
Abstract
In emergency medical services (EMS), the clinical reasoning (CR) of registered nurses (RNs) working in ambulance care plays an important role in providing care and treatment that is timely, accurate, appropriate and safe. However, limited existing knowledge about how CR is formed and influenced by the EMS mission hinders the development of service provision and decision support tools for RNs that would further enhance patient safety. To explore the nature of CR and influencing factors in this context, an inductive case study examined 34 observed patient–RN encounters in an EMS setting focusing on ambulance care. The results reveal a fragmented CR approach involving several parallel decision-making processes grounded in and led by patients’ narratives. The findings indicate that RNs are not always aware of their own CR and associated influences until they actively reflect on the process, and additional research is needed to clarify this complex phenomenon.
Keywords
Background
Emergency Medical Services
In emergency medical services (EMS) focusing on ambulance care, clinical reasoning (CR) plays an important role in providing treatment that is timely, accurate, appropriate and safe. However, a lack of knowledge about how CR is formed and influenced during the EMS mission has hindered the purposeful development of service provision and decision support tools for clinicians that would further enhance patient safety. According to the World Health Organization (2008), EMS is an important component of an advanced healthcare system’s capacity to provide timely care for the injured and acutely ill, but EMS standards differ internationally in terms of staffing, education level and care provision (Al-Shaqsi, 2010; Bos et al., 2015; WHO, 2008).
Standards of staffing and care provision can be classified as basic or advanced life support (BLS or ALS), and/or Franco-German or Anglo-American systems. The BLS and Anglo-American model provide care on a ‘load and go’ principle, which means that most patients are transferred to an emergency department for further assessment by a physician. On-scene treatment is limited and non-invasive and may include basic cardiopulmonary resuscitation, fracture splinting and, in some cases, oxygen administration. Transport to hospital is often rapid, with less time spent at the scene. In contrast, the ALS and Franco–German system provide care on a ‘stay and stabilize’ principle, which means that fewer patients are transferred to an emergency department. Instead, patients may be taken directly to a hospital ward, referred to community health care or left at the scene following assessment and potential treatment. ALS may also include invasive procedures such as endotracheal intubation, intravenous lines and administration of potent controlled drugs. Direct comparison of the two systems is difficult, as application contexts and regulations differ significantly, and there are no unified measures or international standards (Al-Shaqsi, 2010).
In Sweden, RNs must complete 3 years of higher education and a bachelor’s degree. They may also study for a further year to gain a master’s degree in ambulance care, but this is not currently a requirement for working in EMS. RNs are authorized to administer about 40 drugs independently and to make triage and treatment decisions in accordance with written guidelines or general requirements specified by their organization’s physicians (Lindström et al., 2015). A Swedish RN’s skills and competences are comparable to those of an ALS paramedic or combined elements of the Anglo-American and Franco-German systems (Al-Shaqsi, 2010).
Sweden’s EMS has developed rapidly over the last two decades and RNs in ambulances can provide life-saving health care both on the scene and during transport, making decisions about the most suitable level of patient care: emergency department, specialist treatment, referral to a local healthcare centre, treatment at the scene or non-conveyance (when the patient is not transported by ambulance) (Lindström et al., 2015). Care and treatment may be provided at the patient’s home and in a range of settings (indoor, outdoor, public, private, urban or rural), as well as in the ambulance or at a healthcare facility. These care decisions require extensive real-world experience, as any uncertainty can pose a threat to patient health and trust (Lindström et al., 2015; Norberg-Boysen, 2017; Rantala, 2017). Since 2005, Swedish law (National Board of Health and Welfare, 2009) requires the presence of an RN in every ambulance vehicle, and developments in Swedish EMS place increasing emphasis on the RN’s ability to assess patients, employing CR to ensure timely care and treatment and to make decisions about the most appropriate level of health care.
Clinical Reasoning as a Cognitive Work Process
Several accounts characterize CR as an overarching cognitive process of gathering, evaluating and discarding information to determine the best action as perceived in a given context (Higgs & Jensen, 2019; Simmons, 2010). This process is seen to involve a set of interrelated and overlapping parts, often described as primary macrocognitive functions that include ‘detecting problems’, ‘sensemaking’, ‘adapting’, ‘replanning’, ‘coordinating’ and ‘decision’ (Patterson & Hoffman, 2012). Although this cognitive work is fundamentally similar across high risk environments such as aviation, control centres and military command posts, we use the term CR here to specify the clinical element of this work in the present context (EMS).
In EMS settings, actions are informed by RN–patient assessment, based on information provided or acquired about the patient and the situation. To make informed care and treatment decisions, RNs must reflect on multiple informational cues and may be influenced by factors related to individual cognitive and/or affective disposition (Croskerry, 2002; Croskerry et al., 2013). Despite claims that knowledge, experience or support tools can help to overcome these issues, there is a widespread view that CR involves both intuitive and analytical thinking (Croskerry et al., 2013; Evans et al., 2013; Norman et al., 2017) and that the process is likely to be influenced by biases and knowledge deficits (Norman et al., 2017).
Clinical Reasoning in Healthcare Research
Clinical reasoning has attracted significant research interest, especially in hospital contexts. While these studies often focus on physicians and patient safety, some recent work has taken a broader view (Andersson et al., 2019; Perona et al., 2019; Sedlár, 2020), with increased attention to CR in EMS contexts. Much of the extensive research on CR relates to diagnosis, including the accuracy of EMS field diagnoses as compared to hospital discharge diagnoses (Magnusson et al., 2020; Wilson et al., 2018) and difficulties in assessing or managing conditions like sepsis (Sjösten et al., 2019), stroke (Andersson et al., 2018) or cases involving resuscitation (Andersson et al., 2021; Brandling et al., 2017).
Other topics include ethical issues around EMS missions (Bremer & Holmberg, 2020; Torabi et al., 2019) and systemic or organizational influences (Blodgett et al., 2021; O’Hara et al., 2014). However, these retrospective studies often fail to capture the dynamics of EMS processes that cannot later be fully accounted for. In particular, CR processes are thought to be influenced by issues beyond the physical encounter with the patient (Andersson et al., 2019; Blodgett et al., 2021; Hernborg et al., 2020; O’Hara et al., 2014).
To address this complexity, there is a need for more empirical data on CR among expert EMS RNs. This is crucial if we are to understand how CR can be supported, given its decisive impact on patient safety along the healthcare chain (Croskerry, 2017; Hagiwara et al., 2019; Singh et al., 2014). To that end, the present study investigated CR activities and processes at every stage of the EMS mission.
Rationale
Emergency medical services development efforts emphasize the importance of RNs’ CR capability in assessing patient needs and making decisions about appropriate care and treatment. Studies of CR in EMS contexts have typically focused (often retrospectively) on particular clinical conditions and the physical encounter with the patient. For that reason, little is known about the CR process at different stages of the EMS mission or the cognitive factors that influence clinical practice. These issues are central to the development of decision support tools and work processes that can improve patient safety by supporting RNs’ CR.
Aim
The aim of the present study was to explore and describe RNs’ CR and influencing factors during EMS missions, focusing on ambulance care. To that end, the study addressed the following questions. (1) What are the relevant sources of information? (2) What factors are influential? (3) How do RNs describe the CR process?
Method
Employing a qualitative single case study design (Yin, 2014), the study explored EMS as a contextually and socially bounded system comprising the organization, its employees and a geographical catchment area.
Setting
The research setting was an EMS organization in southwestern Sweden comprising nine EMS stations, with eleven 24/7 ambulances and four additional daytime ambulances available Monday to Friday. Covering an area of 2685 sq miles (6956 km2) with a total population of approximately 300,000, the organization’s rural and urban EMS stations serve local populations ranging from 9500 to 114,000 inhabitants, typically completing about a hundred missions each day.
The organization’s employees include RNs (some with a specialist education) and emergency medical technicians (EMTs) who have completed high school and 20–40 weeks of prehospital care education (National Board of Health and Welfare, 2009). The EMS team consist of two RNs or one RN and one EMT; in terms of skills and competences, they (EMTs) are comparable to BLS paramedics. During missions, team members take turns caring for the patient and driving the ambulance; this is determined by the patient’s condition, and the RN always assumes medical responsibility within the team.
Study Participants
Participant demographics.

Data Collection
Data distribution.
The observation protocol was pilot tested to specify a structure for observation field notes. The pilot study indicated that the protocol was considered too rigid and difficult to use, and observers subsequently captured detailed field notes spontaneously, referring to the protocol for reminders. The pilot also highlighted the need to audio-record discussions in the ambulance cockpit en route to the patient.
Each patient encounter was defined as one observation (see Appendix A for details). The authors (UA and BWS) followed a team for a full work-shift (8–14 hours, day/night, 1–6 observations per shift). RNs were asked to work as usual and to ignore the researcher, who maintained a low profile throughout. When embarking on a mission, an audio-recorder was placed in the cockpit to capture information about any preparations and discussions during the drive to the patient (n = 15; min = 2 minutes, max = 40 minutes; total: 231.5 minutes). Supported by field notes (min = 1 page, max = 7 pages; total: 112 pages), researchers documented the observable elements of RNs’ CR (n = 34; min = 13 minutes, max = 172 minutes; total: 108 hours), including communication, discussions and physical actions involving the RN, the patient and/or bystanders. After each observation, when and if operational demands permitted, the researchers conducted a follow-up interview (n = 22; min = 0.5 minutes, max = 29.5 minutes; total: 223 minutes) to address any questions arising, focussing on content, information gathering and reflections. To elucidate CR, the RN was asked to re-tell, elaborate or explain the ‘how’ and ‘why’ of what they did and any mission-related events that the observer was curious about. Typical questions included the following. ‘I noticed that you and your colleague disagreed on this matter, is this common? How do you usually resolve it?’ ‘How do you reason about the differing narratives of patient, relatives and healthcare personnel?’
