
Abstract
Background:
Advancements in surgical procedures for total joint arthroplasty (TJA) have resulted in more effective procedures with more rapid recovery. To prepare patients for surgery, many organizations offer a preoperative “joint class,” which has been associated with reduced length of stay (LOS). Virtual modes of education are increasingly favored for those having TJA.
Purpose:
To determine whether participation in an individually administered preoperative educational session (“Prehab”) relates to reduced LOS or increased likelihood of same-day discharge (SDD) for those undergoing TJA. Additionally, to establish whether and the virtual mode of education provision is superior or inferior to the in-person mode with regards to LOS benefits.
Methods:
The author conducted a case-control study of 2532 patients who had a primary or revision TJA between January 2022 and August 2022 at a single institution. Data were obtained from the electronic medical record. A total of 1118 patients attended Prehab; 1414 patients did not. Patients were included if they were over the age of 18 and had a total hip arthroplasty (THA) or total knee arthroplasty (TKA) during the study period. T-tests, chi-square χ2 tests, and binomial logistic regression were used to evaluate the LOS and SDD outcomes for those who participated in Prehab compared with those who did not.
Results:
Those receiving Prehab in any form had shorter LOS than those who had not. Those receiving virtual Prehab had the shortest LOS. There was no difference in the rate of SDD for outpatient-class patients.
Conclusion:
Preoperative education is associated with LOS benefits to patients undergoing TJA. The virtual mode of education provision is at minimum non-inferior, and may be superior, to the in-person mode. The lack of statistically significant between-group differences for SDD outcomes may be explained by a lack of SDD-specific educational content provided during Prehab.
Keywords
Introduction
Over 1 million total knee arthroplasty (TKA) and total hip arthroplasty (THA) (referred to collectively as total joint arthroplasty or TJA) procedures are performed every year [8]; these are the most commonly performed surgical procedures covered by Medicare [17]. Advancements in surgical procedures and clinical pathways for TJA have created safer, more efficient, and more effective procedures, which have resulted in a more rapid recovery for many patients [1,29,32]. In fact, a typical hospital length of stay (LOS) is between 2 and 4 days [29,32]. Outpatient TJA is increasingly common [3,12,25]. Defined as requiring a hospital stay of less than 24 hours, outpatient TJA may include a stay of 1 midnight [4], although some may be discharged on the same day of surgery [1,2,3,6,29,32]. Investigators have identified distinct patient management components deemed essential for successful execution of outpatient TJA, which include careful patient selection and screening [3,9,19], preoperative patient/family education, perioperative multidisciplinary coordination, and early and effective post-discharge planning [19].
The provision of enhanced education in preparation for TJA is well-established as a method of improving TJA outcomes [14,16]; in fact, the American Academy of Orthopedic Surgeons considered such education to be essential for successful outpatient TJA [20]. As an alternative to written educational materials or phone calls, many programs offer preoperative education classes to prepare patients for TJA, aimed at aligning physician and patient expectations for the postoperative period. Frequently, education classes are offered to patients in groups where multiple patients receive the same or similar information all at once [11,13,18,21,27,28,30]. Session content can vary considerably across sites and populations. Topics covered have been documented to include preoperative preparation, expectations for the postoperative period, discharge instructions, activities of daily living after surgery, goal setting, expectations regarding recovery [11,13,18,23,27,28,30], nutrition/diet, medications [18], and exercise for after surgery [11,18].
There have been many reports of statistically significant LOS reductions for patients who have participated in total joint education classes compared with those who did not attend. In one study, TJA patients who participated in preoperative education class were reported to have an LOS of 1.7 days compared with 2.7 days for those who had not [28]. Studies including patients undergoing THA reported an LOS difference of 2.12 [30], .74 [21], and .77 [27] days between those who had and had not attended a preoperative educational session. Those undergoing TKA had an LOS difference of 2.0 [13], .37 [27], and .54 [22] days between groups. In one study, the LOS benefit was even more pronounced (greater than 2 days of difference) for a cohort of patients who were predicted to require a prolonged stay [27]. Studies examining the benefit of educational classes aimed specifically at facilitating same-day discharge (SDD) do not exist.
