
Abstract
The study aimed to determine the effects of a 4-month Tai Chi intervention on tenderness, functional capacity, symptomatology, and quality of life in men with fibromyalgia. The effect of a 3-month detraining period was also analyzed. Six men with fibromyalgia (age 52.3 ± 9.3 years) followed a 4-month Tai Chi intervention. The outcome variables were tenderness, functional capacity (30-second chair stand, handgrip strength, chair sit and reach, back scratch, blind flamingo, 8 feet up and go, and 6-minute walk tests), and self-administered questionnaires. A significant improvement (p = .028) after the intervention period for the chair sit and reach test was found, such improvement was maintained after the detraining phase. Tenderness, symptomatology, and quality of life did not significantly change after the intervention period or the detraining phase. In summary, a 4-month Tai Chi intervention improved lower body flexibility in men with fibromyalgia. This improvement persisted after the detraining period.
There is growing evidence that exercise plays a key role in the management of fibromyalgia (Goldenberg, Burckhardt, & Crofford, 2004; Jones, Adams, Winters-Stone, & Burckhardt, 2006; Mannerkorpi & Henriksson, 2007; Maquet, Demoulin, Croisier, & Crielaard, 2007). Fibromyalgia is characterized by the concurrent existence of chronic, widespread musculoskeletal pain, and multiple sites of tenderness (Wolfe et al., 1990). Core symptoms include debilitating fatigue, sleep disturbance, joint stiffness, and memory or cognitive difficulties (Bennett, Jones, Turk, Russell, & Matallana, 2007; Wilson, Robinson, & Turk, 2009; Wolfe et al., 1990), and patients may experience conditions such as anxiety and depression (Bennett et al., 2007; Wilson et al., 2009). Because of these circumstances, exercise interventions in these patients are of low impact and low intensity in nature to avoid any side effect.
Tai Chi, an ancient Chinese form of exercise, is a low-speed and low-impact exercise (Lan, Lai, & Chen, 2002). Tai Chi is a “balanced” exercise that integrates key components of exercise training, cardiorespiratory function, strength, balance, and flexibility (Lan et al., 2002; Taylor-Piliae & Froelicher, 2004). Furthermore, Tai Chi integrates the movements with deep breathing and incorporates elements of relaxation and mental concentration (Taggart, Arslanian, Bae, & Singh, 2003). Therefore, Tai Chi exercises combined aspect of mind–body therapy and physical exercise (Taggart et al., 2003).
Overall, Tai Chi seems to have physiologic and psychosocial benefits and appears to be safe and effective in promoting balance control, flexibility, and cardiovascular fitness for patients with chronic conditions (Hall, Maher, Latimer, & Ferreira, 2009; Klein & Adams, 2004; Wang, Collet, & Lau, 2004). Therefore, it is potentially beneficial to fibromyalgia patients but further research is needed to support the evidence-based practice (Taggart et al., 2003).
Descriptive data as well as exercise intervention studies in men with fibromyalgia are lacking (Jones et al., 2006; Mannerkorpi & Henriksson, 2007), mainly because fibromyalgia is more common in women (~4.2%) than in men (~0.2%; Mas, Carmona, Valverde, & Ribas, 2008). However, men with fibromyalgia report more severe symptoms than women, decreased physical function, and lower quality of life (Buskila, Neumann, Alhoashle, & Abu-Shakra, 2000; Ruiz Perez et al., 2007).
To our knowledge, only one study examined the effect of exercise training in two male patients (Karper, 2007). Whether Tai Chi intervention influences tenderness, functional capacity, symptomatology, and quality of life in men with fibromyalgia is unknown. A recent randomized controlled trial (Wang et al., 2010) analyzed the effect of 12 weeks of Tai Chi intervention and 12 weeks of detraining period in fibromyalgia patients (85% female), but they did not report the results for male sample.
The purpose of the present study was to determine the effects of 4-month Tai Chi intervention on tenderness, functional capacity, symptomatology, and quality of life in men with fibromyalgia. The effect of a 3-month detraining period on these parameters was analyzed. Since exercise has positive effects in patients with fibromyalgia, and Tai Chi has physiologic and psychosocial benefits in patients with chronic conditions, it was hypothesized that a Tai Chi intervention has overall positive effects on health in men with fibromyalgia.
