
Abstract

Keywords
Effective communication and collaboration are essential to delivering efficient, high-quality patient care. Information technology (IT) enables health care workflow and crucial patient information, such as medical history, preoperative assessments, and postoperative progress, and has immense potential to improve care coordination by supporting providers, enabling identification of pertinent information and workflows, and facilitating collaboration on the care team [1]. Sharing this information promotes a comprehensive understanding of the patient’s condition and enables timely, coordinated care. At our institution, HSS, IT enhances the patient journey across the entire continuum of care (Table 1).
List of IT changes categorized by patient phase of care.
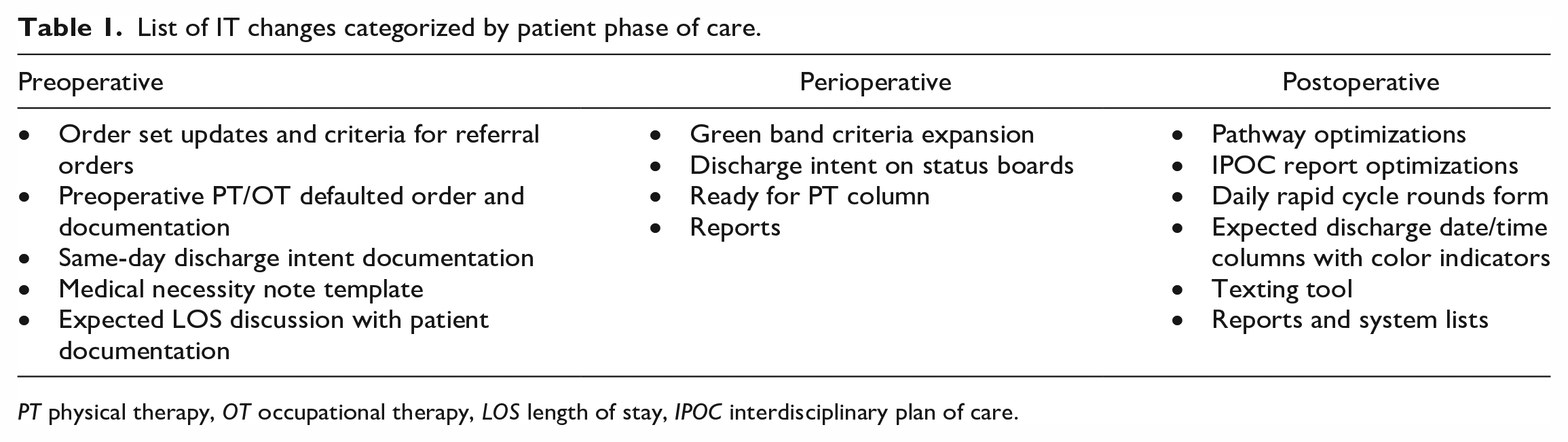
PT physical therapy, OT occupational therapy, LOS length of stay, IPOC interdisciplinary plan of care.
As the constraints of third-party payors have required health systems to optimize perioperative care for patients undergoing total joint arthroplasty (TJA), IT can play a pivotal role in optimizing length of stay (LOS). At HSS, IT has contributed to successfully reducing patient LOS following TJA by partnering with clinicians to optimize the electronic medical record (EMR) to support changing workflows. Over the last few years, HSS has seen a steady increase in patients undergoing TJA discharged in less than 24 hours. In 2020, 22% of TJA patients were discharged in less than 24 hours; from January through August of 2023, 53% of cases were discharged in this time period (Fig. 1). Through analysis of data from the EMR, operational care teams identified gaps in knowledge transfer and determined opportunities for improvement within the EMR to communicate necessary information across teams. This has enhanced both the care team’s and the patient’s experience, while addressing LOS goals. The implementation of new clinical workflows and adjustments to existing ones necessitated modifications and enhancements in the EMR system. These modifications were crucial in supporting the changes required to streamline care and enhance efficiency.
