
Abstract
Background:
Lower extremity lymphedema affects a growing number of cancer survivors. Standard-of-care therapy for lymphedema is complete decongestive therapy (CDT), yet the primary outcome measurement of therapeutic efficacy is limb volume, which is relatively insensitive to both well-managed and severe disease. The primary goal of this study was to examine whether physiological sodium magnetic resonance imaging (23Na-MRI) is sensitive to the effect of CDT on leg lymphedema, and how this effect compares with the measurement reproducibility limits.
Methods and Results:
Participants with lymphedema (n = 11) underwent ≥5 sessions of CDT per participant in their affected leg(s) (n = 12) over 9.2 ± 5.6 weeks, following individual treatment plans with a licensed therapist. At the baseline visit and intervention visit, at least one leg was scanned with 23Na-MRI to measure tissue sodium content (TSC) in the skin, muscle, and adipose tissue. Control subjects (n = 16) were scanned at two visits separated by a similar timeframe with no treatment to establish measurement reproducibility. Skin TSC significantly reduced by 4.32 mmol/L (p = 0.027) in affected legs treated by CDT, a change greater than the reproducibility coefficient (RPC) (3.82 mmol/L) in controls. Adipose TSC decreased in treated legs (2.27 mmol/L; p = 0.046), a change less than the RPC (5.83 mmol/L). Muscle TSC (p = 0.171) and leg circumference (p = 0.764) did not decrease in treated legs.
Conclusions:
TSC is reduced in the skin of affected legs with lymphedema treated by CDT, which is observable within the reproducibility limits of 23Na-MRI. Results provide a basis for applying sodium MRI to observe the physiological effects of emerging lymphedema therapies.
Keywords
Introduction
Chronic lymphatic impairment from lymph node removal surgery affects a growing number of cancer survivors, leading to fluid buildup and tissue remodeling known as lymphedema. 1 Patients may receive physical therapy as a part of lymphedema management to reduce swelling, enhance mobility, and improve the quality of life for the 10 million Americans affected by lymphedema.2,3 Standard-of-care therapy is a conservative approach, called complete decongestive therapy (CDT). 4 CDT is administered by a trained physical therapist who performs manual lymphatic drainage massage and prescribes compression, tailored exercise and movement, and skin care. The goal of CDT is to reduce lymph stasis by mobilizing lymphatic fluid. 3 Currently, limb volume is the primary outcome measure of therapeutic efficacy; however, it is relatively insensitive to advanced or well-managed disease. 3 In addition, anthropomorphic measurements are not sensitive to internal tissue compositional changes. As novel treatments are being developed for lymphedema, including pharmaceutical and surgical interventions, more sensitive metrics of disease response are needed to demonstrate physiological relevance and effectiveness. 5
Sodium magnetic resonance imaging (23Na-MRI) is a noninvasive modality capable of measuring standardized tissue sodium content (TSC), which captures physiological tissue changes in deeper tissues, including the adipose tissue, that may change in the setting of lymphatic impairment. 6 Prior work reveals TSC is elevated in legs affected by lymphedema compared with contralateral, unaffected legs in patients with unilateral lower extremity lymphedema (LEL). 7 The goal of this prospective study was to explore if TSC can be modified by standard-of-care CDT in patients with LEL, testing the hypothesis that this conservative intervention, which mobilizes the lymph, reduces TSC despite no change in leg circumference. Furthermore, we sought to confirm the 23Na-MRI measurement reproducibility in the untreated control subjects to evaluate if the treatment effect of CDT in patients was greater than measurement variations in tissue sodium.
Findings reveal a statistically significant reduction in skin tissue sodium storage following CDT, motivating future work with controlled treatment guidelines to determine if 23Na-MRI could serve as an imaging metric for lymphedema therapy in research settings, detecting change in the molecular composition of skin and adipose tissue.
Materials and Methods
Recruitment
All participants provided written informed consent in accordance with the Institutional Review Board (VUMC IRB #202424 and #210181) approved protocol as a part of this prospective study. Enrolled participants, including controls, self-reported female sex, consistent with the higher prevalence of LEL in females following treatment for gynecological cancers.2,8 Eligible participants with LEL planned to receive manual lymphatic drainage as a component of the CDT, consisting of ≥5 sessions per participant on the leg(s) affected by lymphedema with a licensed physical therapist over ≥5 weeks. Inclusion criteria for subjects with LEL consisted of (i) having at least one leg diagnosed with lymphedema, according to the 2020 International Society of Lymphology (ISL) Consensus, 3 and (ii) not undergoing radiation therapy or chemotherapy at the time of the examination.
Participants with LEL either had secondary lymphedema as a result of cancer treatments to the pelvic region or primary lymphedema. In participants with unilateral lymphedema, one leg is affected by lymphedema, and the other (contralateral) side is not; contralateral legs inherently did not receive treatment. Healthy female controls who (i) did not meet ISL criteria for lymphedema and (ii) had no history of cancer or prior radiation treatment were eligible. All volunteers were compatible with MRI and had a calf circumference of <50 cm to fit the extremity 23Na-MRI coil. Exclusion criteria for both cohorts consisted of uncontrolled hypertensive blood pressure (greater than 140 mmHg systolic or greater than 90 mmHg diastolic), chronic kidney disease, or active infection at the time of the examination.
