
Abstract
Objective
To evaluate the long-term changes in pulmonary function, exercise capacity, mental health status, and health-related quality of life in individuals with mild coronavirus disease 2019 (COVID-19) over a 12-month period and to assess the implications for post-COVID rehabilitation and healthcare strategies.
Method
This prospective, longitudinal cohort study included 33 patients diagnosed with mild COVID-19. The following pulmonary function tests were used to assess mild COVID-19: the 6-minute walk test, Zung Self-Rating Depression Scale, Zung Self-Rating Anxiety Scale, and 36-Item Short-Form General Health Survey. Repeated measures analysis of variance and linear regression analyses were utilized to evaluate changes over time and identify factors associated with exercise capacity.
Results
Pulmonary function parameters showed significant improvement over 12 months (p < 0.001). The 6-minute walk distance increased significantly from 401.7 ± 12.3 m at 3 months to 523.8 ± 10.4 m at 12 months (p < 0.001); however, it remained below the normative values. Notably, the forced vital capacity, forced expiratory volume in one second, and sex were identified as independent predictors of the 6-minute walk distance at 12 months (p < 0.05).
Conclusion
Patients recovering from mild COVID-19 may experience persistent impairments in pulmonary function, exercise capacity, and mental health up to 1 year postdischarge. These findings underscore the importance of long-term rehabilitation and monitoring for mild COVID-19 patients who are often overlooked in post-COVID healthcare strategies.
Keywords
Introduction
Since the outbreak of the novel coronavirus disease 2019 (COVID-19) in late 2019, the global pandemic caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has resulted in hundreds of millions of confirmed cases and millions of deaths. 1 Although the majority of infected individuals experience mild symptoms and recover without hospitalization, increasing evidence suggests that SARS-CoV-2 infection leads to long-term multisystem sequelae, even among those initially classified as mild cases. 2
Existing studies have demonstrated that COVID-19 can affect multiple physiological systems. For instance, one report described the case of a 57-year-old female with mild COVID-19 who developed hyponatremia and presented with altered mental status, suggesting that SARS-CoV-2 infection affects the hypothalamic–pituitary–adrenal axis and disrupts hormonal regulation. 3 Another study reported that 27.9% of patients with acute COVID-19 who presented with cognitive symptoms continued to experience these symptoms for ≥24 weeks after the acute phase. 4 Additionally, post-acute sequelae of COVID-19 (PASC) have been associated with increased insulin resistance, with inflammation being a key pathological mechanism. 5
Despite significant advancements in understanding post-acute sequelae of moderate-to-severe COVID-19, the long-term effects in mild cases remain poorly characterized. Most existing research has focused on the long-term effects in patients with moderate-to-severe illness; however, the long-term consequences in mild cases remain underexplored.6–9 Studies have shown that even nonhospitalized patients with mild COVID-19 may experience ventilation deficits, particularly in the form of restrictive patterns and small airway disease. 10 Conversely, some studies have reported no significant changes in clinical variables within the first 6 months following acute COVID-19, indicating that such follow-up programs are not universally required and should be instead personalized to avoid the overuse of resources.11,12
Current research on the effects of vaccination policies on patients with mild COVID-19 and their long-term consequences is gradually increasing. With rising vaccination rates, countries are adjusting their management and follow-up strategies for mild cases. Evidence on whether vaccination can mitigate long-term consequences in mild cases is currently limited; however, this area of study remains crucial for public health.
Materials and methods
This was a prospective, longitudinal follow-up study involving adults with mild COVID-19 who were treated and subsequently discharged from Nanchong Central Hospital between January 2020 and May 2020. Patients were enrolled consecutively at their first postdischarge visit.
Definition of mild COVID-19
Mild COVID-19 was defined as laboratory-confirmed SARS-CoV-2 infection with mild clinical symptoms (fever, cough, sore throat, fatigue, headache, myalgia, or loss of taste/smell), respiratory rate <30 breaths/min, peripheral oxygen saturation (SpO2) >93% at rest on room air, partial pressure of arterial oxygen (PaO2)/fraction of inspired oxygen (FiO2) >300 mmHg, no respiratory failure requiring mechanical ventilation, no shock or other organ failure requiring intensive care unit (ICU) admission, and no rapid radiographic progression. 13
Eligibility criteria
Inclusion criteria were as follows: (a) age ≥ 18 years; (b) laboratory-confirmed SARS-CoV-2 infection; (c) fulfillment of the abovementioned definition of mild COVID-19 during the index illness; (d) discharged ≥30 days before baseline assessment; and (e) provided written informed consent.
