
Abstract
Background: Bundled payments for total joint arthroplasty (TJA) were instituted by the Centers for Medicare and Medicaid Services (CMS) to reimburse providers a lump sum for operative and 90-day postoperative costs. Gaining a better understanding of which TJA patients are at risk for early return to the operating room (OR) is critical in preoperative optimization of those with modifiable risks, which could improve bundled-payment performance. Purpose: We sought to identify the most common reason for readmissions, as well as patient characteristics and costs, associated with early return to the OR among TJA patients. Methods: This was a retrospective cohort study of Medicare patients who had undergone primary total hip or knee arthroplasty (THA or TKA) between 2013 and 2018 at a tertiary care hospital. We used the CMS research identifiable files database to identify the most common reasons for readmissions and revisions within 90 days of surgery. Total billing claims were used to determine the cost of early readmissions and revisions. Multivariate regression analysis was used to determine the characteristics associated with early readmission or revision. Results: Out of 20 166 primary TJA patients identified, we found 1349 readmissions (5.6%) and 163 (0.8%) revisions within 90 days of surgery. Dislocation was the most common indication for readmission, and periprosthetic joint infection was the most common indication for revision. Early return to the OR was associated with a mean $105,988 (standard deviation [SD] = $76,865) in CMS claims for the inpatient stay. Factors associated with a higher risk of early reoperation were female sex, THA, longer length of stay, and discharge to long-term care facility. Conclusions: This retrospective cohort study found that early return to the OR after TJA increased overall 90-day costs by 260%, suggesting that early reoperation might have a significant impact on bundled payments. Further study is warranted.
Introduction
Total joint arthroplasty (TJA) is among the most common orthopedic procedures performed in the United States [36,37]. In 2013, the Centers for Medicare and Medicaid Services (CMS) instituted bundled payments for TJAs via the voluntary Bundled Payments for Care Improvement (BPCI) initiative to try to curtail costs. This program was expanded in 2016 with the mandatory Comprehensive Care for Joint Replacement (CJR) initiative [6], which gave participating providers a fixed reimbursement rate covering all costs during a 90-day episode of care. After almost a decade, bundled-payment initiatives have decreased average TJA episode-of-care costs, but they have also been met with concerns of patient “cherry picking” and uneven revenue sharing [2,17,31,35].
To improve CJR performance, providers have undertaken multiple strategies toward decreasing costs. These include a shift to outpatient TJA, shorter inpatient stays when required, and a higher percentage of patients being discharged home after an inpatient stay [3,12,13,20,29,40]. A more difficult factor to control, however, is avoiding early readmissions and reoperations. These “bundle-buster” patients who require early revision can significantly affect bundled payments; an unplanned readmission after TJA can increase episode-of-care costs from $5000 to $200 000 [24].
Much of the existing literature, however, has studied only all-cause readmission (medical and surgical), and few have studied the costs associated with an early return to the operating room (OR) [7,19,27,31]. Given that modifiable and non-modifiable risk factors have been associated with early revision after TJA, developing a better understanding of which patients are at high risk for early return to the OR can be critical in preoperative risk stratification and optimization for those with modifiable risks [18,30]. This could ultimately improve bundled payments.
The purpose of this study was to identify the causes and cost of early readmissions and reoperations within 90 days after TJA. Second, we aimed to identify the characteristics of patients who returned to the OR. By identifying the causes and costs of early readmissions and reoperations, we hoped to identify the subset of high-risk patients who may benefit from interventions that can improve patient outcomes and bundled payments.
Methods
Following institutional review board approval, we conducted a retrospective cohort study of patients who underwent primary hip or knee arthroplasty covered by Medicare at a single tertiary care hospital, which has more than 20 fellowship-trained arthroplasty surgeons, from 2013 to 2018. The CMS provided research identifiable files (RIFs) for this cohort. Our study focused on 1 institution in order to use that institution’s electronic medical records to verify the CMS claims.
The data set included demographic and surgical details for each patient, including diagnoses and costs associated with each claim. In addition, each Medicare beneficiary is assigned a unique encrypted beneficiary ID to identify the initial TJA admission and any subsequent readmissions. Of note, the tertiary care hospital does not have its own emergency department. Readmitted patients can receive care elsewhere or be transferred to the surgical hospital once triaged. However, all readmissions were captured by this data set regardless of location.
All Medicare patients who obtained an elective, primary total hip or knee arthroplasty (THA or TKA) during the study period were included in the study. Exclusion criteria were a revision surgery as the first index procedure, cases labeled as emergent or urgent, hemiarthroplasty, hip resurfacing, and unicompartmental TKA.
