
Abstract
Background:
Post-acute care for orthopedic surgery patients continues to evolve with the reduction in hospital length of stay (LOS), shift to ambulatory surgery, increased number of surgeries, and focus on value-based care.
Purpose:
We sought to examine outcomes of a cohort of lower-extremity arthroplasty patients receiving telephysical therapy (TelePT) according to hospital LOS, as a means of exploring the viability of TelePT as a value-based discharge option.
Methods:
A retrospective review was conducted of patients who participated in our institution’s HSS@Home TelePT program after undergoing primary unilateral hip or knee arthroplasty, unicondylar knee replacement, or hip resurfacing. Demographic data and outcomes such as hospital LOS, number of days between discharge and TelePT evaluation, number of TelePT visits, number of re-admissions, Hip dysfunction and Osteoarthritis Outcome (HOOS Jr.) or Knee injury and Osteoarthritis Outcome (KOOS Jr.) scores, and patient satisfaction scores were collected. Patients were divided into categories based on hospital LOS to help determine the versatility of program.
Results:
In the 2814 patients included, we observed an average of 4.1 TelePT visits; 1% of patients were readmitted within 90 days, and 97% of patients were satisfied or highly satisfied. There was no difference in HOOS or KOOS Jr. scores at each follow-up time point, except for the 6-month HOOS Jr. scores.
Conclusion:
This retrospective study suggests that TelePT may be a viable option for care of lower-extremity arthroplasty patients in the post-acute setting, regardless of hospital LOS. As a discharge option, it may meet the needs of select patients to fill a gap in providing value-based care.
Keywords
Introduction
Lower-extremity arthroplasty procedures, including total hip (THA) and total knee (TKA) arthroplasty, are high-volume surgeries that have seen many changes in postoperative course of care. In the recent past, THA and TKA were inpatient-only procedures, requiring multiple night hospital stays, but they have since shifted to include ambulatory surgery (AMS) options; THA and TKA were removed from the inpatient-only list in 2020 and 2018, respectively [2,4]. Postoperative physical therapy (PT) needs have also shifted, from facility-based acute and sub-acute rehabilitation to predominantly home care or outpatient PT [1]. Surgical volume for THA and TKA continues to increase and is expected to grow substantially by 2030 [10, 20, 21]. Accompanying these changes are alternative practice models and value-based care initiatives such as Bundled Payments for Care Improvement (BPCI) and Comprehensive Care for Joint Replacement (CJR), which have demonstrated reduced costs in the post-acute period [1].
With the shift to AMS, shorter lengths of stay (LOS), increasing arthroplasty numbers, and a focus on value-based care, health care leaders need to carefully and strategically consider options for postoperative care that combine quality with judicious use of resources that best meet patients’ needs.
Home discharges are typically less expensive than acute or sub-acute rehabilitation and have similar outcomes [1,20,22]. With the transition to ambulatory surgeries and shorter LOS, total joint arthroplasty (TJA) patients are also being discharged home more acutely. Same-day discharges have increased from 1% to 21% between 2011 and 2015 [5] and have since continued to increase [16]. The percentage of same-day discharges at our hospital increased from 19% in 2020 to 45% in 2022 and to over 50% in the first quarter of 2023. The shift to shorter hospital stays may require more timely access to care and clinical communication among the patient, the hospital team, and post-acute care provider.
For some patients, traditional home care PT is not an ideal option due to changes in home care PT reimbursement design. The Low Utilization Payment Adjustment (LUPA) reimburses home care agencies at a lower rate when patients receive less than 6 visits for a 30-day period [3]. This incentivizes home care PT to provide 6 or more visits for any TJA patient, even when more than 6 visits are not clinically indicated. This is especially true for higher functioning patients who have fewer comorbidities and qualify for AMS. This gap in the current system results in higher costs, affecting the value of care provided for patients whose PT needs can be met in fewer visits.
To address this gap, our institution, HSS, piloted a telephysical therapy (TelePT) program in 2019 called HSS@Home, which provided TelePT for a specific cohort of TJA patients, with results suggesting it may be a promising alternative to home health PT [7]. Other studies published in 2015, 2019, and 2020 also demonstrated positive results for TelePT for TKA and THA patients [8,17,18].
