
Abstract
Objective
To evaluate, under replicable, blinded and standardised conditions, the effect of acute exposure to hypobaric hypoxia (HH) (equivalent to 200 or 3000 or 5000 m above sea level (asl)) on selected cognitive domains and physiological parameters in personnel of helicopter emergency medical service (HEMS).
Methods
We conducted a randomized clinical trial using a single-blind crossover design in an environmental chamber (terraXcube) to induce HH in 48 HEMS personnel. Participants performed cognitive tests (CT) before the ascent, after 5 min at altitude, and after simulated cardiopulmonary resuscitation (SCR). CT evaluated: sustained attention using the psychomotor vigilance test (PVT) that included measurement of reaction time (RT); risky decision making using the balloon analogue risk task (BART), and attention and speed of processing using the digit symbol substitution test (DSST). CT performance was subjectively rated with a visual analogue scale (VAS). Physiological data were recorded with a physiological monitoring system. Data were analysed using a linear mixed model and correlation analysis.
Results
Mean reaction time was significantly slower (p = 0.002) at HH (5000 m asl), but there were no independent effects of HH on the other parameters of the PVT, BART or DSST. Participants did not detect subjectively the slower RT at altitude since VAS performance results showed a positive correlation with mean RT (p = 0.009). DSST results significantly improved (p = 0.001) after SCR.
Conclusion
Acute exposure of HEMS personnel to HH induced a slower RT but no changes in any other investigated measures of cognition. The reduced RT was not detected subjectively by the participants. Trial number 3489044136, ClinicalTrials.gov trial registration.
Keywords
INTRODUCTION
The partial pressure of oxygen in the inspired air decreases exponentially with altitude exposure due to a decrease in barometric pressure, resulting in hypobaric hypoxia (HH). The brain is particularly sensitive to hypoxia and is the first organ to be compromised when compensatory responses are insufficient (e.g., after acute HH exposure). The neurological effects of HH include symptoms like headache and dizziness and specific neurological altitude illnesses and can involve higher cortical functions and lead to cognitive disturbances (Falla et al., 2021; Wilson et al., 2009). In contrast to other neurological effects of HH, it can be challenging for affected individuals to promptly recognise cognitive impairments at altitude and are therefore particularly dangerous. Reduced cognitive abilities may cause accidents and have fatal consequences during high-risk working operations at HH (Cable, 2003). For many years, astronauts and aircraft pilots have been trained to promptly recognise HH exposure as an emergency event, yet notoriously difficult for them to detect because of its insidious nature.
Previous studies in astronauts (Basner et al., 2015), aircraft pilots (Asmaro et al., 2013; Bustamante-Sánchez et al., 2019; Legg et al., 2012) and military helicopter pilots (Bouak et al., 2018; Legg et al., 2016) have explored the influence of HH on multiple cognitive domains but the precise effects on cognition are still unclear (Jung et al., 2020; McMorris et al., 2017). Contradictory results have been reported in different studies (De Bels et al., 2019; Li et al., 2000; Loprinzi et al., 2019; McMorris et al., 2011; McMorris & Hale, 2012; Pavlicek et al., 2015; Taylor et al., 2016), especially at moderate altitude. Some studies have reported reduced psychomotor vigilance (i.e., slowing of reaction time, RT) after exposure to reduced oxygen availability (altitude between 4350 and 5260 m above sea level (asl)) (Davranche et al., 2016; Pun et al., 2018; Roach et al., 2014) while others reported no effects (altitude between 1630 to 3962 m asl) (De Bels et al., 2019; Heinrich et al., 2019; Latshang et al., 2013; Thomas et al., 2007). Other studies have reported the influence of hypobaric (Heinrich et al., 2019) and normobaric hypoxia (Pighin et al., 2014, 2020) on decision making investigated with different tasks (decision under risk and decision under ambiguity) while others reported no effects using a complex logical reasoning test (Legg et al., 2012) and a test that evaluated propensity to impulsivity (Thomas et al., 2007). Impairment of working memory was described in aircraft pilots after exposure to HH (10,000 m asl) during hypoxia awareness training (Asmaro et al., 2013; Malle et al., 2013), in military helicopter pilots (Bouak et al., 2018; Legg et al., 2016) and other study populations (Hu et al., 2016; Wang et al., 2013), while others reported no effects (Walsh et al., 2020).
Helicopter emergency medical service (HEMS) personnel are routinely exposed to rapid ascent to altitudes between 3000 and 5000 m asl without pressurized cabins in services operating in mountainous areas (EASA, 2018; Pietsch et al., 2018). Although cognitive abilities are of utmost importance for flight safety and the management of critically injured patients (e.g., performance of in-flight cardiopulmonary resuscitation), there have been no previous studied of the effects of HH exposure on cognition of HEMS personnel.
The aim of the current study was to evaluate under replicable, blinded and standardised conditions, the effect of acute exposure with a rapid ascent (4 m/s) to different levels of HH (equivalent to 200, 3000 and 5000 m asl) on selected cognitive domains and physiological parameters in HEMS personnel. We hypothesised that altitude would independently affect cognition, specifically in three tests investigating speed of processing, attention and risk-taking behaviour. Secondary aims were to explore the relation between the effects of HH on cognition and its subjective effects and the effect of physical effort in the form of simulated cardiopulmonary resuscitation (SCR).