Virtual health care technologies are increasingly popular in health care, gaining favor among providers and patients. Some benefits of virtual interventions relate to convenience, access, and practicality. Virtual therapy visits permit the provider to view the patient’s home and make patient-specific recommendations regarding safety and home modifications. In addition, caregiver presence is encouraged during virtual visits, which is an advantage over in-person care, where caregiver presence may not be possible [7]. Authors have concluded that benefit of virtual administration of education includes the alleviation of barriers related to physical distance [24]. It is unclear whether the LOS benefits typically experienced by patients who attend in-person educational sessions would be similar in patients who receive virtual education.
The purpose of the study was to investigate whether participation in an individually administered preoperative educational session—delivered in-person, virtually, or telephonically—relates to reduced LOS or increased likelihood of SDD for those undergoing TJA. An additional purpose is to determine how the virtual mode of education compares to the in-person mode with regard to LOS benefits.
Methods
We conducted a case-control study using information obtained from the NYU Langone Orthopedic Hospital (LOH) electronic medical record (EMR). Institutional review board approval was obtained prior to review of the medical record. Informed consent was not required for retrospective review of EMR data.
Preoperative education class (Prehab) is offered by our rehabilitation department to patients scheduled to undergo TJA via a virtual visit, an in-person visit to our clinic, or a telephone call, typically within 1 month of the scheduled surgery. Patients are scheduled for virtual visits if they are New York State residents and agree to the virtual mode of delivery. Patients unable to utilize a virtual visit may schedule an in-person visit (if they are willing to travel to our site) or a telephone visit. Because a Prehab visit is considered optional, not all surgical patients received Prehab sessions during the study period, permitting between-group comparison of outcomes.
Regardless of the mode of delivery, the Prehab visit was consistent with some exceptions. In-person visits occur on-site at a clinic designated for the task. All Prehab sessions last 1 hour and include 30 minutes with a physical therapist and another 30 minutes with an occupational therapist. The session begins with information gathering on the patient’s level of function, preferences, home environment, typical activity level, and plans for after hospital discharge. Education is delivered on topics related to expectations after surgery, postoperative care and anticipated: LOS, home safety and modification, techniques for mobility and activities of daily living, and community re-entry. Those who receive a telephone session receive all information verbally. During virtual and in-person sessions, the patient can observe as therapists demonstrate mobility and self-care tasks with adaptive equipment as they receive instruction on how to perform tasks (ambulation, stair negotiation, bathtub transfer, or car transfer, among others). During virtual visits, the therapist is also able to view the patient’s environment and/or observe the patient performing tasks within their home. If known, information is provided regarding the anticipated discharge location and timeframe (ie, SDD, overnight, or 2-midnight stay), but this information is not always available at the time of the Prehab visit.
To perform sampling, a Medicare Coverage of Innovative Technology (MCIT)-generated report was obtained that contained all patients who have had a primary or revision TJA, unilateral or bilateral, at LOH between January 2022 and August 2022. Patients were included in the report if they were over the age of 18 and had a THA or TKA (inclusive of the several procedural diagnoses; see Appendix 1) during the study period. There were no exclusion criteria.
The MCIT report contained all independent and dependent variable data for the identified patients, including age in years, gender, ethnicity, ultimate surgical classification (inpatient or outpatient), and LOS. A separate report was extracted from the EMR with a list of completed Prehab visits with accompanying mode of Prehab (in-person, virtual, or telephonic), which was then merged with the primary report. Length of stay was also re-coded as a dichotomous variable SDD (yes or no), defined as a discharge on the same calendar day as surgery.
Statistical Analysis
All statistical analyses were performed using IBM SPSS version 26. Demographic characteristics of the 2 groups were reported as counts and percentages of the whole. Continuous variables were reported as means with standard deviation. The sample was compared using independent samples t-tests and chi-square χ2 tests to establish baseline equivalence of the Prehab groups. The between-group difference is reported as a P value along with the Cohen’s H score for comparison of proportions and the Cohen’s D score for comparison of means. According to Cohen, an effect size of .2 is considered a small effect, .5 medium, and .8 large [5], representing the magnitude of difference between the groups.
