
Abstract
Background:
Total joint arthroplasty (TJA) performed in the ambulatory surgical center (ASC) has been shown to be safe and cost-effective for an expanding cohort of patients. As criteria for TJA in the ASC become less restrictive, data guiding the efficient use of ASC resources are crucial.
Purpose:
We sought to identify factors associated with length of stay in the recovery room after primary total hip arthroplasty (THA) and total knee arthroplasty (TKA) performed in the ASC.
Methods:
We conducted a retrospective review of 411 patients who underwent primary THA or TKA at our institution’s ASC between November 2020 and March 2022. We collected patient demographics, perioperative factors, success of same-day discharge (SDD), and length of time in the recovery room.
Results:
Of 411 patients, 100% had successful SDD. The average length of time spent in recovery was 207 minutes (SD: 73.9 minutes). Predictors of longer time in recovery were increased age, male sex, and operative start time before 9:59
Conclusion:
In this retrospective study, factors associated with increased length of time in the recovery room included older age, male sex, and operative start time before 9:59
Keywords
Introduction
Total hip arthroplasty (THA) and total knee arthroplasty (TKA) are successful, cost-effective procedures shown to improve patients’ quality of life [10,11]. The demand for these procedures is projected to increase in the next decade [17,22]. Advances in perioperative care and surgical technique have led to a decrease in length of stay for total joint arthroplasty (TJA) [19]. As a result of these advancements and the Center for Medicare and Medicaid Services’ removal of these procedures from the inpatient-only list, there has been an increased interest in optimizing outpatient TJA.
Outpatient TJA can be performed in the hospital or the ambulatory surgical center (ASC). The safety, efficacy, cost, and patient satisfaction of TJA in the ASC have been well described in the literature [1,4,5,7,9,13,16,24,25,28,30]. Regardless of whether it is performed in the hospital or ASC, the goal of outpatient TJA is to safely decrease postoperative time spent in the health care setting, often with same-day discharge (SDD).
Patient selection is crucial for successful SDD following TJA. Some studies that have investigated factors affecting successful early discharge [20,26,27,29] have found younger age, male sex, lower American Society of Anesthesiologists (ASA) scores, less chronic health comorbidities, lower postoperative pain scores, and earlier operative start time to be predictors [26,27,29]. Using these findings, various predictive models, scoring systems, and recommendations have been developed to assist surgeons in selecting patients who may be suitable for TJA in the ASC [20,21,31]. However, none of these models is universally accepted, and each is criticized for different reasons, such as failing to include variations in comorbidities, patient home support, or patient motivation [20].
While imperfect recommendations surrounding patient selection for the ASC do exist, there are limited data on predictors of prolonged time in the recovery room prior to SDD from the ASC. Because ASCs have limited capacity for overnight stay, it is paramount to recognize patients who may require additional time in the recovery room prior to discharge. We therefore sought to investigate factors associated with increased time spent in the recovery room following TJA performed in the ASC setting. Understanding factors associated with time in recovery may assist arthroplasty surgeons in maximizing efficiency and likelihood of successful SDD.
Methods
Approval from the institutional review board was obtained prior to initiation of this study. We performed a retrospective review at a single, large, academically affiliated institution. An electronic query was performed to identify all patients who underwent a primary elective THA (Current Procedural Terminology [CPT] code 27130) or TKA (CPT code 27447) between November 2020 and March 2022 at our institution’s ASC. All surgeries were performed by one of 4 adult reconstruction, fellowship-trained orthopedic surgeons. All patients provided written informed consent for their procedure and for the deidentified use of their information for research purposes. Inclusion criteria consisted of age ≥18 years, primary THA or TKA, preoperative designation for the SDD pathway, and surgery performed in the ASC. Exclusion criteria consisted of age <18 years, unicompartmental knee arthroplasty, revision TJA, bilateral TJA, and patients not eligible for our SDD pathway. Currently, our institution performs 35% to 40% of TJA cases in the ASC.