METHODS
A randomized clinical trial (RCT) study using a single-blind crossover design was performed from the 25th October to the 11th of November 2019 in the terraXcube in Bolzano, Italy. The terraXcube is a research infrastructure that can simulate the most extreme climatic conditions under controlled, replicable and safe conditions (https://terraxcube.eurac.edu/) (Figure 1). The study was approved by the institutional review board of Bolzano (Protocol Number 0122265-BZ) and registered in ClinicalTrials.gov (Protocol Record 3489044136). The study was conducted according to the declaration of Helsinki and the CONSORT guidelines. Schematic representation (on the left) of the study setting in the terraXcube in Bolzano, Italy for each study arm (4 participants) inside of the hypobaric chamber (upper panel) and of the control room (lower panel). Pictures (on the right) refer to the experimental setup inside the hypobaric chamber (upper panel) and in the control room (lower panel).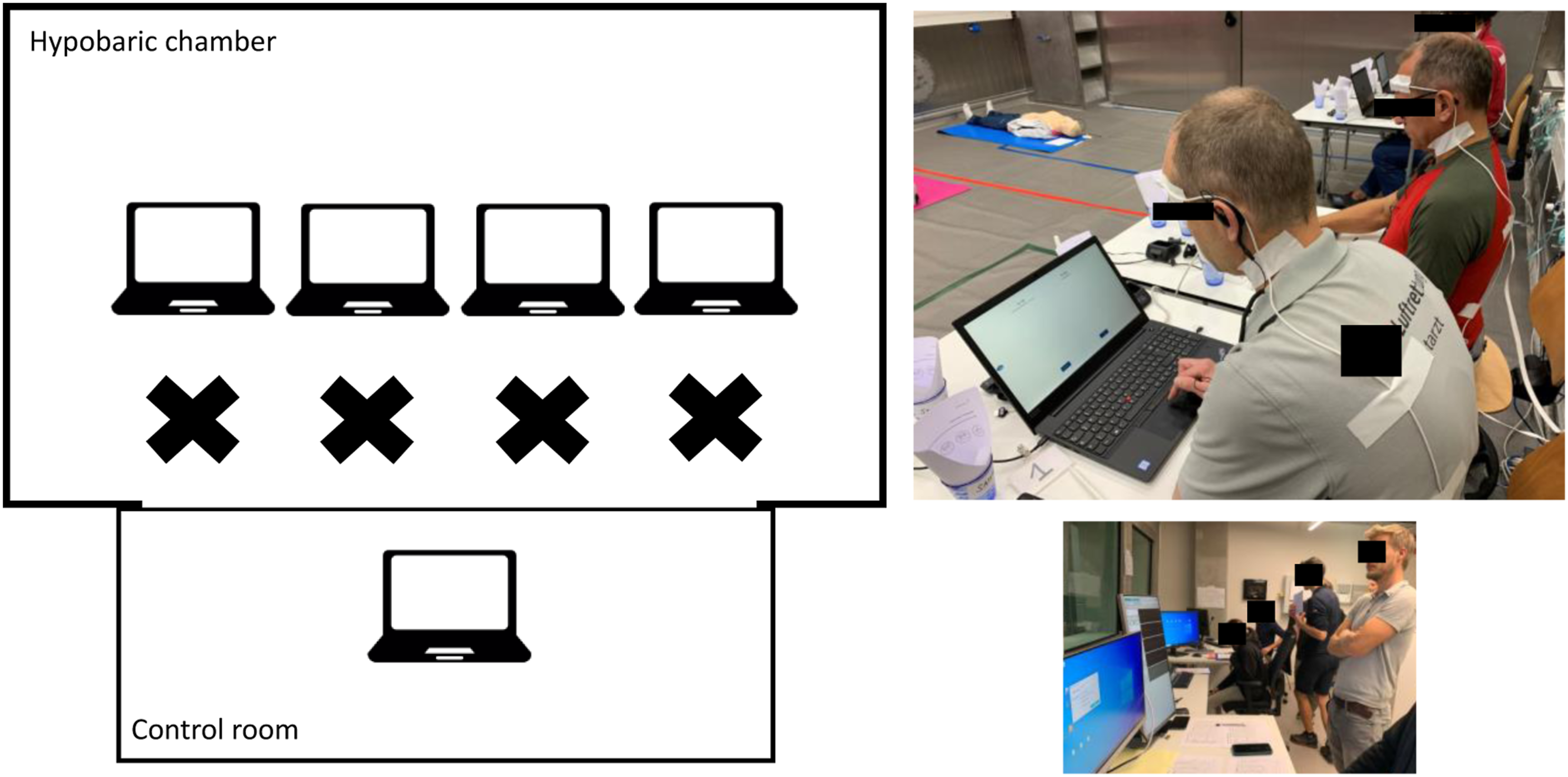
Study participants
Study participants were recruited from prehospital emergency service personnel (i.e., medical doctors, nurses, paramedics, rescue technicians and pilots) in Austria, Germany, Italy and Switzerland. Inclusion criteria were an age between 18 and 60 years, and an American Society of Anaesthesiologists (ASA) physical status class I (healthy patient). Participants between 40 to 60 years old, or below 40 years old with cardiovascular risk factors according to the European Society of Cardiology (ESC) guidelines (Perk et al., 2012), were screened with a cardiovascular stress test and excluded in presence of arrhythmias, increasing chest pain or marked ST-depressions during exercise. Exclusion criteria were age above 60 years, an ASA class II or more, a medical history of psychiatric disorders and neurological diseases, or previous high altitude pulmonary oedema (HAPE) or high altitude cerebral oedema (HACE) or severe acute mountain sickness (AMS) (defined as a Lake Louise Score (LLS) > 9) (Roach et al., 2018) which occurred at altitudes similar to the ones used in our study.
Study protocol
Each participant took part in two experimental sessions on two consecutive days (Figure 2). After a baseline test at 200 m asl (i.e., altitude of the terraXcube), the experimental sessions were performed at three different levels of HH (equivalent to 200 (control test) or 3000 or 5000 m asl). Participants and researchers were blinded towards the altitude profiles; only the principal investigator and the chamber technicians knew the simulated altitude. The temperature, humidity and carbon dioxide levels in the terraXcube were continuously monitored and kept constant at normal indoor values. Study design. Six study arms: 1 (day 1–200 m, day 2–3000 m); 2 (day 1–3000 m, day 2–200 m); 3 (day 1–200 m, day 2–5000 m); 4 (day 1–5000 m, day 2–200 m); 5 (day 1–3000 m, day 2–5000 m); 6 (day 1–5000 m, day 2–3000 m). CT: cognitive tests. SCR: simulated cardiopulmonary resuscitation.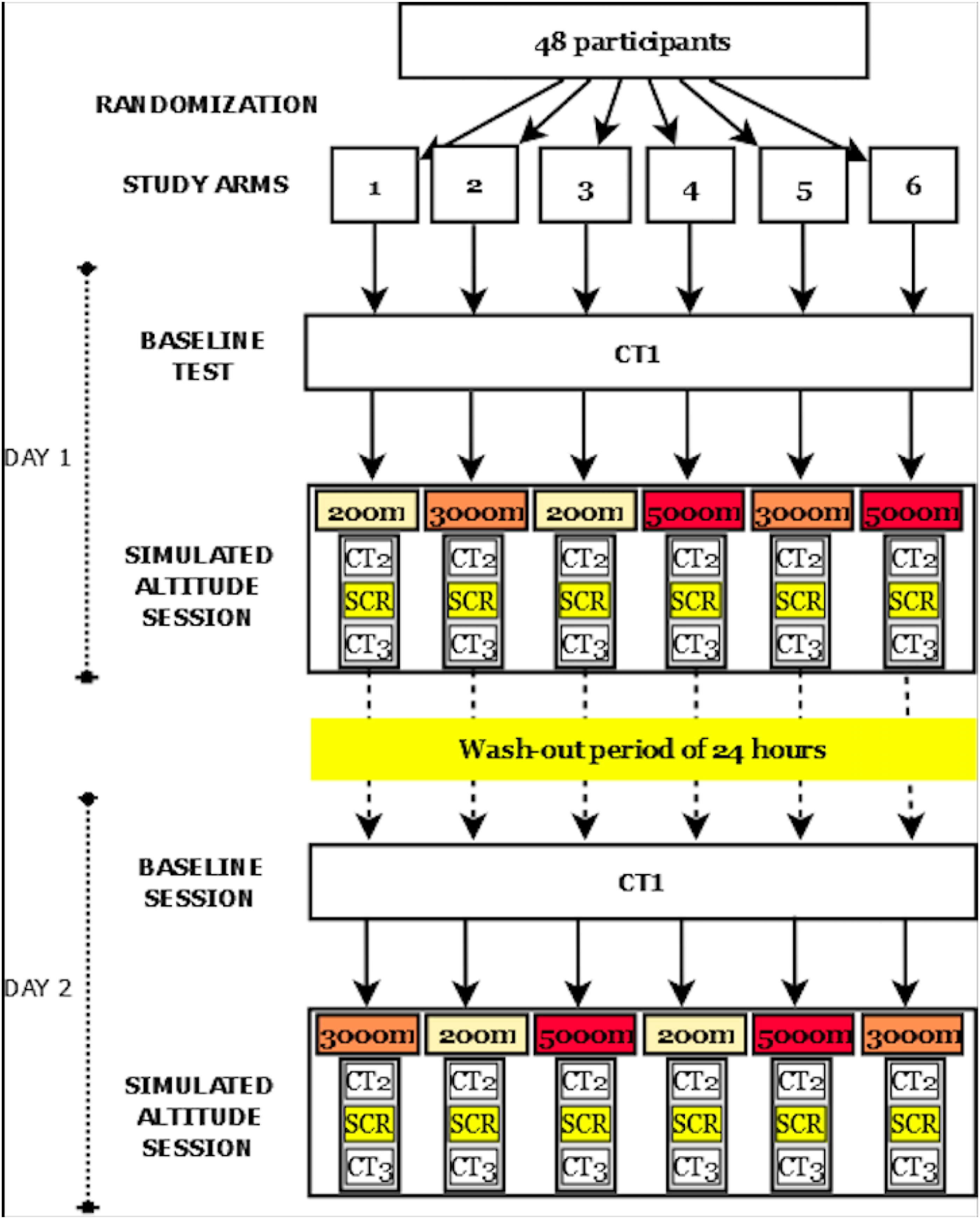
Participants were divided into 12 groups of four participants each. The crossover design of the study consisted of six study arms - one for each of the two combined altitude profiles – as shown in Figure 2. Each study arm was applied to eight participants (i.e., two groups of four). Ascent and descent times to the three different altitudes were standardized to 20 min to guarantee the blind design. The control ascent to 200 m asl consisted of an oscillating ascent-descent between 200 and ∼600 m asl for 20 min, with the purpose of evoking the typical pressure change on the eardrums during altitude changes. The ascent to 3000 m asl consisted of an oscillating ascent-descent between 200 and ∼600 m before going up to 3000 m asl. The ascent to 5000 m asl was a constant ascent for 20 min. The rate of ascent and descent in the chamber was 4 m/s, which corresponds to a realistic ascent speed for HEMS (IVAO, 2020).