Study visit and standard-of-care therapy
All subjects participated in two identical study visits consisting of a noninvasive, multinuclear MRI scan in the lower extremities following standardized protocols.9,10 Briefly, subjects were scanned at the widest part of the calf in a 3.0 T research-dedicated MRI scanner with a 23Na extremity coil. The protocol included a 23Na-MRI scan (repetition time/echo time = 130/0.99 ms; field-of-view [FOV] = 192 × 192 mm2; in-plane spatial resolution = 3 × 3mm2; slice thickness = 30 mm; number of signal acquisitions = 26; duration = 15:54 minutes:seconds) and a proton 1H-MRI reference scan with water-weighted and fat-weighted contrast to localize anatomy. Four standard aqueous sodium solutions with known concentrations (10, 20, 30, 40 mmol/L) were placed in the FOV of each scan to standardize the 23Na-MRI signal.
Participants with LEL underwent two visits, one performed at a baseline state (untreated by physical therapy for at least 2 months) and the other after the conclusion of the CDT intervention (within 1 week of their last therapy session). CDT consisted of manual lymphatic drainage therapy, compression therapy, exercise, skin care, and education. This study did not dictate the terms of physical therapy treatment, and participants followed the physical therapy plan designed and managed by the treating clinicians, which ranged from approximately 5–10 weeks of intervention. Each participant received at least five sessions of physical therapy treatment on their affected leg(s). Contralateral legs inherently did not receive physical therapy treatment. In 3 of the 11 participants with LEL who completed the study, the intervention visit (post-CDT) was performed before the baseline visit, allowing a 5- to 10-week washout period between visits where no therapy was administered by the treating clinician. In these cases, three affected and one contralateral leg measurements were made. This visit schedule occurred because of logistical and scheduling challenges, since it was difficult to identify and schedule participants before they began therapy, and we did not interfere with the subjects’ treatment plans.
The therapeutic modalities and number of sessions were recorded from both subject reports and electronic health records. Control participants also had two 23Na-MRI study visits with a similar time interval, but they did not receive any treatment or intervention between visits. An outline of the study design and enrollment is shown in Figure 1.
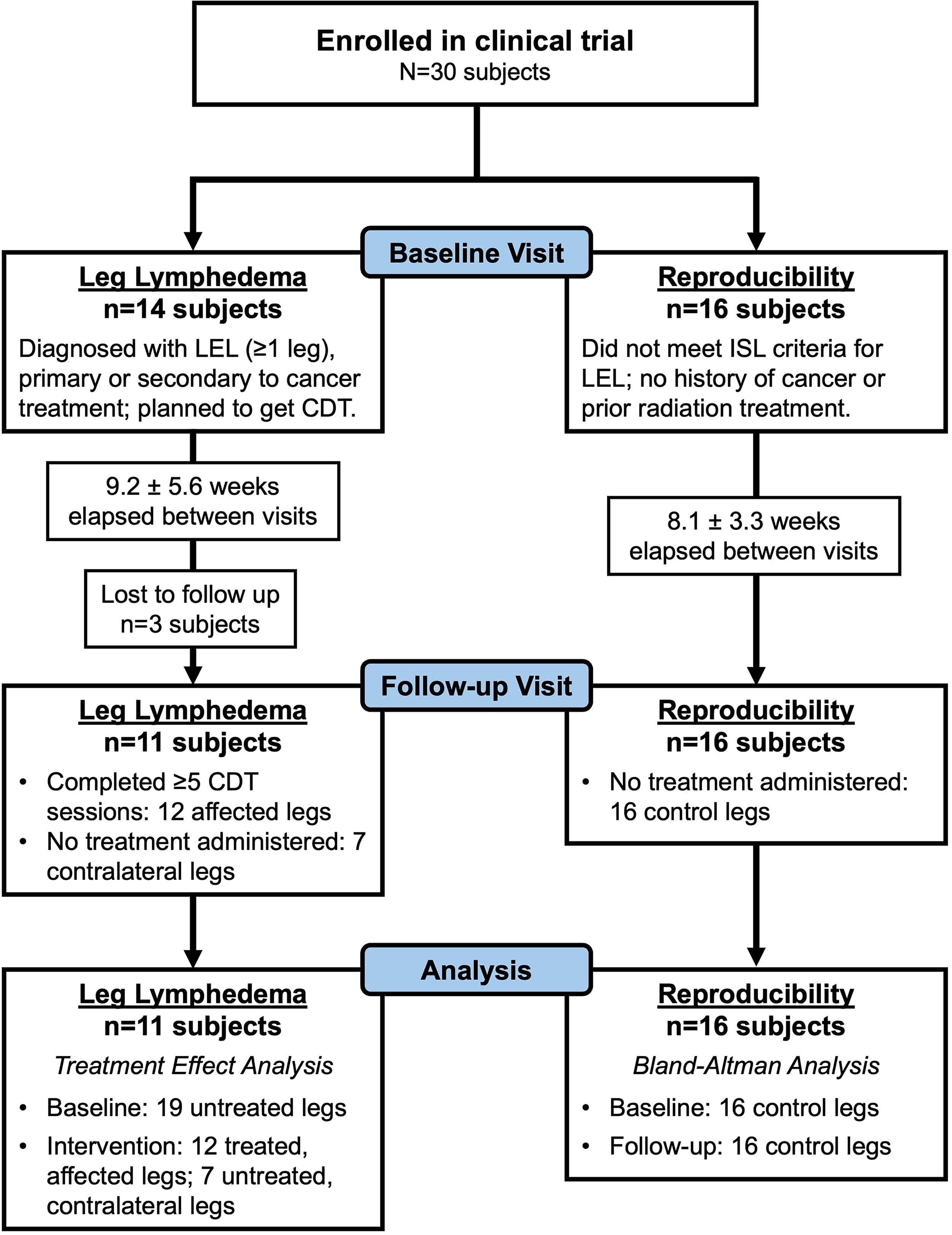
Study design flowchart. Of the participants enrolled in the prospective clinical trial (n = 30), there were 14 subjects who met inclusion criteria for lower extremity lymphedema (LEL) and 16 control subjects without LEL were enrolled for a reproducibility analysis. A baseline visit was conducted in all enrolled subjects. Follow-up visits were conducted, during which three leg lymphedema subjects were lost due to follow-up. During this elapsed time between visits, participants with leg lymphedema (n = 11) received a standard-of-care complete decongestive therapy (CDT) course (≥5 sessions) dictated by their individual treating clinician. At the follow-up visit, imaging data were collected for 12 LEL-affected legs that completed a CDT therapy course and 7 contralateral legs that did not receive treatment. For the reproducibility subjects (n = 16), data were collected for 16 control legs that did not have treatment administered between the baseline and follow-up visits. Analyses were conducted separately for each group.