Per our institution’s protocol, the surgeon screened elective THA and TKA patients for eligibility for our SDD pathway, using predefined institutional guidelines developed by a team of hospitalists and anesthesiologists (Supplemental Table S1). Patients meeting criteria were given the choice to be designated for the SDD pathway. Shared decision-making was then utilized between the patient, surgeon, anesthesiologists, and perioperative hospitalists to determine whether a patient should ultimately be included in the SDD pathway. If selected for the pathway, the location of surgery (ASC vs hospital) was based on patient preference for date of surgery. Of note, the surgical scheduler determined the order of TJA cases using several factors. For example, patients who travel a long distance are generally given an earlier start. In addition, the first case of the day is usually a THA because our institution does not utilize peripheral blocks for THA patients. After the first case is determined, the subsequent THA patients generally stay in the same room and the same laterality is scheduled sequentially to eliminate the need for the operating room team to reorganize the X-ray machine. Patients above the age of 65 years and those with risk of urinary retention are also given preference for an earlier start.
All patients were optimized prior to surgery by one of 2 perioperative hospitalists, and additional medical subspecialty clearances were obtained at the hospitalists’ discretion. All patients were evaluated for urinary retention risk using criteria established by our perioperative team (Supplemental Table S2), which includes the American Urological Association score [3]; if the score is ≥3, a postvoid residual (PVR) is performed during preadmission testing. If the PVR is ≥250 mL or the PVR is < 250 mL but score ≥5, the patient is flagged as high risk. Patients deemed high risk for urinary retention are not excluded from the SDD pathway. Alternatively, they are placed on tamsulosin in the perioperative period, and medications such as antihistamines, long-acting opioids, and those with anticholinergic properties are decreased or discontinued as tolerated to limit the risk of iatrogenic postoperative urinary retention.
Procedural anesthetic was chosen by the anesthesia team, with a preference for spinal anesthesia, given its reduced risk of complications, effectiveness in pain relief, and short duration of action [18]. Spinal anesthesia was achieved using either 1.6 cc or 2 cc of 7.5% bupivacaine. For patients undergoing TKA, ultrasound-guided adductor and interspace between popliteal artery and capsule of the knee blocks were also performed using 10 cc of 0.5% bupivacaine and 10 cc of liposomal bupivacaine. Patients received 1 dose of cefazolin within 1 hour of incision. Alternatively, 1 dose of weight-based vancomycin was administered if patients had an anaphylactic penicillin allergy. Patients with a history of methicillin-resistant Staphylococcus aureus (MRSA) infection or a positive preoperative MRSA nares screen were given both cefazolin and vancomycin. Upon completion of the surgical case, each patient was transferred directly to the recovery room.
Per our ASC protocol, upon return of motor sensation to the lower extremities, patients met with a licensed physical therapist in the recovery room. The therapist evaluated patients in the order in which they underwent surgery. If a patient was deemed unsuitable for physical therapy at the time of evaluation (eg, spinal anesthesia was still in effect), the therapist deferred treatment and returned to reevaluate the patient after each subsequent session. The physical therapist determined whether the patient was able to safely ambulate for basic needs and made discharge recommendations accordingly. All patients were cleared for discharge by the physical therapy and anesthesia teams prior to leaving the ASC. Patients were given aspirin 81 mg twice daily for 35 days for pharmacologic deep vein thrombosis prophylaxis, unless they were prescribed an alternative anticoagulation medication prior to surgery. In those cases, patients resumed their anticoagulant postoperatively.
Our ASC has the capability for an overnight <24-hour stay with 2 nurses and an on-call physician. Patients requiring advanced medical treatment and those expected to stay for more than 24 hours are transferred to an affiliate hospital using ambulance. Successful SDD was defined as being SDD (prior to midnight); failure of SDD was defined as an overnight stay in the ASC or a transfer to an affiliate hospital for admission.