Exclusion criteria were as follows: a history of pulmonary resection; any major neurological disease (e.g. stroke or neurodegenerative disorders); current major psychiatric disorders diagnosed before COVID-19; and inability to perform spirometry or 6-minute walk test (6MWT) despite coaching or contraindications to exercise testing.
Follow-up
Patients were assessed at 3, 6, and 12 months postdischarge (visit windows of ±2 weeks). Participants underwent physical examination including pulmonary function test, a standardized 6MWT, and mental health (MH) evaluation. They were instructed to complete the Medical Outcomes Study 36-Item Short-Form General Health Survey (SF-36), which measures the health-related quality of life (HRQoL).
The study was conducted in accordance with the Declaration of Helsinki (1975), as revised in 2024, and was approved by the Medical Ethics Commission of West China Hospital, Sichuan university (Approval No.: 163; Date: 16 February 2020). All participants provided written informed consent. All patient details were fully deidentified to ensure confidentiality and privacy protection. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 14
Outcomes measures
Baseline covariates included age, sex, body mass index (BMI), smoking status (never/former/current), and key comorbidities (hypertension, diabetes, and dyslipidemia). Resting SpO2 and heart rate were recorded at each visit.
Primary outcomes were longitudinal changes in pulmonary function and 6-minute walk distance (6MWD) over 12 months. Secondary outcomes included changes in the Zung Self-Rating Depression Scale (SDS)/ Zung Self-Rating Anxiety Scale (SAS) scores, SF-36 domain scores, and the prevalence of abnormal ventilatory patterns at each visit.
Pulmonary function testing
The pulmonary ventilation function test was performed using a pulmonary function test system (X1, XEEK Medical Equipment Co., Ltd., XiaMen, China) following the procedure instructions of the test. The reported parameters included the following: forced expiratory volume in one second (FEV1), forced vital capacity (FVC), FEV1/FVC, forced expiratory flows at 75%, 50%, and 25% (FEF75%, FEF50%, and FEF25%) of pulmonary volume, and peak expiratory flow (PEF). Each test was repeated three times to achieve acceptability and repeatability.
Operational definitions of ventilatory patterns are as follows: FEV1/FVC of <70% was defined as obstructive ventilatory dysfunction, FVC of <80% predicted with FEV1/FVC of ≥70% indicated restrictive ventilatory dysfunction, and FEF25%–75% <70% predicted was defined as small airway dysfunction. 15
6MWT
6MWT was conducted in a 30-m corridor according to the American Thoracic Society (ATS) guidelines, with continuous pulse oximetry and standardized encouragement. The primary outcome was 6MWD. Age- and sex-specific normative values for healthy Chinese adults (≥60 years, 518 ± 72 m and 18–59 years, 601.6 ± 55.51 m) were used as reference.16–18
HRQoL
HRQoL was measured using SF-36, which generates eight domain scores: physical functioning (PF), social functioning (SF), role limitations due to physical problems (RP), role limitations due to emotional problems (RE), MH, bodily pain (BP), vitality (VT), and general health (GH). 19 The scores for each domain can range from 0 (worst) to 100 (best), with higher scores indicating better HRQoL. Age-stratified norms for Chinese population (n = 1688 adults; 18–44 years, 45–64 years, and ≥65 years) served as references. 20
MH
SDS and SAS were used to screen for depression and anxiety.21,22 Both scales consist of 20 items assessing behaviors or symptoms associated with depression/anxiety disorders, with four response choices ranging from “none or a little of the time” to “most or all of the time.” The cutoff values for SDS and SAS are 40 points, as established by validation studies in Chinese adults. 23 Higher the score, higher the levels of depression.
Statistical analysis
All statistical analyses were conducted using IBM Statistical Package for Social Sciences (SPSS; IBM Corp.; Armonk, NY, USA) statistics for Windows, version 22.0. Continuous variables were tested for normality (Shapiro–Wilk tests, Q-Q plots, and skewness/kurtosis). Normally distributed data were presented as mean ± SD and skewed data as median (interquartile range; IQR). Categorical variables were summarized as n (%).
To assess changes in pulmonary function, exercise capacity, and psychological scores across the 3-, 6-, and 12-month visits, repeated measures analysis of variance (ANOVA) was applied. Bonferroni correction was used for multiple comparisons. For non-normal variables, Friedman or Wilcoxon signed-rank tests were used.
Independent-sample t-test or Mann–Whitney U test was used to perform sex-based comparisons at each time point. Pearson or Spearman correlation analysis was performed to examine the relationships between pulmonary function indices, 6MWD, SDS, SAS, and SF-36 domains.