Medicare beneficiaries admitted under Diagnosis Related Group (DRG) 469 (major TJA with major complication and comorbidity) and 470 (Major TJA without major complication and comorbidity) were included in the cohort. Next, this was filtered to ensure only the inclusion of primary TJAs. International Classification of Diseases, 9th edition (ICD-9), Clinical Modification codes 81.51 and 81.54 were used to identify primary THA and TKA, respectively. The ICD-10 codes 0SR9, 0SRB, 0SRC, 0SRD were also used to identify primary THA and TKA. Next, we filtered for elective procedures. Finally, we screened by provider number to make sure that all index procedures were done at our institution. This resulted in 20 166 primary TJA (11 027 TKA and 9139 THA) claims during the 6-year study period.
The following demographic characteristics were available for each patient in the cohort: age, sex, race, and state of residence. In addition, we used the DRG codes 469 and 470 to indicate the presence of a major comorbidity. The DRG code 469 is strictly monitored by CMS and is defined as a major comorbidity such as acute heart, renal, or respiratory failure [4,32]. Other comorbidities such as hypertension or dementia are not captured by this designation.
Of the 20 166 primary TJAs performed during the study period (Table 1), there were 11 027 TKAs and 9139 THAs performed on 17 550 patients. There were 2800 (14%) primary TJA cases billed as including either robotic assistance or computer navigation. The average patient age was 73 years (standard deviation [SD] = 7), and the majority were women (65%) and White (89%). In addition, the vast majority were classified as having no major comorbidities (99%) such as acute heart, renal, or respiratory failure; 70% of patients lived in the same state as the operative hospital.
Primary TJA patient demographics.
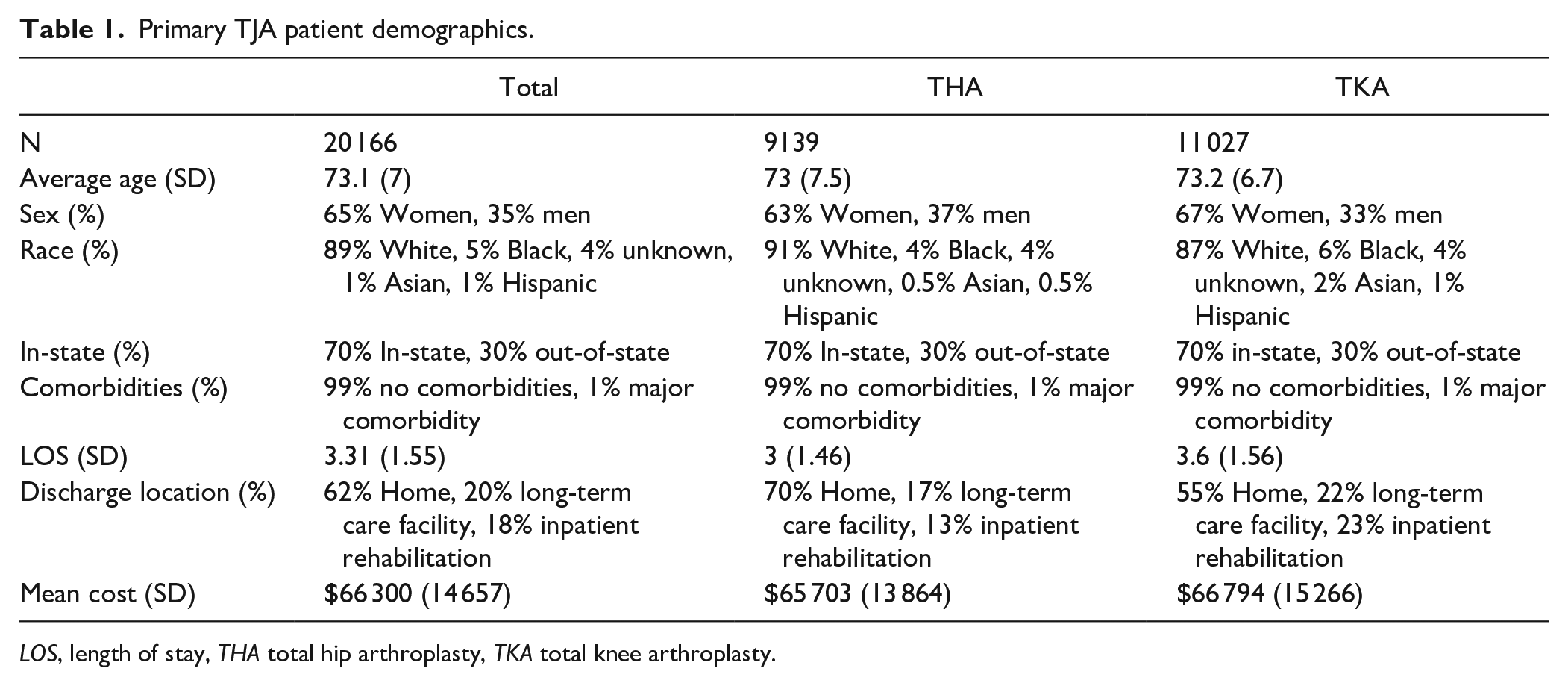
LOS, length of stay, THA total hip arthroplasty, TKA total knee arthroplasty.