Materials and Method
Study Participants
A total of 27 Spanish male members from a local association of fibromyalgia patients were contacted. Nine potentially eligible patients responded and gave their written informed consent after receiving detailed information about the aims and study procedures. The inclusion criteria were (a) meeting the American College of Rheumatology criteria—widespread pain for more than 3 months and pain with 4 kg/cm of pressure for 11 or more of 18 tender points (Wolfe et al., 1990); (b) not having other severe somatic or psychiatric disorders, such as stroke or schizophrenia, or other diseases that prevent physical loading; and (c) not attending another type of physical therapy at the same time. Three patients were not included in the study because they did not have 11 of the 18 tender points. Therefore, a total of 6 men with fibromyalgia (mean ± SD; age, 52.3 ±9.3 years; weight, 78.2 ± 5.4 kg; height, 171.1 ± 7.9 cm) participated in the study.
Study Design
Originally, the aim was to assess a control group of age- and gender-matched patients. However, it was not possible to recruit such a group as none of the other male patients contacted were willing to participate and did not give their permission to recruit information. Thus, though a control group would have strengthened the experimental design, for logistic reasons, this was not possible. Despite the lack of a “formal” control group, our study used a controlled design as each patient served as his own control to compare pretest, posttest at 4 months, and detraining results after 3 months.
All the tests were carried out on two separate days, with at least 48 hours between each session. This was done to prevent fatigue and flare-ups (acute exacerbation of symptoms). The assessment of the tender-points count, 30-second blind flamingo, and 30-second chair stand tests were completed on the first visit. Anthropometry, chair sit and reach, back scratch, 8 feet up and go, handgrip strength, and 6-minute walking tests were assessed on the second day. All patients were assessed by the same researcher group to reduce interexaminer error.
The research protocol was reviewed and approved by the Ethics Committee of the Hospital Virgen de las Nieves. The study was developed between September 2008 and September 2009, following the ethical guidelines of the Declaration of Helsinki, last modified in 2000.
Intervention
The Tai Chi intervention was based on the classical Yang Style. The characteristics of Yang Tai Chi are extended and natural postures, slow and even motions, light and steady movements, and curved, flowing lines of performance (Sports, 1983). Patients participated in three 60-minute Tai Chi sessions conducted weekly for 16 weeks. Each session included 15 minutes of warm up while stretching, mobility and breathing techniques, 30 minutes of Tai Chi exercise principles and techniques, and finally 15 minutes of various relaxation methods. The intervention consisted of eight forms from classic Yang Style Tai Chi, with minor modifications that were suitable for patients with fibromyalgia. For example, in the first month, some exercises were realized with the participants sitting to avoid too much fatigue.
A master Tai Chi instructor was present during the sessions to supervise the participants and also assist with movements/exercises. The first 2 weeks of the 16-week intervention focused on learning fundamental movement patterns. The participants then began learning the sequential movements of eight-Form, Yang Style Tai Chi for the following weeks. The instructor controlled the adherence daily by registering the patient’s attendance.
Outcome Measures
Tenderness
Tenderness was assessed by means of the measurement of the 18 tender points according to the American College of Rheumatology criteria for classification of fibromyalgia using a standard pressure algometer (EFFEGI, FPK 20, Italy; Wolfe et al., 1990). Tender point scored as positive when the patient noted pain at pressure of 4 kg/cm2 or less. The total count of such positive tender points was recorded for each participant. The algometer score was calculated as the sum of the minimum pain–pressure values obtained for each tender point (Altan, Bingol, Aykac, Koc, & Yurtkuran, 2004; Harden et al., 2007).
Functional capacity
Weight (kg) and height (cm) were measured using standard procedures, and body mass index (BMI) was calculated as weight (in kilograms) divided by height (in meters) squared.
Functional tests were part of the Functional Senior Fitness Test Battery (Rikli & Jones, 1999). The handgrip strength and the blind flamingo test were also assessed, because of the fact that these tests have been used in patients with fibromyalgia (Tomas-Carus et al., 2007).
Lower body muscular strength
The “30-second chair stand test” involves counting the number of times within 30 seconds that an individual can rise to a full stand from a seated position with back straight and feet flat on the floor, without pushing off with the arms. The patients carried out one trial after familiarization (Rikli & Jones, 1999).
Upper body muscular strength
“Handgrip strength” was measured using a digital dynamometer (TKK 5101 Grip-D; Takey, Tokyo, Japan) as described elsewhere (Ruiz-Ruiz, Mesa, Gutierrez, & Castillo, 2002). Patients performed (alternately with both hands) the test twice allowing a 1-minute rest period between measures. The best value of two trials for each hand was chosen and the average of both hands was registered.