Univariate linear regression analyses were first performed to identify predictors of 6MWD at 12 months. Variables with p < 0.10 were then entered into the multivariate model, which was adjusted for sex as a known confounder. The regression model was specified as follows:

Results
A total of 33 patients (84.6%) completed the 12-month follow-up, comprising 15 females (45.5%) and 18 males (54.5%) who completed the three assessments. The mean age of these 33 patients was 40.8 ±13.8 years, and their mean BMI was 22.7 ± 1.3 kg/m2. The average hospital length of stay (LOS) for the group was 19.6 ± 6.6 days. Three patients were smokers (9.1%), 6 had medical comorbidities (1, chronic obstructive pulmonary disease (COPD); 1, tuberculosis; 1, cardiomegaly; and 3, hypertension). All patients were diagnosed with mild COVID-19, with fever, cough, fatigue, muscle soreness, and sore throat as the main symptoms (Table 1).
Baseline demographic and clinical characteristics of mild COVID-19 survivors (n = 33).

BMI: body mass index; COPD: chronic obstructive pulmonary disease; COVID-19: coronavirus disease 2019; IQR: interquartile range.
Pulmonary function tests
Pulmonary function showed significant improvement over the 12-month follow-up period among mild COVID-19 survivors. As illustrated in Figure 1, FVC, FEV1, and small airway indices (FEF25%, FEF50%, and FEF75%) demonstrated a progressive upward trend from 3 to 12 months postdischarge.

Longitudinal changes in pulmonary function parameters over 3, 6, and 12 months after discharge in mild COVID-19 survivors. (a) Forced vital capacity (FVC); (b) forced expiratory volume in one second (FEV1); (c) forced expiratory flow at 25% of pulmonary volume (FEF25%); (d) FEF50%; (e) FEF75%; and (f) peak expiratory flow (PEF). Data are presented as mean ± SEM. *p < 0.05, **p < 0.01, ***p < 0.001; asterisks (*) indicate significant correlations (p < 0.05). COVID-19: coronavirus disease 2019; FEF50%: forced expiratory flow at 50% of pulmonary volume; FEF75%: forced expiratory flow at 75% of pulmonary volume.
At 3, 6, and 12 months following discharge, the mean FVC (% predicted) values were 81.88 ± 2.08, 94.36 ± 7.19, and 88.30 ± 6.75, respectively, whereas the corresponding mean FEV1 (% predicted) values were 70.49 ± 4.19, 71.37 ± 5.74, and 75.39 ± 6.98. No statistically significant differences were observed between 3 and 6 months for either FVC or FEV1, and the magnitude of change during this interval did not exceed the minimal clinically important difference (MCID). In contrast, both parameters demonstrated significant improvements at 12 months compared with those at 3 and 6 months. The increase in FVC surpassed the established MCID threshold, whereas the gain in FEV1 approached clinical relevance, indicating more substantial recovery over the longer follow-up period. Restrictive ventilatory dysfunction defined by FVC <80% of the predicted value was observed in 6 (18.2%), 10 (30.3%), and 5 (15.2%) patients at 3, 6, and 12 months, respectively. Abnormal FEV1 <80% of the predicted value was more frequent, present in 33 (100%), 30 (90.9%), and 20 (60.6%) patients at the same time points.
Among small airway parameters, FEF25% improved significantly from 68.3% ± 5.4% at 3 months to 74.5% ± 6.9% at 12 months (p < 0.001). A similar recovery trend was observed for FEF50% (73.0% ± 4.4%, 74.3% ± 4.9%, and 77.8% ± 5.3% at 3, 6, and 12 months, respectively; p < 0.05) and FEF75% (76.3% ± 4.0%, 78.4% ± 4.4%, and 79.9% ± 4.8% at 3, 6, and 12 months, respectively). Notably, PEF demonstrated a biphasic pattern: it declined markedly from 76.3% ± 4.0% at 3 months to 62.5% ± 17.4% at 6 months (p < 0.001), followed by partial recovery at 12 months (68.6% ± 9.8%; p < 0.01) compared with that at 3 months.
Overall, these findings indicated that although lung function progressively improved over time, mild COVID-19 survivors may still experience delayed or incomplete recovery, particularly with respect to small airway and peak flow function.
Factors associated with pulmonary recovery
To identify factors independently associated with functional recovery, linear regression analyses were performed using Δ6MWD (Δ6MWD = 6MWD at 12 months − 6MWD at baseline) as the dependent variable. The results of univariate and multivariate linear regression analyses are presented in Table 2.