The average length of hospital stay was 3 (1.46) days after THA and 3.6 (1.56) days after TKA. Most patients were discharged home (62%), whereas 18% went to an inpatient rehabilitation center and 20% went to a long-term care facility. The mean cost for TJA and subsequent hospital stay was $66 300 (SD = $14 657). The average total claim amount for encounters with robotics/computer navigation was $69 971 (SD = $14 939) and $65 708 (SD = $14 525) without.
Additional variables available in the data set included claim start and end dates, discharge location, provider location, total claim cost, ICD-9/10 codes for primary diagnosis, and procedures. The claim dates were used to determine the date of surgery, as well as the length of hospital stay. In addition, all claims were separated based on whether they occurred before or after the CJR initiative implementation (in 2016). Finally, discharge location was organized into 3 groups: home (home and home health services), inpatient rehabilitation center (short term inpatient care and inpatient rehabilitation center), and long-term care facility (skilled nursing facility, hospice, and long-term care hospital).
Employing the unique beneficiary ID, we defined readmissions as the presence of new hospital claim records within 90 days of the patient’s discharge. Rehabilitation service claims (ICD-9 code V57, ICD-10 Z51), as well as any other codes for “Aftercare following joint replacement surgery” (ICD-10 Z47.1), were excluded. Postoperative claims associated with a diagnosis of osteoarthritis (ICD-9 715, ICD-10 M16, M17) were all excluded as well. Next, the most common reasons for readmission and associated costs were delineated using their principal diagnosis code and claim cost total.
All-cause return to the OR was identified by reviewing new inpatient claims within the 90-day period. Revisions were identified using DRG codes 466, 467, and 468. The indication for reoperation was identified using ICD-9/10 codes. In addition, all revision cases were verified by cross-checking each patient in the institutional electronic medical records. Finally, the average claim cost of each reoperation and subsequent inpatient stay was calculated, defining the economic burden of early return to the OR.
Statistical Analysis
Descriptive statistics, such as means with ranges and frequency statistics, were used to report baseline characteristics. Initial univariate testing was performed for each covariate against the primary outcomes (readmission and revision). Continuous variables (age and length of stay) were evaluated using a Wilcoxon-rank sum test. Categorical variables (sex, presence of a major comorbidity, race, discharge location) were evaluated using a χ2 test. All covariates were advanced into the multivariate logistic regression models. Separate models were run for readmissions and revisions as the primary outcome. Statistically significant association with the primary outcome was considered for P < .05 in the multivariate model. All analyses were performed using SAS Software version 9.4 (SAS Institute, Cary, North Carolina).
Results
Readmissions within 90 days of the 20 166 TJA claims included 1349 additional inpatient claims (Table 2). These claims were recorded for 1120 distinct patients, resulting in a 5.6% (1120/20 166) 90-day readmission rate for both THA and TKA. The average length of stay for these readmissions was 5.8 (5.3) days, and the average claim cost was $62 173 (SD = $61,286). The mean time to readmission was 34 (SD = 26) days. Twenty-two percent of patients were readmitted to the location of their index surgery; 13% were admitted to the general hospital next door. All other hospital percentages were less than 4%. Overall, it appears that patients were readmitted to hospitals closer to their home.
Inpatient claims at <90 days of discharge.
