
Abstract
Objectives
The goal of this study was to evaluate whether immersive virtual reality (VR) training used in conjunction with interactive online learning improved procedural skills in medical students, using chest tube insertion as a model.
Methods
Medical students (n = 30) with limited or no experience with chest tube insertion were randomized into control and VR groups. All participants received access to a previously developed online module to learn the equipment and steps involved in performing chest tube insertion. The VR group received additional training using commercially available software. All participants were then asked to perform chest tube insertion on a standardized mannequin. Technical skills were assessed by surgical experts, blinded to the group allocation, using a modified Objective Structured Assessment of Technical Skill (OSATS) rating scale (11-items, each scored 1-5). Multiple-choice tests and a 5-point Likert-scale were used to assess theoretical knowledge and to rate confidence level before and after training. Data are presented as median and interquartile range.
Results
After training, all participants showed significant improvement in knowledge from baseline; rate of correct answers was 50% pre-training [40.0-66.7]; 80% post-training [73.0-93.3]; P < 0.0001). There was no statistically significant difference between the two groups in knowledge before and after training. The VR group spent <60 min in VR training and had better procedural performance (OSATS scores: controls: 39 [33-45]; VR: 46 [42.0-50]; P = 0.03) and higher confidence (controls: 3 [3-4]; VR: 4 [4-5]; P = 0.002).
Conclusions
Adding VR simulation to online learning improved technical skills and confidence in medical students learning chest tube insertion.
Background
Developing procedural skills is fundamental to undergraduate medical training, and students must demonstrate competence.1,2 Despite efforts to improve learning outcomes, self-reported competence in procedural skills among medical students remains low, suggesting that current teaching approaches remain insufficient. 3 To address this training gap, novel strategies are needed.
Current Training Methods
Procedural skills training has evolved to include a combination of didactic instruction, hands-on simulation, and bedside teaching. However, these well-established training methods have significant limitations. First, didactic approaches have been shown to be relatively ineffective for adult learners in medicine. 4 Second, albeit hands-on simulation is widely accepted as an optimal modality for teaching procedural skills,5-8 the high associated costs and required resources often limit students to a one-off experience with little or no opportunity for further practice. Third, circumstances in which to learn or train with patients in the clinical setting are highly variable and can create concerns for patient safety.
Virtual Reality in Simulation-Based Education