In 2020, the COVID-19 pandemic fueled the expansion of HSS@Home from a pilot program to a standard discharge option for TJA patients at our institution. The program grew from 1400 TelePT visits in 2019 to over 7000 in 2020 and over 6000 in both 2021 and 2022. The literature has similarly demonstrated continued growth of TelePT along with positive outcomes of being clinically effective, cost effective, safe, and satisfactory to patients [11,14].
In continued anticipation of increases in surgical volume, AMS, shorter LOS, and emphasis on value-based care, it is important to examine the continued effectiveness of TelePT on addressing patients’ post-acute needs. We therefore sought to describe a cohort of lower-extremity arthroplasty patients receiving TelePT services during a 2-year period, examine outcomes according to hospital LOS, and explore the viability of TelePT as an ongoing, value-based discharge option.
Methods
This retrospective cohort study was approved by our institutional review board and conducted in an urban orthopedic hospital that supports elective surgery. All patients evaluated by the HSS@Home TelePT program between January 1, 2021, and December 31, 2022, after undergoing primary unilateral TKA or THA, unicondylar knee replacement, or hip resurfacing were included. Nonarthroplasty or revision surgery patients and those with evaluation dates prior to 2021 and after 2022 were excluded.
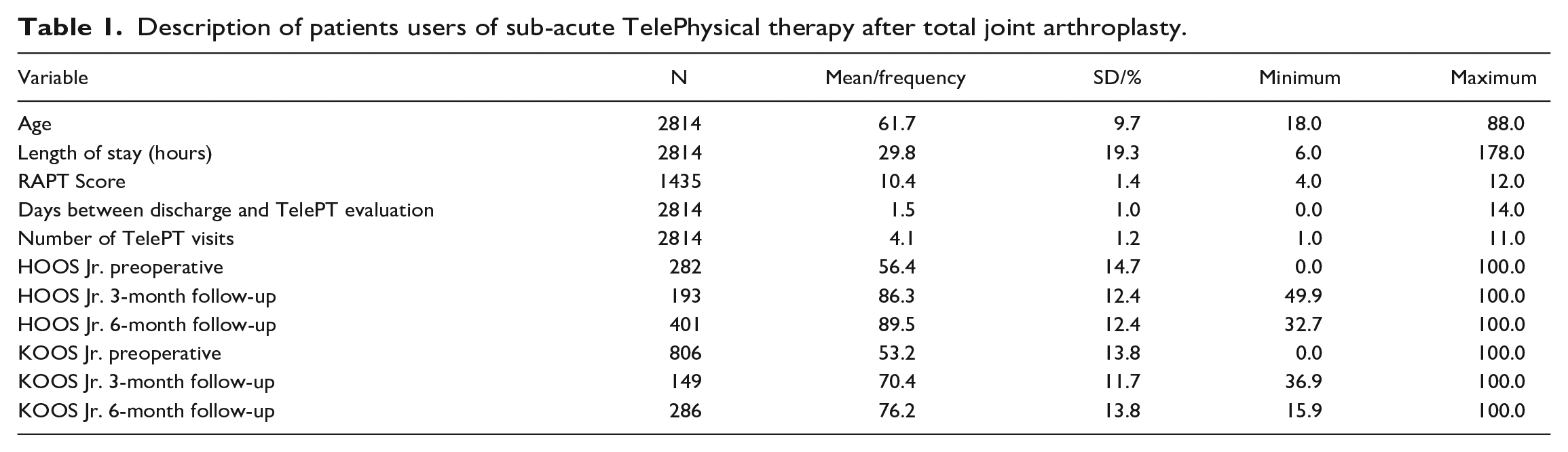
A total of 2814 patients met the inclusion criteria. The mean age of the study population at the time of surgery was 61.7 ± 9.7 years (range 18–88); 47% were female. The mean LOS was 29.8 hours (range 6–178 hours). Patients had an average of 4.1 TelePT visits (range 1–11 sessions). In this study, 55% of patients were THA cases with 25% scheduled as an AMS. Most patients were from New York (64%) or New Jersey (25%) (Table 1).