On days 1 and 2 each group was exposed to two of the three simulated altitudes according to a randomly assigned altitudes’ profile. On each day the same schedule was followed, with cognitive tests (CT) performed at the same time of the day to prevent any circadian influence on arousal (Figure 2). Participants performed the CT three times on each of the 2 days: before the ascent (baseline - CT1), after 5 min from the end of the ascent (CT2) and after physical effort (i.e., 5 min of SCR that include only chest compression; CT3). After completing each CT session, participants were asked to rate their performance using a visual analogue scale (VAS) by placing a mark on a 100 mm-line, horizontally positioned with the extremes labelled “bad performance” (on the left end) and “good performance” (on the right end).
On a familiarisation day (day 0), a medical interview with a general medical examination was performed. This included a questionnaire about previous altitude exposure in accordance with the STrengthening Altitude Research (STAR) data reporting guidelines for clinical high altitude research (Brodmann et al., 2018). Participants received a technical introduction and safety briefing for the terraXcube, as well as a familiarisation session with the CT and the experimental protocol. In addition, on the familiarisation day, assessment of sleep quality, depression/anxiety and stress were also performed using three paper questionnaires. Belts for the physiological monitoring system (Equivital EQ02, Hidalgo, Cambridge, UK) were fitted and worn during the entire duration of the tests inside the chamber. The cerebral oxygen saturation (ScO2) sensor was worn during the first two sessions of the CT (CT1 and CT2) but was removed before SCR for operational reasons. AMS was assessed using the LLS (Roach et al., 2018) three times each day (before, during and after altitude exposure) after each CT session.
Before each experimental session, participants were asked to avoid coffee and tea consumption and/or smoking over the last 2 hours. Participants were questioned about the quality and quantity of the previous night sleep (using the Richards-Campbell Sleep Questionnaire), and whether they had to work a night shift the last three nights. The participants were not accompanied by staff during the tests in the chamber. To guarantee adherence to the experimental protocol, they were, however, continuously monitored and guided (via radio commands) from the control room by staff, without otherwise interfering with the experiment (Figure 1). A wash-out period of 24 hours rest between the testing on day 1 and the testing on day 2 aimed to prevent any carry-over effect of the altitude exposure.
Cognitive Tests and Paper Questionnaires
The stress perception was evaluated using the Perceived Stress Scale (PSS)-10 item (Cohen & Williamson, 1988) and anxiety and depression using the Hospital Anxiety and Depression Scale (HADS) (Zigmond & Snaith, 1983). Sleep quality was evaluated by the Pittsburgh Sleep Quality Index (PSQI) questionnaire that assesses sleep quality and quantity over a month-long period (Buysse et al., 1989).
Three different CT were employed to evaluate: sustained attention, using the Psychomotor Vigilance Test (PVT); risky decision making, using the Balloon Analogue Risk Task (BART); and attention and speed of processing using the Digit Symbol Substitution Test (DSST). Six different versions of the DSST were administered across the multiple timepoints (different session CT1, CT2 and CT3 on day 1 and 2) to avoid learning effect. The three tests were assigned following sequence randomization. All the tests were developed using PsychoPy (version 3.1.0, www.psychopy.org) and were modularly designed. The software for the three cognitive tests was installed on four Eurac Research-issued laptops, used by each group. Each participant performed the tests on the designated laptop in the terraXcube at a separate desk based on the study protocol timeline. To ensure that all laptops performed identically at various altitudes, a laptop benchmark software (NovaBench https://novabench.com/) was run several times on an altitude of 200, 3000 and 5000 m asl, during ascent and descent. In all test cases, the benchmark software produced the same score. Therefore, we concluded that a change in altitude had no significant effect on the performance of the laptops.
Psychomotor Vigilance Test
We used a brief 3-min version of the PVT similar to Basner et al. (2011, 2015). The PVT assesses sustained and vigilant attention and is based on simple RT to visual stimuli that occur at random intervals varying from 2 to 5 s in steps of 200 ms (Dinges & Powell, 1985). The PVT is suitable for administration several times without improvement over time because it is unaffected by learning (intra-subject variability) (Dinges et al., 1997). The following parameters were measured and analysed: reaction time (milliseconds (ms)) (excluding lapses and false starts), the number of omission errors or “lapses” (defined as reaction times ≥355 ms), false starts or errors of commission (defined as a response without a stimulus or a RT <100 ms), and performance score (defined as one minus the number of lapses and false starts divided by the number of valid stimuli, including false starts range 0–100%) (Basner et al., 2011).
Balloon Analogue Risk Task
The BART is a computer-simulated assessment of risk-taking behaviour under ambiguity (the probabilities of possible negative consequences are unknown) (Lejeuz et al., 2002). Participants performed an adjusted version of the BART. Participants had to inflate a series of virtual balloons pressing the enter button on a PC which increase the balloon’s size and will randomly explode. If a balloon popped, the value of that balloon is lost to the participant. The goal is to achieve a virtual monetary reward balancing the possible loss. Participants had to find the best strategy to gain a valuable reward while at the same time avoiding excessive risky decisions. Therefore, they have to weigh the relative risks and benefits of each consecutive pump. The following parameters were measured and analysed: mean earnings and mean pumps for only the balloons not popped (adjusted values).