Digital patient journals (n = 34) from the observations were audited to determine whether and how RNs documented their CR. In addition, UA and HA conducted one group interview (duration 90 minutes, n = 3), asking three main questions to elicit description and discussion of CR. (1) Please describe how you perceive and implement CR in your clinical work. (2) In your experience, what influences your ability to engage in CR? (3) Is there anything else that you or someone else could do to facilitate CR? At the beginning of the group interview, the concept of CR was introduced, and participants could request clarifications. CR was described as part of the reasoning process involved in gathering, analysing, discarding and utilizing information in making decisions about care, treatment or other vital aspects of the mission. To encourage participants to share their views and develop their ideas, the researchers asked follow-up questions such as Could you elaborate on this? Or What do you mean when you say…? At the end of the interview, the researchers posed a final open question: Is there anything that arose during our interview that you would like to discuss further? This generated additional inputs that built on the preceding discussion. All field notes and recordings from the observations and interviews were transcribed and numbered accordingly.
Data Analysis
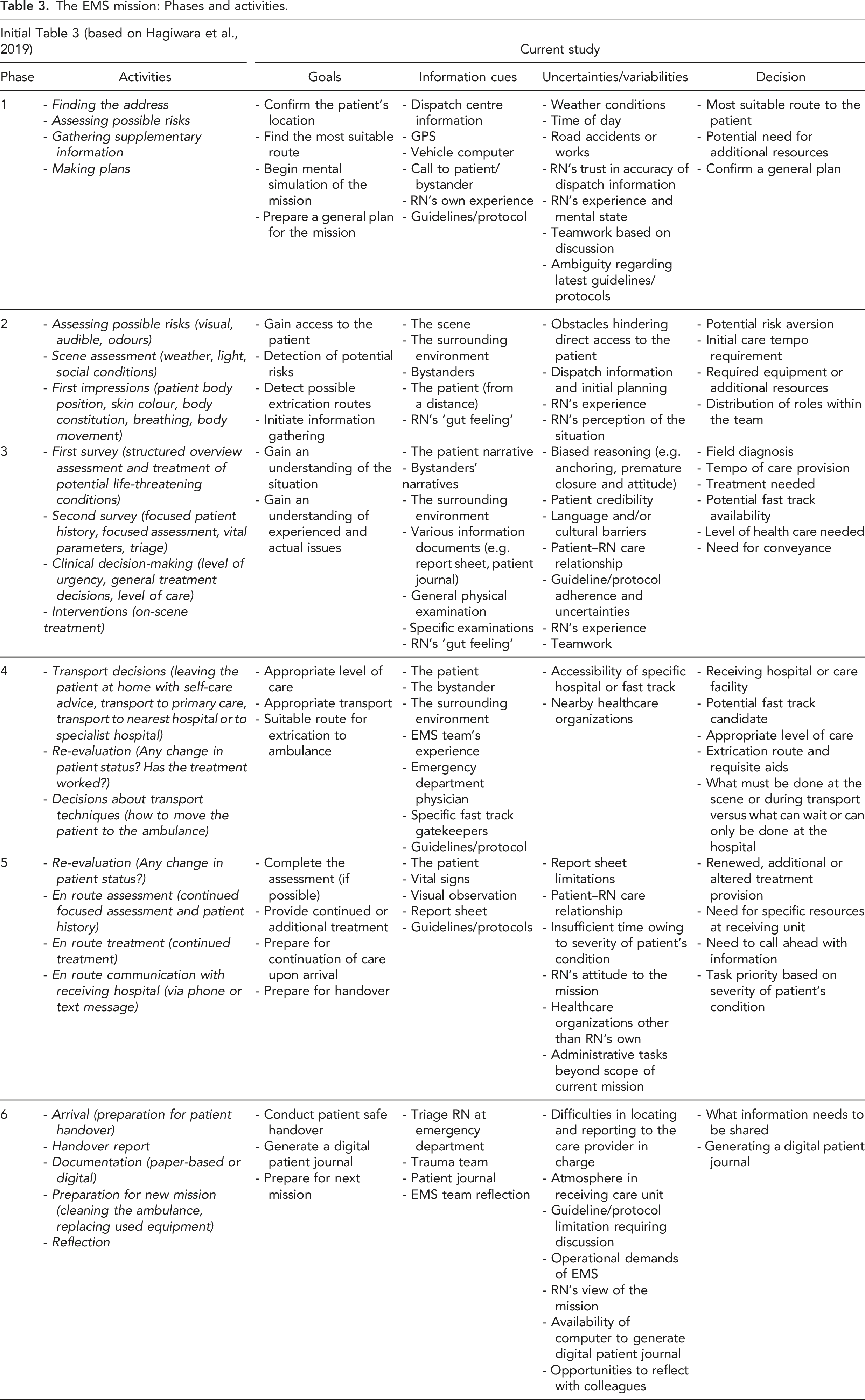
The EMS mission: Phases and activities.
Once the data had been assigned to the relevant phases, the researchers began to group similar content into clusters, describing elements of the CR process as subheadings. The inductive coding procedure was based on the content of the transcripts. Following Yin’s (2014) recommendations for case study research, triangulation was used to assess coherence or contradiction across different data sources by asking questions such as the following. Does the drive out recording align with what the RN shared in the follow-up interview or group interview? Does the patient journal reflect what occurred during the patient encounter? As the aim was to acquire nuanced descriptions of CR, less frequent data items were included in the analysis.
While the first author was responsible for the organization, clustering and initial analysis of the data, the authors engaged in frequent ongoing discussion about clustering, interpretation and the content of the resulting categories. Disagreements and queries were resolved by discussion until a common understanding was reached.
Ethical Considerations
The study received ethical approval from the Regional Ethics Approval Committee in Gothenburg (reference number 453-18). Approvals were also granted by the EMS organization manager (written) and the managers of each EMS station (oral). Each participant signed a consent form that included information about the study and acknowledged their right to withdraw from the study without explanation. Other ethical issues related to data protection and security were addressed by adhering to the Swedish data protection act (SFS 2018:218, 2018). This meant that all names, addresses or other identifying information related to patients and participants remained confidential and were stored in a security locker on a password-restricted portable memory card. A separate file contained participant identities and information, which were linked to the observations by means of unique identifier numbers. No information about the identity or location of RNs, patients and other individuals was included in the transcripts of field notes or audio recordings, which were anonymized before analysis commenced. Given the relatively small sample size at each site, special care was taken when reporting the findings to ensure that individual RNs could not be identified (e.g. by colleagues or managers). By ensuring maintenance of participants’ integrity and confidentiality, the study aligns with accepted ethical principles for research (World Medical Association, 2013).
Where appropriate, the researchers introduced themselves to patients, carers and other health professionals during the observations and briefly explained their role. The researchers sought to ensure that participants could continue to work without any interruption or distraction that might affect patient care. During the study, operational demands took priority, which meant that the researchers might suddenly find themselves excluded from the ambulance vehicle or having to find their own way home.
Results
Overall, the results depict CR in EMS as an iterative and fragmented process with fluctuating goals, based partly on information from various assessments. While the information gathered from context, examinations or provided by patients and bystanders may be consistent, it may change at any time during the EMS mission, making it more difficult for RNs to make informed and appropriate decisions. However, the patient’s narrative is often the key source of information, and patients generally exert a strong influence on CR. Our results highlight several decision-making processes during the EMS mission, all of which involve CR. These decisions cannot be made immediately or one by one; instead, RNs have to manage these processes in parallel, taking account of logistics, safety and administrative tasks as well as medical or caring issues while balancing the differing experiences, opinions and requests of patients, bystanders, receiving care units and the RN’s own organization.
The results are presented here in chronological order, reflecting the phases of the EMS mission, with content-related subheadings (see also Table 3). At the end of each phase, a synthesis summarizes the key findings.
Phase 1: Receiving the Call and Driving to the Address
[The RNs are preparing for lunch and while they are waiting for the microwave to finish there is a beeping signal from the RNs radio and he looks at the screen] – RN1: It’s a priority 1, possible ongoing seizures… – RN2: Well, there goes that lunch again…is it far? – RN1: No, not that far but you could probably eat something on the way. [The RNs put their food into the fridge and walk out to the ambulance garage. On entering the ambulance, they check the vehicle computer for mission information] – RN1: I believe this one is known to us, I have been there before I think….but not for seizures. [Reads from the vehicle computer] ‘normal breathing, a bit blueish in the face, ongoing seizures’. I wonder if this really is this person or if it could be someone else there? [During the relatively short drive (approximately 10 minutes) through town, the RNs talk about the patient’s location and possible entry points to the address. Shortly before arriving at the location, they get an update on the vehicle computer; the seizures have stopped and the patient’s face colour is closer to normal, but the patient is seemingly still unconscious].
Narrative/Goal
This phase includes events from the time the RN receives a call from the dispatch centre to their arrival at the patient’s location. RNs first receive information from the dispatch centre via their handheld radio and the vehicle computer, which initiates the EMS mission and RNs’ associated CR process. In this phase, RNs’ main goals are to locate the patient(s) and find the most suitable route to that location. Secondary goals include mental simulation of the upcoming patient encounter and identifying any potential need for specific assessment, treatment, fast tracking or other solutions.
Primary Information Cues
In this phase, information received from the dispatch centre is the primary source. This varies in quantity and detail but typically includes a priority level (1, 2 or 3) and the patient’s name, age and location, along with a more or less detailed description of the situation or the reason for calling the emergency number. The vehicle computer’s global positioning system (GPS) provides coordinates for the patient’s exact location.
Additional Information Extraction (Specific Questions/Probes)
If the RN believes that additional information is needed, they may contact the dispatch centre, either by cell phone or radio or by updating the case information on the vehicle’s computer. Requests for additional information typically seek to establish who called the emergency number and whether there is a need for additional resources such as ambulance, police or fire services.
If several ambulance resources are assigned to the same mission, RNs can utilize the GPS and vehicle computer to locate the other units and estimate their time of arrival at the destination. If other units are already on site, RNs may try to establish radio or cell phone contact to get a more detailed description from the scene whether additional units are needed or whether any additional units can be dismissed. The vehicle computer can also supply assignment updates and information about roadworks that may hinder progress or limit route selection. In the case EMS, information from shift meetings about road blockages, new treatment guidelines, hazardous addresses and other current issues are shared across the organization.