Description of patients users of sub-acute TelePhysical therapy after total joint arthroplasty.
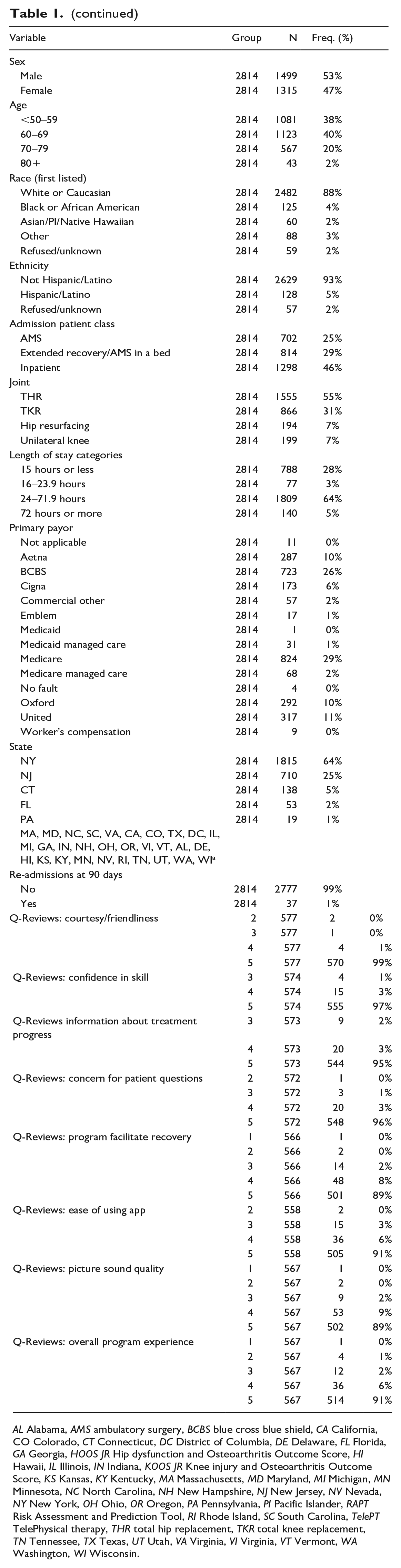
AL Alabama, AMS ambulatory surgery, BCBS blue cross blue shield, CA California, CO Colorado, CT Connecticut, DC District of Columbia, DE Delaware, FL Florida, GA Georgia, HOOS JR Hip dysfunction and Osteoarthritis Outcome Score, HI Hawaii, IL Illinois, IN Indiana, KOOS JR Knee injury and Osteoarthritis Outcome Score, KS Kansas, KY Kentucky, MA Massachusetts, MD Maryland, MI Michigan, MN Minnesota, NC North Carolina, NH New Hampshire, NJ New Jersey, NV Nevada, NY New York, OH Ohio, OR Oregon, PA Pennsylvania, PI Pacific Islander, RAPT Risk Assessment and Prediction Tool, RI Rhode Island, SC South Carolina, TelePT TelePhysical therapy, THR total hip replacement, TKR total knee replacement, TN Tennessee, TX Texas, UT Utah, VA Virginia, VI Virginia, VT Vermont, WA Washington, WI Wisconsin.
A discharge plan of TelePT was determined with the patient, physical therapist, and/or social worker during the preoperative discharge planning process. This included verifying postoperative PT benefits, assessing mobility and psychosocial status, and identifying any other post-acute needs. The Risk Assessment and Prediction Tool (RAPT) was administered to help predict the type of post-acute needs required. The tool suggests a score below 6 is high risk for needing inpatient rehab after TJA, while a score between 6 and 9 would recommend a patient as appropriate for home care PT-level services [19]. The therapist used the information from the assessment and the RAPT score to best align the discharge plan with each patient’s needs. The discharge plan was confirmed or altered in the hospital postoperatively based on the surgery outcome and patient status at the time of discharge.
TelePT visits were scheduled for the first or second day after hospital discharge. Patients used their own personal device (computer, smartphone, or tablet) to access the TelePT visit through the electronic health record (EHR) patient portal. The device used for the session must have internet/mobile network access, a camera, and a microphone for the patient to participate in a TelePT session. All TelePT video visits were 1:1 live, synchronous sessions.