Lower body flexibility
In the “chair sit and reach test,” the patient seated with one leg extended slowly bends forward sliding the hands down the extended leg in an attempt to touch (or past) the toes. The number of centimeters short of reaching the toe (minus score) or reaching beyond it (plus score) was recorded (Rikli & Jones, 1999). Two trials with each leg were measured and the best value of each leg was registered, being the average of both legs used in the analysis.
Upper body flexibility
The “back scratch test,” a measure of overall shoulder range of motion, involves measuring the distance between (or overlap of) the middle fingers behind the back (Rikli & Jones, 1999). This test was measured alternately with both hands twice and the best value was registered. The average of both hands was used in the analysis.
Static balance
It was assessed with the blind flamingo test, in which the patient (barefoot) stood on one leg while the other leg was flexed at knee level and held at the ankle by the hand of the same side of the body with eyes closed (Rodriguez et al., 1998). The number of trials needed to complete 30 seconds of the static position is recorded, and the chronometer is stopped whenever the patient did not comply with the protocol conditions. One trial was accomplished for each leg and the average of both values was selected for the analysis.
Motor agility/dynamic balance
The “8 feet up and go test” involves standing up from a chair, walking 8 feet to and around a cone, and returning to the chair in the shortest possible time (Rikli & Jones, 1999). The best time of two trials was recorded and used in the analysis.
Aerobic endurance
It was assessed by means of the “6-minute walk test.”.This test involves determining the maximum distance (meters) that can be walked in 6 minutes along a 45.7 meters rectangular course (King et al., 1999; Mannerkorpi, Svantesson, Carlsson, & Ekdahl, 1999; Pankoff, Overend, Lucy, & White, 2000; Rikli & Jones, 1999).
Self-Administered Questionnaires
Fibromyalgia Impact Questionnaire (FIQ) was used to assess the fibromyalgia-related symptoms. It is a self-administered questionnaire designed to assess the components of health status that are believed to be most affected by fibromyalgia and has been validated for Spanish population with fibromyalgia (Rivera & Gonzalez, 2004). This questionnaire is composed of three subscales rated on Likert-type scale and seven subscales rated on a visual analogue acale (VAS). All the subscales ranged from 0 to 10 where high scores indicated a higher negative impact and/or a greater severity of symptoms. A total score may be obtained after normalization of some subscales and summing the subscales. The FIQ total score range from 0 to 100, and a higher score indicates a greater impact of the syndrome (Rivera & Gonzalez, 2004). The total score of FIQ and the subscales for physical function, feel good, pain, fatigue, morning tiredness, stiffness, anxiety, and depression were used in the study.
The Short-Form Health Survey 36 (SF-36)
This is a generic instrument assessing health-related quality of life. It contains 36 items grouped into eight subscales: physical functioning, physical role, bodily pain, general health, vitality, social functioning, emotional role, and mental health. The range of scores is between 0 and 100 in every subscale, where higher scores indicate better health. In this study, the Spanish version of SF-36 (Alonso, Prieto, & Anto, 1995) was used.
Hospital Anxiety and Depression Scale (HADS)
The HADS contains 14 statements, ranging from 0 to 3, in which a higher score indicates a higher degree of distress. The scores build two subscales: anxiety (0-21) and depression (0-21: Zigmond & Snaith, 1983). The Spanish version of the scale was used in this study (Quintana et al., 2003).
Vanderbilt Pain Management Inventory (VPMI)
The VPMI (Brown & Nicassio, 1987) adapted into Spanish version (Esteve, Lopez, & Ramirez-Maestre, 1999) was used to assess coping strategies. The scale has 18 items divided into 2 subscales designed to assess how often chronic pain sufferers use active and passive coping.
Participants performed the tests just before treatment, after 16 weeks of treatment, and after 12 weeks of a detraining period, during which the patients did not engage in any structured exercise intervention.
The tests were performed out on two separate days with at least 48 hours between each session. This was done to prevent fatigue and flare-ups (acute exacerbation of symptoms) in the patients. The assessment of the tender points, blind flamingo test, chair stand test, and questionnaires were completed on the first visit. Chair sit and reach, back scratch, 8 feet up and go, handgrip strength, and 6-minute walk test on the second day.
Data Analysis
As previously mentioned, it was not possible to use a true experimental design, that is, randomized controlled trial with two groups of patients: a treatment (training) group and a usual care (nontraining) group. Thus, a quasi-experimental reversal design was applied, that is, lacking a control group. The use of this type of design in scientific research has grown considerably in recent years, especially in those settings/groups of diseases where it is very difficult to have a “control” group.