To answer the research questions, an independent samples t-test was performed for comparison of LOS for Prehab versus no Prehab groups. Comparison of mode of Prehab (in-person Prehab compared with virtual Prehab) was performed using analysis of variance (ANOVA) testing. Similar analysis was performed individually for outpatient and inpatient subgroups. To compare LOS outcomes for those receiving virtual Prehab when compared with in-person, an additional t-test was performed.
Frequency of SDD was compared between the Prehab and no Prehab groups using a chi-square test. Additional chi-square analysis was performed to compare SDD proportions for mode of Prehab (no Prehab, telephonic Prehab, in-person Prehab, and virtual Prehab), and to compare the virtual with the in-person Prehab outcomes more specifically. In addition, binomial logistic regression was performed for the SDD outcome related to mode of Prehab (none, telephonic, in-person, or virtual).
Results
A total of 2532 patients were included in the analysis. The included patients had either primary or revision TKA or THA at LOH between January and August 2022 (Table 1). With exception of ultimate surgical class, the Prehab and no Prehab groups were similar based upon their demographic characteristics. The Prehab group contained a higher proportion of outpatient-class patients than the no Prehab group, although the effect of the difference did not meet Cohen’s criteria [5] for a small effect, suggesting similarity of the groups.
Demographic characteristics of the sample.
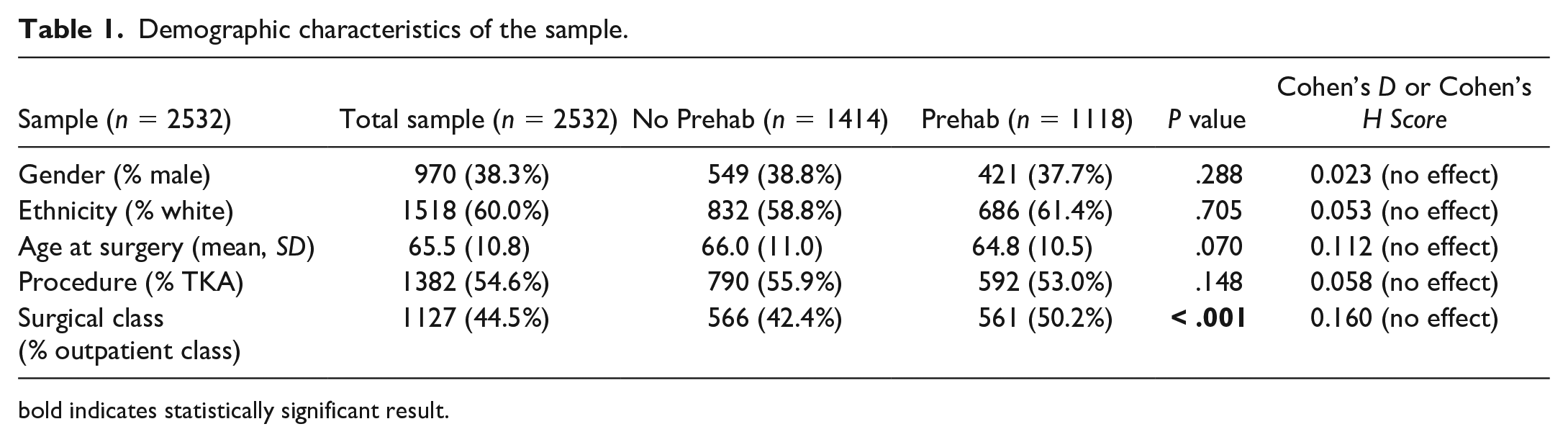
bold indicates statistically significant result.
Patients who attended Prehab had a shorter overall LOS than those who did not, representing a difference of 8.5 hours (.35 days). Results of independent samples t-tests confirmed that the between-group difference was statistically significant. Subgroup analysis confirmed that both inpatient- and outpatient-classified patient groups demonstrated shorter lengths of stay if they had participated in Prehab (see Table 2).