The first visit was a PT evaluation consisting of subjective and objective review of patient status with an emphasis on medical status, medication usage, incision observation, and bowel status. At the evaluation and subsequent TelePT visits, the physical therapist performed live clinical interventions covering aspects of care such as therapeutic exercise, functional mobility, self-care home management, and patient and family education. Any clinical question or need outside of the scope of practice for the therapist was routed to the post-acute nurse practitioner or surgeon for follow-up. Therapists collaborated with patients to determine how many visits were needed prior to program discharge to the next level of care (outpatient PT or surgeon follow-up with home exercise program). Patients received a text-based patient satisfaction survey upon discharge from the program. The Hip dysfunction and Osteoarthritis Outcome Score (HOOS Jr.) and the Knee injury and Osteoarthritis Outcome Score (KOOS Jr.) are the patient-reported outcome measures (PROMs) that were administered to all lower-extremity arthroplasty patients preoperatively and after surgery as standard of care. These disease-specific outcome measures contain 6 (HOOS Jr.) or 7 (KOOS Jr.) questions, with scores ranging from 0 (total hip or knee disability) to 100 (good hip or knee health). Both PROMs were validated and have shown strong measurement properties with this patient population [12,13].
Data were retrieved retrospectively from the EHR of patients meeting the inclusion criteria. Demographic data including patient age, sex, gender identity, ethnicity, race, state, primary insurance payor, joint replaced, admission status (AMS, extended recovery, inpatient), and RAPT score were collected. The following outcomes were also collected: hospital LOS, number of days between discharge and TelePT evaluation, number of TelePT visits, number of re-admissions, HOOS Jr./KOOS Jr. scores, and patient satisfaction scores (Q-Review scores).
Means and standard deviations were used to describe continuous variables and frequencies, and percentages were used to describe categorical variables for patient demographics and outcomes (HOOS/KOOS Jr. scores, 90-day re-admission, and Q-Review scores).
Further analysis was conducted to study the impact of LOS on patient outcomes. Patients were categorized into 4 LOS categories: AMS, 15 hours or less (AMS); ambulatory surgery overnight, 16 to 23.9 hours (AMS-overnight); inpatient, 24 to 71.9 hours (INPT); and inpatient with an extended stay, 72 hours or more (INPT-EXT). Outcomes were examined using these categories to determine the viability and versatility of TelePT. One-way analysis of variance (ANOVA) was used to compare all continuous data elements, while χ2 tests were used to compare the percentage of the categorical variables between the study groups, including the outcomes of 90-day re-admission and Q-Review scores. Tukey correction was used to adjust for potential Type I error in all pairwise comparisons. All analyses were performed using SPSS version 23.0 (IBM Corp).
Results
Overall, 37 patients (1%) of the study population were readmitted to the hospital within 90 days. All questions from the Q-Review survey had a 90% or greater response rate of 4 or 5. For the overall program experience question, 97% of patients responded with a satisfied (6%) or very satisfied (91%) response. Mean HOOS and KOOS Jr. scores at 3 months were 86.3 and 70.4, respectively. At 6 months after the procedure, HOOS and KOOS Jr. scores were 89.5 and 76.2, respectively. (Patient-Acceptable Symptom States [PASS] are 76.7 for HOOS Jr. and 63.7 for KOOS Jr. [9].)
A comparison of patient characteristics and outcomes by LOS categories is reported in Supplemental Table 1. There were statistically significant differences in patient age (P < .001), RAPT score (P < .001), and time from hospital discharge to TelePT evaluation (P < .001) among the LOS groups. Patients in the 15 hours or less group were younger and had higher RAPT scores yet had a longer wait from discharge to TelePT evaluation. Time from hospital discharge to TelePT evaluation was significant among the groups overall (P ≤ .001), but the mean duration was still under 2 days for all LOS groups. There was no difference in the number of TelePT visits between the LOS groups (P = .090).