Demographics and clinical characteristics for all patients were collected, including age, sex, body mass index (BMI), Charlson Comorbidity Index (CCI), urinary retention risk, and preoperative opioid use. Preoperative opioid use was defined as self-reported opioid use within 60 days preceding surgery. Other data gathered from chart review included procedure type (THA vs TKA), operative start time, length of time in the recovery room, success or failure of SDD, and reason for failed SDD if applicable. A total of 411 patients were eligible for our study. Of the 411 patients, 166 (40.4%) underwent THA and 245 (59.6%) underwent TKA (other patient data are in Table 1).
Demographics and clinical characteristics.
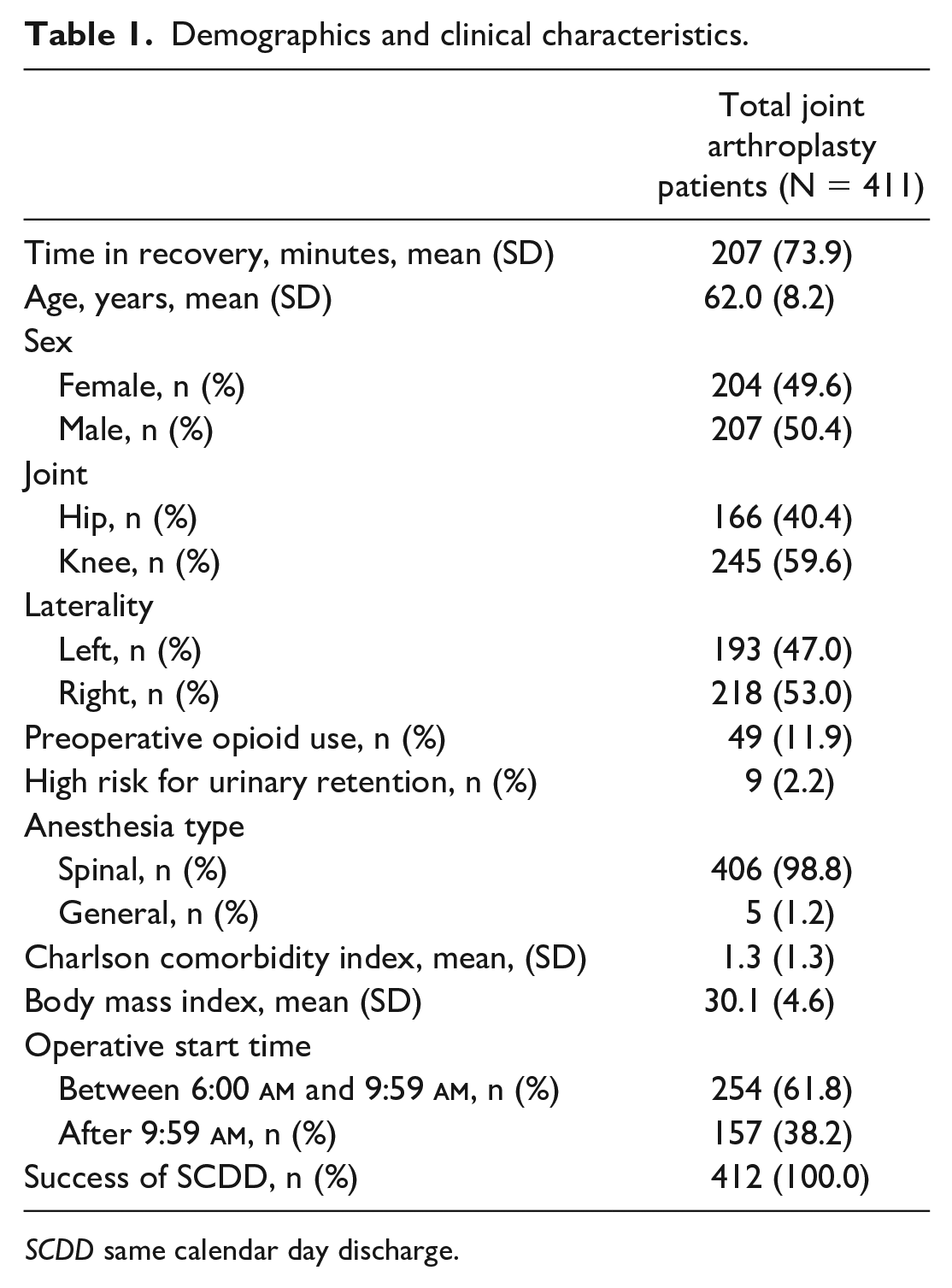
SCDD same calendar day discharge.