Image analysis
Multinuclear MRI data were processed to produce standardized TSC (mmol/L). TSC and leg circumference were analyzed from the central slice of each acquisition, capturing the widest part of the calf in the FOV. Standardized TSC, which is comparable across visits and participants, was determined by a voxel-wise linear calibration of the 23Na-MRI signal to the known concentrations of the four standard solutions. Regions of interest were manually identified on the Dixon water-weighted image and used to calculate mean TSC in the skin, subcutaneous adipose tissue (SAT), and muscle; leg circumference was measured as the perimeter of the leg on 1H-MRI.
Statistical analysis
The primary statistical objective is to test the hypothesis that TSC in each region (skin, SAT, and muscle) and leg circumference decreases following CDT treatment. The linear mixed-effects model approach incorporates observations at baseline and intervention visits from affected legs treated with CDT and contralateral legs that did not receive treatment. For a multivariable analysis of the treatment effect, mixed-effects models assessed the difference between treated and untreated legs with leg classification (contralateral vs. affected legs) as an additional fixed effect. Thus, at the intervention visit, affected legs were considered “treated” observations. Observations were also adjusted according to subject ID and leg side, as nested random effects, since one or both of the participants’ legs were scanned across two visits. The nested random effects were included for the intercept at the subject level and at the side of legs within the subject level.
Using model-based (least-squares) means, treatment group means were estimated and compared using Wald tests. Standard residual analysis was performed. The 95% confidence interval (CI) for the mean group difference was also reported.
The secondary statistical objective was to evaluate the reproducibility coefficient (RPC) of TSC measurements for control subjects scanned at two study visits to determine if the observed treatment effects on TSC were within the limits of our method’s reproducibility. Based on a prior reproducibility study of 23Na-MRI in the lower leg skeletal muscle at 3.0 T, our acceptable a priori limits of agreement were ±4.80 mmol/L.
11
Using a Bland–Altman analysis with TSC measurements from both visits for control subjects, we calculated: the bias as the mean difference in TSC between the two visits (
All statistical analyses were performed using R Statistical Software (version 4.4.0). For all tests, a two-sided p < 0.05 was considered significant. Skewed data were transformed to the log scale to meet the homogeneity of variance assumption.
Results
We enrolled 14 participants with LEL for this study and 16 control subjects for reproducibility. However, three participants with LEL did not return for a follow-up visit at the conclusion of treatment course (Fig. 1). Thus, in this prospective analysis, we report baseline and postintervention TSC measurements in 11 participants with LEL (mean ± standard deviation, age = 60.64 ± 8.97 years, body–mass index [BMI] = 29.48 ± 6.80 kg/m2). In total, we scanned 12 affected legs (number with lymphedema ISL stage I/II/III = 5/3/4) that received treatment, and 7 contralateral legs did not receive treatment. One participant with bilateral LEL had two affected legs that were scanned, and three participants with unilateral LEL did not receive scans of their contralateral legs. The elapsed weeks between the baseline and intervention visits were 9.21 ± 5.59 weeks, and the number of treatment sessions was 8.91 ± 5.58 visits. Elapsed weeks between visits did not affect the treatment effect models (likelihood ratio test p values for skin, p = 0.356; SAT p = 0.675; muscle p = 0.515; circumference p = 0.111).
Control participants (n = 16, age = 48.13 ± 12.7 years, BMI = 31.68 ± 5.15 kg/m2) had 8.09 ± 3.26 elapsed weeks between visits. Participant characteristics for the participants with lymphedema and controls are presented in Table 1.