During the drive to the patient, RNs consult guidelines to check dosages of relevant pharmaceuticals or to update knowledge of relevant fast tracks. The guidelines may also specify conditions that always require conveyance, especially for first-time patients. Finally, the guidelines include a list of keys for gaining access to various residential and industrial areas. To accelerate access to the patient, RNs can search these lists to find the relevant gate key. RN2: [reads the dispatch information] Well if she had a hip replacement already, will she be excluded from the hip-fast track? RN1: It depends on the procedure, I think… RN2: [checks fast track protocol] No, it only says ‘exclusion if previous hip procedure’… – Observation 14
If the RN is unsure whether the nearest receiving hospital will accept and treat the relevant category of patient, they will typically make contact to find out, which saves time when deciding which hospital should receive the patient and on subsequent arrival.
Making Sense of Information
Based on the information gathered from primary and secondary cues, the RN begins planning to locate and access the patient. The appropriate route may not be the shortest driving distance; the selection process must take account of current weather conditions and potential risks – for example, slippery road conditions or rush-hour traffic. These decisions are often based on the RN’s previous experience or knowledge of the local area, along with any additional information provided at the shift handover.
Any information obtained from dispatch must be interpreted; RNs refer to this as ‘reading between the lines’. Initial planning is relatively short and imprecise and generally involves mental simulation of the assignment. RN1: [reads the dispatch information on the vehicle computer] But this paresis on the right side—would it be from the previous strokes?
RN2: It could be, but it could also be a subarach bleed [in the brain] or something.
RN1: Perhaps —we’ll have to assess the patient properly when we get there.
RN2: It’s probably as in 9 out of 10 cases—they have forgotten to write some of the information. – Observation 29
At this point, the RN also begins to plan for possible appropriate treatment options and estimates a suitable tempo for initial care. Regarding the described care need, potential fast tracking is considered if the patient meets the relevant inclusion criteria. Possible field diagnoses and receiving hospitals are discussed (if several options are available). In some cases, RNs know the patient’s name or address, which can help them to envisage the nature of the assignment; this also applies to specific care facilities, staff and patients.
RN1: I think we should give the patient Ondansetron [antiemetic], Rapifen [analgesic] and Morphine [analgesic].
RN2: Just remember that this patient is older and more fragile, so be careful and perhaps only use Ondansetron and Morphine. – Observation 31
Practical solutions or workarounds (Practical and creative solutions to a given problem that are not covered in the guidelines or are unfeasible using the equipment provided) are also discussed; for example, considering application of a urine catheter may prompt a non-conveyance decision, as the reason for potential hospital admission may be averted. RNs also share information with their colleague based on previous experience or more general knowledge acquired from education or the media that is not always relevant to the current mission.
RN2: I really hope they have tried to apply a new urine catheter. Should we try to apply one if they have not? Then [the patient] could stay at home instead.
RN1: Yes, why should they have to do that in the emergency department? Such a waste of resources. They must have a RN at the facility that can do this instead of the ambulance. – Observation 23
Colleagues are the main support for mission-related reasoning and planning and bring nuance to the discussion by raising possible alternative scenarios and solutions. However, they may also contribute to a one-sided picture based on presumption and interpretation. For example, the RN’s mental simulation and anticipated field diagnoses may vary even when interpreting the same information, which suggests that CR is influenced by the RN’s current state of mind, as well as by experience and triggers from personal experiences in their private life.
RN2: But we talked about this on the way to the patient—that the symptoms had first appeared a couple of days prior to the emergency call. It sounded exactly like my relative’s myocardial infarction.
RN1: And I was moaning, first of all, he had been having chest pains since Friday [suggesting that this would not be anything urgent at all] ...’What day is it today’, I said. ‘Sunday’ you [RN2] said, and ‘It sounds just like your relative’s myocardial infarction’, yes. – Observation 14
Challenges and Uncertainties
RNs tend to use their local knowledge, following well-known routes rather than blindly trusting the GPS because they know it does not always select the optimal route. Another issue in planning the route to the patient is that RNs may try to plan their route to avoid overtime, which is a frequent occurrence at the end of a shift. However, this seems to apply mainly to low-priority calls. RNs also sometimes choose alternative routes simply to explore or for variety, although this again seems to happen mainly on low-priority assignments.
More generally, RNs seem to engage less in CR when the assignment involves a low-priority patient – usually someone being transported between different care facilities. While RNs acknowledged this, the data indicate some level of CR, which suggests either that CR is partly unreflective or that RNs do not regard their seemingly casual discussion as CR.
RN1: Well this patient is going to the palliative care ward, so there’s no need for proper triage.
RN2: No, we didn’t do any triage on this one the last time either. I believe it was more important to maintain a connection and conversation with the patient than to triage at this stage. – Observation 21
Mental simulation of the upcoming patient encounter is partly inhibited by RNs’ experiences that information from the dispatch centre does not always fully correspond to the actual situation on the ground. Mental simulations are based on the RN’s clinical and personal experiences and the plausibility of field diagnoses, which may depend on dispatch information or the RN’s own (or collaborative) reasoning. IP2: You do start to prepare mentally for the assignment based on the dispatch information. Say there is a suspected sepsis; then I will at least start planning for early [intravenous] administration of fluids and additional medical treatment. Then again, [the information] could turn out to be inaccurate on arriving at the patient, but I still prepare nonetheless. IP3: Well that’s true IP2—we do that. But then again, you have learned from experience that just because the information says something—positive or negative—you would not trust it entirely, at least not in the same way as when you were new… – Group interview
These team discussions seem to lessen at night, perhaps because of fatigue or perhaps simply because of team differences. Even if the dispatch centre provides adequate information, RNs may overlook it because they are sometimes distracted by their own conversation. RNs reported that they relax a little if the patient is at a care facility, as other healthcare professionals are perceived to have the situation under control.
On occasion, the attending EMS crew may change during a patient encounter, usually to avoid overtime. The end-of-shift RN provides a short oral report about the patient and the current situation stating what has been done and whether anything further needs to be done before reaching the hospital.
Decisions Made
The main decisions in this phase include choosing a route to the patient and deciding whether there is a need for additional resources. However, there is also a great deal of initial planning for the upcoming patient encounter in terms of possible reasons for the patient’s call, suitable treatments, selection of a receiving hospital and potential fast tracking. In most cases, these discussions end with ‘We’ll just have to wait and see when we get there’, confirming that although RNs may want to plan ahead, they must keep an open mind for additional information from the physical encounter.
Synthesis Phase 1
Phase 1 is the starting point for the mission and the upcoming patient encounter. The RN’s CR is shaped by information from the dispatch centre, typically generating one or more mental simulations with differing goals and a rough plan for anticipated events: locating the patient, field diagnosis and treatment, possible extrication routes (for a known location) and possible receiving hospitals. Individually or as a team, RNs initiate patient care by sorting and connecting the various threads of initial information. Dispatch centre information is interpreted by reading between the lines to account for what is and is not mentioned. RNs can supplement and develop each other’s CR but may also inhibit or impair the process. In general, team-based simulation and planning plays only a very small part in Phase 1, and most of the conversation among RNs is about life in general.
Phase 2: Arrival at the Scene
[The RNs are arriving at the street where the patient is situated] – RN1: Okay, we’ll just grab the bag first and see what we have to work with. [RN2 looks at the house numbers to locate the right address] – RN2: I think it’s the house up there on that hill—could be a tricky one if the patient can’t walk down himself. – RN1: Well there are the bystanders. They look quite calm anyhow, perhaps it is not so bad… [turns off the engine and exits the ambulance]. Hello there, are you the one who called?...
Narrative/Goal
This phase includes activities from the time of arrival at the patient’s location to physical assessment of the patient. The main goal is to gain access to the patient to begin the physical encounter. Secondary goals include assessing the surrounding environment for potential risks, identifying extrication routes and noting any cues that provide information about the patient and their condition.
Information Cues
On arriving at the scene, RNs said they sometimes feel that something about the situation is not right. This feeling seemed difficult to put into words but apparently relates to interpretation of the surrounding environment, including bystanders such as the patient’s relatives, witnesses or other healthcare professionals. RNs noted that they evaluate bystanders’ behaviour (e.g. stressed, agitated and calm) as a means of estimating the severity of the situation they are about to encounter. RN2: We were met at the entrance by a person [the parent] who was very calm and said ‘Hello and welcome, they are in that room over there’. At that point, it felt like…you got a whole other impression of the situation [unlike the dispatch information]. – Observation 13
At this point, information acquired from bystanders typically relates to whether this is the right address and where the patient is located. RNs said that the surrounding environment is an important source of information about what has happened to the patient and when the problem arose.
Other relevant indicators include the weather, which could cause the patient’s situation and status to worsen rapidly. In the case of a traffic accident, the primary RN will scan the scene en route to the patient to assess cues such as distance of travel, skid or brake marks and damage to the vehicles involved. Whether indoors or outdoors, RNs will attempt to identify suitable extrication path(s), noting potential obstacles like staircase design, elevator size or a slippery slope that might impede access to the ambulance.
Even at a distance, a first glimpse of the patient allows the RN to make an initial assessment of their condition and its severity. The information gathered at this point is mainly visual and includes breathing pattern, skin colour (cyanosis, cold sweat and pallor), movement pattern, body position and any signs of pain or nausea. RN1: … and then again, I look at the patient directly after arriving from the stairs. I notice that he is standing up straight, that he is breathing normally and that his [skin] colour is fine. These things take an instant in my mind [and tell me] that he is in no apparent danger. Then I notice from his facial expression that he is in pain. Still, I make a very swift decision in my mind that there might not be any need for conveyance with us to an emergency department…possibly too swift. – Observation 11
Additional Informational Extraction (Specific Questions/Probes)
En route to the patient, the RN will ask any bystanders to provide a brief description of what happened or to outline the current situation.
Making Sense of Information
In the final minutes before reaching the patient’s location or while parking the ambulance, the RN will engage in a short discussion – usually more like a statement – about what equipment to bring initially to the scene. Among other things, this may include a rucksack of medical equipment for measuring vital signs (blood pressure cuff, pulse oximeter, thermometer, β-glucose metre and stethoscope), items for administering the relevant drugs, ECG equipment and the ambulance stretcher. If no equipment is mentioned, it is implicitly understood that only the rucksack should be brought to the patient.