Optimal preparation and subsequent reinforcement may improve the effectiveness and durability of in-person simulation training. 9 Virtual reality (VR) is an emerging tool in surgical education that may fulfill this need. VR is an immersive technology that permits trainees to practice a procedure independently and on demand. 10 VR simulation describes an entirely virtual interactive simulation whereby users are fully immersed within a 3-dimensional environment projected onto a head-mounted display, allowing 360 degrees of visual immersion and real-time manipulation of virtual equipment via hand-held controllers. 11 This technology provides a potential approach to facilitate the transition from theory to practice by empowering trainees to personalize their learning experience and independently develop their clinical competence.11-13 Further, the increasing availability and reduced costs of VR simulation make it possible and practical to create standardized learning opportunities, potentially reducing inequalities within medical education globally. 10 However, the evidence for the effectiveness and value of VR training for procedural skills training in medical students is lacking.
Objective
This pilot study aimed to evaluate the value of adding immersive VR to an interactive online learning module to better prepare medical students for mannequin-based simulation training, using chest tube insertion as a model. Expert surgeons selected this procedure for its clinical importance and the availability of a previously developed and proven effective online learning module. 14 The outcomes assessed were theoretical knowledge, technical skills, and confidence in performing the procedure.
Method
This pilot study was conducted at McGill University’s Steinberg Centre for Simulation and Interactive Learning from June to August 2023. First- and second-year medical students from the 4-year undergraduate medical program at McGill University were eligible and invited to participate via email and online announcements. Exclusion criteria included previous hands-on experience with chest tube insertion or training in Advanced Trauma Life Support (ATLS). A sample size of 30 participants was calculated to be sufficient for a pilot trial. 15 This report has been written in accordance with the Consolidated Standards of Reporting Trials (CONSORT) guidelines and ethics approval was granted by the university’s institutional review board (A04-E18-23A). Written informed consent was obtained from all participants.
Study Design
This study was a single-centre, assessor-blinded, pilot, randomized controlled trial. Thirty medical students, who had limited exposure to, but no personal clinical experience with chest tube insertion, participated in the study. Participants were randomly allocated on a 1:1 basis to either the control (online learning only) or VR (online learning with immersive VR) group before completing a mannequin-based simulation of chest tube insertion (Figure 1). CONSORT flow diagram of study recruitment. VR, virtual reality.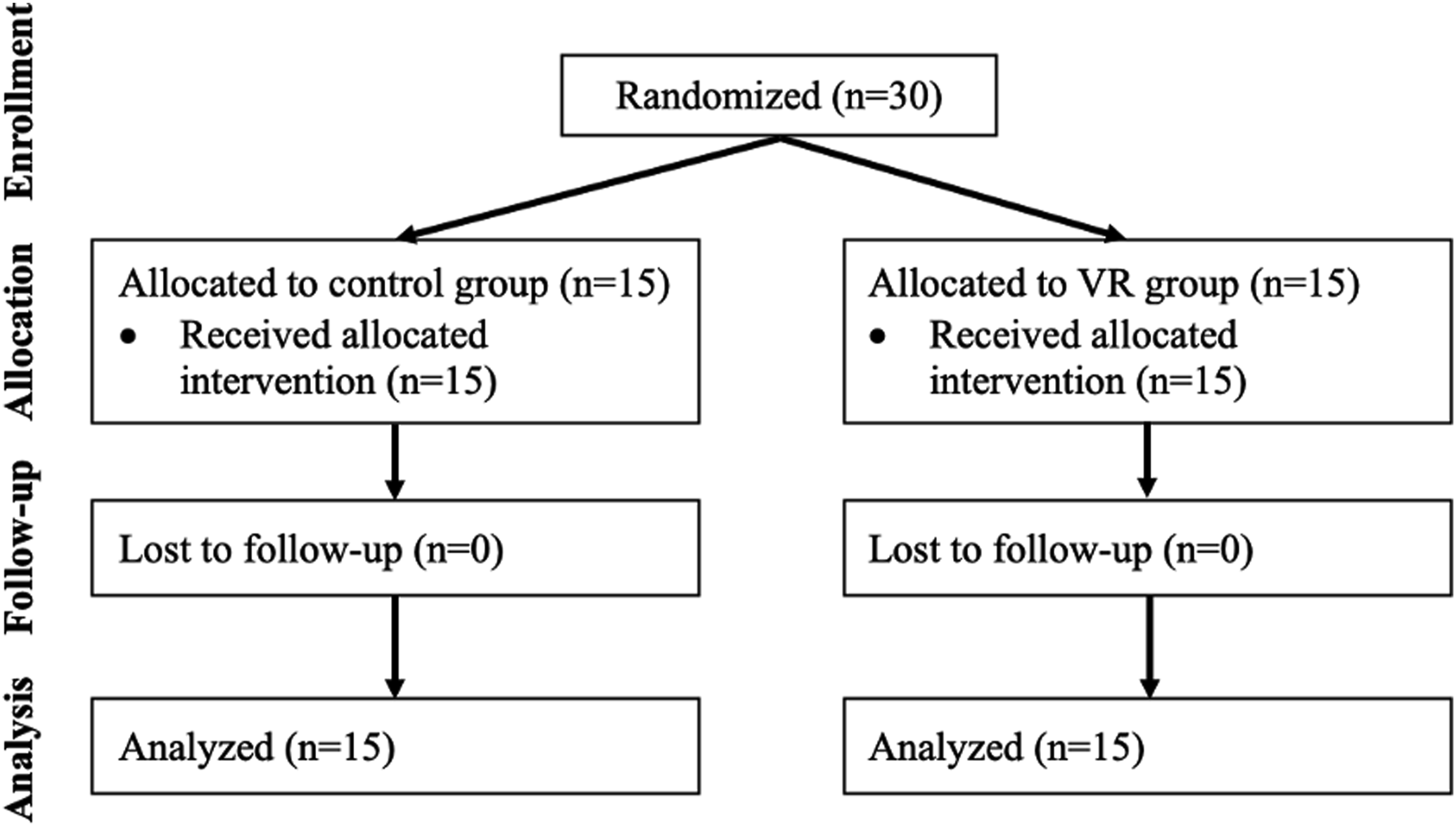