Participant Characteristics for Volunteers with Lower Extremity Lymphedema That Completed Complete Decongestive Therapy and Female Control Subjects for Reproducibility Analyses
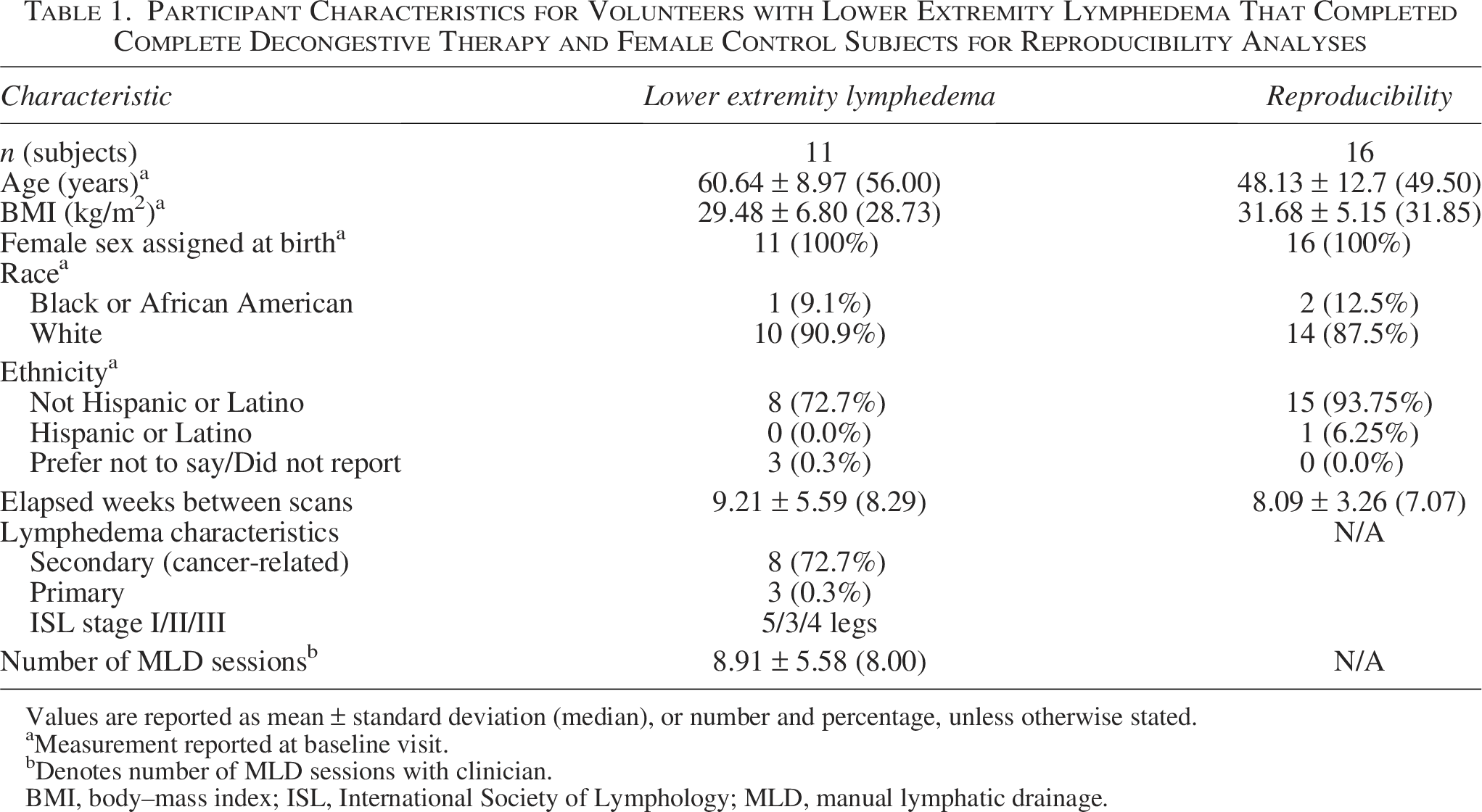
Values are reported as mean ± standard deviation (median), or number and percentage, unless otherwise stated.
Measurement reported at baseline visit.
Denotes number of MLD sessions with clinician.
BMI, body–mass index; ISL, International Society of Lymphology; MLD, manual lymphatic drainage.
To evaluate whether CDT therapy reduced TSC, we first performed linear mixed-effects models to estimate the treatment effect of therapy on TSC. In the skin, TSC in affected, treated legs was significantly reduced by 4.32 mmol/L (95% CI: 0.56–8.08; p = 0.027). Similarly, SAT TSC in treated legs decreased by 2.27 mmol/L (95% CI: 0.04–4.5; p = 0.046). There was no significant change in muscle TSC [difference with 95% CI: 1.28 (−0.6 to 3.16), p = 0.171]. To evaluate whether structural changes were observed on MRI with CDT, a model also evaluated leg circumference at the calf and found no significant change [difference with 95% CI: 0.11 (−0.64 to 0.85), p = 0.764]. A case example is shown in Figure 2. The full group results for skin TSC and leg circumference are summarized in Figure 3 and Table 2.
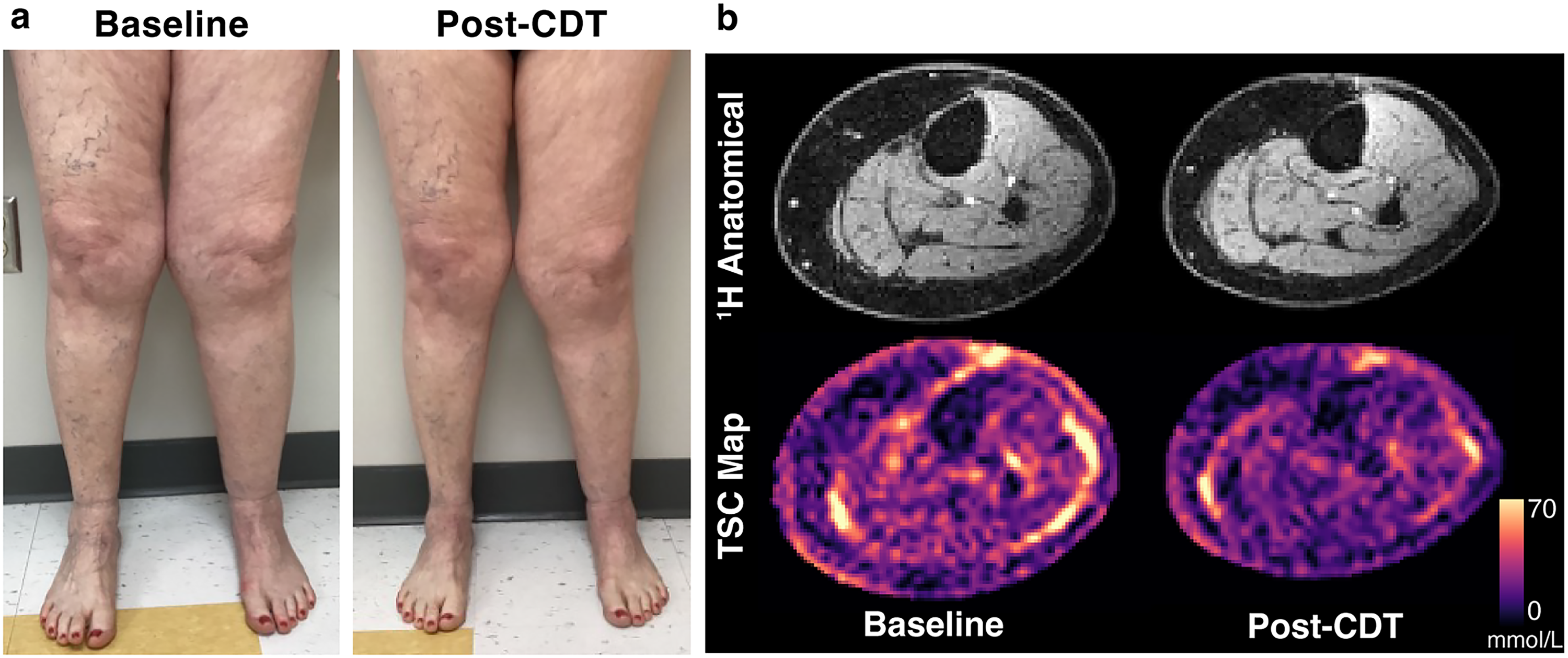
Changes following complete decongestive therapy (CDT) visible with 23Na-MRI.