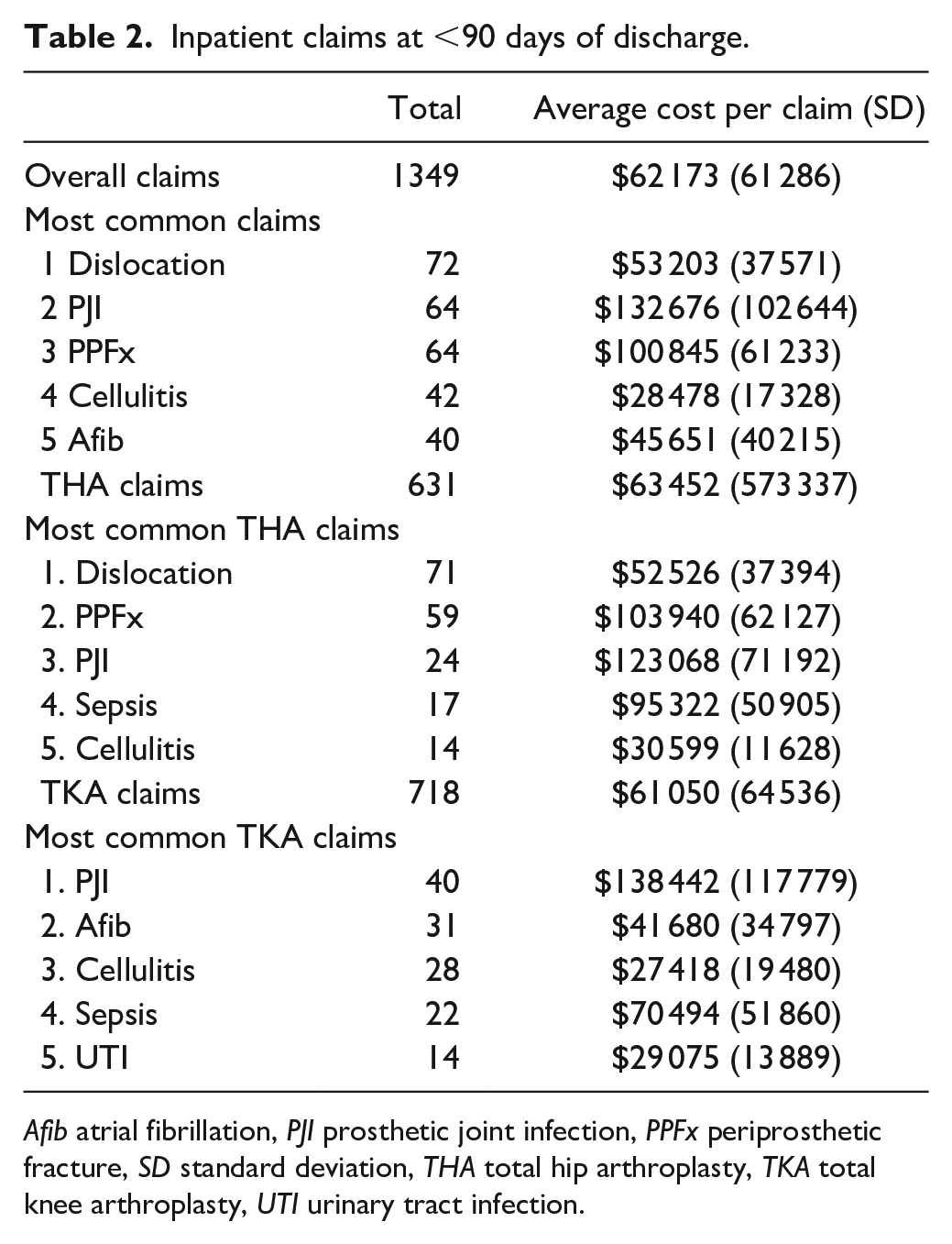
Afib atrial fibrillation, PJI prosthetic joint infection, PPFx periprosthetic fracture, SD standard deviation, THA total hip arthroplasty, TKA total knee arthroplasty, UTI urinary tract infection.
The most common readmission claim diagnoses in the overall TJA cohort were dislocations (5%), periprosthetic joint infection (PJI) (5%), periprosthetic fracture (PPFx) (5%), cellulitis (3%), and atrial fibrillation (3%) (Table 2). There were 72 dislocations (71 THA, 1 patellar dislocation after TKA) within 90 days of surgery that resulted in an inpatient stay, with an average cost of $53 203 (SD = $37 571). The rate of THA dislocation that resulted in a readmission was 0.8% (71/9139); 58% (42/72) of admissions for dislocations included a return to the OR.
There were 64 inpatient stays for PJI, resulting in an overall PJI rate of 0.3% (64/20 166). Periprosthetic joint infection was more common after TKA than THA (0.4% vs 0.3% incidence rate). Admission for PJI was on average 11.2 (9.9) days long and cost $132 676 (102 644); 86% (55/64) of PJI admissions included a return to the OR.
There were 64 inpatient stays for a PPFx, occurring more commonly after THA than TKA (0.6% vs 0.05%). Admissions for PPFx were on average 7.6 (6.1) days long and cost $100 845 (61 233); 81% (52/64) of PPFx admissions included a return to the OR. Of the 52/59 THA PPFx with available X-rays, 71% were classified as Vancouver B2, 15% were AG/L 6% were B1, 4% were C, 2% were B3, and 2% were acetabular fractures. All PPFxs occurred in uncemented THA.