Digit Symbol Substitution Test
The DSST assesses several cognitive domains including: attention, visual-motor speed and coordination. DSST is a computerized adaptation of a paradigm used in the Wechsler Adult Intelligence Scale (WAIS-IV) (Wechsler, 2008). Every subject refers to a fixed legend at the bottom of the screen relating each of the digits 1 to 9 to a specific nonsense symbol. One of the nine symbols appears randomly on the center of the screen and the participant must select the corresponding number as quickly as possible using the keyboard numbers in a row. The test duration is fixed at 90 s, and the legend key is randomly reassigned with each administration. Due to engagement of executive functions this test is subject to learning/practice effects over time (Beres & Baron, 1981). Therefore, due to the repeated administration of this test in our study, we used a randomized design coupled with the use of six parallel forms of the same test. The total mean number of correct and incorrect paired responses were calculated.
Physiological Measurements
A two-lead electrocardiogram (ECG), heart rate (HR), respiratory rate (RR) and peripheral oxygen saturation (SpO2) were recorded continuously in real-time using the Equivital system (EQ02, Hidalgo, UK). Regional ScO2 of the left frontal lobe area of the brain was measured by a near-infrared spectroscopy (NIRS) device (O3TM Regional Oximeter, Masimo Corporation, Irvine, CA, USA).
Statistical Analysis
As no previous data were available, and thus no sample size estimation could be performed, recommendations concerning sample size for pilot studies have been used instead (Julious, 2005). As there were six altitude combinations, a team had four members, and two repetitions were regarded as necessary, a total of 48 participants were enrolled in the study. Specifically, with a sample size of 48 participants per group (alpha = 5%, beta = 80%) an effect size of 0.41 could be detected. This is in line with a likely effect size of 0.49 from a meta-analysis (McMorris et al., 2017).
Data is given as mean with standard deviation, mean with 95% confidence interval or as frequencies, as appropriate. Data from the crossover trial were analysed with a linear mixed model (LMM) using the baseline value of the variable of interest as a covariate, day and session of testing as a repeated effect with an autoregressive covariance type and the fixed effects of age (<39.5 vs. ≥39.5 years), altitude, healthcare provider (HCP), gender, pre-acclimatisation, sleep hours, day of testing, session of testing and sequence of testing. Session of testing was defined as timepoints of the CT administration (CT1, CT2 and CT3). Sequence of testing was defined as the randomized order of the three CT (PVT, BART, DSST) at each session. Pre-acclimatisation was defined to be present, partially present, or clinically absent, considering the number of exposures above 3000 m asl and their duration in the 3 months before the study, as well as their proximity to the study dates. Single group comparisons were conducted using t-test or chi-square-test, as appropriate. Correlation analysis was done between SpO2, ScO2, VAS performance and cognitive tests. All p-values are two-sided, corrected for multiple variable comparisons using Li’s two-step rejection procedure (Li, 2007) and a value of 0.05 or less was considered statistically significant. Statistical analyses were conducted with the use of SPSS version 26 software (IBM Corp., Armonk, NY, USA).
RESULTS
Baseline characteristics of study participants
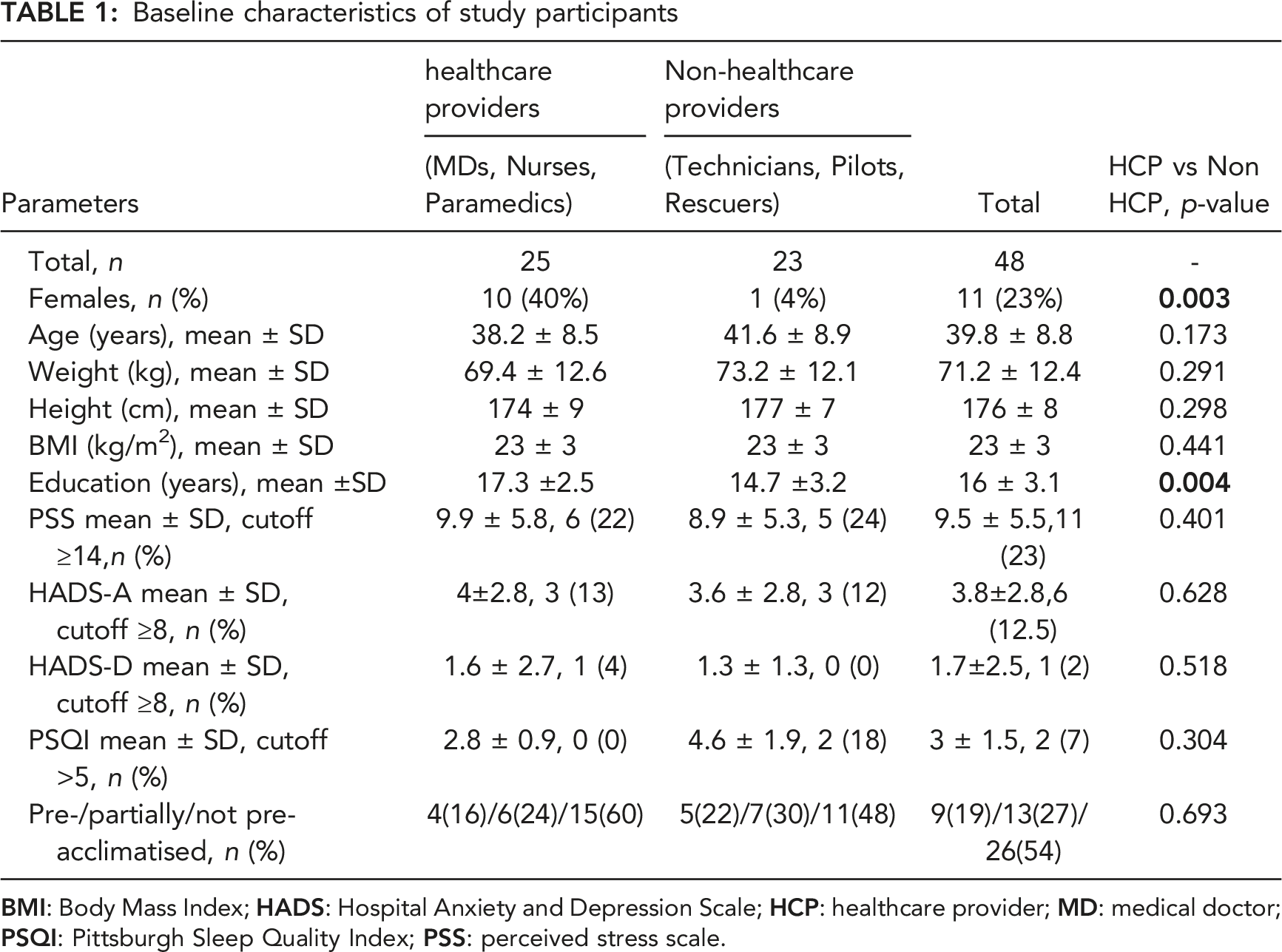
During the tests the barometric pressure was 973.6 ± 11.6, 705.2 ± 0.1, and 543.1 ± 0.1 mbar (p < 0.001), the temperature was 22.9 ± 0.2, 22.6 ± 0.4, and 22.7 ± 0.4°C (p = 0.237) and the relative humidity 45.5 ± 6.9, 36.1 ± 4.6, and 31.0 ± 2.8% (p < 0.001) at HH equivalent to 200, 3000, and 5000 m asl, respectively. Carbon dioxide was constantly kept below the 1100 ppm threshold. There were no dropouts or health issues. All tests (96) were included in the final data analysis.
