate-specific antigen.
p ≤ .05.
The paired t test analysis examines the differences in mean scores for individual knowledge items for participants before and after the intervention. Means increased for all seven items. Although the differences for the first two were not statistically significant, the differences for the remaining five were: the possible need for a biopsy if screen results are positive, the uncertain ability of PSA to detect cancer, the function of the prostate, the greater certainty of diagnosis with biopsy, and the disparity of PCa between African Americans and Caucasians.
Participants’ responses to subjective norm and behavioral beliefs—benefit items moved in the intended direction after the intervention but were not statistically significant (Table 5). Three of the four items measuring beliefs pertaining to screening risks and barriers moved in the intended direction after the intervention at a statistically significant level: the perceived barrier of cost, screening availability during work hours, and the uncertain utility of the PSA test. Two of four decision self-efficacy items displayed a statistically significant increase in the expected direction: sufficient information about PCa and confidence in making an informed decision about getting screened for PCa.
Prostate Cancer Screening Beliefs Among Study Participants Before and After the Education Session

Note. PSA = prostate-specific antigen.
p ≤ .05.
Discussion
This study examined the effects of a community-based PCa outreach strategy grounded in an effort to negotiate an IDM approach in community settings. In doing so, community perspectives on PCa screening and treatment information were incorporated into a communication strategy that empowers African American men with the knowledge to make informed decisions about PCa screening.
Overall, the study reports encouraging findings from using such an approach. The pre–post analyses show increases in PCa knowledge, decisional self-efficacy, and a decrease in barriers to screening. No changes in perceived subjective norms and perceived benefits of screening were noted.
Specific to knowledge, a consistent decline in “I Don’t Know” responses across the seven questions suggests that the outreach presentation was successful in enhancing men’s knowledge and reducing uncertainty. Increases in correct responses to five of seven questions highlight the potential for educational interventions to raise PCa knowledge among African American men, consistent with other research in the area (Drake et al., 2010; Evans et al., 2010). At the same time, parallel increases in incorrect responses to two questions highlight the potential hazards of outreach education to overstate the benefits of the PSA test (though it is of interest to note that the perceived benefits scale did not shift in this study).
The decrease in perceived risks and barriers indicates that educators effectively shared information that addressed concerns about the logistics and costs of getting screened. The increase in decisional self-efficacy—related to using information to make screening decisions—suggests the potential of community outreach programs to disseminate information and enhance IDM outcomes. Intention to screen was universally high among participants and left little room for further increase.
The null result for subjective norms is not surprising as the educational curriculum did not seek to shift these perceptions. In addition, the convenience sample, made up of men with the initiative to attend a PCa screening education event, may already have had high subjective norms and perceived benefits for screening, making them less amenable to change.
Study characteristics impose limits on the study. The convenience sample recruited for this pilot study introduces a potential selectivity bias and impedes the generalizeability of the study findings. The pre- and posttest design of the study goes part of the way in addressing this concern however (Valente, 2002). The small sample size limited the analytical power of the study. Measurement methods also introduce potential social desirability bias and test–retest bias as the pre- and posttests took place in one sitting.
The curriculum assessment sheds light on theoretical questions. The curriculum was successful in affecting the most critical constructs identified by theory. IDM requires attention to knowledge and decision self-efficacy; both of these were enhanced by exposure to the curriculum. Consistent with the integrative model of behavior, study findings also indicate that an emphasis on beliefs and self-efficacy is appropriate and feasible; the results do not assess association of the constructs with intention however.
As posited by the social ecological model, the study also highlights the importance of organizational and community contexts in considering efforts such as these. The study provides an opportunity to reexamine strategies to enhance PCa screening decision making through community-based outreach education. The notion of IDM emerged from the clinical setting, in the context of treatment decisions and informed consent for clinical trials (Briss et al., 2004). In the case of cancer clinical trial participants, research has highlighted important limits in understanding of risks, benefits, and study procedures after consent was obtained, among participants and physicians alike (Joffe, Cook, Cleary, Clark, & Weeks, 2001). The community setting imposes limits to the IDM elements formulated by professional associations in their recommendations regarding PCa screening. For example, community outreach efforts often do not provide a clinician with whom participants can consult. In addition, IDM interventions emphasize individual choice. For example, decision-aids focus on risks and benefits of screening and treatment options and help individual users align their values and preferences to different possible outcomes. Outreach efforts reach groups and do not facilitate the same level of individual work.