In a home setting, environmental cues may offer some sense of the patient’s everyday life: neat and tidy but with a layer of dust, the state of the flowers on display, perhaps a certain smell or scent. These cues may contribute to subsequent decisions about whether the patient is in need of additional everyday assistance and may also help to link or validate other cues.
IP3: I’m fascinated by the amount of information you can gather before you even see the patient. I did not have this experience in my early EMS career even though I had been working as a RN for several years. How do you explain this to someone who is new to the profession—the [significance of] the dead flowers on the staircase or how the wife acts when her husband is ill?
IP1: Well, the difficult part is how to share this later. I mean, when you attend a patient who is intoxicated, it is important to locate the empty packages in order to establish what they have taken. But how are we to report the things that IP3 said? I mean, you can provide a little environmental information about whether there are steps to the front door, the lack of an elevator and other things that it might be useful to know before the patient leaves the hospital. – Group interview
These first impressions also give the RN some sense of an initial care tempo and whether a more cautious or adapted first contact approach is needed. These decisions seem to be based on experience and are typically made subconsciously. RN1: I observe the breathing pattern and the colour of her skin…the body posture; at this time, she is lying down, but I can still see…that it looks relatively fine when we enter the room. I sit down next to her and begin talking… I keep thinking that she is relatively young [about 15] and that I need to be gentle—not just to go straight into examinations but to let her talk a bit first. – Observation 9
Challenges and Uncertainties
Gaining access to the patient is not always a straightforward task. For example, locked gates may require the RN to search for a door code or telephone number from dispatch or from the caller, or it may be necessary to walk some distance to reach the patient. Where possible, neighbours may be asked to assist in gaining access to certain areas. Other barriers might include houses or apartment doors without numbers, names or addresses; sometimes access depends on persuading a patient with dementia to open their front door by talking to them through the letterbox. [We arrive at a four-storey apartment building. On arriving at the entrance, the RNs realize that they need a door code. RN1 sprints back to the ambulance to check the vehicle computer, but there is no [code]. RN2 then contacts dispatch to see if they have the code, but they do not. The observer spots some neighbours looking out through one of the windows and tries to signal to them to open the entrance door…//… On arriving at the right apartment, the door is again locked, and a letterbox conversation begins.] – Observation 18
Decisions Made
Decisions made in this phase relate to which equipment RNs might need immediately and what can be left at the ambulance until later. The distribution of roles within the team may depend on the specific mission but may also relate to the team itself and whether they are accustomed to working together.
Synthesis Phase 2
In this phase, RNs begin to evaluate, verify and discard information received in Phase 1, drawing on supplementary cues from bystanders and the surrounding environment. At this stage, they also begin to develop an initial plan for patient extrication. By gaining access to the scene and the patient, they can confirm, reject or restructure their initial hypotheses. This phase is usually relatively quick – typically one to three minutes – depending on the equipment needed and any difficulties in gaining access to the patient. Information gathered in this phase seems to form a foundation that RNs return to for pattern matching throughout the patient encounter. In other words, RNs check whether the information provided by the patient aligns with information from dispatch and what they noticed on their way in. This is also the beginning of sense making in the current situation.
Phase 3: On-Scene Assessment and Treatment
[When the RNs arrive upstairs, they see the patient standing and leaning over a table, her face telling of her pain. The primary RN walks up to her and presents herself.] – RN1: Hi there, I am Christina from the ambulance. This looks very uncomfortable—could you tell me what has happened? [The patient describes a pain that has been increasing in intensity for a period of time and [says that] when she woke up today she could not move at all. During this time the second RN measures vital signs and takes notes in a paper journal.] – RN1: Well, based on what you told me, it seems the ED is not the most suitable place for you. We could perhaps help you with some prescriptions for pain medication and make an appointment with the local healthcare facility – what do you think? – Patient: Well, I just had that thought as well about local healthcare… – RN1: Perfect, I will just have to make some calls – first to our physician at the ED for the medications and then to the local healthcare facility.
Narrative/Goal
This phase includes events from the moment the RN can physically touch the patient to the decision about moving the patient and extrication to the ambulance for further care and transfer. The main goal is to assess the patient and the situation to identify perceived and actual issues that may need to be solved. This information forms the basis for deciding whether there is a need for treatment on the scene, hospital care, referral to a more suitable level of care or non-conveyance.
Information Cues
The patient is the primary source of information for RNs. After acquiring the patient’s narrative (primarily through direct verbal communication), bystanders may be invited to share their perspectives and experiences of the situation. These conversations may occur in parallel; bystanders may be interviewed separately or while the patient is completing other tasks like putting on their clothes or visiting the bathroom. Bystander narratives become more important when patients are unable, for whatever reason, to recount their experiences or are described as ‘not being themselves’. The observations confirmed that RNs tend to let patients describe and express their experiences freely; this content rarely deepens the patient narrative, but RNs seemed to gain sufficient information just by listening.
RN1: Please tell me, how do you feel?
Patient: I have this pain here on the right side [points to her back]… I had a kidney stone many years ago and this feels the same. [The patient shares her experience of a restless night, with severe pain, vomiting and diarrhoea that began at 05:00. She has not notified any of her relatives but just alerted home care personnel. While the patient shares her narrative, RN1 applies the pulse oximeter.] – Observation 8
If the bystanders include healthcare personnel at a care facility (e.g. health centre, nursing home and home care), RNs will usually receive a report sheet containing up-to-date information about the patient’s vital signs, current problems or conditions and medical history. These bystanders can also contribute to field diagnoses.
In addition to patient and bystander narratives, RNs gather information from physical examinations that measure vital signs (pulse, oxygen saturation, blood pressure, temperature and blood glucose), as well as examinations targeting specific conditions (e.g. electro cardiogram, lung/abdomen auscultation and neurological assessment). RNs reported using the ‘A-E principle’ (airway, breathing, circulation, disability and exposure) to assess their patient. Although RNs said that they perform A-E-assessments, our observations indicate that this assessment is performed subjectively. Other information cues for pain assessment included facial expression, body position and movement.
Additional Information Extraction (Specific Questions/Probes)
Patient and bystander narratives provide the RN with information about the patient’s everyday functioning, current medications and current and previous illnesses. RNs typically ask open-ended questions such as ‘What has happened?’, ‘What can we do for you today?’ or ‘How are you?’. However, these questions tended to become more specific when the patient provided insufficient information or if they had a previously known problem. In such cases, the RN might ask ‘What has been done earlier?’, ‘Have you received this drug?’, ‘When did it start?’ or ‘Where is it located?’.
RN1: Hello, I’m [name], the RN. How are you?
Patient: I can’t really say that I’m fine. I woke up again with chest pain, and it’s the same as before. I have had four myocardial infarctions, you see.
RN1: And when did the pain start? Have you taken any nitroglycerin? […//…] RN1: And what about the pain—where is it located? […//…] - RN1: What about the pain intensity on a 10-level scale?[…//…] - RN1: You should get some morphine for the pain; have you received it previously? – Observation 24
Making Sense of Information
To gain some understanding of how the patient’s condition differs from their habitual state, RNs seek to establish what the patient and any bystanders perceive as troubling, as well as what prompted the emergency call and what assistance the RN can provide. While the findings from physical examinations are evaluated in light of the patient narrative, the latter seems to be assigned greater importance. The participating RNs emphasized the importance of keeping an open mind while also listening closely to what patients share.
IP3: But then it is like when we meet a patient claiming to have severe breathing difficulties, and then they go and lie down flat on the bed. Then you might think to yourself ‘Breathing difficulties, yeah, right’. But then again, we have seen patients who really are struggling to breathe; they are not lying flat on a bed. You do interpret everything—not just what they say or [information from] examinations.
IP1: Just like someone who says ‘It’s not so bad’ but has to divide their sentence into three sections because it is too difficult to say it all at once (due to breathing difficulties). Then, we also know that this might be a little bit worse than they [the patient] are admitting. – Group interview
RNs also described ‘a gut feeling’ they sometimes get during the patient encounter, which guides their CR. This feeling seems to overrule clinical findings; for example, a patient may present with good vital signs, but the RN’s ‘gut feeling’ tells them that something is not quite right. RN2: And he did not seem like…as I said to the observer earlier…it did not feel like the patient just had a seizure that just disappeared. He felt like that he was a little worse than he should be, all clammy and … I thought it could just as likely be something cerebral—either from the fall itself or that he might have hit his head. – Observation 1
This gut feeling is apparently based on a combination of patient and environmental cues. The latter provide information about how a patient manages their everyday life (e.g. hygiene, cleaning and cooking), which may in turn indicate the duration of their current problem. As another example, the scene of a traffic accident tells a story about kinematics and possible injuries, and this may be supplemented by bystanders’ accounts and conversations. Based on our observations, RNs seem to refer to gut feeling as a source of information only when they suspect a more serious condition. While such a feeling would not support a field diagnosis in any case, it might prompt an RN to modify plans that were based on dispatch information or organization guidelines.
Work practices and CR processes differed across the observed teams. In some teams, RNs worked in parallel, interviewing patients and bystanders while performing examinations. The primary RN typically took the lead while the secondary RN listened to the conversation; on the basis of that content, they prepared the equipment needed to examine the patient or administer drugs and for patient extraction. The primary RN often shared their findings verbally while the others wrote them on the report sheet. RNs briefly shared their views about the current situation; once in agreement, they began to plan ahead. This approach requires each RN to engage in their own CR process to form an impression of the situation. Their colleague supports reflection on information provided, clinical findings and a suitable course of action. In combination with other information cues and guidelines, this shared reflection may change the mission goals. Even if the primary goal remains the same, the proposed course of action may have to be revised in light of the available options.