Univariate and multivariate linear regression analysis of factors associated with 6-minute walk distance (6MWD) at 12 months postdischarge.
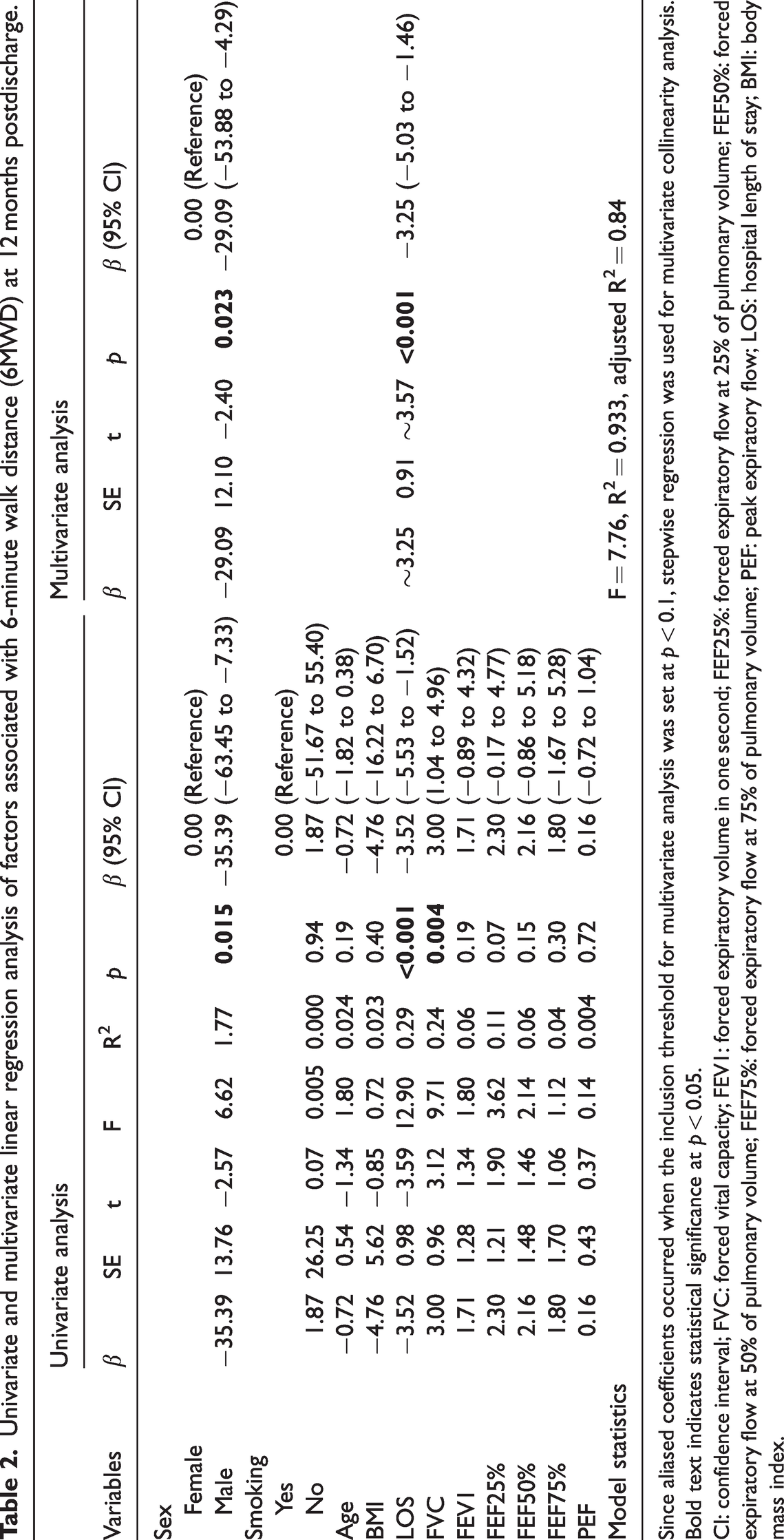
Since aliased coefficients occurred when the inclusion threshold for multivariate analysis was set at p < 0.1, stepwise regression was used for multivariate collinearity analysis.
Bold text indicates statistical significance at p < 0.05.
CI: confidence interval; FVC: forced vital capacity; FEV1: forced expiratory volume in one second; FEF25%: forced expiratory flow at 25% of pulmonary volume; FEF50%: forced expiratory flow at 50% of pulmonary volume; FEF75%: forced expiratory flow at 75% of pulmonary volume; PEF: peak expiratory flow; LOS: hospital length of stay; BMI: body mass index.