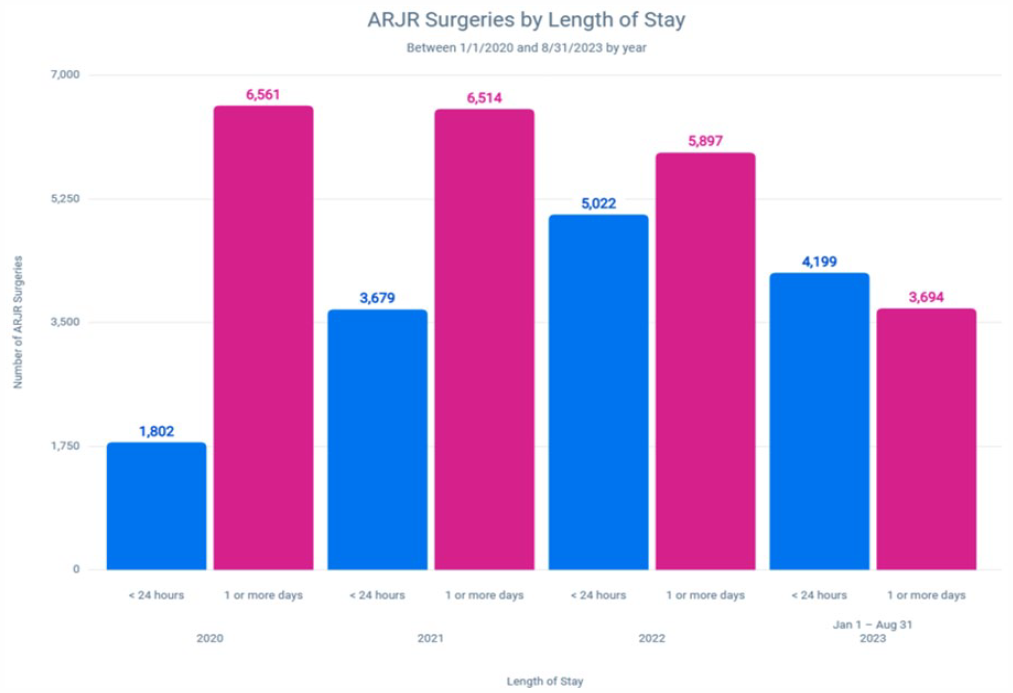
Annual number of ARJR Surgeries categorized by Lenght of Stay: Less than 24 hours vs greater than 24 hours. ARJR adult reconstruction and joint replacement.
Preoperative changes
Optimizations by the IT team enabled coordination of care to begin before a patient arrives for surgery. Patient data collection, as well as education and health management, was moved to earlier in the episode of care. The order sets used to schedule patients for surgery were adjusted to automatically select referrals for health conditions documented in the patient’s record. For example, a patient with a body mass index (BMI) higher than 45 would automatically be referred to lifestyle medicine. Thus, patients with pre-existing conditions can better prepare for surgery by meeting with specialized providers to prevent complications—ultimately minimizing LOS.
Preoperative referrals to physical therapy (PT) and occupational therapy (OT) are included in preoperative consultations. Studies have shown that providing rehabilitation education prior to surgery (“prehab”) reduces the time it takes for patients to meet their postoperative functional milestones, allowing for quicker PT clearance, and potentially shorter LOS [2]. The EMR system was modified to allow data collection during the preoperative PT consultation, providing a coordinated, comprehensive functional context for the hospital’s treatment team throughout the episode of care. For example, if a patient has stairs without a railing, the therapist can confirm this with the patient at the preoperative visit and document this in the EMR, where it is visible to those treating the patient postoperatively.
The surgical case request order was modified to include a question prompt to document whether the physician intends to send the patient home on the day of surgery if they meet the criteria. It is important to identify which patients will be discharged the same day versus those who are to have an overnight stay; this should be done prior to admission; insurance class does not always accurately depict this for care teams. This question ensures that all care team members are aware of which patients are anticipated to be discharged on the same day. It also leads to the identification of patients who may need to be converted to an inpatient class from an ambulatory class based on medical needs. This can be addressed prior to admission and documented using the medical necessity note template, which guides the provider through the essential information needed to demonstrate the requirements for extended care and hospital stay days. In addition, a new flowsheet row was created for social work and PT to complete during a preadmission visit or call, to document that they discussed the expected LOS with the patient or their family. This conversation ensures that the patient and care team’s goals are aligned on the day of surgery. Many studies demonstrate that clear expectations lead to greater patient satisfaction [3].
Day of surgery optimization
Upon patient arrival, wristbands are provided with pertinent patient identifying information. Green wristbands were implemented in December of 2020, designed as a visual indicator for clinicians to distinguish ambulatory surgery (AMS) patients from those expected to be admitted. The green bands included the same information as the white bands but were specifically for AMS patients. Operations recognized the value of this color indicator and requested modifications to the existing EMR logic to include a broader group of patients expected to meet discharge criteria and leave the same day. The updated criteria for the green wristband included lower extremity arthroplasty patients with a patient class of AMS; a case start time before or at 11:00 AM; or if the patient was planned for SDD, as the surgeon indicated on the case request order. The logic excludes patients who were initially requested to be admitted as inpatient, yet their insurance only approved an AMS admission. The workflow was also optimized; instead of the green wristband replacing the white one, it was given in addition. The patients who met AMS criteria would wear both white and green wristbands. A report was developed to provide admitting a list of the patients who met the criteria to have both bands. The green wristband serves as a visual indicator to the care team, enabling them to identify patients who are suitable candidates for SDD, thus ensuring they are placed on an AMS clinical pathway and that their clinical needs are timed appropriately to meet this goal. If at any point, there is a decision to keep the patient overnight, the green band is removed. In the previous workflow, this required a band reprint for the patient to have a white wristband, but with the new workflow of having both wristbands provided during admission, this step was eliminated.