Length of stay for those receiving no Prehab, telephonic Prehab, in-person Prehab, or virtual Prehab.
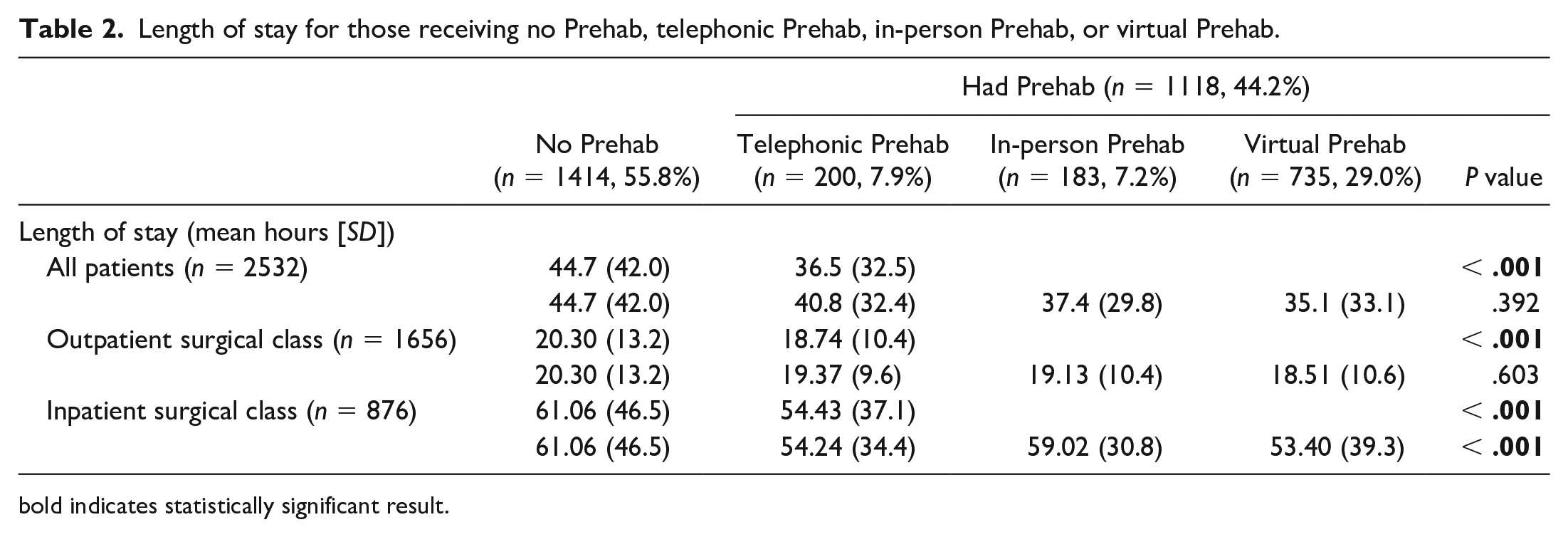
bold indicates statistically significant result.
When comparing the virtual mode of Prehab to the in-person mode, patients receiving virtual Prehab had the shortest LOS, followed by the in-person, telephonic, and no Prehab groups that also represented a statistically significant difference. Comparing the LOS for those receiving the virtual with those receiving the in-person mode of Prehab revealed a lack of difference between groups. Subgroup analysis revealed that LOS differences were non-significant for those with outpatient classification but were non-equivalent for those designated as inpatient class, with a shorter LOS experienced by those having virtual Prehab (see Table 2).
To understand the relationship between participation in Prehab and SDD, analysis of the subgroup of outpatient-class patient records was performed. There were 1127 patients included in the analysis, of which 589 (52.3%) achieved SDD. Prehab in any form did not relate to a higher proportion of patients achieving SDD (P = .254). Similarly, although a higher proportion of those having virtual or in-person Prehab achieved SDD when compared with patients who did not have Prehab in any form, the results were not different (P = .151). A specific comparison for the proportion of patients achieving SDD between those having in-person Prehab and those having virtual Prehab also revealed similar outcomes (see Table 3). These results were confirmed through binary logistic regression analysis of mode of Prehab for SDD outcomes, the results of which were also not statistically significant.