In univariate analysis, sex (F = 6.62, R2 = 1.77, β = −35.39, p = 0.015), hospitalization (LOS, F = 12.90, R2 = 0.29, β = −3.52, p < 0.001), FVC (F = 9.71, R2 = 0.24, β = 3.00, p = 0.004), and FEF25% (F = 3.62, R2 = 0.11, β = 2.30, p = 0.07) were significantly associated with 6MWD at 12 months postdischarge. In the multivariate model, sex (β = −29.09, 95% CI: −53.88 to −4.29, p = 0.023) and LOS (β = −3.25, 95% CI: −5.03 to −1.46, p < 0.001) remained independent predictors of 6MWD.
Exercise capacity and psychological status
Exercise capacity, as assessed using 6MWD, improved significantly over time following discharge. As shown in Figure 2a, the mean 6MWD increased from 401.7 ± 12.3 m at 3 months to 409.2 ± 11.7 m at 6 months and further to 523.8 ± 10.4 m at 12 months. Significant differences were observed in the exercise capacity at 12 months compared with those at 3 and 6 months (p < 0.001), whereas no significant difference was found between the exercise capacities at 3 and 6 months.

Longitudinal changes in exercise capacity and psychological status in mild COVID-19 survivors over 12 months. (a) 6-minute walk distance (6MWD); (b) sex-stratified 6MWD; (c) Zung Self-Rating Depression Scale (SDS) and (d) Zung Self-Rating Anxiety Scale (SAS). Values are expressed as mean ± SEM.
Sex-stratified analyses (Figure 2b) revealed that female patients exhibited significantly greater improvement in 6MWD from baseline to 12 months than male patients (129.3 ± 38.4 m vs. 93.9 ± 40.1 m, p = 0.02), indicating a sex-related difference in physical functional recovery.
In terms of MH, SAS scores exhibited a significant and consistent decline across time points (Figure 2c), decreasing from 52.1 ± 9.8 at 3 months to 48.5 ± 12.0 at 6 months (p < 0.05) and 36.0 ± 10.5 at 12 months (p < 0.001). SDS scores showed a decreasing trend from 50.0 ± 9.2 at 3 months to 45.0 ± 11.7 at 6 months, followed by a slight increase to 46.7 ± 9.8 at 12 months (Figure 2d), with a significant reduction observed only between 3 and 6 months (p < 0.05).
Correlation between physiological measures, psychological measures, and HRQoL
To further explore the associations between physiological and psychological variables and HRQoL, correlation analysis was conducted between pulmonary function parameters, 6MWD, SDS, and SAS, and the eight domains of the SF-36 questionnaire. The results are presented as a heatmap in Figure 3.

Correlation heatmap between pulmonary function (FVC, FEV1, FEF25%, FEF50%, FEF75%, and PEF), exercise capacity (6MWD), mental health (SDS, SAS), and domains of the SF-36 questionnaire in mild COVID-19 survivors. *p < 0.05; **p < 0.01; asterisks (*) indicate significant correlations (p < 0.05). Color intensity reflects correlation strength and direction (red = positive, blue = negative). PF: physical functioning; RP: role physical; BP: bodily pain; GH: general health; VT: vitality; SF: social functioning; RE: role emotional; MH: mental health; COVID-19: coronavirus disease 2019; SDS: Self-Rating Depression Scale; SAS: Self-Rating Anxiety Scale; FVC: forced vital capacity; FEV1: forced expiratory volume in one second; FEF25%: forced expiratory flow at 25% of pulmonary volume, FEF50%: forced expiratory flow at 50% of pulmonary volume, FEF75%: forced expiratory flow at 75% of pulmonary volume, PEF: peak expiratory flow; 6MWD: 6-minute walking distance; SF-36: 36-Item Short-Form General Health Survey.
Among the pulmonary function variables, FVC and FEV1 were significantly and positively correlated with the PF domain (r > 0.5, p < 0.05), indicating that better lung capacity was associated with higher physical performance. FEF25% was also positively associated with PF. PEF showed a significant positive correlation with RP and RE domains (p < 0.05), suggesting that PEF reflects broader role functioning capacities.
6MWD was significantly associated with PF, BP, VT, and SF (p < 0.05), indicating that better exercise capacity was linked to improved physical and psychosocial well-being.
SDS and SAS scores demonstrated broad and consistent negative correlations with multiple SF-36 domains, including GH, VT, SF, RE, and MH (all p < 0.05). These results highlighted that anxiety and depression symptoms had a substantial adverse impact on physical and mental components of quality of life.