The purpose of the research design used was to determine a baseline measurement, evaluate a treatment (Tai Chi intervention), and evaluate a return to a nontreatment condition (detraining) in the same group of participants. One practical advantage of this type of design is its applicability to real-world settings (in which random assignment is sometimes impossible) while still controlling internal validity as best as possible. This type of design particularly controls participant bias well, as the same individual is used at each testing time point. Because of the small sample size of the pilot data and the nonnormality in the distributions of some variables, traditional multilevel modeling techniques that rely on large sample theory for accurate p values were not appropriate. The Friedman Test, a nonparametric technique, was used to assess the training effects on the outcome variables across multiple observations. When Friedman test was significant, differences between two testing time points (pretest vs. posttest, pretest vs. detraining, posttest vs. detraining) were tested with Wilcoxon test. For all tests, the significance level was set at p < .05. Analyses were performed using the Statistical Package for Social Sciences (SPSS, version 16.0 for Windows; SPSS Inc., Chicago, IL).
Results
Adherence to the intervention was 79.5% (range 61.5% to 97.4%). There were no major adverse effects and no major health problems in the male patients during the training and detraining periods. Baseline characteristics of participants and those who did not meet the inclusion criteria were similar except for tender points (16.0 ± 2.8 vs. 4.0 ±3.6; p = .018) and algometer score (47.65 vs. 82.23; p = .020).
Sociodemographic characteristics of men with fibromyalgia included in the present study are shown in Table 1. Mean values of pain thresholds, algometer score, and tender point count at pretest, posttest, and detraining are shown in Table 2. A significant change for the right (R) side of the gluteal tender point was observed (Table 2). Post hoc analysis revealed that the pain threshold significantly improved from pretest to posttest (p = .027). Pain thresholds of the rest of tender point, algometer score, and tender points count did not significantly change after the intervention period or the detraining phase (Table 2).
Sociodemographic Characteristics of Male With Fibromyalgia” to “Sociodemographic Characteristics of Male with Fibromyalgia

One missing data.
Effects of 16-Week Tai Chi Intervention and 12 Week of Detraining Period on the Magnitude of Tender Points Pressure in Men (n = 6) with Fibromyalgia

Note. Data are presented as means (standard deviation). R = right; L = left.
p < .05 for pretest versus posttest.
Significant changes for BMI and chair sit and reach were identified (Table 3). Post hoc analysis revealed that BMI significantly increased from posttest to detraining (p = .028), and chair sit and reach significantly improved from pretest to posttest (p = .028). This improvement was maintained after detraining phase and even improved but the differences were not statistically significant (−5.2 ± 9.4 vs. −4.6 ± 14.7; p = .833). The results of self-administered questionnaires (Table 4) did not significantly change during the intervention period or the detraining phase.