There were 42 inpatient stays for cellulitis and 40 inpatient stays for atrial fibrillation. They both occurred more commonly after TKA than THA (0.3% incidence rate). The average cost of admission was $28 478 for cellulitis and $45 651 for atrial fibrillation.
There were 163 revisions within 90 days of primary TJA, for an overall 0.8% revision rate (Table 3). Seventy-six percent of revisions occurred after THA, resulting in a THA revision rate of 1.4% and a TKA revision rate of 0.4%. Revisions were most common in White women, and 77% of patients who required a revision had a major comorbidity, such as acute heart, renal, or respiratory failure. The most common reasons for revision were PJI (34%), PPFx (32%), dislocation (26%), loosening (7%), arthrofibrosis (1%), and limb length discrepancy (1%). For PJIs, 75% (41/55) were treated with debridement, antibiotics, and implant retention (DAIR), and 22% were treated with debridement and implant removal and antibiotic spacer placement, as part of a 2-stage revision; 3% were treated with 1-stage revision. The mean time to readmission for all 163 patients who required a revision was 39 (23.4) days. The average length of stay was 7.7 (7.6) days, and a majority of patients were discharged home (56%). The mean cost of the revision claim was $105 988 (SD $76 865).
Revisions within 90 days.
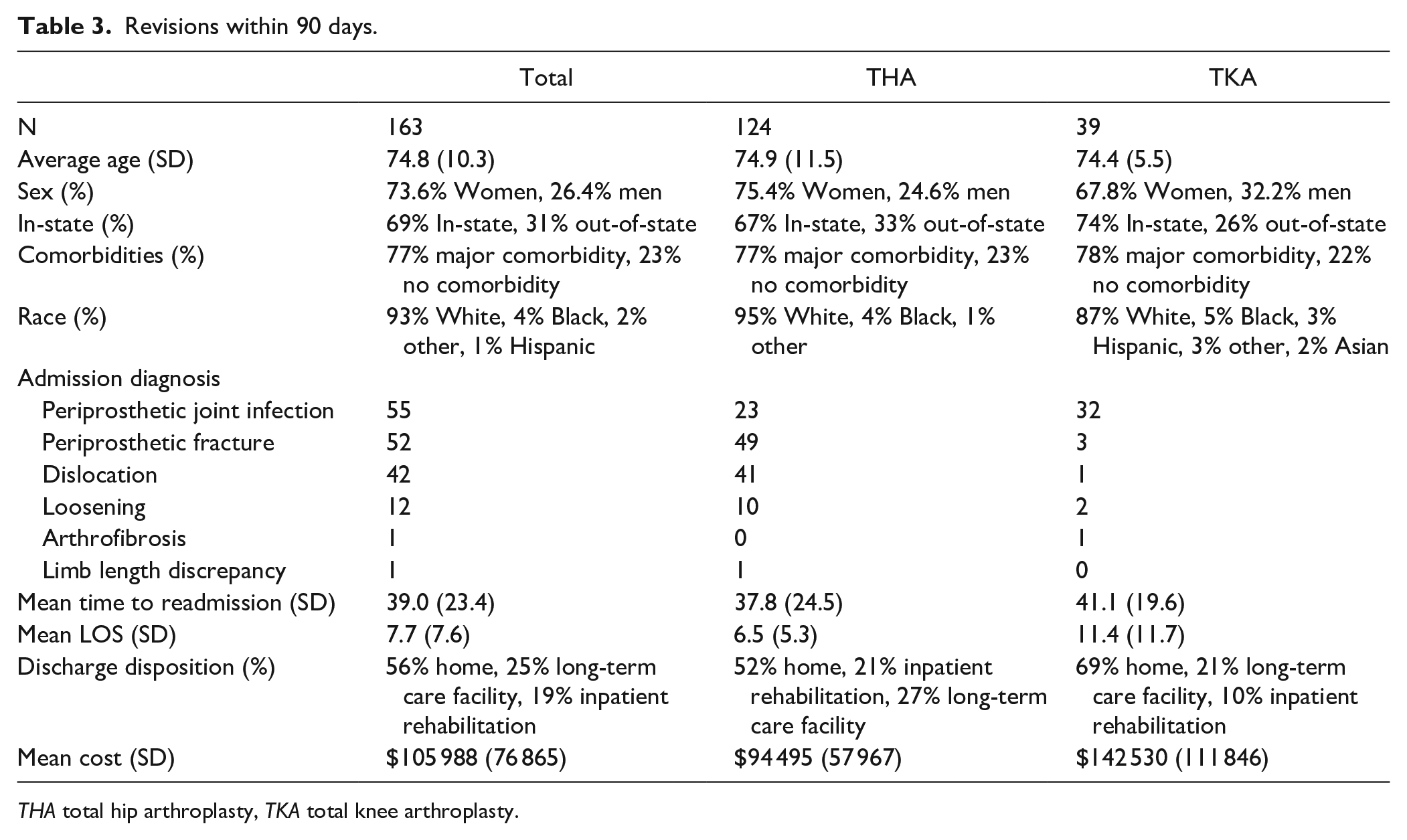
THA total hip arthroplasty, TKA total knee arthroplasty.