A 2-week training protocol was adopted for this study (Figure 2). First, all participants completed a 15-min pre-training questionnaire of demographic information, baseline knowledge and confidence in performing the procedure. This was followed by a 2-week period where all participants were requested to complete a previously created interactive online learning module on chest tube insertion.
14
Participants in the VR group received standardized VR training over two in-person sessions. The first session occurred 1 week after participants received access to the online module. This included a short tutorial for participants to familiarize themselves with the VR equipment and virtual environment followed by two repetitions of the VR chest tube insertion simulation. The second session took place 2-weeks later and involved two additional repetitions of the VR simulation. This was conducted 30-min prior to the hands-on mannequin-based assessment. At the end of the 2-week period, all participants were asked to perform chest tube insertion in a mannequin model, without coaching, while being evaluated by an expert surgical assessor blinded to their study group. Three surgeons participated in the assessment. Participants consented to being recorded (video and audio) during the live assessment. Video-based assessment was done on a selected group of videos reflecting a range of performance scores by at least 2 assessors (self and one other) to assess intra and inter-rater reliability. Immediately following the hands-on simulation, participants completed a post-training assessment to re-evaluate knowledge and confidence. Study flow chart with timeline. VR, virtual reality.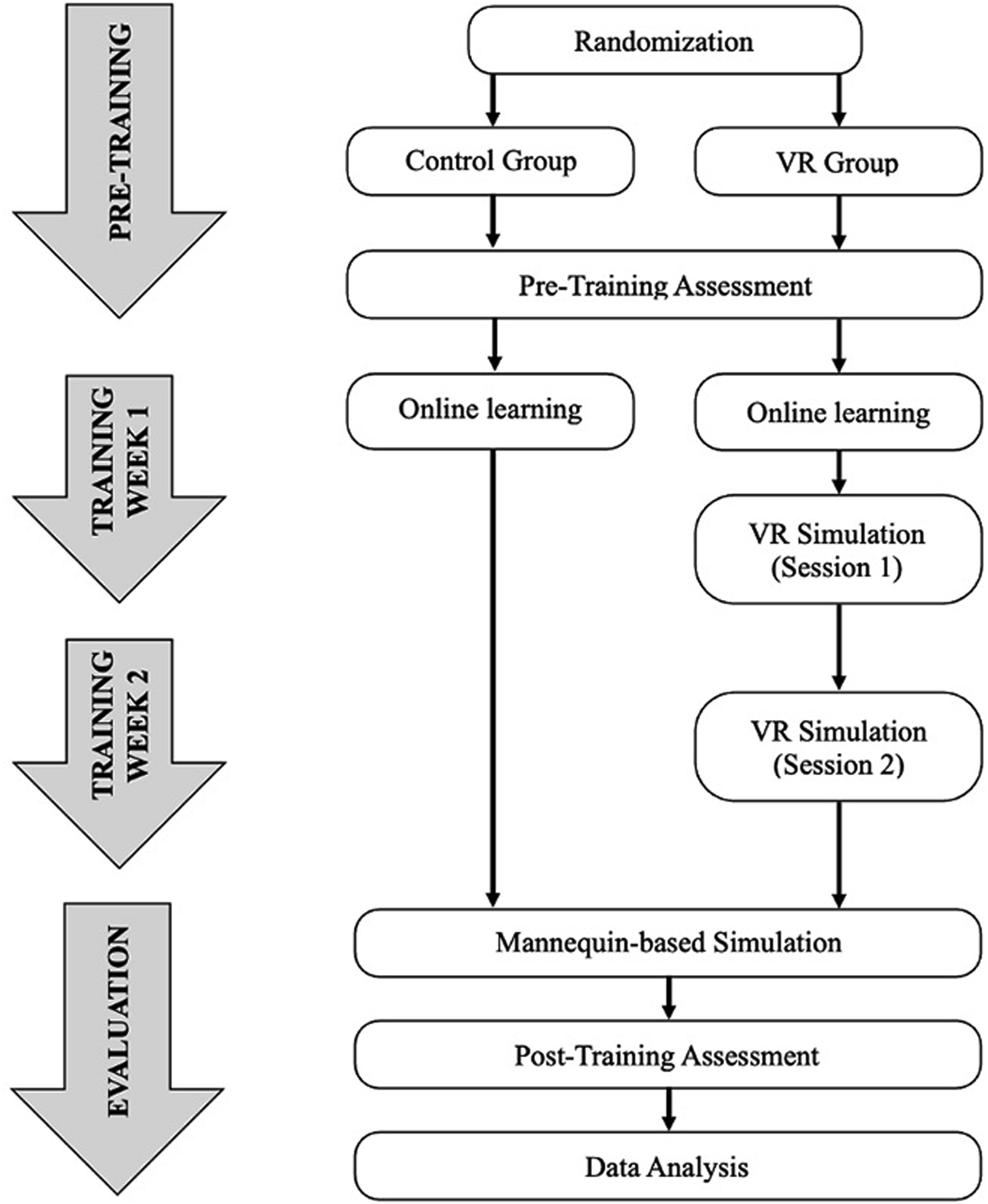
Materials Used
Online Learning Module
All participants were provided access to an interactive online learning module previously developed by our group and found to be effective in preparation for hands-on simulation training. 14 This module incorporated materials on chest tube insertion currently taught to surgical residents at McGill University and was based on the Advanced Trauma Life Support (ATLS) guidelines. The module can be completed in approximately 15-20 minutes and is a comprehensive and interactive educational tool designed to prepare medical trainees to perform chest tube insertion. Procedural learning included: identification of anatomical landmarks, surgical site preparation (eg, disinfection, draping), local anesthesia, skin incision, dissection, digital exploration, tube insertion, and tube fixation. Further, the module included an instructional video demonstrating the procedure as it would be performed in a mannequin-based simulation. Participants were provided access to the online module and the pre- and post-training assessments, used to evaluate knowledge and confidence, through McGill University’s online learning management system (D2L, Kitchener, ON, Canada). Participants were required to complete all components of the online module before attending the hands-on simulation and their activity was tracked throughout the training period to ensure compliance.