Challenges and Uncertainties
CR based on information gathering and mental simulation en route to a mission was liable to change when the scenario differed from what the team had prepared for, taking them by surprise and disrupting CR, as they had to formulate new goals. RNs said it was not particularly surprising when dispatch information differed from what they actually encountered; when their initial expectations were met, they would continue with their premade plans. RN2: I believe that, over the years, almost everyone learns that it is really difficult to make an assessment by telephone, and it is difficult for dispatch operators to gain a sense of what is actually needed. So you should arrive at the patient with a really open mind and then make a broad assessment, either confirming what you first believed or following a completely different track, for your own sake as well as the patient’s. – Observation 9
In pursuing a specific goal, the guidelines should provide a common structure to ensure the safety of RN and patient alike. However, RNs expressed some doubts about the guidelines, which they perceived as too rigid, potentially leading to transport delays and deterioration in the patient’s condition. For that reason, RNs did not adhere strictly to all of the examination or action guidelines; in this regard, RNs said they considered both the content of the guideline and their clinical experience in deciding on an appropriate workaround. According our guidelines, this patient should have been immobilized in the vehicle and extricated in that way … but to me this is a question of on-scene assessment. Sure, it might have occurred to me that he may be in need of immobilization, given the kinematics of the accident, but this suspicion was not that strong, which is why I told the patient to extricate himself from the vehicle in a calm and steady way, with our support…//… this approach to extrication was based on my assessment of the patient, with no signs of injury to the neck or spine. Sure, there was some muscle defence and soreness where the seatbelt had been, but this is still a healthy young person. In addition, I did not want to start cutting in this other bystander’s car [where the patient had been seated while waiting for the ambulance]. I am also aware of a change in the guidelines in the pipeline, which means we will be doing less patient immobilization of this kind, but I still have to consider immobilization to avoid being questioned or reported by the hospital. So, in this case, the patient extricated himself from the vehicle, and we could then immobilize him before entering the ambulance in a much less intrusive way than the guideline suggests. – Observation 16
Other reported difficulties included identifying the right guideline and establishing whether it was up-to-date. Additionally, as guidelines are applicable only within the RN’s own organization, they must find ways of implementing those guidelines when engaging with other organizations.
RNs acknowledged that they sometimes have only a basic perception of the situation rather than a complete picture. They sometimes ask the same questions several times and receive different answers or none at all. They did not explain how they decide on an answer to incorporate in their CR beyond noting the validity of that information to the extent that it provides information about the patient’s mental status. RN1:[…//…] But then again, if their [patients’ and bystanders’] stories really contradict each other, who do you choose to believe?... as I said previously, sometimes you have to just accept that you do not have the complete picture. – Observation 2
Other factors identified as influencing CR included language barriers and disinterest in sharing information. Depending on the situation, time factors and those present, the RN might also seek further information to gain a deeper understanding of the patient’s psychological status, including relationships with their partner, family, friends or work colleagues and managers.
Gut feeling may be influenced by a number of factors, including the RN’s attitude and whether they have made up their mind beforehand about the patient’s problems rather than keeping an open mind. Other possible influences include the patient’s cultural background, which may explain expressions of discomfort or pain that the RN does not usually encounter in their private or professional life. More generally, gut feeling seems to grow exponentially with experience. IP2: Then I believe that our attitude on arrival at the patient matters. If you have already made up your mind—based on the initial information, where the patient lives or what their residence looks like—that ‘this is not going to be so bad’, you may already have judged the patient and therefore have more difficulty keeping an open mind. – Group interview
While team members’ CR may sometimes differ, any disagreements are usually resolved through discussion, and the primary RN seems to have the final say. Discussion tended to fade during night shifts or at the end of a busy shift, with more frequent repetition of information and planning before both RNs grasped the situation. A less experienced RN’s ability to contradict a more experienced colleague was also an influential factor. IP2: I remember one occasion when I was new to EMS and my senior colleague biased our joint decisions on the scene. We were attending an elderly man that had fallen down. My colleague viewed this as a silly and unnecessary mission and felt that we should just put the patient on the stretcher without using immobilisation equipment. I remember feeling this was not the appropriate procedure, but I could not bring myself to argue with this senior colleague. I did not feel good at all afterwards, and I learned from it. – Group interview
On the other hand, RNs seem less likely to engage in CR when they encounter a patient at a healthcare facility or in a low-priority setting, although experience tells them that the mandatory examination may reveal a serious condition that was not discovered or reported during the handover. Decisions about conveyance and an appropriate receiving hospital are based in part on patient and bystander requests for care and treatment. In some cases, patients only want a ‘check-up’, perhaps in a combination with a follow-up by home care providers or the local healthcare centre. Observer: You [RN2] asked me if we should include this patient in the study, given that there isn’t much of an assessment. Do you make less of an assessment when the patient comes from a care facility?
RN1: Well, yes. I believe that one generally does that. I mean…a physician at the health care centre has written a referral having assessed the patient…
RN2: I also believe so. With other patients, you have to reason your way to some sort of field diagnosis, but this time, we already know the reasons for the need for transport to hospital. However, you still make basic measurements of vital signs and such.
Observer: And what if you find something else during your assessments?
RN1: Well, that happens—for instance, if there are chest pains, and the health care centre has not taken an ECG but you find an ST elevation or something else they have not reported. – Observation 3
Decisions Made
Decisions in this phase relate to the initial tempo of care: whether there is a need for urgent treatment or transport to hospital, or whether RNs can take their time in assessing the patient. The need for a specific on-scene treatment or assessment would indicate the patient’s main problem or inform a field diagnosis.
Synthesis Phase 3
This seems to us the most information- and event-rich phase of the EMS mission. In laying the groundwork for progressing the patient encounter, Phase 3 also puts CR to the test. Based mainly on the patient’s narrative, RNs must build a picture of the situation, ideally from several perspectives, prioritizing assessment of the patient’s status and developing an understanding of why emergency care was requested. Any information provided or gathered must be compared and evaluated against the dispatch information drawing on mental simulation and the relevant guidelines. As CR is grounded primarily in conversations with the patient, bystanders and one’s colleague, the process is likely to be undermined if verbal communication becomes complicated. One unanswered question is how RNs prioritize different sources of information, especially when these point to different alternatives; what informs CR in such situations? A further issue is that RNs must work on different decisions simultaneously during this phase, and if the relevant cues are fragmented, the CR process can become unduly complicated.
Phase 4: Transport and Departure
[We are standing in the living room of the patient’s apartment, which is on the third floor of a building with no elevator.] Looking at RN2, RN1 says: Well, she has to get to the hospital, but to get to the ambulance, we might need a mattress to drag down the stairs. But this little lady is a lightweight, so perhaps we could use the chair. – RN2: I think the chair would be quicker. I’ll go get it, and you give her something more for the pain in the meantime…
Narrative/Goal
This phase covers events from the RN’s decision about physical extrication of the patient to the point where the ambulance begins the drive to hospital. The goals are to select an appropriate level of care, a receiving hospital and appropriate transport if needed. Where there is a need for patient extrication to the ambulance, RNs must identify a suitable route.
Information Cues
As in previous phases, communication here is again mainly verbal, focussing on the patient’s wishes regarding the level and form of continued care as an element in the decision-making process. The surrounding environment is assessed for possible extrication routes – a process that often begins in Phase 2, noting paths and obstacles while gaining access to the patient. RN2: We sometimes suggest an appropriate level of care based on our presumptions, which are sometimes formed very early in the patient encounter. In this case, the patient was on the same page; she believed that we would be able to provide some pain management at her house and that she could remain at home and visit the health care centre later that day or the following day. – Observation 11
Additional Information Extraction (Specific Questions/Probes)
Some patients may wish to be referred to their local healthcare centre and can be helped to book an appointment; others may have no interest in further care. These decisions are often (but not always) discussed with a physician at the emergency department. These interactions may also relate to options for pharmaceutical treatment or ECG interpretation. Contact with a physician may also provide a solution that improves an unsustainable home situation.
Where there are several hospital options, some of these may be excluded on the basis of opening hours or available healthcare specialists. Contact with gatekeepers may also rule out a particular hospital for certain ‘fast track’ procedures such as percutaneous coronary intervention, stroke or hip fracture. A patient may also be rejected because they do not meet the inclusion criteria or because the service is currently unavailable. A fast track rejection may also mean that other appropriate options are geographically closer.
Making Sense of Information
Registered nurses piece together the information gathered in Phase 3 to specify the patient’s current needs. If necessary, they make contact with a physician to seek advice on the appropriate course of action or assistance in interpreting the available information such as ECG results or whether the patient can remain at home in their current condition. Advice may also be sought about the appropriate level of care or to confirm CR. RN1: [Calls the physician at the emergency department] Hi, [name] at ambulance 9350. I would like to discuss a patient with you. [RN1 reports the patient’s previous medical history, current issues and the results of physical examinations.] You can assess the ECG yourself on the computer. Our suggestion is that this patient would do better at home, as she has home care on a regular basis throughout the day, and they can keep track of any deterioration. – Observation 18
To ensure safe and manageable extrication, RNs must sometimes combine human resources at the scene with creative use of available aids (e.g. folding stretcher, stair chair and ambulance stretcher). In some cases, RNs use their own bodies to move patients, carrying them manually for short distances; clearly, the easiest scenario involves a patient who can walk to the ambulance.
Challenges and Uncertainties
Selection of a receiving hospital is sometimes more a matter of accessibility than suitability. For example, a suitable or fast track hospital nearby may be closed during certain hours of the day or may belong to another organization, making it more difficult to convey the patient there. RNs also reported that the decision to convey a patient by ambulance is sometimes based on sympathy for someone who has been waiting a long time or resides some distance from the hospital.
Deciding when to depart is not always straightforward. RNs might know from the beginning that the patient would need to be conveyed to a hospital for definitive care, but circumstances at the scene might create challenges for departure. For example, in a case of a cardiac arrest patient who needs cardiopulmonary resuscitation (CPR) during transport, the RN must decide whether to call for assistance and wait for a second ambulance to arrive at the scene. Alternatively, they could choose to depart for the hospital and try to arrange a meeting along the way, but the secondary ambulance would then have to be dispatched from the right direction. The RN must then decide whether to provide optimal CPR at the scene or expedite transport and risk sub-optimal CPR. The CPR process and treatment guidelines are very well-structured in terms of CPR start/end, compression rates, defibrillation and pharmaceuticals up to the point of patient transport but offer little or no guidance for the decision to depart, which is up to the RN.
Decisions Made
Key decisions include the need for further treatment in a general or specialist hospital; potential for fast tracking; appropriate level of care; extrication route to get the patient to the ambulance. RNs must also decide what must be done at the scene, what can be done during transport and what can or should only be done at the hospital.