Univariate analysis of readmissions demonstrated a significant association between readmission and the following covariates: length of stay, age, sex, discharge location, presence of a major comorbidity, and date of surgery before or after policy change (CJR initiative implementation in 2016). Race, whether the patient lived in-state, and type of surgery (THA vs TKA) were not associated with readmission. All covariates were advanced into the multivariate logistic regression. The regression demonstrated an association between readmission and older age, longer length of stay, discharge to a care facility, presence of a major comorbidity, and female sex (Table 4).
Multivariate analysis.
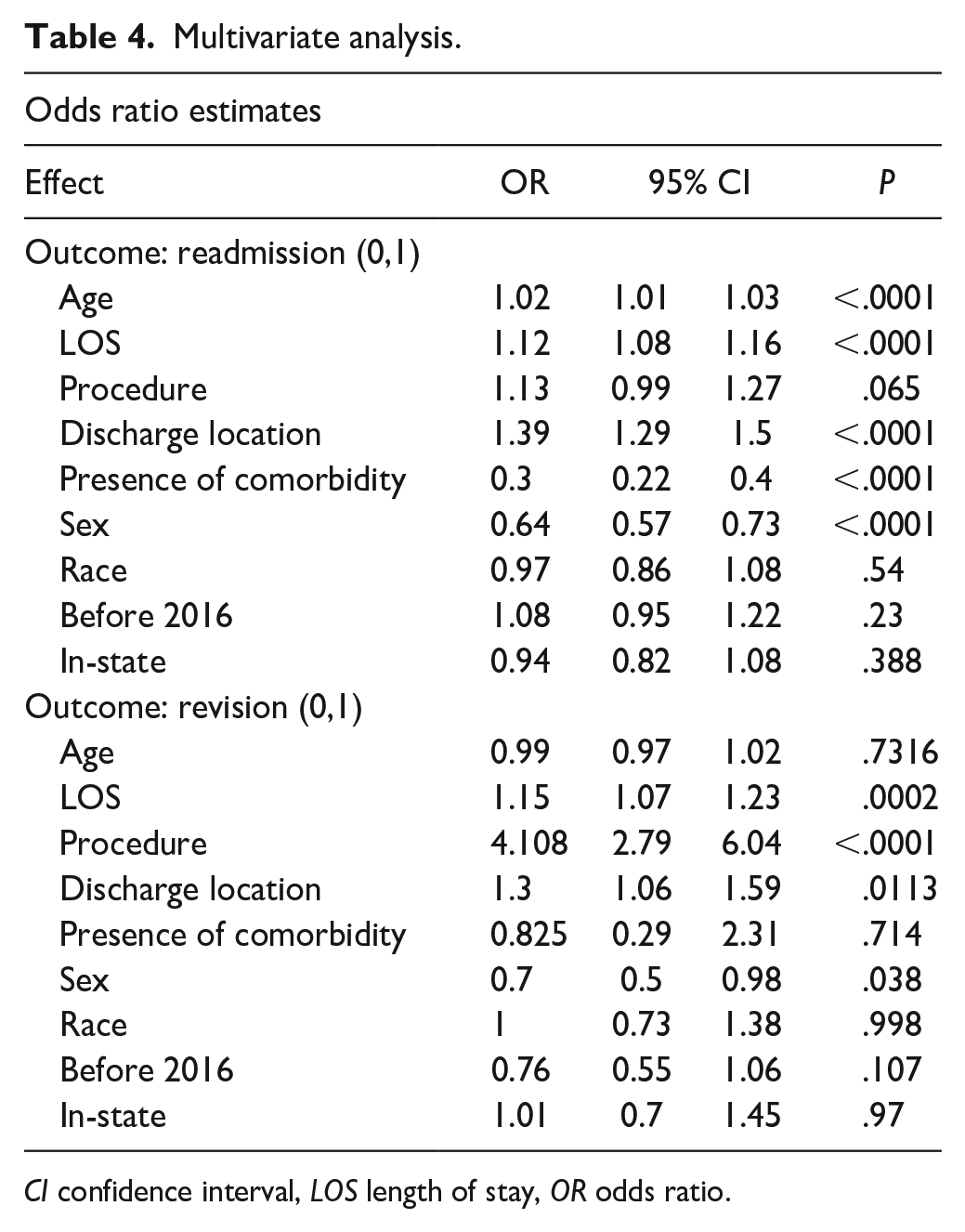
CI confidence interval, LOS length of stay, OR odds ratio.