Effects of 16-Week Tai Chi Intervention on Functional Capacity in Male (n = 6) with Fibromyalgia
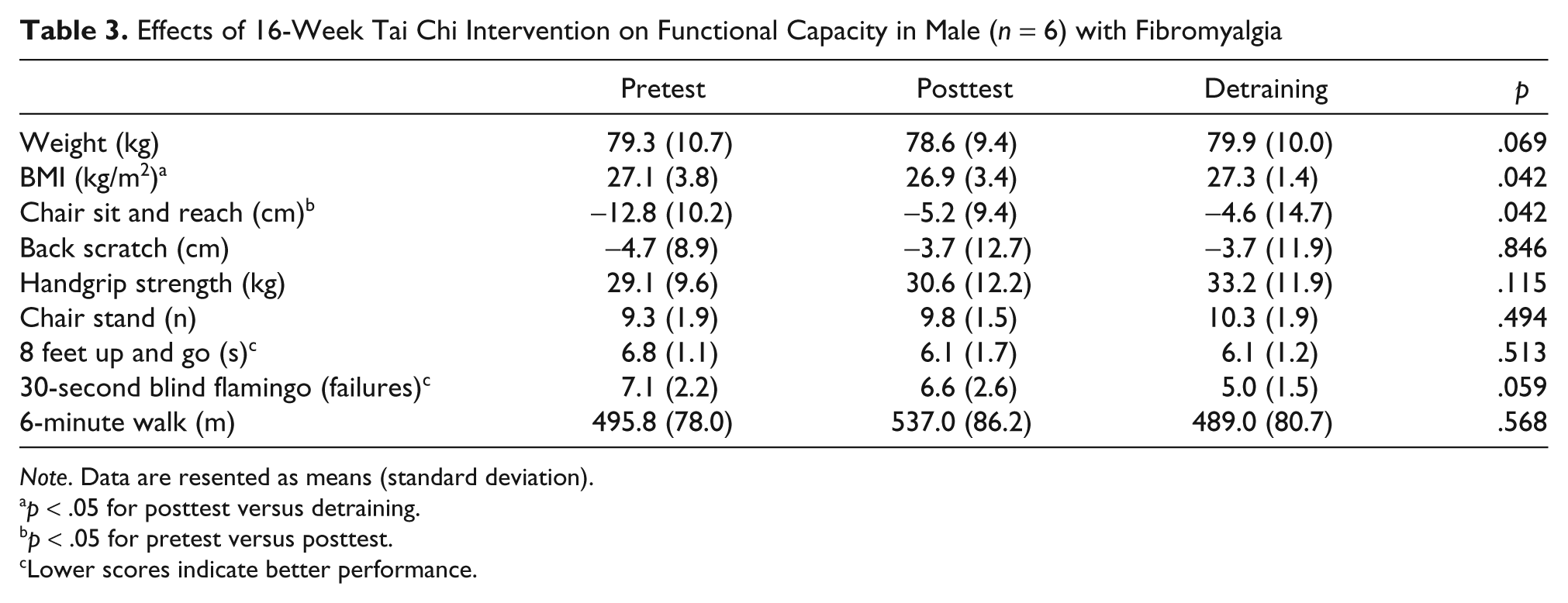
Note. Data are resented as means (standard deviation).
p < .05 for posttest versus detraining.
p < .05 for pretest versus posttest.
Lower scores indicate better performance.
Effects of 16-Week Tai Chi Intervention on Symptomatology, Quality Of Life, and Pain-Coping Strategies Measured in Men (n = 6) with Fibromyalgia

Note. Data are presented as means (standard deviation). FIQ = Fibromyalgia Impact Questionnaire; SF-36 = Short Form 36; VPMI = Vanderbilt Pain Management Inventory; HADS = Hospital Anxiety and Depression Scale: VAS = Visual Analogue Scale.
Discussion
The main finding of present study was that a 4-month Tai Chi intervention improved lower body flexibility but did not significantly affect tenderness, functional capacity, symptomatology, and quality of life in male fibromyalgia patients. The improvement on lower flexibility persisted after the detraining phase. The Tai Chi intervention was well-tolerated and did not have any deleterious effects on patients’ health. Likewise, we observed a statistical improvement in the R-gluteal tender point after treatment and an improvement in L-gluteal tender point and right and left side of great trochanter tender point. Although statistically significant improvement were not observed in other variables, there were positive changes in some of the outcome variables such as the 6-minute walk test (~40 meters) and the subscales of FIQ stiffness (8.9 vs. 7.8, pretest vs. posttest, respectively) and FIQ anxiety (8.1 vs. 5.9, pretest vs. posttest, respectively). Whether these changes are of clinical relevance is not known because of the fact that the minimum clinically important difference for these tests in women with fibromyalgia have not been established. Ries, Echternach, Nof, and Gagnon Blodgett (2009) suggested that an improvement of 33.5 m in the 6-minute walk test could be considered as a minimum detectable change score in people with Alzheimer disease. In our study, 33.3 % (n = 2) improved more than 33.5 meters. Whether the outcomes studied might have changed (impaired) over time in a nontreated group of male fibromyalgia patients is not known. Further randomized controlled trials will be able to answer this issue.
Because of the lack of studies of this nature, and given the uniqueness of our study population, it is difficult to directly compare our results with other studies in male fibromyalgia patients. To our knowledge, only one study analyzed the physical and psychosocial effects of a moderate exercise intervention on two men with fibromyalgia (Karper, 2007). They completed a 14-month exercise intervention (3 days per week, 40 to 45 minutes per session) based on walking and upper and lower body light dumbbell resistance training. Reported changes at the 8th and 14th month included handgrip strength, 32 versus 40 versus 42 kg, respectively, in Participant 1, and 47 versus 55 versus 61 kg, respectively in Participant 2 and chair stand test, 6 versus 11 versus 11 stand in Participant 1 and 12 versus 16 versus 16 stand in Participant 2 (Karper, 2007). We did not observe significant improvement in any of these tests.