Statistical Analysis
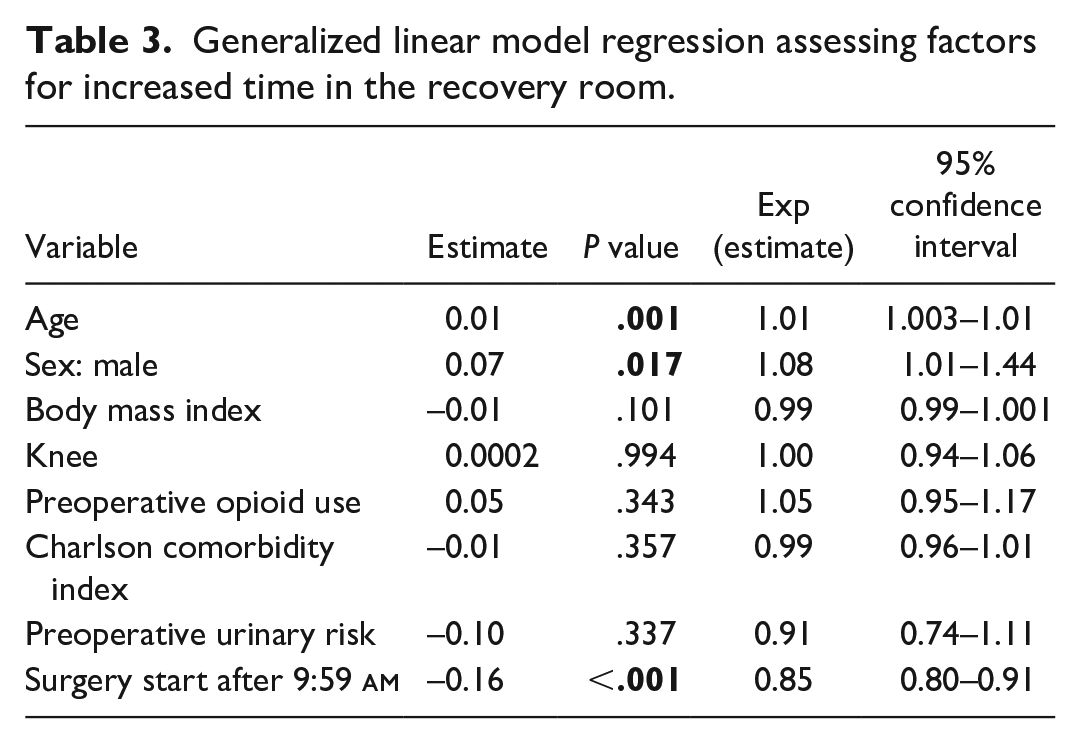
All statistical analyses were performed using R Studio Software (Version 3.5.1). A generalized linear model regression was performed to assess for factors associated with length of time in the recovery room. Independent variables included age, sex, BMI, preoperative opioid use, CCI score, type of surgery (THA vs TKA), high urinary retention risk, use of spinal versus general anesthesia, and operative start time before or after 9:59
Results
All 411 patients had successful SDD. The average length of time spent in the recovery room was 207 minutes (SD: 73.9 minutes). Table 2 reveals the mean time in the recovery room, broken down by specific demographic cohorts. Upon logistic regression analysis, predictors of increased length of time in the recovery room were increased age (P = .001), male sex (P = .02), and time of operation start before 10:00
Time in recovery based on demographics and clinical characteristics.