VR Simulation
VR training was provided using the chest tube module of a commercially available product (Vantari VR, Sydney, Australia) delivered through an Oculus/Meta Quest 2 VR Headset (Meta, Menlo Park, CA, United States), and ergonomic hand controllers. The simulation places the learner in a fully immersive 3D operating room environment and requires them to use natural motor movements to interact with surroundings to sequentially complete 26 procedural steps with the help of integrated instructions (Figure 3).
16
The VR simulation program provides real-time feedback based on its embedded metrics. A Vantari VR instructor was present at each session to teach fundamentals of the use of immersive VR and to provide technical troubleshooting, if needed. Surgical experts verified that the VR simulation was aligned with ATLS guidelines and that there were no significant discrepancies with the online learning module. Screenshots of the Vantari VR chest tube insertion simulation. A: Virtual operating room with patient, surgical tray, and procedural instruments; B: List of completed, current, and pending procedural tasks; C: Administering local anesthetic; D: Handling of clamp and chest tube.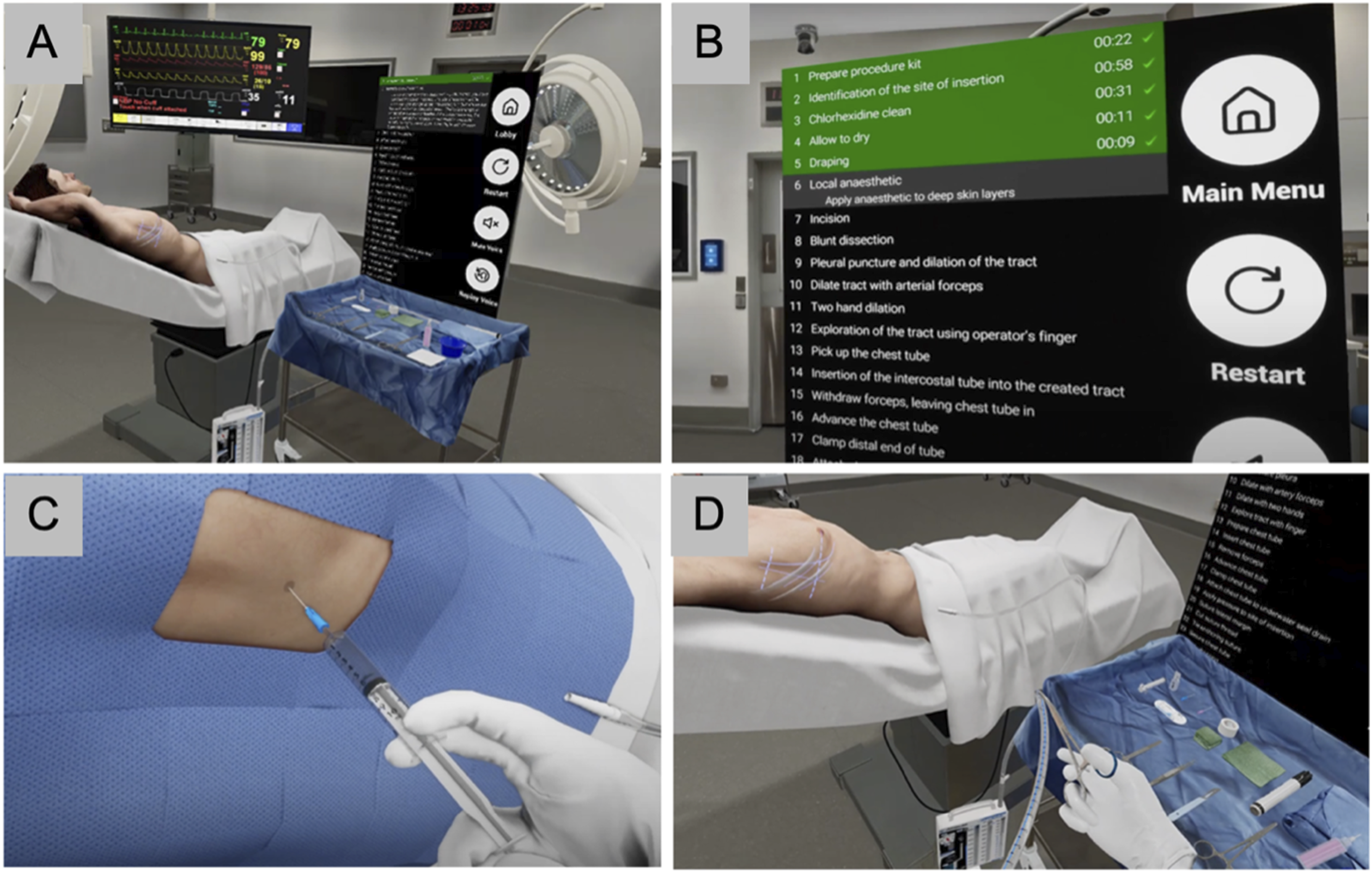
Mannequin-Based Simulation
At the end of the 2-week training period, participants visited the simulation center to perform chest tube insertion on a standardized mannequin (Figure 4). Each participant was observed by an experienced surgeon blinded to the group allocation and given 15 minutes to perform the procedure using similar equipment to that in the online learning module and VR simulation. Additionally, they were asked to explain their steps as they performed them to demonstrate their understanding. If a participant was unable to proceed at any point, they could ask for a prompt, and this was reflected in the assessment score. Participant performing a mannequin-based simulation. A: Technical skill assessment by an expert; B: Standardized mannequin draped for the chest tube insertion.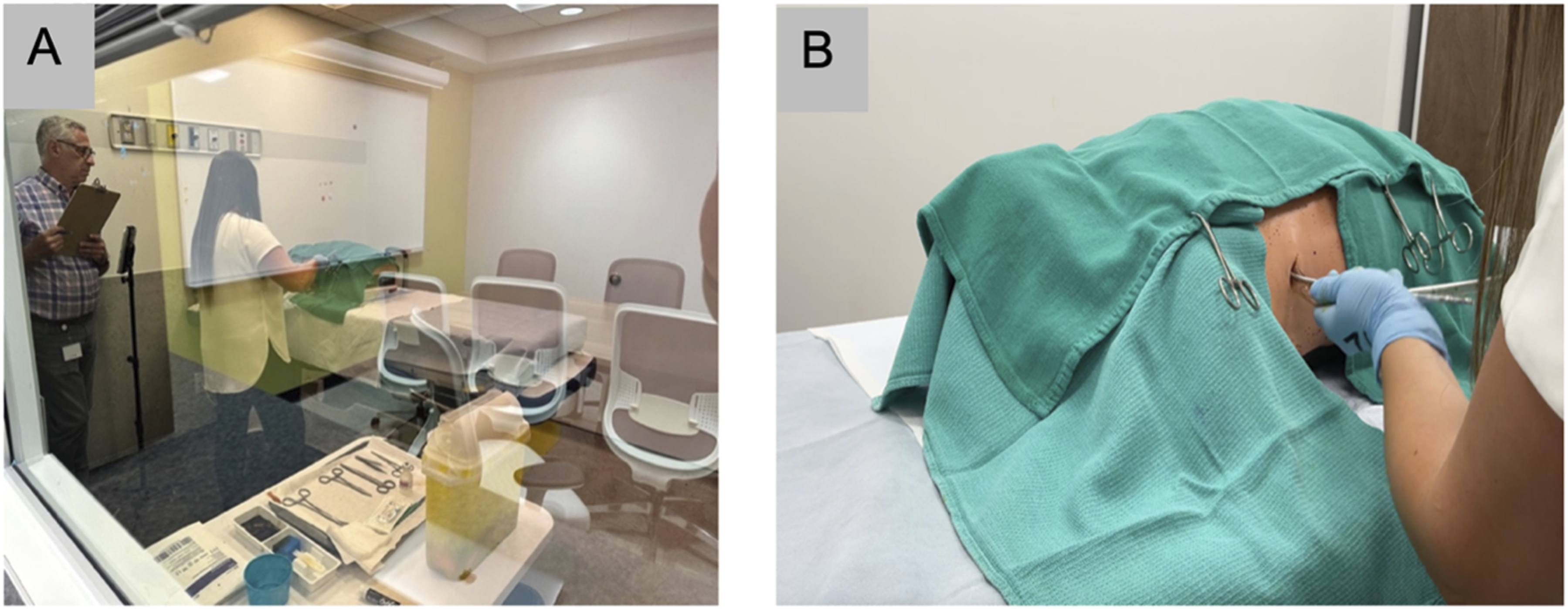
Outcomes
Time spent completing the tutorial and for each VR simulated chest tube insertion was recorded.
Theoretical knowledge was assessed using a 15-question, multiple-choice test administered in the pre-training and post-training assessments via the learning management system. Questions were developed and reviewed by a panel of experts in surgery and education to reflect key learning points about chest tube insertion. 14 These tests were completed remotely for convenience, but participants were encouraged to comply with standard exam conditions (independent completion, closed-book).