Cognitive tests: Psychomotor Vigilance Test (PVT), Balloon Analogue Risk Task (BART), Digit Symbol Substitution Test (DSST)
Psychomotor Vigilance Test (PVT), Balloon Analogue Risk Task (BART) and Digit Substitution Symbol Test (DSST) Parameters Results at the Different Altitudes and Timepoints
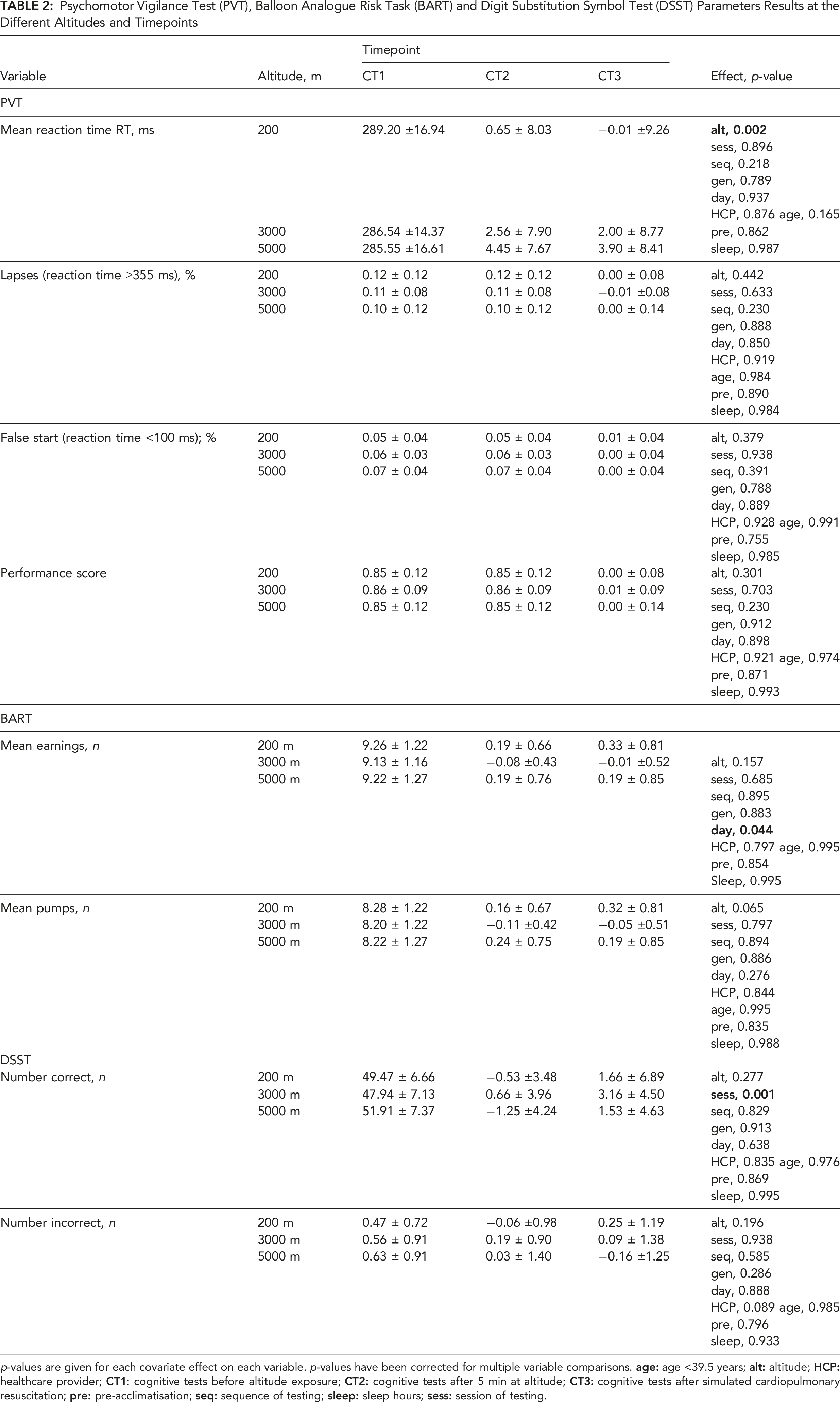
p-values are given for each covariate effect on each variable. p-values have been corrected for multiple variable comparisons.
The LMM analysis of BART results (Table 2) showed no independent effects of altitude on mean earnings and mean pumps. Of all the other factors analysed as covariates only day of testing (day 1 vs. day 2) showed a relationship with mean earnings (9.45 ± 1.45 vs. 9.192 ± 1.46; p = 0.044).
For the DSST the LMM analysis (Table 2) showed no independent effect of altitude on the number of correct and incorrect responses. Of all the other factors analysed as covariates there was an effect of session of testing showing an increased number of correct responses comparing pre- and post-physical effort sessions independent of altitude (see Table 2); the number of correct responses at DSST was higher after physical effort (48.94 ± 5.49 and 51.13 ± 9.83 pre- and post-physical effort, respectively; p = 0.001).