For those designated as outpatient class, proportion of patients achieving SDD for those receiving no Prehab, telephonic Prehab, in-person Prehab, or virtual Prehab.
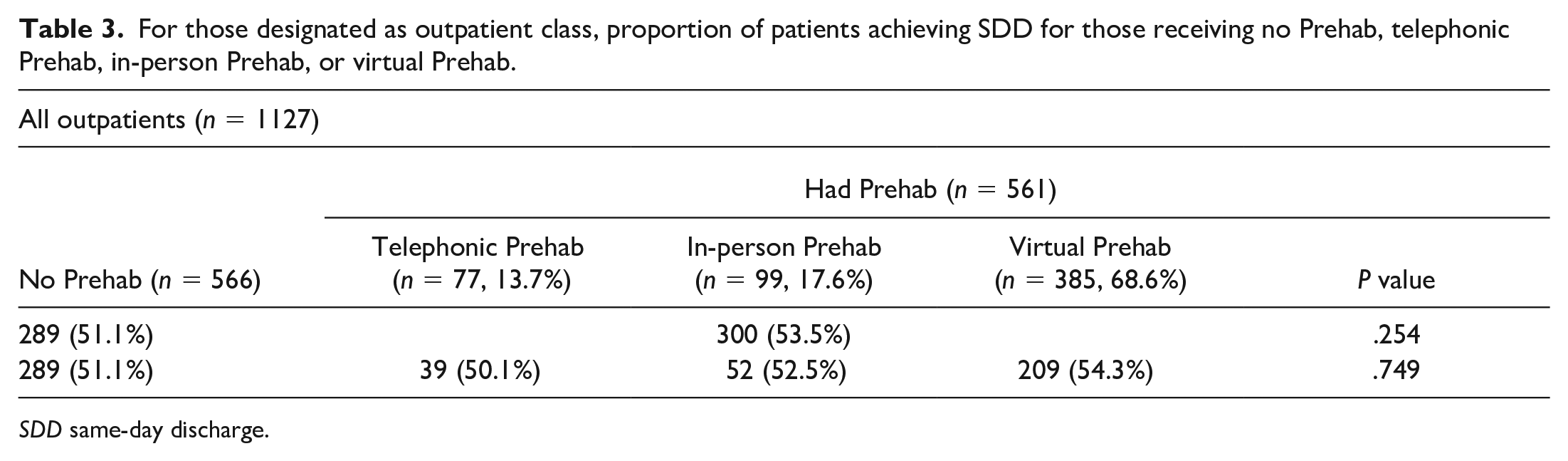
SDD same-day discharge.
Discussion
The results of this retrospective study suggest that patients undergoing TJA at a single institution who had participated in Prehab educational sessions had reduced LOS when compared with those who had not participated. The LOS difference was more marked for patients who were booked for inpatient surgery. In addition, patients who had participated in in-person or virtual Prehab had the shortest LOS. These results confirm (at minimum) non-inferiority of the virtual mode of the Prehab visit.
Limitations of this study relate to the retrospective study design, which lacks control of the interventions and randomization and control of the sample. Consequently, control of the educational content of the Prehab sessions was not possible, and it likely varied between providers. While content guidelines for Prehab exist at our institution, a session may be tailored to the individual patient. Education provided by other interdisciplinary staff outside of formal Prehab may also affect outcomes but was not included as part of this analysis. Factors, such as time of day or day of the week of the surgery, surgeon preference, and/or perioperative and postoperative contributors were also not included in this analysis. In particular, early time of surgery may increase the likelihood of SDD. Patients scheduled for surgery very late in the day are unlikely to achieve SDD due to logistical challenges. Future study should control for this potential confounding factor.