Technical skills were assessed during the mannequin-based simulation by expert surgeon-assessors, blinded to the group, via direct observation using a previously reported modified Objective Structured Assessment of Technical Skill (OSATS) rating scale for chest tube insertion. 17 The OSATS rating scale is composed of 11 items; each item is scored using a 5-point Likert scale to generate a total score (Supplemental Material). Higher scores reflect greater technical skill; the best possible score is 55. In an effort to reduce inter-rater variability, assessors met in advance of the study, reviewed some trial performances together (not included in study data), and came to consensus regarding scoring. Live performance ratings were correlated with video-based ratings to assess intra- and inter-rater reliability using Intraclass Correlation Coefficients as described above.
Confidence in performing chest tube insertion was rated using a self-reported, 5-point Likert scale from 1: “not confident at all” to 5: “very confident.” The questionnaire was administered in the pre- and post-training assessments via the learning management system.
Statistics
Quantitative analysis was conducted to examine the scores for knowledge, technical skills, and confidence. Data are reported as median with interquartile range. Results are shown as box and whisker plots. Intergroup and intragroup comparisons were done using non-parametric Mann-Whitney U test, Wilcoxon signed rank testing, and Pearson’s chi square test. Statistical analysis was conducted using JMP Pro 15 (SAS Institute, North Carolina, USA). P values less than 0.05 were considered statistically significant. Intra- and inter-rater reliability was calculated using the intraclass correlation coefficient (ICC). ICC values less than 0.5 were regarded as poor reliability, 0.5 to 0.75 as moderate reliability, 0.75 to 0.9 as good reliability, and those greater than 0.9 as excellent reliability.
Results
Participant Characteristics
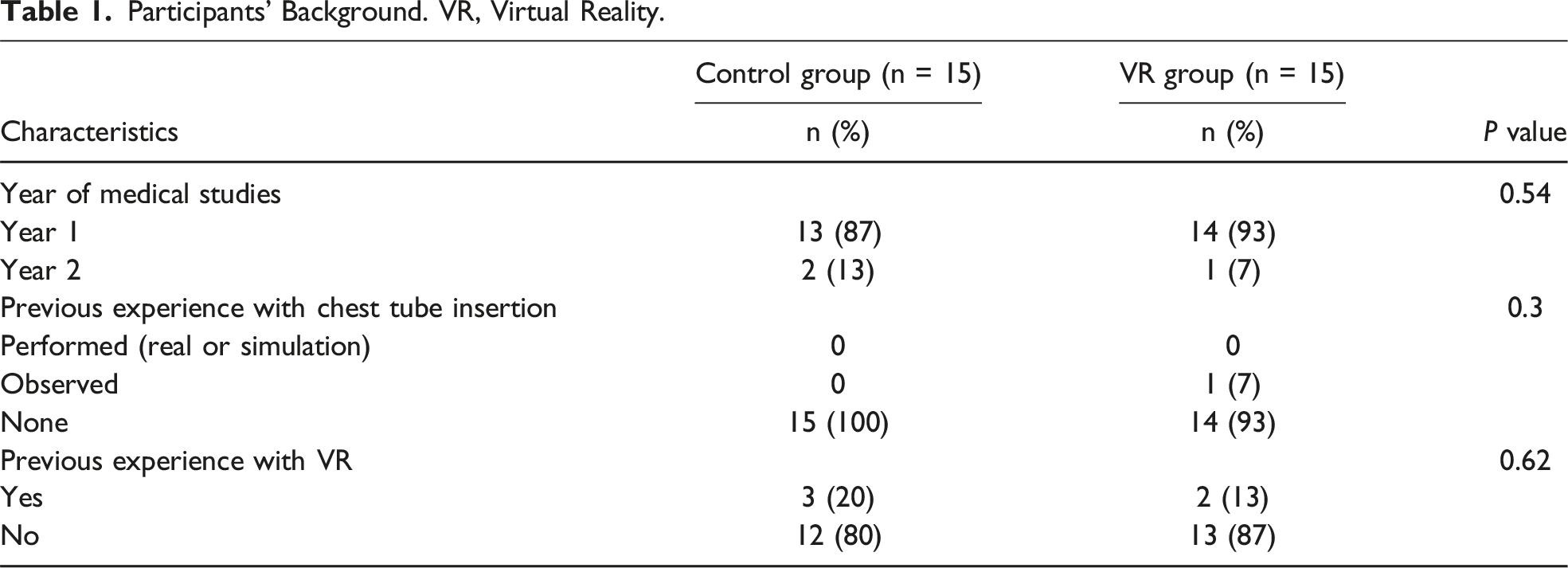
Participants’ Background. VR, Virtual Reality.
Time Spent in VR Simulation
Participants in the immersive VR group spent less than 60 cumulative minutes in VR training: the VR tutorial took 4 minutes [3-5]; VR chest tube insertion simulations (4 total, including 2 repetitions during each of the two training sessions) totalled 39 minutes [30-4]. Median time to complete each VR simulation was 9 minutes [8-10]. There were no reports of cybersickness during VR simulation.
Theoretical Knowledge, Technical Skills and Confidence Level
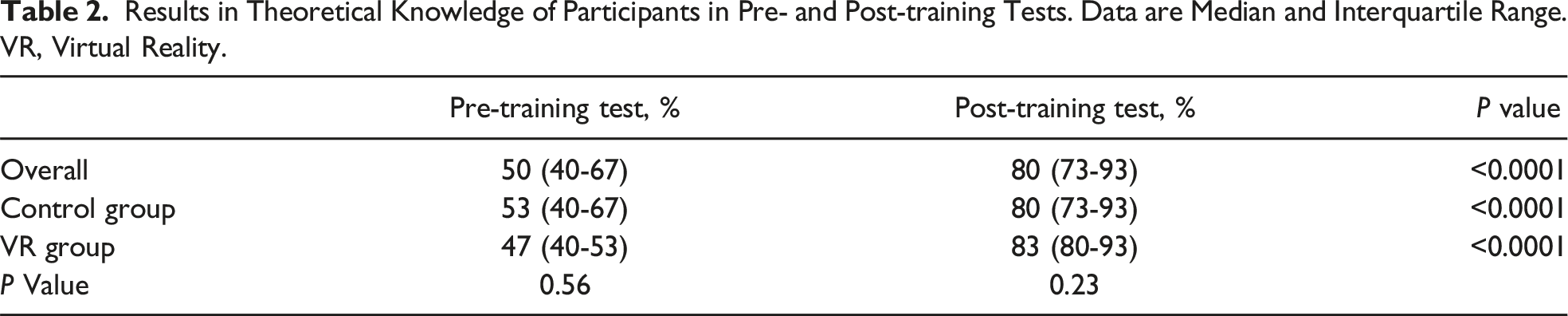
Results in Theoretical Knowledge of Participants in Pre- and Post-training Tests. Data are Median and Interquartile Range. VR, Virtual Reality.