There was no difference in the HOOS or KOOS Jr. scores at any of the follow-up time points, except for the 6-month HOOS Jr. scores. Post-hoc analysis found that patients in the 72-hour or longer group had significantly lower HOOS Jr. scores than the 24- to 72-hour category of patients (78.1 ± 20.2 vs 89.5 ± 12.2, P = .003) and ≤15 hours (78.1 ± 20.2 vs 91.1 ± 10.6, P = .001). For the Q-Review score, “Overall Program Experience” demonstrated no significant difference between groups (P = .905). The only Q-Review item that was statistically significant was “Courtesy and Friendliness” (P = .030); the 16- to 23.9-hour stay group was lower than the 24- to 71.9-hour group (P = .001). However, while statistically significant, 95% of 16- to 23.9-hour stay patients still responded with 4 or 5, a response of satisfied or very satisfied.
Discussion
Post-acute care after orthopedic surgery requires strategic and effective use of health care resources, particularly in light of a growing number of patients undergoing lower-extremity arthroplasty and shortening of hospital LOS. Our findings demonstrate that the use of TelePT sessions after hospital discharge could safely and effectively bridge care in that interim phase until patients were ready to attend outpatient therapy or continue with a home exercise program and physician follow-up, as evidenced by the positive results for the outcome measures collected.
The strengths of this study lie in the opportunity to examine outcomes of over 2800 patients who have used TelePT after lower-extremity arthroplasty. The limitations of this study include using data collected retrospectively and using only data recorded in the EHR. Missing or incomplete items, such as RAPT and PROMs scores, impact data analysis. Another limitation is the challenge in generalizing our findings. Our institution is a specialty hospital with a high volume of orthopedic surgeries, and results may not relate to hospitals with lower surgical volumes and more diverse patient populations. Another challenge to the generalizability of these findings is our standard of care of prescribing home care PT, even for patients with a RAPT score greater than 9. The average RAPT score of the patients in our study was 10.4 (range of 4–12), and a score of 10 or greater generally indicates home discharge without intervention in the home. Lastly, our breakdown of hospital LOS categories accounted for our unique patient population and operational design. This breakdown may not be generalizable to other organizations. Of note, this TelePT program is used for other procedures including but not limited to revision and bilateral arthroplasty, reimplantation, and spine procedures, among others. For this study, we focused on primary lower-extremity arthroplasty. Future studies can examine the outcomes of TelePT for patients undergoing other surgical procedures.
From a clinical outcome perspective, PROMs were not significantly different across categories with the exception for the 6-month HOOS Jr. However, while the score was significantly lower, it should be noted that the average score at 6 months in that group (mean 78.1) did meet the previously published PASS, which was reported as 76.7 [9]. When all mean outcomes are compared to established norms, all are above the PASS and documented norms for those timeframes [9]. This study is also consistent with other findings in the literature in which TelePT has shown to provide comparable PROM scores to in-person PT for THA and TKA patients [8,11]. This indicates that regardless of hospital LOS, TelePT provided clinically meaningful outcomes.
Concerns have been raised about the impact of reduced number of visits on patient safety, outcomes, and satisfaction. We averaged 4.1 visits per patient, with the number of visits not differing significantly for each LOS category. With this reduced number of visits, we found a 1% re-admission rate, which is less than that previously reported in the literature, ranging from 1.8% to 9% [15].
TelePT is situated to provide fewer visits than home care PT per patient for each LOS category because of the LUPA design, which requires 6 visits [3]. Falvey suggests 6 to 9 home care PT visits are optimal for TKA patients, which is more than the average number of visits used by our cohort [6]. TelePT has the ability to provide the clinically necessary number of visits to patients. In comparison, home care PT is of lesser overall value with significantly higher costs with comparable rates of complications, re-admissions, and emergency department visits [1]. McKeon reported in a systemic review that telerehabilitation was significantly less costly than in-person PT [14]. Lower visit utilization is cost-effective and in alignment with value-based care.
Patients were able to access TelePT services in a timely manner, with evaluations taking place an average of 1.5 days after hospital discharge. Timely access to care supports patients during recovery and facilitates timely remediation of issues that arise. Patient satisfaction results indicated 97% of patients scoring the program a 4 or 5 out of 5 for overall program experience. High patient satisfaction is consistent with outcomes in the literature for TelePT [8,14,22].