In addition, sampling bias may have affected our results. The sample included was a relatively young, primarily female population of TJA patients residing within or near the New York City metropolitan area; they may represent a unique demographic, which may limit the external validity of the findings. Characteristics of this population, such as socioeconomic status and medical literacy, in particular, may be distinct from that of TJA populations in other locations. Although the sample included in the Prehab and no Prehab groups would be considered similar according to the variables measured in this analysis, equivalence of the sample was not established through a randomized sampling approach. As such, relationships highlighted in this study should be interpreted with consideration of this. The LOS benefits of participation in Prehab may be attributed to multiple factors, including alignment of patient and physician expectations, frontloading of education points that would otherwise be received postoperatively, and the early identification of barriers to discharge [10,21,23]. It has been previously established that alignment of patient and provider expectations is crucial to ensuring both successful outcomes and high patient satisfaction with their surgical experience; patient-provider alignment has also been demonstrated to benefit patients through reduced LOS [31]. It is our experience that information about the planned LOS—although likely provided initially by the surgeon—bears repeating by other providers to ensure patients are cognitively and emotionally prepared for a short stay.
The provision of information about and demonstration of mobility tasks, equipment usage, and postoperative patient-provider exercise in the period prior to surgery may be another way in which Prehab contributes to decreased LOS. Describing and demonstrating how tasks are performed with durable medical equipment, assessing and discussing the patient’s home environment, and screening for barriers to discharge during Prehab sessions, may all contribute to reduced time spent on these tasks during the postoperative period. Redundancy in education provision is a well-established method to more effectively induce learning [15].
Similar to previous investigations on virtual health care for this population, our results support the use of the virtual mode of education delivery as, at minimum, non-inferior to the in-person mode, and potentially superior to in-person, as related to reduced LOS. The benefits of a virtual visit may be attributed to the ability for the provider to interact with the patient while they are in their own home, allowing for a more specific and patient-centered intervention than can be accomplished in a clinic. This provides support for the virtual mode, which has logistical and practical benefits for patients and providers [7,24], and could be favored over in-person care delivery models. Virtual modes of education delivery have been associated with lower costs to organizations, as well [26].
The reduction in LOS experienced by patients who have had Prehab may have significant fiscal implications. Reducing LOS while maintaining safety of the patient has the potential to reduce the costs associated with procedures, including those related to overhead and staffing. Shortening LOS also facilitates throughput that permits scheduling of additional procedures, further benefiting organizations.
The lack of a statistically significant difference between groups suggests that the Prehab sessions at our institution did not relate to the SDD outcome; in fact, they were used similarly for inpatients and outpatients who may or may not be well-suited for SDD. Our results also suggest that there may be a need for development of Prehab content specific for outpatients who are intended for SDD. Future study should focus on whether specific educational content geared toward SDD, when delivered during Prehab, results in increased success of SDD.
In conclusion, in patients who had participated in Prehab prior to TJA, this study found an association with reduced LOS but not with increased likelihood of SDD. In addition, the virtual provision of Prehab was found to be at least non-inferior or superior to the in-person mode for the LOS outcome, suggesting that virtual preoperative education may be a viable alternative to in-person education. The lack of statistically significant findings for the SDD outcome may relate to the intervention’s lack of specificity for the SDD outcome. Future study should focus on the delivery of more targeted educational content to those planned for SDD. In addition, further study is needed on other potential benefits of virtual preoperative education, including patient and provider satisfaction and practical and financial benefits.
Supplemental Material
sj-docx-1-hss-10.1177_15563316231208454 – Supplemental material for Does Participation in Virtual or In-Person Preoperative Education Relate to Reduced Length of Stay After Total Joint Arthroplasty?
Supplemental material, sj-docx-1-hss-10.1177_15563316231208454 for Does Participation in Virtual or In-Person Preoperative Education Relate to Reduced Length of Stay After Total Joint Arthroplasty? by Susan Camillieri in HSS Journal®
Footnotes
Appendix 1
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human/Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
Informed Consent
Informed consent was waived for the patients included in this study.
Level of Evidence
Level III, retrospective case-control study.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.