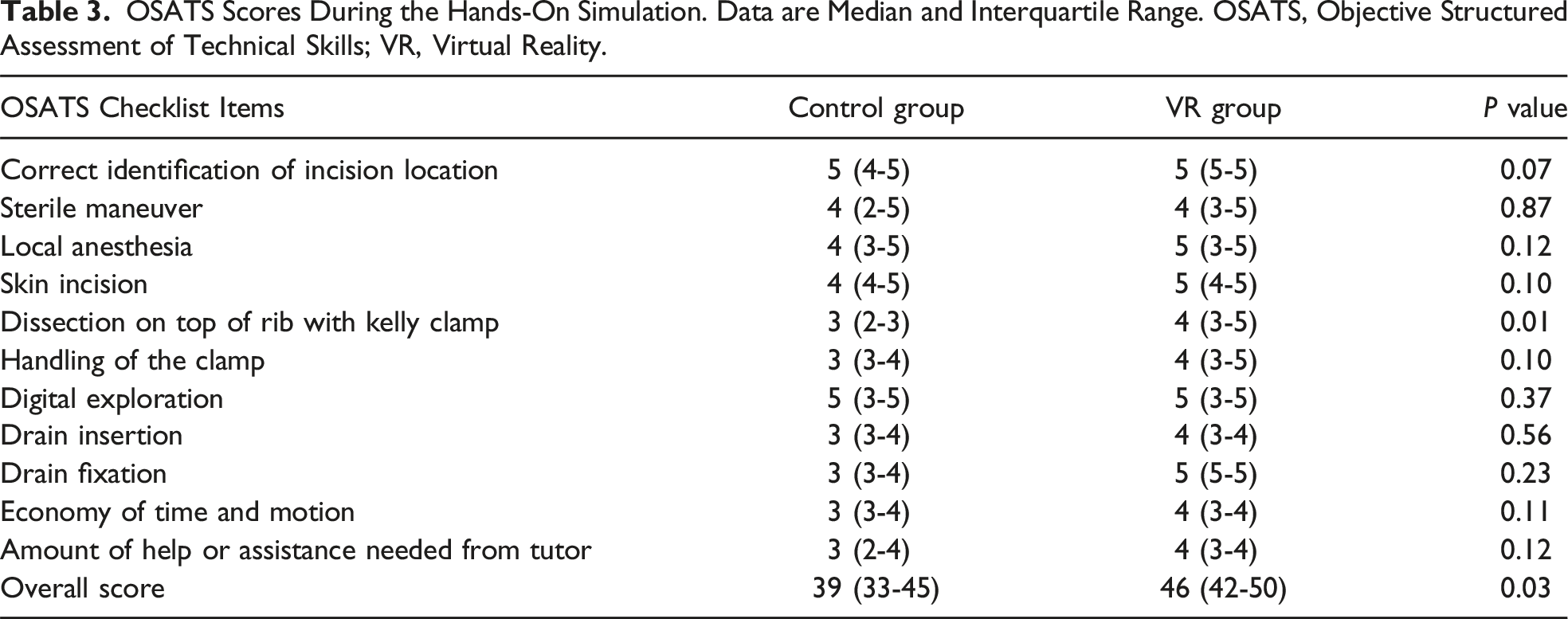
OSATS Scores During the Hands-On Simulation. Data are Median and Interquartile Range. OSATS, Objective Structured Assessment of Technical Skills; VR, Virtual Reality.
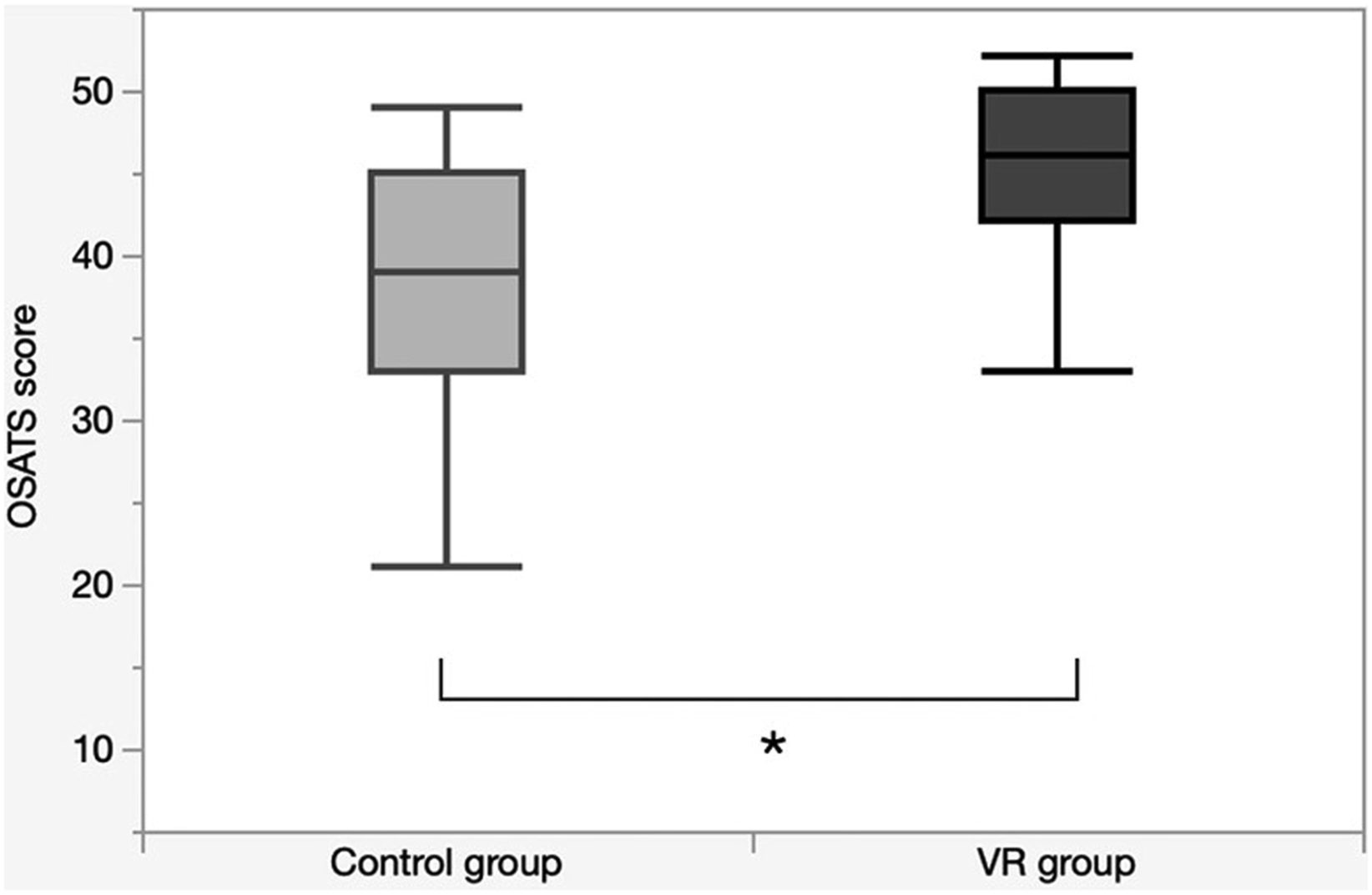
Comparative analysis of technical skills by total OSATS scores between the control and VR groups (*), P = 0.03. OSATS, Objective Structured Assessment of Technical Skills; VR, virtual reality.
Discussion
The teaching of procedural skills in undergraduate medical training remains an ongoing challenge. 5 While the majority of hands-on clinical training occurs during residency, many universities recognize the benefit of integrating these experiences early on, particularly through simulation. Despite efforts to fuel early skill development through hands-on simulation experiences, competence requires repeated exposure and standardized practice, but opportunities are limited. Our goal is to optimize the value and impact of in-person simulation training with improved preparation, while minimizing expense and faculty demand. Online learning and independent immersive VR training have the potential to provide such opportunities, but evidence of their value for teaching procedural skills to medical students is lacking.
Multiple studies have demonstrated the benefits of VR in medical education and surgical training,18-20 with some institutions having already made VR training mandatory as preparation for surgical residents. 21 In a systematic review published by Mao and colleagues 19 in 2021, the authors stated that incorporating VR into surgical training programs is supported by high-quality studies demonstrating improved procedural times, successful and accurate task completion, positive user ratings, and cost-effectiveness. 19 They also concluded that VR has strong potential to fulfill institutional training requirements within a competency-based curriculum without exhausting financial resources. In a similar study, authors concluded that medical education programs that systematically and efficiently use VR in their training strategies will significantly enhance the core competencies of their learners and concurrently improve patient care. 22
Despite some evidence supporting the use of VR in medical and surgical education, several gaps still need to be addressed within the literature. First, there is a predominance of systematic reviews and meta-analyses that focus on surgical residents. These studies are limited in the generalizability of their findings by not considering a broader range of learners, including those with less theoretical knowledge and fewer clinical experiences. Second, most of the literature examines the utility of VR for skill acquisition, with few studies considering the effects on knowledge or confidence. Lastly, a majority of these studies do not differentiate between different VR modalities (ie, immersive vs screen-based).