Three studies analyzed the effect of Tai Chi intervention in female fibromyalgia patients (Hammond & Freeman, 2006; Taggart et al., 2003; Wang et al., 2010). Hammond and Freeman (2006) included Tai Chi as part of the sessions combined with stretch, strengthening exercises and education, and compared this program (2 times/week for 10 weeks) with a relaxation program (considered as control group). They reported a significant improvement in total score of FIQ after treatment, self-efficacy for managing pain and other symptoms in comparison with a relaxation intervention group, but these changes were not sustained after the detraining period. To note is that the severity of fibromyalgia in our male patients was higher than that observed in the female patients (total score FIQ: 76.1 ± 14.6 vs. 56.9 ± 12.5, respectively) enrolled in the study by Hammond and Freeman (2006). Taggart et al. (2003) implemented an intervention of Tai Chi (Yang style) 1-hour twice weekly classes for 6 weeks in women with fibromyalgia. They observed significant improvement in the dimensions of SF-36 physical functioning, bodily pain, general health, vitally and role emotional, and in the subscales physical function, days feel good, pain, morning tiredness, stiffness, and anxiety of the FIQ. This study did not report the total FIQ score or tender point count, and they did not establish as inclusion criteria the American College of Rheumatology diagnosis criteria for fibromyalgia. Therefore, it is not possible to know the level of severity in these patients.
A recent study (Wang et al., 2010) analyzed the effect of 12 weeks of Tai Chi intervention (10 forms Yang Style 2 times/week) and 12 week of detraining period in fibromyalgia patients (85% female), and they found improvements in total score of FIQ and distance walked in 6-minute walk test after the Tai Chi intervention compared with a control intervention consisting of wellness education and stretching. However they did not report the results for male sample.
The effect of a Tai Chi intervention has been studied in other chronic pain conditions (Fransen, Nairn, Winstanley, Lam, & Edmonds, 2007; Wang, 2008; Wang et al., 2009). Wang (2008) studied the effect of a 12-week Tai Chi (Yang style) intervention in adults with rheumatoid arthritis (n = 10, 2 males) and observed an improvement in the subscale of vitality (SF-36), depression index, and disability index compared with control group, but they did not find improvement in functional capacity. Fransen et al. (2007) compared the effects of a 12-week Tai Chi intervention (twice a week, 24 forms from the Sun Style; n = 56, 18 males) or hydrotherapy in adults with hip or knee osteoarthritis. Both programs achieved significant improvements in the SF-12 physical component summary score, but only hydrotherapy achieved significant gains in physical performance. Wang et al. (2009) reported improvement in physical component summary of SF-36 and chair stand time compared with control group after 12-week Tai Chi intervention (twice a week, 10 modified forms from Yang style) in adults (n = 20, 4 males) with knee osteoarthritis. In the 6-minute walk test, BMI, and balance, they did not obtain significant change (Wang et al., 2009). Lee et al. (2009) implemented an 8-week Tai Chi Qigong intervention (twice a week, n = 29, 2 males) and observed improvements on mental and physical components of SF-36 compared with the control group.
Study Limitations
Some limitations need to be mentioned. First, the findings of the present study should be taken as preliminary because of the small sample size and the lack of a control group. Second, it was not possible to control the changes in the fibromyalgia pharmacological treatment during the intervention. Third, most of the effects reported in this study would become statistically nonsignificant after correction for multiple testing. Furthermore, many of the nonsignificant findings are at elevated risk of Type II error since the study was not adequately powered; however, to conclude negatively from a purely statistical point of view would be too stringent. Nevertheless, most of the observed changes are informative. To note is that this is the first study that analyzed the effect of a Tai Chi intervention in a group of male fibromyalgia patients. The assessment of a large range of functional tests, which are very limited in other studies, is strength of this study. This study should stimulate further research, involving larger sample sizes, on physical fitness and other fibromyalgia indicators in this understudied population.
In summary, a 4-month Tai Chi intervention (three times per week) improved lower body flexibility in men with fibromyalgia. This improvement persisted after the detraining phase. The intervention does not significantly affect tenderness, functional capacity, symptomatology, and quality of life in male fibromyalgia patients. Information on the usefulness of exercise interventions in men with fibromyalgia is specially lacking and future studies are needed.
Footnotes
The author(s) declared no conflicts of interest with respect to the authorship and/or publication of this article.
Financial support was provided by Ministry of Education (grant no. AP-2006-03676, EX-2008-0641), Ministry of Science and Innovation (BES-2009-013442, RYC-2010-05957), Center of Initiatives and Cooperation to the Development (CICODE, University of Granada), Foundation MAPFRE (Spain).