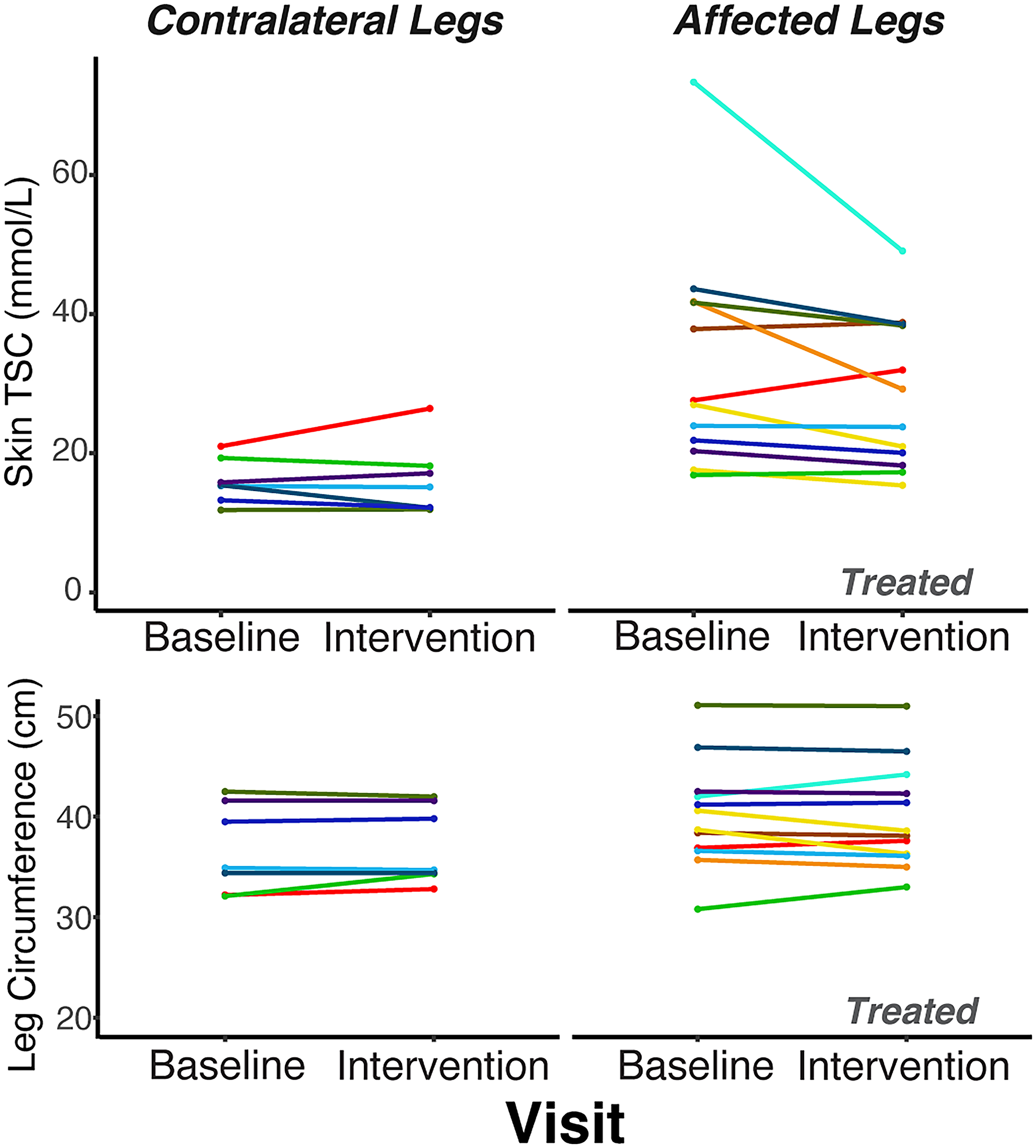
Lymphatic mobilization therapy reduces tissue sodium, measurable by 23Na-MRI. In row 1, skin TSC demonstrates a trend of reduced skin TSC at the intervention visit compared with the baseline visit in the affected legs (Wald test, p = 0.027) (right, n = 12 legs, abs. val. mean difference = 4.32 ± 7.57 mmol/L) compared with the change in TSC between visits for contralateral legs (left, n = 7 legs, abs. val. mean difference = 0.176 ± 2.71 mmol/L). In row 2, leg circumference for contralateral legs and affected legs at intervention versus baseline visits shows limited change following lymphatic mobilization treatment that was administered to affected legs. The mean difference in leg circumference in affected legs between visits (abs. val. mean difference = 0.108 ± 1.38 cm) is not significantly different from contralateral legs (abs. val. mean difference = 0.343 ± 0.890 cm) that did not receive treatment (Wald test, p = 0.764). Colors indicate measurements from the same participant. Lines connect datapoints from the same leg measured at the baseline and intervention visits (2 observations per leg).