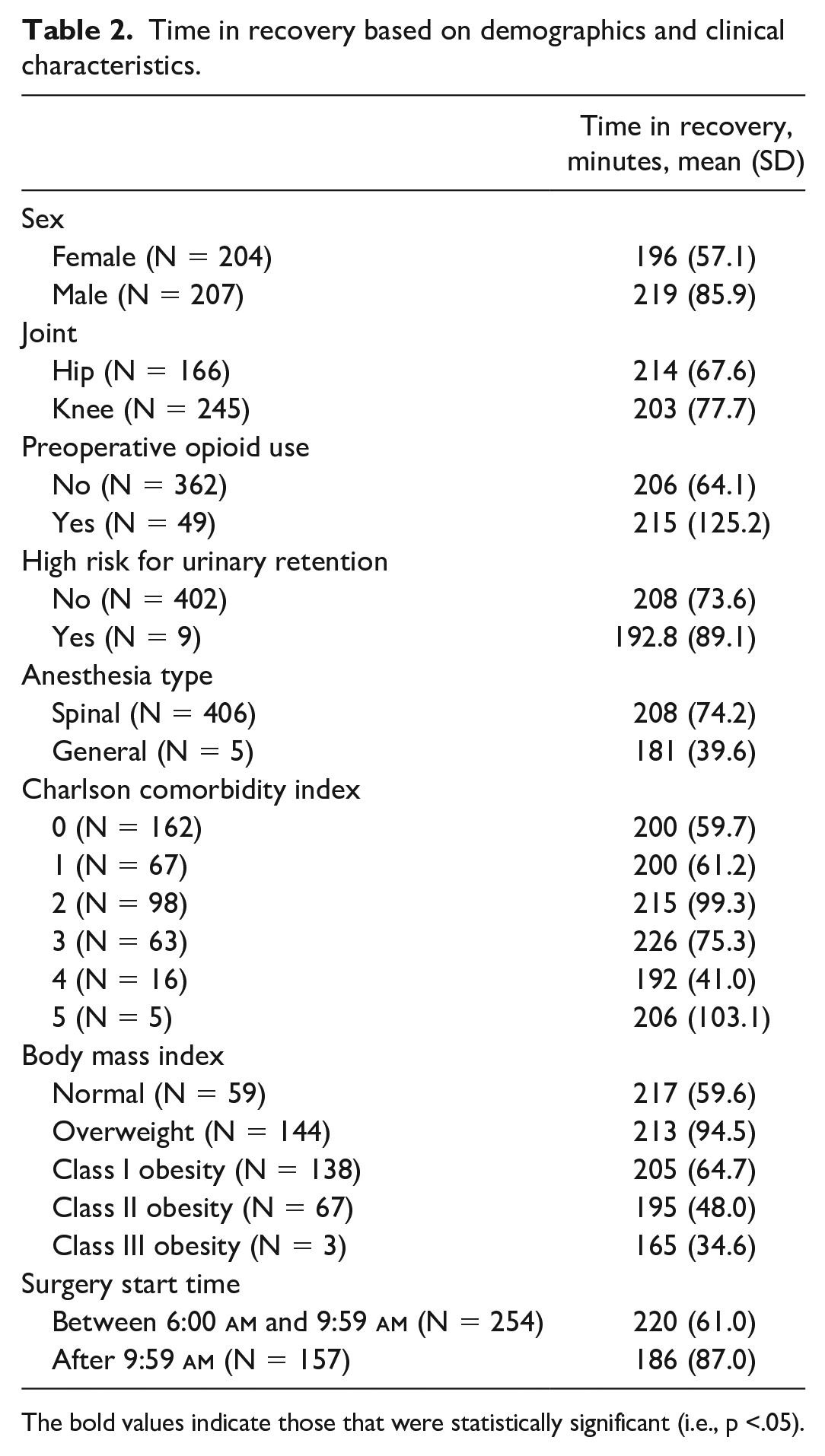
The bold values indicate those that were statistically significant (i.e., p <.05).