Univariate analysis of revisions demonstrated a significant association between procedure type and revision, as revisions were more common after THA than TKA. There was also an association with the presence of a major comorbidity. Univariate analysis did not demonstrate an association with revision and the following variables: age, sex, length of stay, discharge location, in-state address, or date of surgery before or after policy change. All covariates were advanced into the multivariate logistic regression. The regression demonstrated an association between revision and length of stay, procedure type, sex, and discharge location. Specifically, a longer length of stay, THA, female sex, and discharge to long-term care facility were associated with a revision procedure (Table 4).
Discussion
Because of the introduction of bundled-payment structures, all-cause hospital readmission is an important marker of care quality for TJA, resulting in a research push to identify patients at risk of early readmissions. Nonetheless, there has been a paucity of data on early reoperations and their associated costs. We sought to better understand the causes and costs of 90-day readmissions and revisions after TJA at 1 institution. We found that dislocation was the most common indication for readmission and periprosthetic joint infection was the most common indication for revision. Also, we identified patient demographics and postoperative variables associated with both early readmission and revision. Finally, we calculated costs associated with early return to the hospital.
There are several limitations of this study. We relied on the accuracy of the ICD-CM codes that were reported to CMS to determine the cause of readmission. Previous studies have noted the high frequency of misclassifications in this database [8,25]. However, for the cohort of revision patients, we mitigated this potential cause of error by cross-checking the patient’s electronic medical record to confirm the diagnosis and revision procedure. In addition, we denoted the presence of a major comorbidity as defined by Medicare’s DRG 469 code (Centers for Medicare and Medicaid services), resulting in a likely underestimation given the lack of medical history details. Also, we included patients from only 1 institution, limiting the generalizability of the findings; readmission rate and cost burden may differ at other hospitals. Moreover, we reported hospital claim data submitted to CMS and not CMS reimbursements, as these data were not available. However, previous studies have illustrated the difference between hospital charges for a primary TJA ($49 726 in the Northeast) and CMS reimbursements ($12 844) [23]. Furthermore, we included no data on non-Medicare patients and therefore could not compare how insurance level may affect readmission and revision rates. Finally, we did not include outpatient costs, such as physical therapy visits, thus likely underestimating the overall cost burden.
Our study identified a readmission rate of 5.6% after both THA and TKA. The cost of readmissions after THA averaged $63 452 (57 337), whereas the cost of readmissions after TKA averaged $61 050 (64 536). The most common reasons for readmissions were dislocations ($52 526) for THA and infection ($138 442) for TKA. Clair et al [7] conducted a retrospective review of CMS claims at 1 institution and reported a 90-day readmission rate of 10% and at an average cost of $36 038 (range = $6375 to $60 137) for THA and $38 953 (range = $4790 to $104 794) for TKA, with infection as the most common reason. Other studies have reported 90-day readmission rates ranging from 0% to 32%, with the average near 10% [16,21,22,34]. Our readmission rate (5.6%) and average cost ($62 173) fall within this range.
Previous studies have also reported dislocation as the most common reason for readmission after THA [16]. Mantel et al [26] analyzed Medicare claims for dislocations after THA and reported a 1.7% 1-year dislocation rate with an increase in costs of $20 000. Other literature has reported an increase in costs ranging from 19% to 342% [11,14,33]. Our dislocation rate of 0.8% is lower than that reported in the literature, although we report a shorter 90-day window as opposed to a 1-year timeline. In addition, our higher readmission cost ($53 203) reflects that 58% of claims include a return to the OR.
We found the most common reason for TKA readmission was infection, at an average cost of $138 442 (117 779) and an overall infection rate of 0.3%. This aligns with Curtis et al [9], who used a national database to report a 30-day readmission rate after TKA of 3.2%, with the most common reason listed as surgical site infection. Cost analysis of 90-day readmissions after TKA is limited, but Chan et al [5] utilized state inpatient data to report an average 90-day readmission cost of $9335 ($10 527), compared with our average overall cost of $61 050. However, they did not specify the reasons for readmission. Focusing on the economic burden of PJI, Premkumar et al [28] estimated a $28 161 (27 262-29 061) mean cost per case of infected TKA in 2018. These values are drastically lower than our results, which suggest a difference in cost calculation or sample size effect (they identified 18 000 infected TKA cases in a national database). They do not report how many of those cases required a costly reoperation, whereas we found 86% of patients returned to the OR.