Treatment Effect of Standard-of-Care Complete Decongestive Therapy on Tissue Sodium Content and Leg Circumference
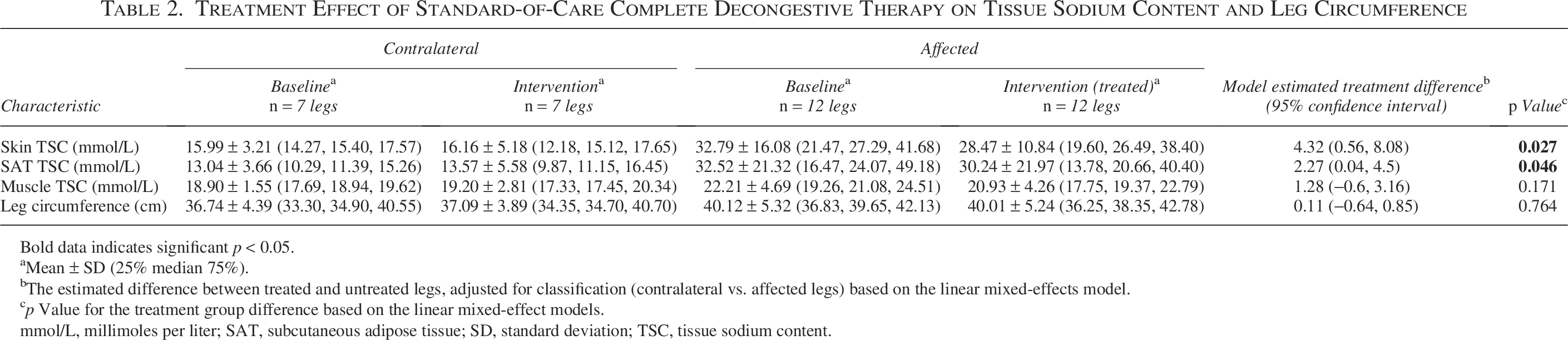
Bold data indicates significant p < 0.05.
Mean ± SD (25% median 75%).
The estimated difference between treated and untreated legs, adjusted for classification (contralateral vs. affected legs) based on the linear mixed-effects model.
p Value for the treatment group difference based on the linear mixed-effect models.
mmol/L, millimoles per liter; SAT, subcutaneous adipose tissue; SD, standard deviation; TSC, tissue sodium content.
For the second statistical objective, we evaluated the reproducibility of TSC measurements in the skin, SAT, and muscle of 16 female control subjects (Fig. 4). The skin, SAT, and muscle TSC have insignificant measurement biases less than 0.25 mmol/L, p > 0.05 which is consistent with a prior repeatability study of lower leg skeletal muscle TSC. 11 In our study, the RPC for skin TSC is 3.82 mmol/L (mean difference ± standard deviation in controls = 0.132 ± 1.95 mmol/L, Bland–Altman p = 0.790), and the treatment effect on skin TSC in lymphedema (4.32 mmol/L) is greater. This underscores the significance and observability of lymphatic therapy by CDT to reduce TSC in the skin of patients with lymphedema. The RPC for SAT TSC was 5.83 mmol/L (mean difference ± standard deviation in controls = 0.248 ± 2.98, Bland–Altman p = 0.744). Because the treatment effect on SAT TSC (2.27 mmol/L) is less than the RPC, the observed difference in TSC in treated legs may not be solely attributed to the intervention. In the muscle region, the RPC was 3.33 mmol/L (mean difference in controls = 0.110 ± 1.70, Bland–Altman p = 0.798), which is greater than the observed, nonsignificant treatment effect in the lymphedema cohort.