Together, these findings emphasize the interconnection between lung function, physical performance, psychological status, and perceived health quality in mild COVID-19 survivors, even 1 year after discharge.
Discussion
This prospective cohort study investigated the long-term respiratory and psychological sequelae of patients with mild COVID-19 over a 12-month follow-up period. To provide a concise overview, Table 3 summarizes the principal outcomes across pulmonary function, exercise capacity, MH, and SF-36. Our results revealed persistent small airway dysfunction and reduced exercise capacity, alongside ongoing symptoms of anxiety and depression, even 1 year after hospital discharge. Notably, although majority of survivors demonstrated progressive improvements in FVC, FEV1, and 6MWD, FEF25% and several SF-36 domains showed only partial recovery by 12 months, indicating incomplete normalization. The novelty of this study lies in its focus on initially mild cases, often presumed to recover fully; however, our data revealed residual ventilatory and psychological deficits persisting up to 12 months. Furthermore, the longitudinal design with three standardized follow-up visits (3, 6, and 12 months) provides rare temporal insights into the delayed trajectory of recovery. Collectively, these findings underscore the long-term burden of post-acute sequelae in mild COVID-19 and highlight the need for structured monitoring beyond the acute phase.
Summary of the key findings of this study.

6MWD: 6-minute walking distance; SDS: Self-Rating Depression Scale; SAS: Self-Rating Anxiety Scale; SF-36: 36-Item Short-Form General Health Survey; FVC: forced vital capacity; FEV1: forced expiratory volume in one second; PF: physical functioning; BP: bodily pain; VT: vitality; SF: social functioning; HRQoL: health-related quality of life.
Pulmonary function in our cohort exhibited a heterogeneous and delayed recovery trajectory. Particularly, FVC and FEV1 showed no significant improvement during the first 6 months after discharge but increased significantly by 12 months, suggesting a gradual ventilatory recovery pattern. This delayed improvement is consistent with previous longitudinal studies, which reported minimal or no changes in spirometric parameters such as FVC and diffusing capacity of the lung for carbon (DLCOc) between 3 and 6 months, with noticeable recovery only at 12 months of follow-up. 12 In contrast, a study of vaccinated airline pilots reported that mild COVID-19 did not significantly affect pulmonary function in the early postinfection phase, highlighting the variability of outcomes across populations and exposure settings. 12
Notably, our analysis encompassed a broader range of spirometric indices (FEF25%, FEF50%, FEF75%, and PEF) than most previous studies, which have typically focused on FVC, FEV1, and DLCOc. Small airway indices (e.g. FEF25%, FEF50%, and FEF75%) showed earlier and more consistent improvements, whereas mild airflow limitation persisted in a subset of patients. This observation is consistent with evidence from survivors of severe acute respiratory syndrome (SARS) and Middle East Respiratory Syndrome (MERS), in whom small airway dysfunction and restrictive patterns were detectable years after recovery.24–26 Recently, Cho et al. reported measurable postinfection declines in small airway parameters among healthy young adults with mild SARS-CoV-2 infection, reinforcing that such dysfunction can occur irrespective of disease severity. 27
The persistence of these abnormalities suggests that airway remodeling and immune-mediated injury underlie the slow normalization of ventilatory function after coronavirus infections.28–32 Interestingly, PEF displayed a biphasic trajectory, declining markedly from 3 to 6 months before partially recovering at 12 months, contrasting with the generally progressive improvements in other spirometric indices. This unexpected fluctuation may reflect the effort-dependent nature of PEF measurement, particularly among individuals with variable fatigue, anxiety, or inconsistent respiratory effort. Alternatively, transient airway hyperreactivity or inflammation responses at mid-follow-up may have contributed to this temporary decline.
Collectively, these findings underscore that even nonhospitalized or mildly symptomatic COVID-19 patients can experience persistent ventilatory impairment, which may not be fully captured by conventional spirometric parameters alone. Longitudinal monitoring with small airway, sensitive indices could therefore provide a more nuanced understanding of post-COVID pulmonary recovery.