Consistent with our expectations, RAPT scores decreased as hospital LOS increased, while as hospital LOS increased, so did patient age. The longer the hospital stay, the older and more reliant the patient was on post-acute services.
We observed some differences between the LOS groups (age, sex, RAPT scores), but patients achieved clinically meaningful improvements and positive results for all outcome measures, regardless of hospital LOS. This study supports TelePT as a potential option and aligns with evidence suggesting that TelePT can be comparable to in-person care with lower costs [14,22].
This study is a follow-up to a case series piloting our TelePT program [7]. That study recommended directions for growth and future research suggesting the use of PROMs at designated time points to track effectiveness, satisfaction, and long-term outcomes and expanding the program to include patients covered by commercial payers. This current study incorporates those recommendations, allowing for a multifaceted look at the viability of implementing a TelePT program on a larger scale with an examination of outcomes measures.
In conclusion, our retrospective cohort study suggests that TelePT in the post-acute setting may be a viable option for care of lower-extremity arthroplasty patients, including those in all LOS categories. Future research should include a comparative, prospective design with a sample size determined by power analysis comparing various outcomes of TelePT to home care PT.
Supplemental Material
sj-docx-1-hss-10.1177_15563316231210865 – Supplemental material for Scaled TelePhysical Therapy Program a Promising Option for Post-acute Care of Lower-Extremity Arthroplasty Patients
Supplemental material, sj-docx-1-hss-10.1177_15563316231210865 for Scaled TelePhysical Therapy Program a Promising Option for Post-acute Care of Lower-Extremity Arthroplasty Patients by Charles Fisher, Catherine Wysin, Lauren Moeller and Joseph Nguyen in HSS Journal®
Supplemental Material
sj-docx-2-hss-10.1177_15563316231210865 – Supplemental material for Scaled TelePhysical Therapy Program a Promising Option for Post-acute Care of Lower-Extremity Arthroplasty Patients
Supplemental material, sj-docx-2-hss-10.1177_15563316231210865 for Scaled TelePhysical Therapy Program a Promising Option for Post-acute Care of Lower-Extremity Arthroplasty Patients by Charles Fisher, Catherine Wysin, Lauren Moeller and Joseph Nguyen in HSS Journal®
Supplemental Material
sj-docx-3-hss-10.1177_15563316231210865 – Supplemental material for Scaled TelePhysical Therapy Program a Promising Option for Post-acute Care of Lower-Extremity Arthroplasty Patients
Supplemental material, sj-docx-3-hss-10.1177_15563316231210865 for Scaled TelePhysical Therapy Program a Promising Option for Post-acute Care of Lower-Extremity Arthroplasty Patients by Charles Fisher, Catherine Wysin, Lauren Moeller and Joseph Nguyen in HSS Journal®
Supplemental Material
sj-docx-4-hss-10.1177_15563316231210865 – Supplemental material for Scaled TelePhysical Therapy Program a Promising Option for Post-acute Care of Lower-Extremity Arthroplasty Patients
Supplemental material, sj-docx-4-hss-10.1177_15563316231210865 for Scaled TelePhysical Therapy Program a Promising Option for Post-acute Care of Lower-Extremity Arthroplasty Patients by Charles Fisher, Catherine Wysin, Lauren Moeller and Joseph Nguyen in HSS Journal®
Supplemental Material
sj-docx-5-hss-10.1177_15563316231210865 – Supplemental material for Scaled TelePhysical Therapy Program a Promising Option for Post-acute Care of Lower-Extremity Arthroplasty Patients
Supplemental material, sj-docx-5-hss-10.1177_15563316231210865 for Scaled TelePhysical Therapy Program a Promising Option for Post-acute Care of Lower-Extremity Arthroplasty Patients by Charles Fisher, Catherine Wysin, Lauren Moeller and Joseph Nguyen in HSS Journal®
Footnotes
Declaration of Conflicting Interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Joseph Nguyen, MPH, declares relationships with the American Journal of Sports Medicine and the Journal of Women’s Sports Medicine. The other authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human/Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
Informed Consent
Informed consent was waived from all patients included in this study.
Level of Evidence
Level IV, retrospective therapeutic study
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.