A recent randomized trial with laparoscopic novices showed that VR may not sufficiently address theoretical learning in novice learners and should be supplemented by independent cognitive training. 23 Lastly, the literature remains lacking regarding suggestions on how VR can be integrated into existing simulation-based curricula. In a previous study, we found that a well-designed, interactive online module was more effective at preparing surgical residents for a single in-person simulation experiences than traditional methods, such as lectures or suggested readings. 14 According to current suggestions, adding VR to this blended approach may prove particularly effective in a population of medical students.24-26
This pilot study compared the learning effect of two modalities (online learning only vs online learning with VR) as part of a blended learning approach for teaching procedural skills to medical students in preparation for a hands-on simulation experience: Overall, the results demonstrate that a relatively short time in VR simulation can effectively enhance technical skills and confidence when used in such a blended approach.
All participants demonstrated a statistically significant increase in post-training knowledge compared to baseline. As one might expect, there was no difference between the study groups, suggesting that a well-designed online learning module is highly effective at teaching the underlying knowledge about chest tube insertion.
We have also found that immersive VR training is effective at teaching technical skills to novice learners. Taken together, our data supports the use of blended or multimodal approaches to procedural training. Previous studies that have investigated the use of VR head-mounted displays in medical education have identified immersion as an essential element in enhancing the effect of simulation-based learning. 27 It is proposed that immersion elicits a higher level of presence within participants, whereby they truly perceive themselves to be in the virtual environment in which the simulation is occurring. 28 Enhancing immersive presence has been shown to induce centricity and enrich the user experience, which has been shown to have a significant influence on learning outcomes in VR simulation for health care education. 29
An alternative explanation for the observed findings is that the performance improvements may be less attributable to the VR training specifically, but rather to practice effect. Those who received VR training had several attempts to practice chest tube insertion virtually and familiarize themselves with the equipment and movements needed to execute the procedure correctly. Further, the VR simulator feedback allowed trainees to recognize and understand mistakes in real-time and improve their performance. No matter the reason, our data demonstrates the true potential of VR as an educational tool that can be used independently and on-demand for self-directed procedural training. The frequency and repetition with which a skill or technique is practiced influences the degree of retention, recall, and transferability. 5 VR practice may be more likely to be adopted by learners and can be a beneficial training adjunct to increase the value, impact and durability of hands-on simulation in developing procedural skills.