Generalized linear model regression assessing factors for increased time in the recovery room.
The ANOVA testing demonstrated a statistically significant difference in length of time in recovery when patients were grouped by age (P = .019; Table 4; Supplemental Fig. 2). Patients aged 70 years or older spent on average 50 minutes longer in the recovery room than patients aged below 50 years.
Analysis of variance assessing time in the recovery room based on patient age.

Discussion
Total joint arthroplasty in the ASC has been shown to reduce cost and improve patient satisfaction without increasing the risk of postoperative complications, but these facilities are designed for same-day procedures and are not always equipped for an overnight stay [9]. Surgeons performing TJA in an ASC are challenged to maximize the caseload while ensuring successful SDD. Because optimizing the order of surgical cases each day should help to accomplish this, we sought to identify factors associated with length of time in recovery after TJA in the ASC. We found increased length of time in the recovery to be associated with older age, male sex, and operative start time before 10:00
Our study has limitations. Most notably, our population was underpowered to detect a difference for some of the independent variables studied. Only 5 patients underwent general anesthesia, only 9 patients were deemed high risk for postoperative urinary retention, and only 49 patients used opioids preoperatively. Future studies with larger patient populations are needed to investigate the variables that contribute to longer recovery room times. In addition, while our purpose was primarily to identify patient-specific factors associated with length of time spent in recovery, the pragmatic nature of this study lends itself to confounding variables. Operational and ancillary staff practices may have masked or otherwise interacted with the independent variables and affected our finding that earlier surgery start time was associated with increased time spent in recovery, limiting the generalizability of our study. Although this can be viewed as a study weakness, these observations hold value and highlight important issues for future investigation. Finally, because our data were retrieved from retrospective chart review, their accuracy depend on diligent documentation; errors or omissions in documentation could affect the internal validity of our findings.
Multiple prior studies have investigated the association between age and early discharge after TJA. Some studies found no significant difference [12,26], whereas others found increased rates of successful early discharge with decreased age [27,29]. Because of prior conflicting evidence, we do not utilize an age limit to exclude patients from the SDD pathway. However, age was associated with time spent in recovery in our study (Table 4; Supplemental Fig. 2). Patients aged below 50 years spent a mean of 170 (SD: 46) minutes in recovery, which is 50 minutes less than patients aged 70 years or older. Our findings suggest that most patients aged below 50 years with surgery end times between 1:00
Whereas male sex was associated with prolonged recovery time in in our study, multiple prior studies investigating successful early discharge after TJA found higher success rates in male than in female patients [26,27,29]. It has been shown that females exhibit greater pain intensity and require higher doses of analgesics compared with males in the postoperative period [14]. However, these observations are likely best explained by patient-specific factors, such as pain sensitivity and the presence of chronic conditions, rather than any inherent gender-based difference [2,8,15,23]. As such, we do not suggest that gender should play a direct role in determining suitability for SDD after TJA. While it is unclear why women spent less time in recovery in our study, a possible explanation is that male patients may have demonstrated higher rates of postoperative urinary retention, although this was not detected as a significant factor in this study. This phenomenon is well studied in TJA literature and occurs in greater incidence in male patients [6]. At our ASC, patients are straight catheterized once they reach a bladder volume of 350 cc. If patients cannot void after reaching a bladder volume of 350 cc for a second time, they are discharged with an indwelling Foley catheter and instructed to follow up with a urologist 5 days postoperatively. Despite a detailed preoperative screening (Table 3) and treatment protocol, postoperative urinary retention certainly continues to present a primary obstacle to timely discharge in some patients.