Synthesis Phase 4
In general, this phase centres on the planning and execution of logistics. To plan for further care and conveyance to a hospital, RNs must combine their findings from the previous phases. If there is a need for hospital care, they must find a way of extricating the patient to the ambulance that works for both the patient and the RN. While the participating RNs seemed to appreciate the option of consulting an emergency room physician when making treatment and conveyance decisions, that option is not always utilized, and geographic location and potential ‘fast tracks’ influence the choice of receiving hospital. In this phase, RNs seek to verify their goals and perhaps revise the course of action in light of interactions with physicians or gatekeepers.
Phase 5: En Route Assessment and Treatment
[During the drive to the hospital, RN1 sits in the back of the ambulance with the patient on his left-hand side. The only sounds are the wheels on the road and an occasional beep from the monitor, and the patient seems to be relaxing a little, perhaps as an effect of the administered analgesics. The RN checks the monitor for vital signs and notes them on a sheet of paper. He also looks at some of the documents provided by the physician at the local health care centre, but no further notes seems to be added. Shortly before arriving at the ED, the RN speaks gently to the patient about their imminent arrival and indicates that he will be removing the equipment for measuring vital signs.] – RN1: Do you have any questions about what will happen now?
Narrative/Goal
This phase includes events from commencement of patient transport to arrival at the receiving hospital. The goals are to finalize patient assessment and treatment in order to provide a summary and to prepare the patient for handover and ongoing CR and care at the receiving unit.
Information Cues
During transport, the RN monitors and addresses any changes in the patient’s condition and evaluates the effect of any treatment by engaging in verbal communication, visual observation and measurement of vital signs.
RN1: I can see that your heartbeat is nice and even, and oxygen saturation also looks good given the amount you received; we could even try to lower it a bit. How are you finding the pain? You estimated a 5 [out of 10] before?
Patient: Perhaps a 4 now, then.
RN1: A 4—so, a bit lower. Do you feel that the pain is radiating somewhere or has relocated in other ways? I will also administer a little more morphine. – Observation 24
Additional Information Extraction (Specific Questions/Probes)
While the RN may sometimes seek to extend their understanding of the patient’s narrative, conversation often remains casual, depending on the patient’s condition.
Making Sense of Information
In this phase, RNs compile the information they have gathered and enter this on the report sheet. The report sheet is seen as a guideline that provides a common language for interactions between RNs and the various healthcare facilities they engage with. It is mandatory for RNs to specify a field diagnosis or chief complaint (numbered 1 to 53) and a prioritization level (green, yellow, orange or red), along with vital signs, drugs administered and a short description of the problem. IP1: I believe that the triage system we have today provides a structure for all patients. There is at least a common ground; you are not free to do entirely as you wish. You must report the physiological aspects [vital signs], but the assessment itself can be more difficult to capture and describe on the report sheet. It plays an important part in providing the whole picture. – Group interview
The ongoing patient assessment may affect subsequent decisions about additional, renewed or withheld pharmaceutical treatment, as well as examinations and measurement of vital signs. Guidelines and fast tracking are revised if there are any missing data or tasks that were not completed during previous phases.
The RN who is driving the ambulance must find the fastest or most appropriate route to the receiving care unit, either by following GPS instructions or by selecting a route based on their own geographic and experiential knowledge of the area. Unforeseen obstacles and events such as fallen trees or traffic jams may force the RN to look for an alternative route.
Challenges and Uncertainties
The report sheet should be completed for every patient encounter, but RNs do not always comply with this requirement. In some instances, there may be insufficient time to do so because the RN must prioritize care and treatment. However, it seems that RNs may also fail to provide this information if the assignment is seen as ‘mere transport’ or when leaving the scene without making a patient assessment. To avoid problems at handover, items related to fast tracks or the triage tool are checked to ensure that all criteria and information boxes are completed. This includes some ‘standardized questions’ about contagious diseases, allergies and the need for confidentiality (if the patient’s identity is protected).
As mentioned earlier, RNs found the guidelines somewhat restrictive and inflexible; for instance, only one field diagnosis can be noted, and any additional information must fit into four rows on an A4 sheet. In reality, a patient may have more than one problem of equal importance, and further investigation may be warranted. RN1: Well, I usually reason like this. It’s like the ‘chicken and the egg’; what came first—the syncope or the abdominal pain? I also want to identify the issue that warrants the highest level of priority because the patient should receive the best and most efficient care possible. High priority means direct treatment and care. – Observation 7
The triage guidelines are relatively straightforward and specify what warrants a full triage. However, these guidelines do not indicate how to choose between two options of equal priority, and it is left to the RN to decide or to seek further discussion on arriving at the ED.
Other issues arise in relation to guidelines stating that certain examinations or tasks should be performed for a particular complaint. Although RNs may not believe this to be applicable to every patient, they complete the task and note it down to protect themselves rather than for the patient’s benefit. RN1: For me, this [using a flashlight to assess the patient’s pupillary response] is something I often do only for documentation purposes. It is highly unlikely that a fully conscious, speaking and neurologically intact patient would have a fixed and dilated pupil. If the patient had had a brain haemorrhage, he would have physical symptoms of some sort long before the oculus nerve was squeezed enough to present that sign. – Observation 16
In some cases, the patient may be unwilling to speak at all to the RN, which may indicate a failure to establish a relationship. This also complicates efforts to capture the patient narrative.
RNs reported that they sometimes have to modify their usual approach to ensure that the patient will be admitted without undue difficulty if the receiving care unit is outside their own organization. For example, they might be redirected to another hospital if a patient assessed by emergency department physicians ‘belongs’ to another catchment area. Similarly, it may be necessary to persuade a physician examining the patient for a stroke that another hospital may be more suitable, regardless of the ‘correct’ option specified by the guidelines. RN2: Sometimes I may offer a suggestion to a physician about which hospital the patient should be transferred to if the current one is full. They usually want us to transfer to a hospital about 70 km away when in fact there is one about 20 km away that’s on our way back to the station. This is better for the patient and for us because it reduces transport time and makes us available sooner for other missions. – Observation 7
During the mission, cell phones seem to be used for both personal and work-related purposes, which include accessing online resources to find out about specific pharmaceuticals and resolving staffing matters that arise during the shift. This latter issue arises for RNs with extended responsibility for administrative tasks; having to resolve such matters during a patient encounter seems to impact on CR and teamwork. OBS: I noticed that your cell phone rang several times today, and you [RN1] had to answer during the patient encounter. Is this a distraction? I mean, you disappear for a while from the situation.
RN2: It doesn’t really matter…
RN1: Well I think I does; it’s a bit stressful. If someone calls in sick, you have to resolve this before the shift ends—otherwise, you or one of your colleagues might have to work overtime.
OBS: Do you always have to answer the phone?
RN1: Well, it depends of course on what kind of patient you’re attending. If it is calm, you could ask the patient whether it would be all right to answer, but if it is a high priority patient, you do not answer. – Observation 4
Decisions Made
Is there a need for any specific resources or preparations at the receiving unit? Is there a need to call ahead to give a ‘heads-up’? Does the patient need any further treatment during transport, or can ongoing treatment be reduced or cancelled?
Synthesis Phase 5
During this phase (if the situation allows), RNs can supplement information gathering for CR purposes by deepening their knowledge and understanding of the patient’s experience and by evaluating the treatment provided and any changes in the patient’s condition. As there are only limited opportunities for documenting CR and findings in any detail during the mission, there is a risk that vital information may be lost. While this phase is generally perceived as one of the calmest during the EMS mission, this obviously depends on the patient’s current status.
Phase 6: Handover
[The ambulance pulls up in the ED garage, and the RNs offload the patient and head for the trauma room. On entering the room, five personnel are waiting for them, all wearing protective gear.] – RN1: Who wants the report? – HCW: We all do, but you can talk to me. – RN1: Well then, we have assessed Lisa here, who has been complaining of chest pain for the last two days. [RN1 continues to deliver the report; when she is finished, she asks if there are any further questions] – RN1: Well Lisa, these people here will take good care of you now. Get well soon! [RN1 walks to the ambulance bay and sits down at the computer to write the digital patient journal. She does not get far before there is another call on the radio.]
Narrative/Goal
This phase includes events from the moment of arrival at the receiving unit to writing the digital patient journal before the vehicle is restocked and readied for another mission. Goals include ensuring safe patient handover to the receiving unit and continuation of care, producing a digital patient journal and preparing for the next mission.
Information Cues
The triage nurse in the receiving hospital’s emergency department indicates the patient’s designated room, corridor and team.
Additional Information Extraction (Specific Questions/Probes)
There is frequent discussion about where the patient should initially be placed to ensure the most efficient care, especially when there are several possible field diagnoses. RN2: Well, I was flipping back and forth through the triage guidelines, but I think … whether it’s right or wrong, I want to find the number that assigns the highest priority to the symptoms we observed in the patient. In this case, as far as I can see, he’s at the same priority level for both knee and thorax. So I have to wait and discuss this further with the triage RN at the emergency department because it's their duty to support me in these decisions. – Observation 14
Making Sense of Information
According to the participating RNs, they share information that is most likely to enhance the care process. They also like to share important information gathered from the patient’s environment.
In principle, RNs try to improve future CR by revisiting their patient journals, following up on what happens to the patient after handover and reflecting on patient encounters with their colleagues or other healthcare clinicians. While these reflections supposedly help to clarify whether their actions and reasoning were correct, they do not always lead to any definite conclusion; instead, RNs realize there may have been no definitive right or wrong decision.
Challenges and Uncertainties
Ideally, RNs prefer to report to the physician or nurse in charge of patient care. However, it can be difficult to locate these individuals, as everyone looks the same when wearing protective gear with no distinguishing markings. RNs often try to make eye contact with the person they report to in order to check whether they are actually listening and understand the information. Some RNs report aloud for everyone to hear. RN2: It is really hard to just speak right out into the air, I think. I really want to give the report to the leader of the team—it just feels more natural. Then, with the physician, I really want to see that he listens to me when I speak because we don’t have the same connection that we have with the nurses. In my experience, I often get a lot of follow-up questions from physicians about information that I have already reported. – Observation 1
In general, RNs are aware that the atmosphere in the receiving care unit affects information sharing, and it was considered easier to share information with healthcare staff who are known to you or who are open and welcoming rather than being stressed, tired or uneasy.