There also exists a potential for recency bias in the VR group, with participants potentially benefiting from practicing the procedure immediately prior to the mannequin-based assessment. This is unlikely to explain the observed differences in performance. First, it is important to note that the VR sessions were designed not only to allow practice of the procedure, but also to provide immediate, real-time feedback. This feedback loop likely contributed to learning and skill retention during the VR sessions themselves. Second, the VR group had multiple VR sessions spread across a 2-week training period, and the final session was designed to reinforce concepts learned previously. Given that each VR session involved repetition and independent interaction with the virtual environment, the recency effect of a single session directly preceding the mannequin-based assessment would likely be minimal in comparison to the cumulative learning benefits throughout. Finally, even if the final session resulted in a minor recency effect, it would not explain the significant differences observed between the two groups in technical skill scores and confidence. Rather, the improvements in the VR group are more likely attributed to the combined outcomes of immersive practice and real-time feedback over a prescribed learning period than to a temporal effect.
The post-training assessment revealed that participants who received VR training had significantly higher confidence in performing chest tube insertion, as demonstrated by the Likert-scale responses. In contrast, there was no significant post-training change in confidence from baseline in the control group, suggesting that online learning alone may not impact confidence in novice learners significantly. These findings are supported by current evidence showing how immersive simulation experiences are conducive to positively impacting confidence in trainees. 30
Several training programs have adopted competency-based learning models requiring trainees to demonstrate basic procedural competence. 31 In general, this approach emphasizes experiential learning in the clinical setting, but these experiences and assessments are challenged by significant heterogeneity among patients, indications, supervision, and urgency. In the clinical environment, patient safety must be paramount. Variability in clinical experience and lack of standardized training have been shown to adversely impact confidence in performing common bedside procedures longitudinally. 32 With VR training, as with simulation training in general, the learner is central. VR may serve as an optimal modality for autonomous and self-guided practice of procedures for trainees to increase confidence in their knowledge and technical skills. Further, VR-based clinical skills training could help with confidence and competence development for students who do not have the opportunity to rotate through high-volume, high-acuity health centers. Even for students who train in these environments, the number of learners will continue to outweigh the number of available learning opportunities, hindering the chance to develop core procedural skills during clinical rotations.33,34
Our findings are consistent with the conclusions of previous studies that evaluated the educational effectiveness of VR simulation in procedural skills training, 22 and add further evidence to its value. Our findings provide evidence in support of the use of this specific VR module in training in a specific procedure (chest tube insertion) for medical students not yet exposed to this procedure clinically. Further, the high intra-rater and inter-rater reliability demonstrate that raters were consistent in their evaluations, which strengthens the validity of these results.
However, one must be cautious in generalizing these findings. Not all commercial VR products are the same and, even within one vendor’s catalog, there may be variability in the effectiveness and quality of individual modules. Our study addressed relatively naïve early-year medical students. We cannot extrapolate these data to more experienced students, residents and practicing doctors. These will need to be studied separately. As evidence in the literature accumulates, more general conclusions may be possible across VR products and for a wider range of procedures and skills.
Limitations
This pilot study presents certain limitations. The small sample size, recruited from a single institution, may limit the generalizability of the results. One commercial VR product was used in this study and one procedure was evaluated. Further studies will need to assess whether these findings for chest tube insertion can be extended to other critical procedures, such as central venous catheterization and emergency airway control. In addition, resource constraints limited the pairing of participants to a single surgeon assessor for the mannequin-based simulation, increasing the risk of interrater variability during direct observation. To minimize this, the raters met in advance of the study, conducted live assessments on volunteers (not included in the study) and came to a consensus about scoring to optimize reliability. The multiple-choice questions used pre- and post-training were identical, increasing the risk of memory recall rather than knowledge acquisition, but this should not, in itself, negate any difference between groups.
Finally, a formal cost analysis was not conducted as part of this study. This was a pilot investigation with a primary focus on evaluating the educational outcomes of VR in procedural skills training, rather than a comprehensive cost-benefit analysis. The costs associated with VR, including equipment purchase, software development, and maintenance, vary widely across institutions and depend on the scale of VR adoption. As such, a detailed cost analysis was beyond the scope of this investigation. However, studies have demonstrated that VR simulation incurs lower overall costs than traditional training methods while achieving comparable or superior learning outcomes.35-37
Conclusion
Our findings demonstrate that immersive VR training improves procedural skills in medical students trained to perform chest tube insertion and is a promising technology in simulation education. A curriculum blending interactive online learning and self-directed training with immersive VR may improve learning and optimize the use of both expensive simulation resources and faculty time. Future studies should examine whether periodic VR reinforcement can increase the durability of learning and whether the findings for chest tube insertion can be extended to other procedures and learners.
Supplemental Material
Supplemental Material - Virtual Reality Training Improves Procedural Skills in Mannequin-Based Simulation in Medical Students: A Pilot Randomized Controlled Trial
Supplemental Material for Virtual Reality Training Improves Procedural Skills in Mannequin-Based Simulation in Medical Students: A Pilot Randomized Controlled Trial by Ryan M. Knobovitch, Junko Tokuno, Fabio Botelho, Howard B. Fried, Tamara E. Carver and Gerald M. Fried in Surgical Innovation.
Footnotes
Declaration of Conflicting Interests
Howard Fried is the senior director of strategic partnerships and professional affairs for Vantari VR. He coached participants in the optimal use of VR technology but did not participate in the assessments of performance.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by McGill University Faculty of Medicine and Health Sciences; Summer Research Bursary Program; Foundation of Health Care Science Institute; Research Grant.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.