The final factor associated with prolonged time spent in recovery was surgery start time before 10:00
Despite a growing body of research on which patients may be suitable for TJA in the ASC, we are unaware of existing evidence to guide surgeons in determining the optimal order of cases for each day at the ASC. Utilizing a group of patients already deemed appropriate for the ASC, our study provides insight into which patients may require a longer length of stay in the recovery room prior to discharge from the ASC. We found that predictors of prolonged length of time in the recovery room were older age, male sex, and operative start time before 10:00
Supplemental Material
sj-docx-1-hss-10.1177_15563316231208977 – Supplemental material for Older Age, Male Sex, and Early Start Time Lengthen the Recovery Room Stay Following Total Joint Arthroplasty in an Ambulatory Surgical Center
Supplemental material, sj-docx-1-hss-10.1177_15563316231208977 for Older Age, Male Sex, and Early Start Time Lengthen the Recovery Room Stay Following Total Joint Arthroplasty in an Ambulatory Surgical Center by Matthew J. Schultz, Hope S. Thalody, Rex W. Lutz, Quincy T. Cheesman, Alvin C. Ong, Zachary D. Post and Danielle Y. Ponzio in HSS Journal®
Supplemental Material
sj-docx-10-hss-10.1177_15563316231208977 – Supplemental material for Older Age, Male Sex, and Early Start Time Lengthen the Recovery Room Stay Following Total Joint Arthroplasty in an Ambulatory Surgical Center
Supplemental material, sj-docx-10-hss-10.1177_15563316231208977 for Older Age, Male Sex, and Early Start Time Lengthen the Recovery Room Stay Following Total Joint Arthroplasty in an Ambulatory Surgical Center by Matthew J. Schultz, Hope S. Thalody, Rex W. Lutz, Quincy T. Cheesman, Alvin C. Ong, Zachary D. Post and Danielle Y. Ponzio in HSS Journal®
Supplemental Material
sj-docx-2-hss-10.1177_15563316231208977 – Supplemental material for Older Age, Male Sex, and Early Start Time Lengthen the Recovery Room Stay Following Total Joint Arthroplasty in an Ambulatory Surgical Center
Supplemental material, sj-docx-2-hss-10.1177_15563316231208977 for Older Age, Male Sex, and Early Start Time Lengthen the Recovery Room Stay Following Total Joint Arthroplasty in an Ambulatory Surgical Center by Matthew J. Schultz, Hope S. Thalody, Rex W. Lutz, Quincy T. Cheesman, Alvin C. Ong, Zachary D. Post and Danielle Y. Ponzio in HSS Journal®
Supplemental Material
sj-docx-3-hss-10.1177_15563316231208977 – Supplemental material for Older Age, Male Sex, and Early Start Time Lengthen the Recovery Room Stay Following Total Joint Arthroplasty in an Ambulatory Surgical Center
Supplemental material, sj-docx-3-hss-10.1177_15563316231208977 for Older Age, Male Sex, and Early Start Time Lengthen the Recovery Room Stay Following Total Joint Arthroplasty in an Ambulatory Surgical Center by Matthew J. Schultz, Hope S. Thalody, Rex W. Lutz, Quincy T. Cheesman, Alvin C. Ong, Zachary D. Post and Danielle Y. Ponzio in HSS Journal®
Supplemental Material
sj-docx-4-hss-10.1177_15563316231208977 – Supplemental material for Older Age, Male Sex, and Early Start Time Lengthen the Recovery Room Stay Following Total Joint Arthroplasty in an Ambulatory Surgical Center
Supplemental material, sj-docx-4-hss-10.1177_15563316231208977 for Older Age, Male Sex, and Early Start Time Lengthen the Recovery Room Stay Following Total Joint Arthroplasty in an Ambulatory Surgical Center by Matthew J. Schultz, Hope S. Thalody, Rex W. Lutz, Quincy T. Cheesman, Alvin C. Ong, Zachary D. Post and Danielle Y. Ponzio in HSS Journal®