The handover process is to some extent made more difficult by the inflexibility of the guidelines, as these items require further discussion. For example, the RN might be asked about their field diagnosis and priority, which may lead to further questions; if the RN, the patient or bystanders are unable to answer, it is up to the receiving care unit to find out. RNs also noted that they often want to share information about the patient’s home environment, but it can be difficult to find the right time and place for this. IP3: Well, the only opportunity to provide information about the patient’s home situation is in the digital patient journal. Even then, there is no specific place or heading for this—so how, when and where should we pass this information on, which may be of use in planning the patient’s future care and discharge planning? – Group interview
The digital patient journal is supposed to provide a detailed description of the patient encounter. However, these journals generally provide only a very brief description of why the patient is seeking emergency care. Only a few of the observed journal entries described the RN’s CR in terms of their findings or how they arrived at these conclusions. According to the RNs, journals for non-conveyed patients tend to be more thorough, but this was not reflected in the observed journals. In a few cases, the journal was completely empty because the RN regarded the mission as ‘mere transport’, or there was no patient examination or interview. Writing a digital patient journal is apparently considered less important than other issues like getting back to the EMS station in time for a shift change or to eat. Other barriers included the unavailability of computers in the ambulance bay at the receiving hospital or assignment to a new mission. RNs said that while they aspired to complete all patient journals during their current shift, these often remain unwritten until their next shift.
RNs noted that reflection with colleagues played an important part in improving CR. These mutual reflections typically occur during spare time rather than at work and commonly relate to shift changes.
Decisions Made
Key decisions include ensuring continuation of patient care and providing an understanding of the home environment by sharing the relevant information; deciding whether to write up the digital patient journal immediately, get something to eat or end the shift on time; and deciding whether to refill ambulance supplies.
Synthesis Phase 6
This phase is often experienced as somewhat stressful. After handing over the patient, RNs get ready for their next assignment but do not know how long they will have before this happens. RNs appear to want the best possible care for their patients, and they try to ensure this by prioritizing information that seems important for future care. However, this depends on CR that delivers a correct field diagnosis and appropriate decisions along the way. The receiving care unit serves a supplementary control function in this regard by asking questions that may have been overlooked during the patient encounter. These supplementary questions seem more important to care providers inside the hospital than to RNs. The patient journal is probably the one place where RNs can describe their CR during the patient encounter in terms of their findings, discussions with the patient or bystanders and descriptions of the patient’s environment or the accident scene. This raises the question of why patient journals are so sparse and whether they might contain more information if RNs could write them up during rather than after the patient encounter. The participating RNs expressed their willingness to improve their CR, preferably through reflection with others, as well as by attending education programmes within their organization.
Discussion
The account of CR that emerges from our results suggests that the process is iterative and characterized by fluctuating goals. Based on the organizational guidelines provided, we can assume that RNs working in EMS establish their main goals at the beginning of each patient encounter. First, they must decide on a suitable level of care, which depends in the first place on whether the patient is suffering from a life-threatening condition. Secondly, they must decide whether the patient is in need of hospital care (perhaps of a specialized kind) or whether they can be referred to a local healthcare centre or even remain at home.
Each of these major decisions entails a number of sub-decisions, and any or all of these may change during the course of the mission and patient encounter as information is added or altered. This underscores the complexity and characteristic interdependence and overlap of the elements of CR as a metacognitive process in this context (Patterson & Hoffman, 2012). As the information provided (or discovered) becomes fragmented during the mission, the CR process is necessarily iterative. This in turn makes demands on RNs’ ability to value and incorporate new information and to adjust their goals accordingly. This idea of paramedics’ decision-making as an iterative process is also discussed by Reay et al. (2018).
The EMS Mission as a Series of Tasks
Drawing on Hammond’s (1988) cognitive continuum theory (CCT), it can be argued that an EMS mission consists of a number of tasks that fluctuate in scale and structure. A task’s properties reflect its complexity – the number of cues and information combinations – ambiguity of task content, presentation of the task – including how the task is decomposed into smaller subtasks and visual or quantitative presentation – and the time available to perform the task. A well-structured task supports analysis into smaller segments to improve certainty of resolution. In contrast, an ill-structured task triggers intuition, and the solution is experience-based; this is a rapid process, with little or no possibility of decomposing the task. In our results, reasoning about CPR (well-structured) and transport (ill-structured) is one example of such tasks. According to CCT, the individual moves along a continuum between analysis and intuition, depending on the task; this view is supported by Dual Process Theory (see, for example, Evans, 2008). During the EMS mission, RNs must manage both well- and ill-structured tasks in order to make decisions that are appropriate to the given situation. Previous research suggests that most of these tasks could be decomposed if presented individually. In clinical settings, however, the RN must address these tasks more or less simultaneously on the basis of fragmented information. It follows that CR must switch between different tasks and goals during the mission, and this iterative process forces RNs to move along the continuum. This process was illuminated by Cowan (2010), who showed that human working memory can only keep track of three to five cues (although this depends on the task and differs across individuals). It seems possible that previous experience of performing a certain task may help to prioritize cues or to retain additional cues in working memory. In the current study, this is exemplified in phases 1 and 5, describing how RNs only use their guidelines for specific issues rather than the guideline as a whole. This point towards an internalization of the guidelines based on RN experience.
Experience-Based CR
Whilborg et al. (2019) reported that more experienced EMS RNs made greater use of their CR experience and reflexivity during a written assignment about examining a patient. As well as reasoning more intuitively, they made greater use of the content provided than their less experienced colleagues. Evans (2010) suggested that intuition-based decision-making only works when the situation resembles previous experiences. The present results indicate that RNs’ patient assessments are largely intuitive or subjective; as there are no visual or audible cues to support a structured assessment, they must depend on open-ended questions to determine how they can assist the patient. This may reflect the participating RNs’ lengthy experience, which perhaps enables them to assess the patient’s condition on the basis of observation alone.
However, lengthy experience does not always compensate for cognitive dispositions such as anchoring. This occurs when the RN relies too heavily on the initial information only to discover that their mental simulation does not align with the reality of the patient encounter. The likely effect of this biased reasoning is to prolong the time needed to identify the real issue, leading to errors in treatment and care that may have serious consequences for the patient (Croskerry, 2002). In addition, the guidelines require RNs to conduct a structured A-E assessment, along with a SOPQRST anamnesis (symptoms and signs, onset, provocation, quality, radiation, severity and time).
While the relevant literature focuses on structured patient assessment (using e.g. A-B-C-D-E, SOPQRST AMPLE, MIST and other tools) (National Association of Emergency Medical Technicians, 2017), it seems possible that the experienced RN can make goal-related decisions based on open-ended questions. For example, Forsgärde et al. (2021) reported that the RN’s dialogue with the patient, bystanders and other healthcare providers can become a living decision support tool. By bridging information gaps in CR, this dialogue can reduce uncertainty about perceived and actual patient needs in support of shared decision-making. This account largely corroborates the present findings and Wireklint Sundström and Dahlberg’s (2012) view that the patient narrative leads care provision.
Klein (1999) described a similar iterative process among fire commanders who, like EMS RNs, must strive to achieve a number of fluctuating goals. According to Klein, fire commanders see themselves as weighing different alternatives rather than making real decisions; as they describe it, the ‘choice’ evolves naturally as the only appropriate option at that moment. This seems to echo the experienced RN’s pursuit of a number of broad goals by selecting the most appropriate available alternative in the moment. Rather than reasoning about different solutions, this process sometimes seems to depend on an intuitive sense of what ‘fits’ the immediate situation.
We contend that the RN’s desire to fulfil the patient’s wishes contributes significantly to their decision-making. While this can be understood as a caring perspective, it may also involve an element of social desirability bias. In making apparently intuitive decisions, RNs seemed aware that the situation may not always turn out as planned, and this is also based on experience. However, it is also possible that RNs are not fully aware of their reasoning and are influenced both privately and professionally by external factors. Intuitive reasoning and decision-making are frequently characterized in the literature either as a flawed process involving more or less predictable biases or as effective in less predictable contexts (Patterson & Eggleston, 2017).
Emergency Medical Services CR Involves More Than Medical and Caring Decisions
Previous studies have suggested that RNs and other EMS clinicians make only medical and caring decisions. This view probably reflects the prevailing research agenda, but the present findings indicate that RNs’ reasoning and decision-making is broader in scope. To improve our understanding of RNs’ CR process in EMS settings, then, it seems important to look at the mission as a whole rather than focussing on specific tasks. For example, Harenčárová (2017) investigated how paramedics manage decision-making uncertainty in relation to three major mission phases (En route to incident, Incident handling and Transportation). Their study was retrospective, which may have affected participants’ recollection and presentation of their actions and what actually happened. Nevertheless, the results are of interest because they anticipate our findings here. For instance, the participating RNs used forestalling and reduction, gathering further information about the patient and their surroundings until an appropriate decision could be made. In the present study, we found that RNs depend on colleagues and their combined experience to arrive at reasonable decisions in a given situation.
Another crucial issue is the transfer of the RN’s reasoning and essential information to the receiving unit as part of the process of patient handover. The current study identifies several issues that EMS RNs perceived as impacting this process, including ED atmosphere, interpersonal relations between the EMS RN and receiving personnel and difficulties to identify the specific roles of healthcare personnel at the receiving unit. Loss of information during patient handover is a major concern for patient safety, and previous research has noted similar problems reported by EMS personnel and receivers alike (Carter et al., 2009; Zakrison et al., 2016). To overcome this difficulty, structured communication and ‘speaking the same language’ is vital for the effective transfer of information (Bost et al., 2009; Bruce & Suserud, 2005; Dúason et al., 2021). Like the RNs in the present study, ED personnel also seem to have concerns about patients with multiple complaints or non-distinct medical problems (Bruce & Suserud, 2005). In addition, there seems to be a lack of clarity about the point at which the transfer of responsibility for the patient actually occurs (Bost et al., 2009; Dúason et al., 2021). While these issues are widely acknowledged, the fact that challenges persist suggests a need for further research.