General IDM recommendations are confounded for groups at higher risk (i.e., African American men and men with a family history of PCa). Results of screening efficacy trials are even more uncertain when it comes to African American men about whom PCa disparities are little understood (A. Miller, 1992). These circumstances heighten the urgency to establish sound educational methods for use with high-risk groups.
Community partners and expert collaborators encouraged the study team to shift the emphasis and content of the IDM educational strategy. They recommended deemphasizing the discussion of PCa treatment, based on the argument that the presentation is about screening rather than treatment. In this way, the presentation emphasizes short-term screening risks (e.g., sore arm, false positives, and emotional upset) rather than risks of treatment and values aligned with different treatment options. The curriculum encourages individual choice and communication with providers, family, and survivors.
This shift acknowledges the circumstances and priorities of community organizations, including getting access to hard-to-reach, underserved, and uninsured men. This shift also recognizes that screening is just the first possible step in a suite of decisions. Research shows that many men receive a PSA test as part of their routine annual, and without an informed decision, clearly a less than optimal outcome (Allen et al., 2010). Informed decision or not, given a positive result, consultation with a physician is imperative, and a more difficult set of decisions is invoked, regarding biopsy and diagnosis first, and subsequent treatment options, should a cancer diagnosis be reached. A decision about treatment occurs in the physician’s office, if and when treatment is under consideration, when information may be provided about options, side effects, and prognosis, and values may be aligned with alternatives. The curriculum introduced here seeks to ensure that community-based screening initiatives are accompanied by educational efforts that successfully enhance knowledge about PCa and decision self-efficacy. Framing informed decision as empowerment and independent choice, the curriculum encourages men to engage with their physicians in the set of decisions related to PCa.
IDM theory poses an ideal type that encumbers community organizations engaged in PCa outreach more than it helps them. Prior research has shown that community organizations routinely ignore the IDM requirement (Wray et al., 2009). This project sought to strike a balance between the requirements of the prescribed IDM model and PCa screening guidelines and the realities in which community-based organizations work. This is not to suggest that the ambiguous efficacy of screening be ignored. Rather, seeking to balance the very real risks of both overtreatment and undertreatment, especially for men at high risk, the curriculum incorporates communication about screening in a realistic way that community organizations can use and recognizes that the much more difficult decision about treatment, should it be necessary, occurs in the setting where an informed decision is most essential and more plausible—the physician’s office. This conclusion is reached in full understanding of the variable and imperfect quality of shared decision making for PCa treatment as well and the need to continue research to improve treatment decision making. On the screening side, further research can explore how screening decision making can inform and enhance treatment decision making that leads to effective treatment choices, less decisional regret, and enhanced survivorship.
Subsequent to the completion of this study, the community partners have adopted the curriculum for use by survivor educators in their outreach efforts. Anecdotally they report the curriculum has contributed to heightened awareness and enhanced conversation about prostate health in the community. In addition, they have observed that men who have sought PCa screening as a result of their outreach have gone on to seek other preventive health care, such as hypertension screening. In this way, PCa outreach efforts may have the additional benefit of encouraging men who may otherwise avoid seeking preventive care to be more comfortable with the idea of entering the health care system and engaging with providers.
Footnotes
Acknowledgements
The authors are indebted to the six experts who contributed to the content and direction of the educational curriculum. We are grateful to our colleagues at the Prostate Cancer Community Partnership of PECaD as well as community partners who facilitated development and assessment of the curriculum. Finally, we appreciate the men in the community who willingly participated in the study pretest and the pilot test of the curriculum.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded through a supplemental grant from the National Cancer Institute to the Program to Eliminate Cancer Disparities (PECaD), Siteman Cancer Institute, Washington University in St. Louis (#5 U01 CA114594-03).