The IT department also developed a report on all patients who met the green wristband criteria and their actual LOS. This enabled stakeholders to closely track and evaluate the progress of SDDs and identify potential process improvements. A recent review of this information resulted in an IT optimization request to include patients with later surgery start times, up until 1 pm, and to exclude patients with a discharge plan of rehabilitation, further optimizing the identification of patients who could be discharged the same day.
In perioperative areas, the information captured in the physician’s office, specifically, the intention to send the patient home on the day of surgery, is prominently displayed on various status boards that are accessible to the care team. Status boards are used primarily by the clinicians working in the perioperative areas, providing a combination of the day’s cases, patients’ current location and status, pertinent related information, as well as easy access to patients’ charts, cases, and logs. If there are any changes in the patient’s condition during the surgical procedure that may require them to stay longer, the intraoperative nurse documents the change, and it is immediately updated on the status boards. This allows for the entire care team to be aware of changes in real-time and appropriately adjust the post-op care plan as needed.
Once a patient has met certain criteria—such as normal sensorimotor assessment, post-op check completed, and hemodynamically stable—the bedside nurse clicks a “Ready for PT” button that notifies the physical therapists that a patient is ready to mobilize. This real-time communication leads to efficient allocation of resources and provision of care to the right patient at the right time.
Postoperative system optimizations
As more patients are admitted as ambulatory patients, this organization is not always able to cohort them separately from the inpatients. To ensure efficient management of AMS patients medically and surgically appropriate for ambulatory LOS, new reports, status boards, and patient lists were developed within the EMR for different disciplines, using the tools most appropriate for their workflows. These tools were set up with specific patient details related to the patient’s expected LOS. These tools allow clinicians to easily identify AMS patients and ensure their needs are met efficiently, keeping them on track for their expected discharge.
Another important aspect of the optimization project involved updating AMS knee and hip pathways, which are created with best practice order options, medication routes, and treatment geared toward optimal patient outcomes. Safety is a high priority. One noteworthy modification involved removing default postoperative labs. Clinical stakeholders determined that routine labs were not necessary for most patients eligible for SDD. Consequently, eliminating this default and, instead, allowing providers to manually select these labs as needed, mitigated potential discharge delays resulting from completing and reviewing lab results.
Using IT reporting tools to extract pathway utilization data, operations identified an issue where AMS patients scheduled for surgery later in the day, who likely would require an overnight stay due to the timing of their surgery, were frequently placed on an inpatient pathway [3]. This led to delayed goal achievement and prolonged LOS, as the inpatient pathways were designed for a more complex patient population. To better account for these patients in the AMS pathways, we further optimized the pathway build by expanding the goals from 8 hours to 23 hours, incorporating the overnight AMS patients into one AMS pathway. Once the changes were implemented and prescribers were further educated on the appropriate use of these pathways, more patients are now put on the appropriate AMS pathways.
In the first quarter of 2022, 44% of adult reconstruction joint replacement patients were placed on the correct hip- and knee-specific AMS pathways. The pathway modifications were completed in April 2022, and by second quarter 2023, we achieved an 83% utilization of the AMS pathways (Fig. 2). The increased utilization highlights the positive impact of our efforts in both optimizing pathways and educating our prescribers.