Supplemental Material
sj-docx-5-hss-10.1177_15563316231208977 – Supplemental material for Older Age, Male Sex, and Early Start Time Lengthen the Recovery Room Stay Following Total Joint Arthroplasty in an Ambulatory Surgical Center
Supplemental material, sj-docx-5-hss-10.1177_15563316231208977 for Older Age, Male Sex, and Early Start Time Lengthen the Recovery Room Stay Following Total Joint Arthroplasty in an Ambulatory Surgical Center by Matthew J. Schultz, Hope S. Thalody, Rex W. Lutz, Quincy T. Cheesman, Alvin C. Ong, Zachary D. Post and Danielle Y. Ponzio in HSS Journal®
Supplemental Material
sj-docx-6-hss-10.1177_15563316231208977 – Supplemental material for Older Age, Male Sex, and Early Start Time Lengthen the Recovery Room Stay Following Total Joint Arthroplasty in an Ambulatory Surgical Center
Supplemental material, sj-docx-6-hss-10.1177_15563316231208977 for Older Age, Male Sex, and Early Start Time Lengthen the Recovery Room Stay Following Total Joint Arthroplasty in an Ambulatory Surgical Center by Matthew J. Schultz, Hope S. Thalody, Rex W. Lutz, Quincy T. Cheesman, Alvin C. Ong, Zachary D. Post and Danielle Y. Ponzio in HSS Journal®
Supplemental Material
sj-docx-7-hss-10.1177_15563316231208977 – Supplemental material for Older Age, Male Sex, and Early Start Time Lengthen the Recovery Room Stay Following Total Joint Arthroplasty in an Ambulatory Surgical Center
Supplemental material, sj-docx-7-hss-10.1177_15563316231208977 for Older Age, Male Sex, and Early Start Time Lengthen the Recovery Room Stay Following Total Joint Arthroplasty in an Ambulatory Surgical Center by Matthew J. Schultz, Hope S. Thalody, Rex W. Lutz, Quincy T. Cheesman, Alvin C. Ong, Zachary D. Post and Danielle Y. Ponzio in HSS Journal®
Supplemental Material
sj-docx-8-hss-10.1177_15563316231208977 – Supplemental material for Older Age, Male Sex, and Early Start Time Lengthen the Recovery Room Stay Following Total Joint Arthroplasty in an Ambulatory Surgical Center
Supplemental material, sj-docx-8-hss-10.1177_15563316231208977 for Older Age, Male Sex, and Early Start Time Lengthen the Recovery Room Stay Following Total Joint Arthroplasty in an Ambulatory Surgical Center by Matthew J. Schultz, Hope S. Thalody, Rex W. Lutz, Quincy T. Cheesman, Alvin C. Ong, Zachary D. Post and Danielle Y. Ponzio in HSS Journal®
Supplemental Material
sj-docx-9-hss-10.1177_15563316231208977 – Supplemental material for Older Age, Male Sex, and Early Start Time Lengthen the Recovery Room Stay Following Total Joint Arthroplasty in an Ambulatory Surgical Center
Supplemental material, sj-docx-9-hss-10.1177_15563316231208977 for Older Age, Male Sex, and Early Start Time Lengthen the Recovery Room Stay Following Total Joint Arthroplasty in an Ambulatory Surgical Center by Matthew J. Schultz, Hope S. Thalody, Rex W. Lutz, Quincy T. Cheesman, Alvin C. Ong, Zachary D. Post and Danielle Y. Ponzio in HSS Journal®
Footnotes
Declaration of Conflicting Interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publicationeclares relationships with Smith and Nephew and Stryker. Z.D.P. declares relationships with Orthodevelopment and Depuy. D.Y.P. declares a relationship with Depuy Synthes. The other authors declare no potential conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human/Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
Informed Consent
Informed consent was waived for all patients included in this study.
Level of Evidence
Level IV: Retrospective prognostic study.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.