In this study, 6MWD did not show significant improvement during the first 6 months of follow-up and only increased markedly at 12 months, although values remained below the reference levels for healthy adults. This pattern suggests a delayed recovery of exercise tolerance among patients with mild COVID-19. A similar trend was reported in a prospective study of ICU COVID-19 survivors, where significant improvements in 6MWT were observed only between 3 and 12 months, further supporting the reliability of our findings. 33
However, conclusions regarding 6MWD in the literature remain inconsistent. For example, one study reported an average 6MWD of 538 ± 56.8 m in mild cases, suggesting minimal postinfection impact, whereas another study found mean distances of 455 m and 490 m at 1 and 3 months postinfection, respectively, values still markedly below normative levels.34,35 These discrepancies may reflect differences in study populations, disease severity, and follow-up intervals as well as the multifactorial determinants of 6MWT performance. Factors such as age, height, BMI, respiratory and cardiovascular function, and comorbidities (e.g. diabetes, hypertension, cardiovascular disease, and history of lung disease), together with muscle strength, endurance, and lifestyle behaviors, are known to influence exercise capacity.33,36
We also observed that female patients demonstrated greater improvement in 6MWD than male patients. This sex-related difference may arise from variations in physiological reserve, socioeconomic conditions, comorbidity burden, adherence to rehabilitation, or behavioral and lifestyle factors. Clinically, these findings underscore the need for individualized rehabilitation programs that incorporate sex-specific and patient-centered considerations to optimize recovery trajectories.
Despite interstudy variability, studies have consistently supported the utility of 6MWD as a comprehensive indicator of post-COVID recovery, reflecting not only pulmonary improvement but also overall functional and psychosocial restoration. Its trajectory provides valuable insights into the multidimensional nature of recovery and should be incorporated as a key measure in long-term follow-up protocols for COVID-19 survivors.
MH assessment using SDS and SAS revealed high rates of depression and anxiety in the early postdischarge period, with gradual improvement over time. Nevertheless, approximately 50% of the survivors continued to experience psychological distress at 12 months, indicating that mental recovery lags behind physical recovery. Our findings align with previous research, although prevalence rates of post-COVID anxiety and depression vary widely. For instance, one cross-sectional study reported that 88.6% of COVID-19 survivors experienced some degree of anxiety or depression, whereas another study found that approximately 32% had depression and 41% had anxiety.37,38 Such discrepancies likely reflect differences in disease severity, follow-up duration, and sociocultural contexts, highlighting the heterogeneous psychological impact of COVID-19 across populations.
Multiple factors may contribute to the persistence of anxiety and depression. All participants in our cohort underwent mandatory isolation and hospitalization, which may have induced feelings of social disconnection, fear, and helplessness. 39 Even after discharge, concerns about potential viral infectivity could have triggered anger, guilt, and stigma-related anxiety. Moreover, ongoing physical symptoms, such as fatigue, dyspnea, or reduced exercise tolerance might have reinforced psychological distress, suggesting a bidirectional relationship between physical and MH in the post-COVID stage. These interlinked pathways emphasize the need for integrated rehabilitation addressing both domains. 40
Notably, although SDS and SAS are widely applied screening tools, their outcomes can be influenced by subjective emotional states, cultural norms, and social desirability bias, which may limit diagnostic precision. Future studies should incorporate structured psychiatric diagnostic interviews or validated clinical tools to improve the reliability of psychological assessments. Additionally, longitudinal and interventional studies are warranted to capture the dynamic trajectory of MH in mild COVID-19 survivors and inform the design of tailored psychosocial rehabilitation strategies.
Our study found that SF-36 remained impaired even 1 year after discharge, particularly in domains related to GH, VT, and MH. This observation is consistent with previous studies reporting persistent HRQoL deficits among COVID-19 survivors, suggesting that functional and psychosocial recovery extend well beyond the acute phase.41,42 Further correlation analyses revealed that physical and psychological status were closely associated with HRQoL domains. Pulmonary function, particularly FVC and FEV1, showed significant positive correlations with PF, indicating that greater ventilatory capacity contributes to improved physical performance in daily activities. PEF was positively associated with RP and RE domains, implying that respiratory capacity influences not only physical endurance but also reintegration into social and emotional roles. Likewise, 6MWD was positively correlated with PF, VT, and SF, underscoring that exercise tolerance plays a pivotal role in physical and psychosocial well-being.
Conversely, SDS and SAS scores exhibited strong negative correlations with multiple SF-36 domains (GH, VT, SF, and MH), indicating that anxiety and depression exerted broad and profound adverse effects on the perceived quality of life. These findings align with previous research showing that >80% of COVID-19 survivors experienced anxiety or depression, both of which were independently associated with a diminished HRQoL. 43 Together, these results highlight the intertwined trajectories of physical and psychological recovery and underscore the necessity of integrated rehabilitation models that address both domains simultaneously.
It is important to emphasize that these associations do not imply causality. Recovery of HRQoL is likely influenced by a constellation of factors, including pre-existing comorbidities, socioeconomic conditions, social support, and access to rehabilitation resources. 44 Future research should employ longitudinal designs with structural equation modeling or mediation analysis to delineate causal pathways. Incorporating standardized psychiatric assessments and interventional approaches will be crucial to better understand and enhance the multidimensional recovery process in patients with mild COVID-19. Collectively, these findings provide an integrative understanding of recovery patterns and the multidimensional burden associated with mild COVID-19.