Physiological parameters, Lake Louise Score (LLS) and Visual Analogue Scale (VAS) scores
Changes in Physiological Parameters, LLS and VAS Performance Scores at the Different Altitudes and Timepoints during Cognitive Testing
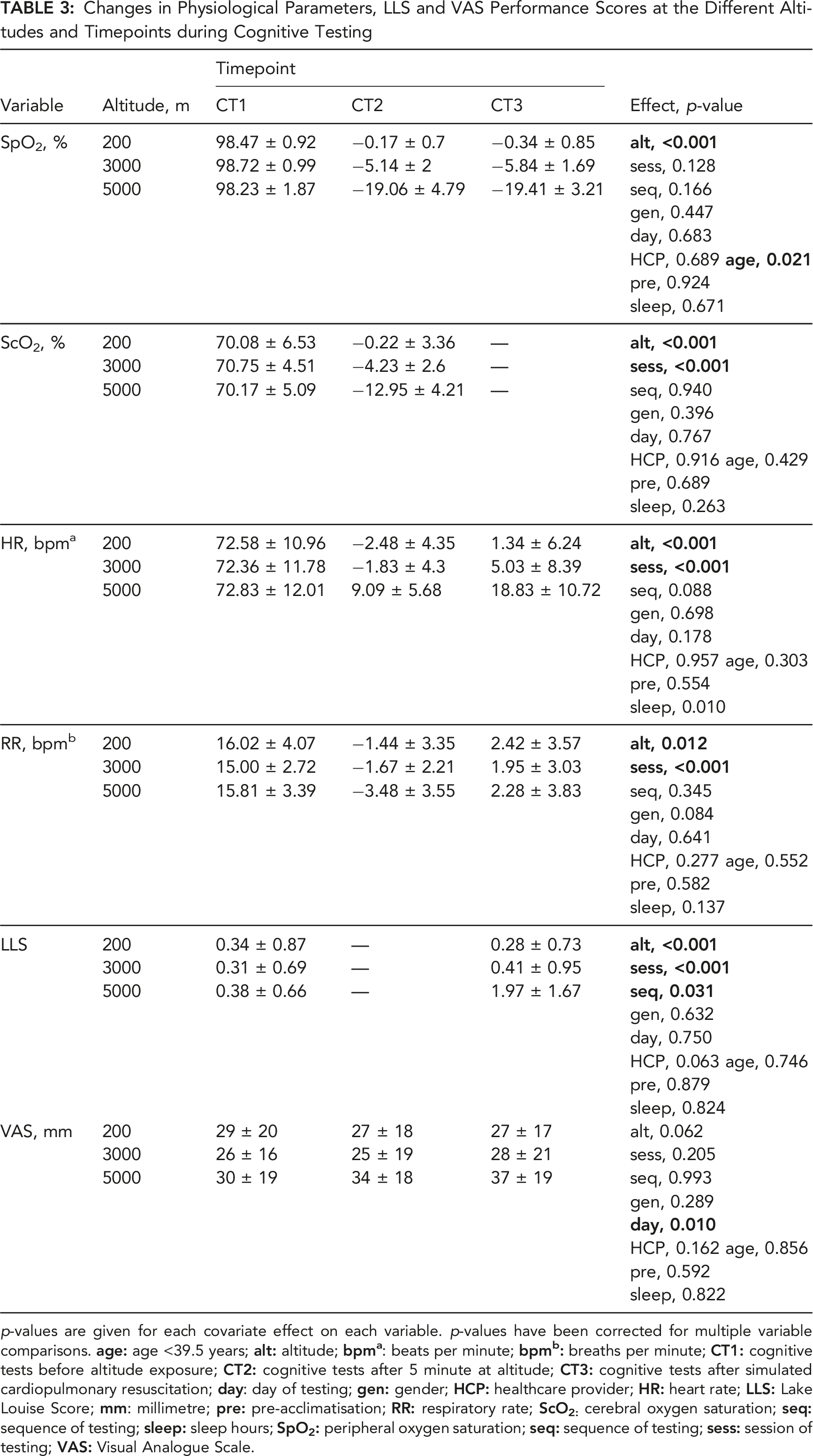
p-values are given for each covariate effect on each variable. p-values have been corrected for multiple variable comparisons.
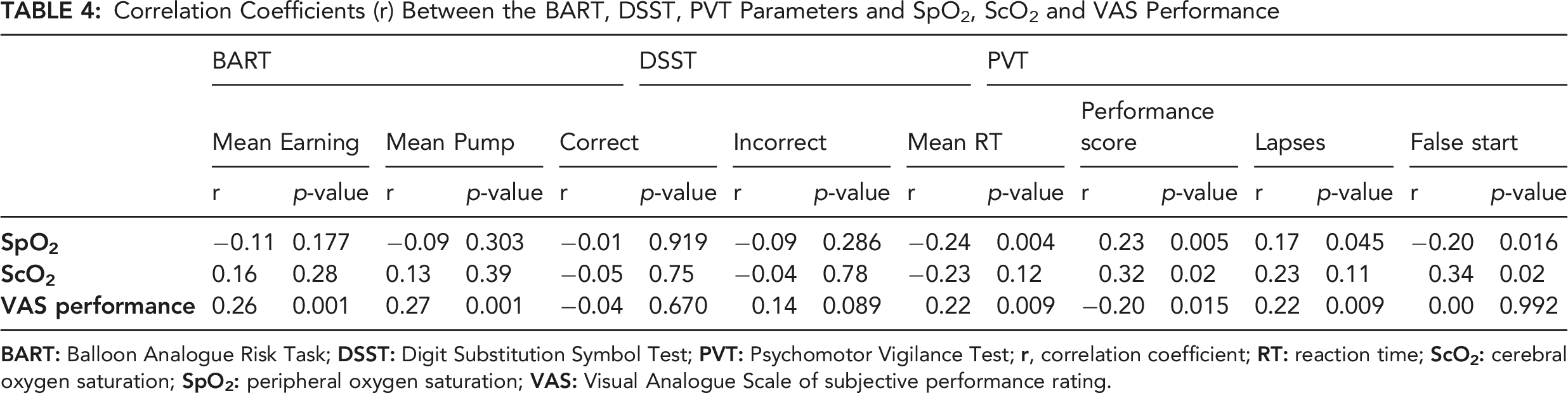
Correlation Coefficients (r) Between the BART, DSST, PVT Parameters and SpO2, ScO2 and VAS Performance
DISCUSSION
The main finding of this randomized, controlled, single-blind, crossover trial is that a single, acute exposure to hypobaric hypoxia (5000 m asl), with a rapid ascent (4 m/s) to altitude, induced a slower reaction time (i.e., reduced psychomotor vigilance) in a group of healthy HEMS personnel. Decision making and speed of processing, however, were not significantly affected by the altitude exposure. Participants (who were blinded to the altitude) overestimated their self-rated cognitive performance using a visual analogue scale even though their reaction times were slower. The findings indicate their slower reaction times were not detectable subjectively. Our results expand the knowledge on the effect of acute exposure to altitude on selected cognitive domains and could have implications in occupational health during prehospital helicopter emergency medical operations.
In prior studies, a slower reaction time has been consistently reported after acute exposure to non-simulated HH using different cognitive tests (e.g., Simon task, PVT-10, Simple Reaction Test), different time of cognitive test administration after altitude exposure (from 3 hours to 75 days), as well as different altitude reached (from 4350 to 6194 m asl) (Cavaletti & Tredici, 1993; Davranche et al., 2016; Kramer et al., 1993; Pun et al., 2018; Roach et al., 2014). In contrast, no difference have been reported in simple RT in other studies after both simulated (from 3842 to 4400 m asl) (De Bels et al., 2019; Li et al., 2000; Thomas et al., 2007) and non-simulated HH exposure (from 1630 to 3800 m asl) (Falla et al., 2021; Heinrich et al., 2019; Latshang et al., 2013) performed within a different time window after altitude exposure (from 1 hour to 4 days) and different cognitive tests (e.g., PVT or simple reaction test). Only two of the above-mentioned studies measured RT within 1 hour of the commencement of altitude exposure. De Bels et al. (2019) measured the PVT percentage of errors before ascent and after 1 hour at altitude (3842 m asl), and Li et al. (2000) used the simple reaction test after 1 hour of exposure to an HH equivalent of 300 m (control), 2800 m, 3600 m and 4400 m asl. Neither of these studies reported an effect of altitude. These findings, which clearly differ from the findings of the present study, could be related to the different altitude reached (<5000 m asl) and to the different test employed (Li et al., 2000) or parameter analysed (De Bels et al., 2019). The controlled environment of the terraXcube and the present study’s blinded design allowed us to analyse the effect of multiple factors (including rest and physical effort) and to show the independent effect of acute altitude exposure on RT. RT lengthening at altitude might be explained by the reduced motor speed or impairment of the required sustained attention. The use of tests such as the 9 Hole Peg Test (9-HPT) could help to elucidate the role of potential motor delay (Oxford Grice et al., 2003) and test such as the Paced Auditory Serial Addition Test (PASAT) could be used to evaluate attention and speed of information processing avoiding confounding motor delays (Gronwall & Sampson, 1974).