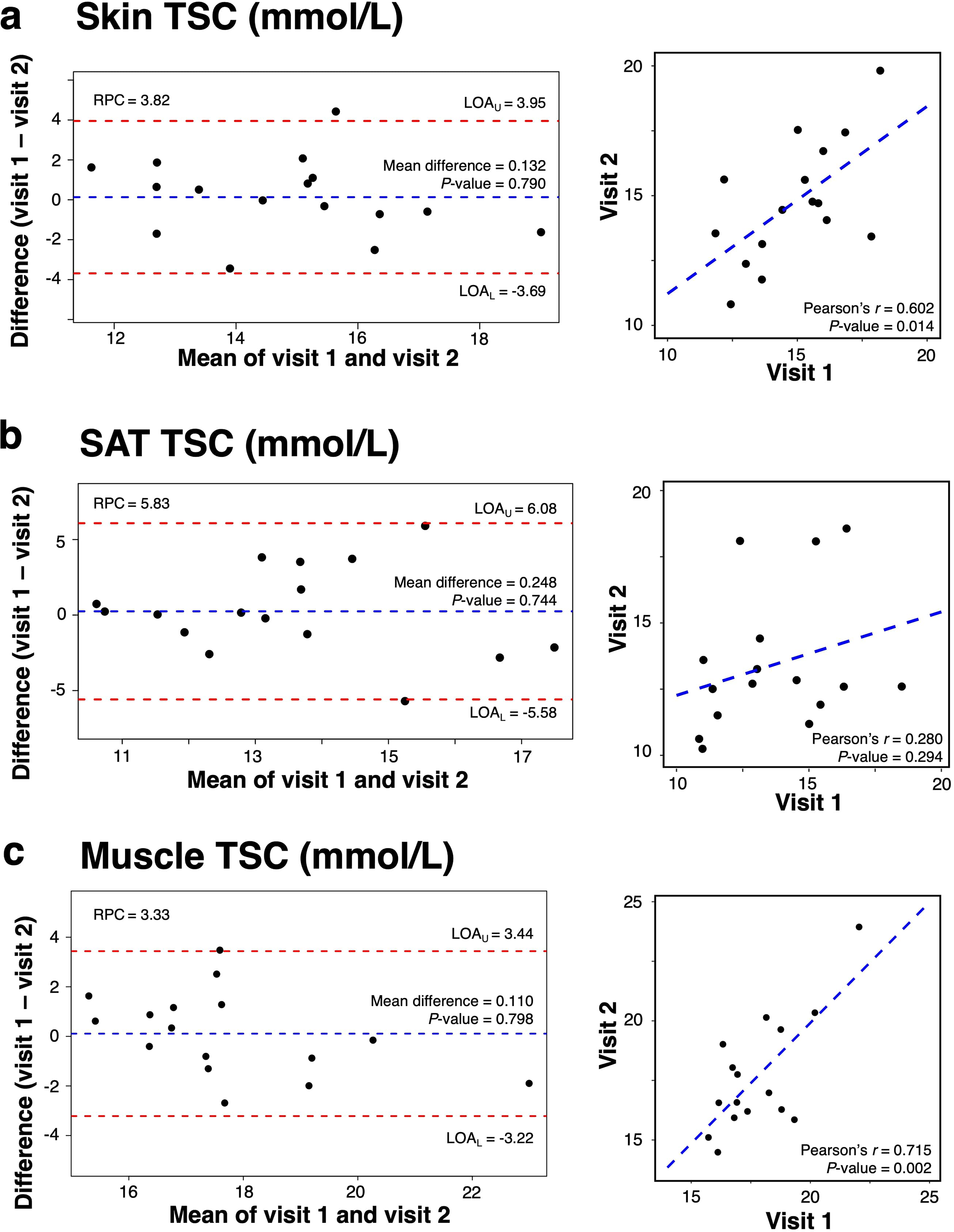
Bland–Altman analyses to assess reproducibility of regional tissue sodium content (TSC) measurements in female controls. Reproducibility and Pearson’s correlation of TSC measurements in the skin
Discussion
TSC was reduced by standard-of-care CDT in limbs affected by lymphedema in the skin and, to a lesser extent, in the SAT. We confirmed the reproducibility of 23Na-MRI in controls over a similar time course to lymphedema therapy, which strengthens the interpretation of the findings in participants with lymphedema who underwent CDT. The treatment effect on skin TSC (reduced 4.32 mmol/L) was greater than the RPC (3.82 mmol/L), suggesting that the decrease in treated legs is due to more than typical variation in 23Na-MRI skin measurements. This result demonstrates potential for sodium MRI to observe the effects of a lymphatic therapy on lymphedema tissue, using a physiological imaging metric of TSC.
Results were less conclusive in the SAT, where the RPC (5.83 mmol/L) is greater than the difference observed with treatment (reduced 2.27 mmol/L). The larger variability in SAT RPC could be because the SAT is a larger, heterogeneous region, and treatment may have more localized effects in the tissue, which may not be captured by averaging TSC in the whole SAT region. No significant changes in muscle TSC were observed due to CDT (p = 0.171). These results are logical, considering that CDT is a conservative treatment of at least the superficial tissue that may not impact deeper adipose tissue, unless the therapist utilizes manual techniques to intentionally target deeper tissues. Evaluating the nuances of the manual approach was outside the scope of this study but warrants further investigation given our understanding of both deep and superficial tissue involvement of lymphedema.