This study demonstrated that patients with mild COVID-19 continued to exhibit pulmonary dysfunction, reduced exercise tolerance, and psychological distress even 1 year after discharge, challenging the conventional assumption that patients with mild COVID-19 achieve full recovery. Notably, FVC and FEV1 showed no significant improvement within the first 6 months, with meaningful recovery observed only at 12 months, a delayed trajectory consistent with findings from larger prospective studies. Clinically, this underscores the importance of long-term rehabilitation management for mild cases, including standardized follow-up protocols focusing on pulmonary function, exercise capacity, and psychological assessment. Interventions should also be tailored to individual characteristics, such as sex-related differences. Moreover, recent evidence has indicated that even asymptomatic individuals and those with mild COVID-19 caused by the Omicron variant may experience long-term physical and psychological sequelae. 45 Early intervention in these populations could not only shorten viral clearance time but also mitigate the risk of persistent post-COVID conditions. 46
From a public health perspective, our findings highlight that mild cases may also represent a substantial component of the “long-COVID” burden and should therefore be included in long-term health investment and surveillance strategies. Existing evidence emphasizes the critical role of rapid and flexible vaccination programs in reducing infection burden during the early stages of viral resurgence as well as sustained investment in healthcare, medical technologies, and information infrastructure to enhance crisis preparedness.47,48 Environmental monitoring of pathogenic microorganisms, including SARS-CoV-2 variants, has also been identified as a key determinant of epidemic diffusion and should be incorporated into public health planning. 49 Furthermore, behavioral studies have shown that individuals with asymptomatic or mild COVID-19 tend to exhibit reduced adherence to protective behaviors such as mask-wearing, social distancing, and hand hygiene practices, which may inadvertently increase transmission risk. 50 Collectively, these insights suggest two key strategies: first, rehabilitation and follow-up programs should explicitly include mild cases to minimize the long-term health burden; second, lessons learned from mild COVID-19 management should inform future public health policy, ensuring that flexible vaccination strategies, environmental surveillance, and long-term health investments are integrated into pandemic preparedness frameworks for potential new viral agents and variants.51,52
This study has several limitations. The sample size of study was relatively small and drawn from a single center, limiting generalizability. No healthy control group or preinfection baseline data were available for comparison. Importantly, we did not evaluate DLCOc, which has been reported as the most sensitive pulmonary function parameter affected by COVID-19 and is strongly correlated with subjective symptoms. The absence of this assessment may have limited our ability to fully characterize the extent of pulmonary impairment. In addition, respiratory muscle strength was not assessed, which may have contributed to reduced exercise performance. Finally, the observational nature of the study precludes any causal inference.
Conclusion
Theoretical implications
This study demonstrates that even patients with mild COVID-19 may experience prolonged pulmonary, physical, and psychological impairment up to 12 months postdischarge. The delayed improvement in FVC and FEV1 highlights a slower recovery trajectory than previously assumed, challenging the notion of full recovery in mild infections. By integrating pulmonary, functional, and psychological outcomes, this report enriches the theoretical understanding of long COVID as a multidimensional syndrome encompassing physiological and psychosocial domains.
Health policy implications
From a health system perspective, patients with mild COVID-19 should be included in structured long-term follow-up and rehabilitation programs, as they represent a significant share of the long-COVID burden. Early, individualized interventions targeting respiratory recovery, exercise tolerance, and MH may prevent chronic sequelae. Sustained investments in vaccination, environmental monitoring, and digital health infrastructure are also vital to strengthen preparedness for future pandemics and emerging variants.
Direction for future research
Future studies should expand to multicenter cohorts with baseline or control data to better define causality. Incorporating DLCOc, respiratory muscle testing, and standardized psychiatric evaluations will refine the understanding of recovery mechanisms. Integrating socioeconomic and behavioral factors may further explain heterogeneity in outcomes and inform targeted rehabilitation strategies.
Footnotes
Acknowledgments
We thank Kang He for assistance with statistical analysis.
Author contributions
Conceptualization, YF and HYY; methodology, ZH; investigation, ZH; writing, YF; review and editing, HYY; project administration, ZH and YF. All authors have read and agreed to the published version of the manuscript and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
All authors declare that there are no conflicts of interest.
Funding
This study was funded by the Technology Research and Development Projects Foundation of Nanchong (No. 20YFZJ0120).