BART evaluates decision under ambiguity rather than under risk. Such a situation is similar to real life where most decisions are taken under ambiguity. Our results showed no effect induced by rapid ascent and acute HH exposure of 3000 and 5000 m asl. The number of pumps was not different at altitude. In contrast, previous studies using the BART test showed a higher number of pumps at altitude, thus indicating an increased risk-taking behaviour (Heinrich et al., 2019; Pighin et al., 2020). Heinrich et al. (2019) observed increased risk behaviour after 1 day of exposure to HH (3800 m asl), followed by a reduction in the next 2 days. Pighin et al. (2020) observed it after 20 min of exposure to hypoxia (FiO2 = 14.1%, corresponding to an altitude of 3000 m asl). It is possible that the different age of the participants (23.3 ± 6.8 and 28 ± 4.2 vs 39.8 ± 8.8 years in our study) and the specific study groups (in our study we focused on HEMS providers, while the previous two studies targeted climbers or university students) might explain the differences in findings. Age-related changes in decision making have been suggested to be related to alterations in cognitive abilities and emotional processing. Studies focusing on the effect of age on emotion-processing showed that processing of negative information, negative feedback and loss/punishment are reduced in older adults (Liebherr et al., 2017).
Our negative results on the DSST at rest agree with those of Walsh et al. (2020). However, the latter performed cognitive tests after several days at altitude (from 2800 to 4240 m asl in 7 days) and found no effect of altitude on cognitive performance at rest. Other studies with exposure to altitude from 3269 to 4400 m asl between a few hours to one night showed impaired performance on the DSST (Falla et al., 2021; Hu et al., 2016; Wang et al., 2013). Differences in the study population and the study design might explain the discrepancies between previous findings and those of the present study.
An improvement of cognitive functions has been described during exercise under simulated hypoxic conditions (1300 m and 2600 m asl, respectively) (Ando et al., 2013; Komiyama et al., 2015). Our study showed that the number of correct responses at DSST increased after physical effort at all altitudes. A recent narrative review suggested that the effects of exercise combined with hypoxia on cognitive function may be related to different factors such as exercise duration (>20 min, intensity, hypoxia level and cognitive task type) (Ando et al., 2020). Exercise to volitional exhaustion can cause worsening of cognitive functions under hypoxia (3000 m asl) (Piotrowicz et al., 2020). Limmer and Platen (2018) reported impairment of attentional performance during extreme and HH exposure without any influence of prolonged exercise. Walsh et al. (2020) showed a negative effect of combined exercise and hypobaric hypoxia (4240 m asl) on DSST results but not on other tests that assessed processing speed, working memory, selective and visuospatial attention, and inhibitory control (e.g., Stroop, task-switching task, visual search task).
Our data have practical implications for occupational safety not only for pilots, but also for other professional and non-professional healthcare providers of HEMS personnel. Helicopters are unpressurised and usually not equipped with a fixed oxygen installation despite the fact that they temporarily ascend to an altitude between 3000 and 5000 m asl during search and rescue (SAR) missions and during secondary transports in mountainous and remote areas. HEMS crews are routinely exposed to HH of altitudes between 3000 and 5000 m asl, not only with rapid ascents (of around 4 m/s), but also after landing, during take-off, and hoist operations (Pietsch et al., 2018).
Slowing of RT in our PVT (of around 5 ms at 5000 m asl) after acute exposure to altitude is similar to what has been found by Behrens et al. (2019) in another group of healthcare providers (i.e., nurses) in which the same PVT was used. Behrens et al. (2019) reported a similar slowing of mean RT (of around 6 ms) after sleep deprivation due to working a night shift, when compared to a day shift. As reduced psychomotor vigilance occurred in HEMS personnel after only a single rapid ascent at rest, in the absence of sleep deprivation and additional stressors (Nowacki et al., 2019), the additive effects of multiple factors, as well as multiple exposure, should be investigated. Currently, the European Aviation Safety Agency (EASA, 2018) states that the need for oxygen is lower in HEMS mountain rescue operations at altitude, because of the shorter time periods spent compared to general aviation. However, our data show that even in a short period selective cognitive function (i.e., attention) can be affected in HEMS personnel. Moreover, the HEMS participants in our study were not able to subjectively detect the worsening of their cognitive performance (slower RT). The comparison of a subjective evaluation (blinded to altitude reached) with an objective one showed that the objective performance score (PVT) correlated negatively with the subjective VAS performance. Pre-acclimatisation was not a protecting factor. It was interesting to note that simulated cardiopulmonary manoeuvres (up to 5 min of continued chest compressions) seem to have a protective effect, probably stimulating the respiratory drive that is inhibited after a rapid ascent to altitude.
Future studies should focus on explaining the reason for RT lengthening at altitude, monitoring motor speed and sustained and vigilant attention effects even at different altitudes between 3000 and 5000 m asl and verifying the present findings in field studies. Countermeasures such as the use of oxygen should be investigated, as well as the potentially additive effects of repeated altitude ascent on the same day, sleep deprivation and additional stressors.
Strengths and Limitations
This is the first single-blind RCT investigating the effect of acute exposure to altitude on cognitive functions in HEMS providers under controlled laboratory conditions. The study replicated a typical altitude ascent and operation for helicopter crews in an international group of HEMS personnel in a controlled simulated hypobaric hypoxic environment. A strength of the study was its blindedness, so it was highly likely to produce results unbiased by prior knowledge of altitude exposure. The short test battery used in the present study included tests used by other studies investigating the effects of these levels of altitude in high performing subjects (Basner et al., 2015; Pighin et al., 2020) and is supported by parallel physiological monitoring. Computer-based PVT to assess sustained attention lacks normative data accounting for different age and gender groups. This hampers the application of the current data in the evaluation of impaired attention for occupational purposes. HEMS personnel, in their rescues, experience both processive stressors (e.g., time pressure) and systemic stressors (e.g., HH, fatigue, extreme temperature, wind) and it is known that stressful condition elicit riskier behaviour (Nowacki et al., 2019). Simulated environments, such as in the present study, make it possible to control many of these stressors, but the current study design did not aim to evaluate their additive effects on altitude. An evaluation is planned in the future at the terraXcube and in-field studies that would afford examination of any combined systemic and environmental stressor on cognition.
Conclusions
Acute exposure to HH equivalent to 5000 m asl induced a slower reaction time amongst HEMS personnel. The slower RT was not detectable subjectively. Decision making and speed of processing were not significantly affected by the altitude exposure. Cognitive function seemed to differ with and without physical effort such as simulated resuscitation manoeuvres also at altitude.
Footnotes
ACKNOWLEDGMENTS
We thank Giada Nicoletto (Faculty of Medicine, University of Padova, Italy) for support in experimental setting preparation and data collection, and the colleagues from the terraXcube facility (Eurac Research, Italy) for support in experimental setting preparation. We thank the colleagues of the International Commission for Alpine Rescue (ICAR, Kloten, Switzerland) for invaluable scientific discussion. We thank Croce Bianca (Bolzano, Italy) for the resuscitation manikins. We thank Jenny Kim (Southwestern Medical Center, University of Texas, Dallas, TX) for editing the manuscript. The authors thank the Department of Innovation, Research, University and Museums of the Autonomous Province of Bozen/Bolzano, Italy for covering the Open Access publication costs.