Furthermore, this study measured reproducibility to provide a reference for longitudinal TSC measurements over the typical duration of lymphedema CDT. The measured reproducibility of TSC by 23Na-MRI in this study is slightly improved compared with prior reports in the literature that measured the repeatability coefficient (variability between two scans back-to-back) to be 4.8 mmol/L in the skeletal muscle. 11
23Na-MRI is a completely noninvasive, physiological imaging modality that demonstrates tissue sodium reduction in affected extremities with lymphedema in response to CDT. Plasma sodium, a systemic measurement of electrolyte balance, did not change in previous studies of manual lymphatic drainage therapy in patients with LEL.12,13 Systemic sodium did not decrease, despite small changes in fluid volume that confirm lymph fluid mobilization, a component of standard-of-care CDT. Thus, 23Na-MRI can measure a local change of TSC, which is dynamic during lymphatic treatment and may not be detectable with bioimpedance tools alone. 12 Tissue sodium reduction in legs with lymphedema demonstrates the relevance of local sodium measurements in vivo to understanding human lymphatic function and dysfunction. Regional tissue sodium could also relate to the lymphatic anatomy revealed in imaging studies using lymphography. 14 Multinuclear 23Na/1H MRI can be further developed to image both lymphatic anatomy together with a functional correlate, such as tissue sodium. This could be important to apply personalized therapy for unique cases of lymphedema. For instance, in primary lymphedemas or contralateral extremities, tissue sodium and lymphatic imaging together may help identify lymphatic collectors and tissue territories which can/cannot accept rerouted fluid during decongestion. In addition, 23Na/1H MRI may enable the study of how interstitial sodium and lymphatic clearance could affect immune cell function in lymphedema, given that some immune cells sense sodium.15,16
Although promising, the treatment study results are exploratory, considering the limited sample size and the noncontrolled treatment course. This study enrolled participants receiving CDT, and procedures did not interfere with treatment schedules or plans. The choice of personal treatment plans and participant adherence could impact the effect of the therapy on TSC outcome measures. This study took a pragmatic approach to evaluate therapy findings without prescription of the therapy including frequency and dosing to potentially give “real-world” findings from therapy. Several participants underwent baseline measurements after a washout period following CDT, rather than prior to the CDT session. It is reasonable to interpret their results with the other participants because most participants are not treatment-naïve and have received prior CDT sessions. Still, disease progression could have occurred during this washout period, which may have affected the primary outcome measure of skin sodium. Participants with primary or secondary lymphedema were included in this study, who received a similar treatment approach by CDT. Primary lymphedema cases may have inherently different lymphatic anatomy, which could affect their ability to reroute lymphatic fluid and thereby tissue sodium response to CDT. Further investigations in primary lymphedema would benefit from anatomical and functional imaging to personalize approaches to therapy. Although substantial changes in tissue sodium were not observed in the contralateral untreated extremity, this study cannot rule out potential systemic or contralateral effects of CDT on tissue sodium in LEL. MRI observation of subclinical lymphedema in contralateral extremities may be possible and, if determined sensitive through further research, could be useful to indicate a patient’s need for preventative treatment of bilateral LEL. Future work in this ongoing study aims to increase the sample size to provide benchmark reference values of TSC in lymphedema following a standard-of-care therapy and apply 23Na-MRI to evaluate emerging lymphedema therapy practices.
Lymphatic disease treatment strategies are emerging for lymphedema beyond conservative management. 17 Inflammation and adipose tissue are becoming desirable therapeutic targets in lymphedema.5,18 Emerging candidate therapies include anti-inflammatory pharmaceuticals,19–21 microsurgical techniques, 22 and engineered implants. 23 However, only coarse biomarkers of total limb volume or bioimpedance are used to triage patients into clinical trials and monitor treatment outcomes.19,23,24 Initial treatment trials indicate a limited effect of therapy candidates on limb volume or bioimpedance. 24 For these emerging therapies to be optimized in treating lymphedema, mechanistic outcome measures other than limb volume are needed.
Our study found that while skin TSC was reduced significantly, leg circumference did not significantly decrease in treated legs. Some participants were not treatment naïve and may have previously optimized limb volume. An observed effect on skin TSC without limb volume reduction is consistent with a previous study in patients with leg lipedema that showed reduced skin TSC following a course of tailored CDT, including manual lymphatic drainage therapy. 25 Anthropomorphic and structural measurements of the legs are typically used by clinicians for therapy management, although these measurements may not detect underlying, dynamic changes in tissue that correspond to therapeutic response. This work demonstrates the potential of 23Na-MRI to provide sensitive, mechanistic characterization of lymphedema treatment response. While this study was designed to demonstrate that novel sodium imaging is sensitive to an established lymphatic therapy, future research is warranted to investigate whether tissue sodium changes following novel therapies for lymphedema. 26
Conclusion
TSC is reduced in the skin of affected legs with lymphedema treated by CDT, which is observable within the reproducibility limits of 23Na-MRI. These findings demonstrate that tissue sodium can be reduced following standard-of-care therapy for lymphedema, which is measurable by standardized 23Na-MRI. A multinuclear MRI approach could provide physiological outcome measures to evaluate emerging lymphatic therapies. Overall, the study establishes a basis for assessing tissue sodium by 23Na-MRI in response to lymphatic disease treatment, amid the growing recognition of imaging science as a gap in lymphatic disease research. 27
Authors’ Contributions
S.L.T.: Methodology, software, formal analysis, investigation, writing—original draft, and visualization. V.N.C.: Methodology, validation, investigation, and data curation. P.M.C.D.: Conceptualization, methodology, resources, validation, and writing—reviewing and editing. S.-C.C.: Methodology, formal analysis, writing—reviewing and editing, and visualization. M.D.P.: Methodology, software, validation, and formal analysis. M.E.G.: Investigation, data curation, and project administration. J.A.B.: Investigation and data curation. M.P.D.: Investigation and data curation. A.O.S.: Investigation and data curation. C.N.W.: Investigation and data curation. Y.L.: Methodology, formal analysis, visualization, and supervision. A.J.B.: Conceptualization, resources, and supervision. R.L.C.: Conceptualization, methodology, resources, writing—original draft, supervision, project administration, and funding acquisition.
Footnotes
Acknowledgments
The authors thank the VUIIS Human Imaging Core technologists and Philips support from Charles Nockowski and Ryan Robison for imaging experiment support.
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
This work was supported by the National Institutes of Health (NIH), National Heart, Lung, and Blood Institute (NHLBI; Bethesda, MD) R01HL155523, R01HL157378, and the Lipedema Foundation (LF; New York, NY). Imaging experiments were performed at the Vanderbilt University Institute of Imaging Science (VUIIS) Human Imaging Core, with instruments funded by National Institutes of Health (NIH) grant 1S10OD021771-01. Research resources included REDCap, supported by the National Center for Advancing Translational Sciences Clinical Translational Science Award Program of the NIH, award number UL1 TR000445. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.