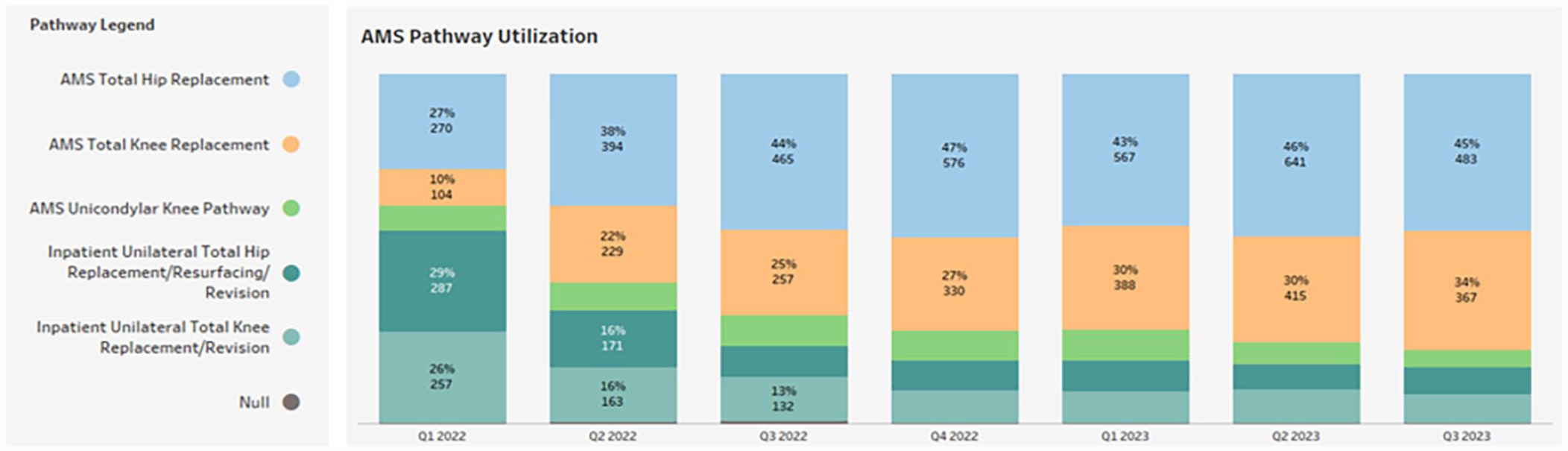
Quarterly distribution of Pathway usage from Q1 2022 to Q2 2023. AMS ambulatory surgery.
The interdisciplinary plan of care (IPOC) report, a real-time tool for care coordination, was further optimized to support multidisciplinary care team rounds. Acknowledging the benefits of morning rounds, it was evident that an additional round later in the day for patients expected to have a less than 24-hour LOS would facilitate timely review and clearance of discharge barriers. A new daily rapid cycle rounds form was introduced, designed specifically for clinicians to document essential patient discharge plan information, and note any outstanding barriers. These data elements are summarized and displayed in the IPOC report, fostering a comprehensive review, and facilitating meaningful discussions during the rounds. The IPOC report integrates data collected prior to admission, which includes the initial intent for SDD, as well as the discussions held with the patient or their family regarding this intent. This approach ensures that all relevant information is consolidated within the report, contributing to more effective care planning and decision-making during the rounds.
Finally, a process was implemented to ensure timely discharge once a patient was cleared to leave the hospital. The expected discharge date and time are provided to patients during a preadmission phone call in which they are informed of their surgical time so they can prepare for discharge transportation. This information is also entered into the EMR by the call center nurse. Anticipated discharge date and time is reviewed and adjusted during rounds based on the outstanding items and expectations for clearance. Logic was built into the expected discharge field on the system list to display colored icons to remind the staff to regularly review and update the discharge plan. A green check displays if review was done, white indicates it is time to review, and yellow means the review is overdue. The digital monitors on the wall at each nursing station also display the expected discharge date and time for all patients on that unit. This also has logic to turn the field green when the discharge time is confirmed. Nursing reviews this information to provide an accurate estimated discharge hour to the escort the evening before (if adequately determined) or morning of discharge, giving the escort ample time to prepare for pickup. Given our institution is in a busy urban center, traffic delays can be long, so planning is important for timely discharges. Information technology developed a tool in the EMR system to improve the communication process with patients’ families. This tool gave nursing the ability to send text messages to patients’ escorts. For added convenience, it includes prewritten messages for each potential hour, along with the hospital’s address and phone number. The nurse can select the appropriate message and share the expected discharge time for pickup, minimizing clicks and manual typing.
In conclusion, system modifications and the development of new tools within the EMR system enhance communication, streamline processes, and facilitate efficient care delivery. In working with stakeholders to optimize these functions, IT plays a critical role on the multidisciplinary team. These advancements allow health care teams to work collaboratively and deliver more effective and timely care, ultimately leading to successful reductions in patient LOS.
Supplemental Material
sj-docx-1-hss-10.1177_15563316231209027 – Supplemental material for Leveraging Technology Across the Patient Care Journey to Reduce Length of Stay After Total Joint Surgery
Supplemental material, sj-docx-1-hss-10.1177_15563316231209027 for Leveraging Technology Across the Patient Care Journey to Reduce Length of Stay After Total Joint Surgery by Christine Carey in HSS Journal®
Footnotes
Acknowledgements
The author thanks Elizabeth Biehl, Danielle Edwards, and Sharlynn Tuohy for their contributions, including providing workflow details, constructive feedback, insightful edits, and support through the writing process.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human/Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
Informed Consent
Informed consent was not required for this commentary.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.