Key Points
Simulated hypobaric hypoxia at altitudes equivalent to 5000 m above sea level, slowed reaction times in HEMS personnel, but did not affect other investigated cognitive domains. Participants did not subjectively notice their slower reaction times. These findings expand the knowledge on the effect of acute exposure to hypobaric hypoxia on cognitive domains, confirm an independent effect of altitude and have practical implications in the clinical setting of prehospital emergency medicine.
Author contribution
MFa, KH, MFk, EMW, AV, AD, HB and GS conceptualization. MFa, AV, HB and GS project administration and supervision. MFa, KH, MFk, EMW, AV, BW, MP, HB and GS methodology. MFa, KH, AV, MJvV, JB, MP, HB and GS investigation. MFa, KH, MFk, EMW, HB and GS data analysis and interpretation. MFa, MFk and GS original draft. MFa, KH, MFk, EMW, AV, MvV, BW, JB, MP, AD, HB and GS review and editing.
Marika Falla is a trained neurologist specialized in movement disorders and currently senior researcher at the Center for Mind/Brain Sciences of the University of Trento in Italy and collaborator at the Institute of Mountain Emergency Medicine at Eurac Research, Bolzano, Italy. She is member of the board of the Italian Society of Mountain Medicine. She is interested in high-altitude neurological effects in healthy individuals as well as in neurological patients and in the understanding of several aspects of different movement disorders (e.g., Parkinson’s disease). In clinical practice she works with neurological patients. Lecturer at the University of Trento (Italy).
Katharina Hüfner is a trained neurologist as well as specialist in psychiatry and psychotherapeutic medicine. She is a professor at the University Clinic for Psychiatry II (Psychosomatic Medicine) at Innsbruck Medical University in Austria. Her current research focus is on the effect of physical activity and the alpine environment on mental health as well as psychiatric symptoms at high and extreme altitude. In clinical practice she works primarily with patients with somatoform and functional neurological disorders and aims to help individuals bring about behaviour changes in order to reduce symptom load. Every free minute she spends out and about in the mountains near her home or abroad.
Markus Falk has the master degree of Mathematics in Biostatistics, is a self-employed biostatistician, data analyst, contract lecturer.
Elisabeth M. Weiss, MD, PhD. University of Innsbruck, Department of Psychology, Innrain 52 f 6020 Innsbruck, Phone: 0512–507-56057, email:
Anna Vögele is a General Practitioner, working in medical research since 2012. She worked at the Medical University Paracelsus of Salzburg, Austria and the South Tyrolean Academy of General Medicine in Bolzano, Italy where- besides teaching activities-her research focus was on polypharmacy in the elderly population. Since 2018 she is a senior researcher at the Institute of Mountain Emergency Medicine at the European Academy (Eurac) in Bolzano and focusses on research in search and rescue (SAR) and mountain medicine. Besides her research activities she is clinically working in local nursing homes in South Tyrol. Whenever she can she spends time hiking or paragliding in the mountains.
Michiel J. (Jan) van Veelen. Current Affiliation: Institute of Emergency Medicine, Eurac Research, Bolzano, Italy. Medical Doctor (MD), 2010, Erasmus University, Rotterdam, The Netherlands Emergency Medicine Specialist, 2015, Haaglanden Medical Center, The Hague, The Netherlands Diploma in Tropical Medicine and Hygiene, 2015, Royal Tropical Institute (KIT), Amsterdam, The Netherlands. Lecturer Emergency Medicine, 2016–2018, University of Botswana, Botswana Fields of research: Emergency medicine, Prehospital emergency medicine, Mountain emergency medicine, Resuscitation science, Medicine in extreme environments, Medicine in limited resources, Wilderness medicine.
Bernhard Weber is a Psychological and Technical Assistant (PTA) and Doctoral Student at the Department of Psychology, University of Graz, Austria. His research interests mainly focus on brain imaging techniques (fMRI, Voxel-Based Morphometry (VBM), and Resting-State fMRI). Together with another Lab-Member, he received the Styrian Brain Research Initiative (inge.st) Research Award 2019 for the work on “Learning Unicycling Evokes Manifold Changes in Gray and White Matter Networks Related to Motor and Cognitive Functions.” **Weber et al. (2019). Scientific Reports, 9 (1), 532. ![]()
Jonas Brandner, MD. As a passionate rock climber and mountaineer with no prior research involvement I was given the unique chance to support this project when still a medical student. My main fields of interest are mountain and high altitude medicine and I am looking forward to taking more responsabilities in future research projects.
Martin Palma. Current Affiliation: Information Technologies and Institute of Emergency Medicine, Eurac Research, Bolzano, Italy. Research Software Engineer, since 2013, Eurac Research. Systems Engineer, 2010–2013, Free University of Bozen-Bolzano. Research Assistent, May - July 2010, at the Software and Systems Engineering Center of the Free University of Bozen-Bolzano. Bachelor of Science (BSc), 2005–2010 in Computer Science at the Free University of Bozen-Bolzano. Fields of research and interests: Mountain emergency medicine, distributed systems, big data storage.
Alexander Dejaco currently works as Anaesthesiologist at the University Hospital Regensburg, Germany. He is dual trained as biomedical engineer and medical doctor. He completed a bachelor and master in informatics at the Vienna University of Technology, following that up with a PhD in biomedical engineering with focus on computationally complex problems in biomechanics. In parallel he studied medicine at the Medical University of Vienna. Having completed all studies he began working as anaesthesiologist and prehospital emergency physician. Next to the clinical tasks he continues doing scientific work in the areas of emergency mountain medicine, medical informatics and anaesthesia.
Hermann Brugger, General Practitioner at the National Health Service, Bruneck, Italy, from 1983–2017 and emergency physician for the Emergency Medical System and mountain rescue physician of the Mountain Rescue Organization of South Tyrol from 1983–2017. Founder and vice-head of the EURAC Institute of Mountain Emergency Medicine, Bolzano, Italy, 2009–2022, founder of terraXcube. Associate Professor at the Innsbruck Medical University, from 2006. Member of the Board of the Medical Commission of the Union Internationale des Associations d’Alpinisme UIAA MEDCOM, 2001-date; President of the International Commission for Mountain Emergency Medicine ICAR MEDCOM, 2001–2009. President of the International Society of Mountain Medicine, 2016–2021. Scientist and author in emergency medicine, enthusiastic alpinist with several ascents in all continents.
Giacomo Strapazzon is the head of the Institute of Mountain Emergency Medicine at Eurac Research, Bolzano, Italy and member of the steering committee that conceptualized and developed the environmental chamber terraXcube. He is a consultant in emergency medicine and delegate for the Italian Mountain Rescue – CNSAS at the International Commission for Alpine Rescue – ICAR. He is interested in mountain emergency medicine including helicopter and search and rescue operations, cold injuries and high altitude effects with a special interest in cerebral effects and new imaging monitoring perspective. Lecturer at the University of Padova, Varese and Verona (Italy).