RNs suggested that education should be prioritized to enhance CR, along with time to reflect with colleagues. While expressing their appreciation of the organization’s educational interventions, RNs noted that these are too infrequent and that more are needed. Building on the present findings, future research should seek to clarify where decision support tools are needed and how EMS organizations can provide better support for RNs. Finally, to improve CR and so enhance patient safety, researchers must address the EMS mission as a whole.
Strengths and Limitations
The present study was conducted in a socially and organizationally bounded Swedish EMS system, and this is likely to affect the generalizability and transferability of the findings. According to Yin (2014), one limitation of the case study approach is that there are no general step-by-step guidelines for data collection, analysis or presentation of results, which adds to the burden of maintaining rigour, transparency and validity. In the present case, we sought to ensure that a rigorous audit trail detailed the various data sources and how the results were grounded in the data (Appendix B). Another limitation is that the first author had sole responsibility for the process of data collection and the summary of the analysis. While this might impact the results, we addressed the issue by ensuring that all of the authors could access the transcribed files in ATLAS.ti and could comment if they saw a need for a shift of focus in data collection. In addition, the data and associated analysis were discussed by the authors at frequent research meetings to ensure consensus.
While convenience sampling ensured that participants were representative of the research setting, the participants’ specialist education and relatively lengthy experience of EMS care mean that the results might differ for less experienced participants (Shin, 2019; Whilborg et al., 2019). Additionally, although the participating RNs did not report any such effect, they were likely to be influenced by the presence of an observer (Angrosino, 2007); equally, the lengthy shift-based observations may have affected researchers’ ability to remain attentive throughout. Observers may also have found it difficult to remain in the researcher role, raising ethical and moral issues in their role as a professional RN; for example, the first author (UA) abandoned the role of researcher on one occasion to assist with a cardiac arrest. Finally, as the study was conducted in a Swedish EMS organization, all of the original data were in Swedish, and some subtle notions may have been lost in translation. To address this issue, the authors reviewed the translation of specific quotes several times to ensure that the wording was appropriate.
Among the study’s strengths, all patient encounters fell within the normal scope of EMS missions. Some of the factors that can influence CR did not feature in the case encounters, including violence (or the threat of violence) and RN–patient language barriers, which frequently arise during EMS missions. Nevertheless, we are confident that the study accurately reflects the everyday work of RNs in Sweden’s EMS. Another strength of the study is the range of data sources used to capture different aspects of the CR process. Additionally, the authors’ diverse research and educational backgrounds brought different perspectives and experiences to the analysis and interpretation of the data. At every point in the process, the authors made a concerted effort to avoid introducing their own preconceptions and to focus on the data to hand.
With regard to methodology, the research design is considered appropriate to the aims of the study. However, we did not foresee the high operational demands on ambulances during the study period. This limited the scope for in-depth follow-up interviews to allow RNs to clarify and verbalize any reasoning that may not have been detectable during the observations. This undoubted loss of detail could be resolved in future studies by a more hermeneutical approach, drawing to a greater extent on the authors’ own experiences and previous research to interpret the data. Other methods of data collection and analysis may also prove useful. For example, in a recent Dutch study, Dercksen et al. (2021) used video recording glasses to capture the EMS mission from the clinician’s perspective. In combination with follow-up interviews in an off-duty setting, tools of this kind would facilitate in-depth probing of the reasoning process. Video recording would enable repeated analysis of each mission to identify specific points of interest as the basis for further questions about the RN’s reasoning process. Video playback might also help the RN to remember the specifics of the case reducing the risk of faulty recollection or a more socially acceptable account.
Conclusions
In EMS settings, RNs’ CR is a complex process that can be difficult to comprehend or describe. In capturing the fragmented accumulation of information throughout the EMS mission and especially during the patient encounter, the present findings confirm the need for a fuller understanding of the CR process. Throughout their missions, the participating RNs had to sustain alternative decision-making processes, adjusting to new or amended incoming or previous information and reconstructing the work plan accordingly. The patient narrative was identified as the primary source of information, and RNs try as far as possible to fulfil the patient’s wishes in terms of care and treatment. During these missions, an RN’s CR can be influenced by multiple factors, including their own attitudes and those of team members. Further research is needed to clarify the CR process and how this influences clinical practice during an EMS mission.
Implications
The RN’s CR extends beyond the patient encounter, and all of these elements must be accounted for in developing decision support tools, developing the EMS organization and working practices and pursuing future research.
Decision Support (as Separate Tool or Functionality in an Existing System)
• Provide a cognitive bias checklist for RNs. • Provide suggestions regarding diagnosis, additional assessments or examinations, potential treatment and dosages. • Enable real time information sharing within the team (and to other units) to support a joint understanding during the mission.
Emergency Medical Services Organization
• Enhance the validity and credibility of dispatch information. • Provide accessible digital guidelines (e.g. a decision support tool) with automatic update capabilities. • Provide RNs with access to patient health records. • Provide RNs with opportunities to write up the digital patient journal during the mission rather than afterwards. • Create opportunities for RNs to participate in scheduled reflection to discuss patient encounters and associated issues as a means of developing CR competence.
Future Research
• Investigate the impact of RN access to patient health records during the mission. • Investigation of EMS cognitive work processes using methods such as talk-aloud protocols, critical incident studies and SAGAT protocol. • Investigate the impact of a decision support tool for CR process in the EMS. • Investigate patient handover processes from EMS to hospitals from a CR perspective.
Footnotes
Acknowledgements
The authors would like to express their gratitude to the study participants for their valued contribution. It has been a privilege to be allowed to follow and participate in your everyday work and to share your experiences.
Authors’ contributions
UA, HA and BWS collected the data, with UA as lead. UA performed the initial data processing, including transcription and sorting of data into the relevant phases. All authors participated in the analysis through active discussion and close reading of the data. All authors participated in the manuscript’s production, and all contributed actively to the revisions. UA was the main contributor to the write-up. All authors have read and approved the final manuscript.
Details of patient encounters
Chief complaints (n = 34)
Age (n = 35) (mean = years)
Environment (n = 34)
Abdominal pain (5)
Total (range = 5–97, mean = 63)
Community healthcare centre (3)
Back pain (1)
0–20 (6) (mean = 16)
Hospital (1)
Cardiac arrest (1)
20–40 (0)
Nursing home (6)
Chest pain (7)
40–60 (5) (mean = 50,2)
Patient’s home (16)
Deteriorating health (2)
60–80 (11) (mean = 70,3)
Public, indoor (3)
Deviating blood values (1)
80+ (13) (mean = 88,2)
Public, outdoor (5)
Head trauma (2)
Hip fracture (2)
Infection (2)
Seizures (1)
Stroke (4)
Traffic accident (2)
Urinary problems (2)
Vertigo (1)
Data audit trail: Triangulation and presentation of results
‘X1’ = drive out recording; ‘X2’ = field notes; ‘X3’ = follow-up interview; ‘X4’ = patient journal audit; ‘GI’ = group interview.
Phase
Data source (OBS Xx)
Phase 1
12,3, 22, 32,3, 42,3, 52,3, 62,3, 72,3, 82,3, 92,3, 102, 131,2,3, 141,2, 151,2,3, 161,3, 171,2, 181,2,3, 191,2,3, 201,2, 211,2, 221, 231,3, 242,3, 252, 261,2, 271, 291,2, 302, 311,2, GI
Phase 2
12,3, 22, 32, 42, 52,3, 62, 72,3, 82,3, 92,3, 102, 113, 122, 132,3, 152, 161,2,3, 171,2, 181,2,3, 191,2,3, 202, 212, 221,2, 232, 242,3, 252, 272, 282, 292, 302, 311,2, 322, 332, 342, GI
Phase 3
12,3, 22,3, 31,2,3, 42,3, 52,3, 62, 72,3, 82,3, 92,3, 102,3, 112,3, 122, 132,3, 142,3, 152,3,4, 162,3,4, 172, 182,3, 192,3, 202,3, 222,3, 233, 242,3, 252, 262, 272, 282,3, 292, 312, 322, 332, 342, GI
Phase 4
12,3, 22, 52,3, 72, 83, 92,3, 103, 112,3, 122, 132, 142, 152,3, 162,3, 172, 182,3, 193, 222, 242, 252, 262, 272, 282, 292, 302, 312, 322, 332, 342 GI
Phase 5
12,3, 22, 32, 42, 54, 62,3, 72,3, 82,3, 102, 132, 142,3, 152, 162,3,4, 192,3, 202,3, 214, 222,4, 232, 242, 252, 262, 272, 282,3,4, 292, 312, 322, 332, 342, GI
Phase 6
12,3, 22,4, 32, 43, 52,3, 62,3, 72,3,4, 83, 94, 102, 132, 142,3,4, 152, 162,3, 174, 184, 192, 222,4, 232,3,4, 242, 262, 272, 282,4, 292, 302, 322, 332, 342, GI
Ulf Andersson, a PhD student within the human perspectives in care at the University of Borås. The thesis focus is on clinical reasoning within emergency medical services. Furthermore, a registered nurse with a specialist education towards prehospital and ambulance nursing. Member of the research group PreHospen – Centre for prehospital care.
Magnus Andersson Hagiwara, Professor within prehospital emergency care at the University of Borås. Main research focus towards patient safety, computerized decision support and emergency medical services. A registered nurse with a specialist education towards prehospital and ambulance nursing. Experience from emergency medical services. Member of the research group PreHospen – Centre for prehospital research.
Birgitta Wireklint Sundström, Professor in human perspective in care at University of Borås. Main research focus on early assessment and optimal care levels in prehospital care. Registered nurse with a specialist education towards anaesthesia. Member of the research group PreHospen – Centre for prehospital research.
Henrik Andersson, Associate professor at the University of Borås. Main research focus on patient assessment in emergency and prehospital care, simulation and gaming. Registered nurse with experience from emergency care. Member of the research group PreHospen – Centre for prehospital research.
Hanna Maurin Söderholm, PhD from Swedish school of Library and information science at the University of Borås. Senior Lecturer in the human perspectives in care at University of Borås. Main research focus on future technologies for collaboration and information sharing, primarily within a prehospital context. Member of the research group PreHospen – Centre for prehospital research.