Multiple studies have identified predictors for readmission after both THA and TKA, including insurance status (higher in Medicare patients), discharge disposition, and sex (higher in men) [1,10,22,38,39]. In our cohort of Medicare patients, older age, longer length of stay, discharge to a care facility, presence of a major comorbidity, and female sex were associated with readmission. Most of these factors may indicate a higher level of frailty, which may place patients at risk of postoperative complications.
There is limited literature on early reoperations after THA or TKA. George et al reported reoperation rates of 2.1% 30-day for THA and 1.2% for TKA, specifying that THA patients had a higher rate of reoperation but not the indications or costs [15]. To our knowledge, our study is the first to delineate the rate, cause, and cost of early reoperations after TJA. Although our overall 90-day reoperation rate was lower (0.8%), the average additional cost, $105 998 (76 865), increased the overall 90-day cost by 260%. These rare but costly events were mostly due to PJI and PPFx occurring within a month of surgery. In our cohort, factors associated with a higher risk of reoperation were female sex, THA, longer length of stay, and discharge to long-term care facility.
In conclusion, this study highlights the cost burden of readmissions and reoperations within 90 days after TJA in a Medicare population, substantiating prior work on readmissions and adding new information on reoperations. Delineating the causes and costs of readmissions and reoperations can help surgeons and institutions identify patients who may be at high risk and improve the quality of care delivered. We found that female sex, longer length of stay, and discharge to a care facility were associated with readmission and reoperation. Further research on the Medicare population, which has a higher risk of readmission, can delve into prolonged length of stay and discharge to a facility and whether risk factors can be modified. Also needed are studies on postoperative emergency department visits to determine how often patients present, why, and how they are triaged.
Supplemental Material
sj-docx-1-hss-10.1177_15563316241230052 – Supplemental material for Early Readmission and Revision After Total Joint Arthroplasty: An Analysis of Cause and Cost
Supplemental material, sj-docx-1-hss-10.1177_15563316241230052 for Early Readmission and Revision After Total Joint Arthroplasty: An Analysis of Cause and Cost by Jennifer Bido, Ricardo Torres, Austin C. Kaidi, Samuel Rodriguez and Jose A. Rodriguez in HSS Journal®
Supplemental Material
sj-docx-2-hss-10.1177_15563316241230052 – Supplemental material for Early Readmission and Revision After Total Joint Arthroplasty: An Analysis of Cause and Cost
Supplemental material, sj-docx-2-hss-10.1177_15563316241230052 for Early Readmission and Revision After Total Joint Arthroplasty: An Analysis of Cause and Cost by Jennifer Bido, Ricardo Torres, Austin C. Kaidi, Samuel Rodriguez and Jose A. Rodriguez in HSS Journal®
Supplemental Material
sj-docx-3-hss-10.1177_15563316241230052 – Supplemental material for Early Readmission and Revision After Total Joint Arthroplasty: An Analysis of Cause and Cost
Supplemental material, sj-docx-3-hss-10.1177_15563316241230052 for Early Readmission and Revision After Total Joint Arthroplasty: An Analysis of Cause and Cost by Jennifer Bido, Ricardo Torres, Austin C. Kaidi, Samuel Rodriguez and Jose A. Rodriguez in HSS Journal®
Supplemental Material
sj-docx-4-hss-10.1177_15563316241230052 – Supplemental material for Early Readmission and Revision After Total Joint Arthroplasty: An Analysis of Cause and Cost
Supplemental material, sj-docx-4-hss-10.1177_15563316241230052 for Early Readmission and Revision After Total Joint Arthroplasty: An Analysis of Cause and Cost by Jennifer Bido, Ricardo Torres, Austin C. Kaidi, Samuel Rodriguez and Jose A. Rodriguez in HSS Journal®
Supplemental Material
sj-docx-5-hss-10.1177_15563316241230052 – Supplemental material for Early Readmission and Revision After Total Joint Arthroplasty: An Analysis of Cause and Cost
Supplemental material, sj-docx-5-hss-10.1177_15563316241230052 for Early Readmission and Revision After Total Joint Arthroplasty: An Analysis of Cause and Cost by Jennifer Bido, Ricardo Torres, Austin C. Kaidi, Samuel Rodriguez and Jose A. Rodriguez in HSS Journal®
Footnotes
CME Credit
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: J.A.R., MD, reports relationships with Conformis, Exactech, Medacta, and Smith & Nephew. The other authors declared no potential conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human/Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
Informed Consent
Informed consent was waived from all patients included in this study.
Level of Evidence
Level IV, therapeutic and economic analysis.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.