
Abstract
Background
Emerging technologies are being incorporated in surgical education. The use of such technology should be supported by evidence that the technology neither distracts nor overloads the learner and is easy to use. To teach chest tube insertion, we developed an e-learning module, as part of a blended learning program delivered prior to in-person hands-on simulation. This pilot study was aimed to assess learning effectiveness of this blended learning, and cognitive load and the usability of e-learning.
Methods
The interactive e-learning module with multimedia content was created following learning design principles. In advance of the standard simulation, 13 first-year surgical residents were randomized into two groups: 7 received the e-learning module and online reading materials (e-learning group); 6 received only the online reading materials (controls). Knowledge was evaluated by pre-and post-tests; technical performance was assessed using a Global Rating Scale by blinded assessors. Cognitive load and usability were evaluated using rating scales.
Results
The e-learning group showed significant improvement from baseline in knowledge (P = .047), while controls did not (P = .500). For technical skill, 100% of residents in the e-learning group reached a predetermined proficiency level vs 60% of controls (P = .06). The addition of e-learning was associated with lower extrinsic and greater germane cognitive load (P = .04, .03, respectively). Usability was evaluated highly by all participants in e-learning group.
Conclusion
Interactive e-learning added to hands-on simulation led to improved learning and desired cognitive load and usability. This approach should be evaluated in teaching of other procedural skills.
Introduction
Chest tube insertion is a fundamental procedure for management of chest trauma and pleural diseases, and surgical trainees must master the procedure. Despite efforts to improve surgical training by adding simulation to educational courses, e.g., Advanced Trauma Life Support (ATLS), reported complication rates after chest tube insertion by residents remain high. 1 To address this gap in training, an alternative teaching strategy should be considered.
In many residency training programs, chest tube insertion is taught during a single hands-on simulation experience and residents have little or no opportunity for further practice. Optimal preparation for the in-person simulation experience and subsequent reinforcement may improve the effectiveness of simulation training. This can be conveniently provided through a blended learning approach. In this context, blended learning is a combination of asynchronous and synchronous learning: the asynchronous component can be provided by e-learning, a form of electronic and internet-based teaching, which allows trainees flexible, self-directed learning. With the e-learning, trainees can prepare for the subsequent synchronous component, in-person simulation. Although there are reports on the effectiveness of blended learning for medical education,2,3 the evidence for procedural training has not been well studied. One study demonstrated that such an asynchronous component can significantly improve trainees’ knowledge and satisfaction. 4 However, because few faculty members have been formally trained to create and use e-learning, there has been a great deal of variability in quality of these programs in surgical education. 5
The development of an online learning program should first be based on sound principles of instructional design. Effectively incorporating active learning features in education technology, such as multimedia and interactive elements, 6 has been shown to improve learning outcomes and learning experience, whereas poorly designed products or inappropriate use of technology can lead to poor learners’ satisfaction and high dropout rates.7-11 The cognitive load theory is an important consideration when developing an educational program delivered with new technology. 9 The main premise of this theory is that the capacity of our working memory and information processing for long-term memory is limited.10,11 Because learners must learn how to interact with technology, in addition to the actual learning task, cognitive load that learners experience should be assessed and managed not to exceed the individual learner’s cognitive capacities. Further, the theory posits that there are three different types of cognitive load: the intrinsic load derived from the learning task (inherent to the complexity of the task), the extraneous load caused by the way the learning task is presented or the learning situation (poor teaching and instructions, and distractions in learning environment), and the germane load of the learning process and the retention (mental schema formation for the actual learning). In the context of medical education, it is widely recommended that cognitive load theory should be integrated into medical instruction; intrinsic load should be managed according to learners’ levels, extraneous load should be reduced by avoiding irrelevant elements and complex instructions to foster generative processing.9-12
From the engineering perspective, usability is an important concept to evaluate human-computer interactions in terms of the degree of ease of use. Literature suggests that the concept of usability and cognitive load theory are correlative; poor usability can be viewed as a significant component of extraneous cognitive load. 13 The International Organization for Standardization (ISO) suggests that usability evaluations encompass effectiveness, efficiency, and satisfaction, and questionnaire for usability of blended learning was recently developed.
In this pilot study, we developed a novel blended learning program to teach chest tube insertion for junior surgery residents by combining a new interactive e-learning module with in-person mannequin simulation training. We hypothesized that residents who were prepared with the e-learning module would demonstrate greater improvement in knowledge and skill, report better cognitive load compared to residents with a traditional teaching method, and that the usability of the computer-based e-learning module will be rated highly.
Material and Methods
Experimental Design
This study was designed as an assessor-blinded randomized controlled study, conducted at the Steinberg Centre for Simulation and Interactive Learning, McGill University (Montreal, Canada). The study was approved by McGill University’s internal review board (A09-E48-21A). Hands-on simulation training is part of the standard training for first-year surgical residents from all surgical disciplines at McGill University. The program includes instructional materials for several basic surgical procedures, including suturing, anastomosis, chest tube insertion, etc. Only chest tube insertion was addressed in this study. Study participants were allocated randomly on a 1:1 ratio into two groups: e-learning and controls. One of the investigators not involved with resident training or assessment carried out the randomization method. Participants were asked to take a pre-test to assess baseline knowledge and complete a survey to provide demographics (age, gender, handedness, prior clinical exposure to chest tube insertion, prior simulation training, including ATLS course). One week before the hands-on simulation session, the e-learning module and a list of reading materials (textbook chapters)14-16 were provided to the e-learning group; the same reading materials, without the e-learning module, were given to the control group. During hands-on training, participants in both groups received guidance from an experienced instructor, blinded to group allocation. Then, participants' skill performance for chest tube insertion procedure were assessed by two blinded evaluators. Immediately after the skill assessment, all participants were asked to take a post-test to evaluate their knowledge, complete surveys for cognitive load, and provide other feedback related to their educational experience. The e-learning module, the list of reading materials, tests, and surveys were provided through the McGill University online learning management system, myCourses. All participants were familiar with its use. The Consolidated Standards of Reporting Trials (CONSORT) diagram is shown in Figure 1. CONSORT flow diagram of study recruitment.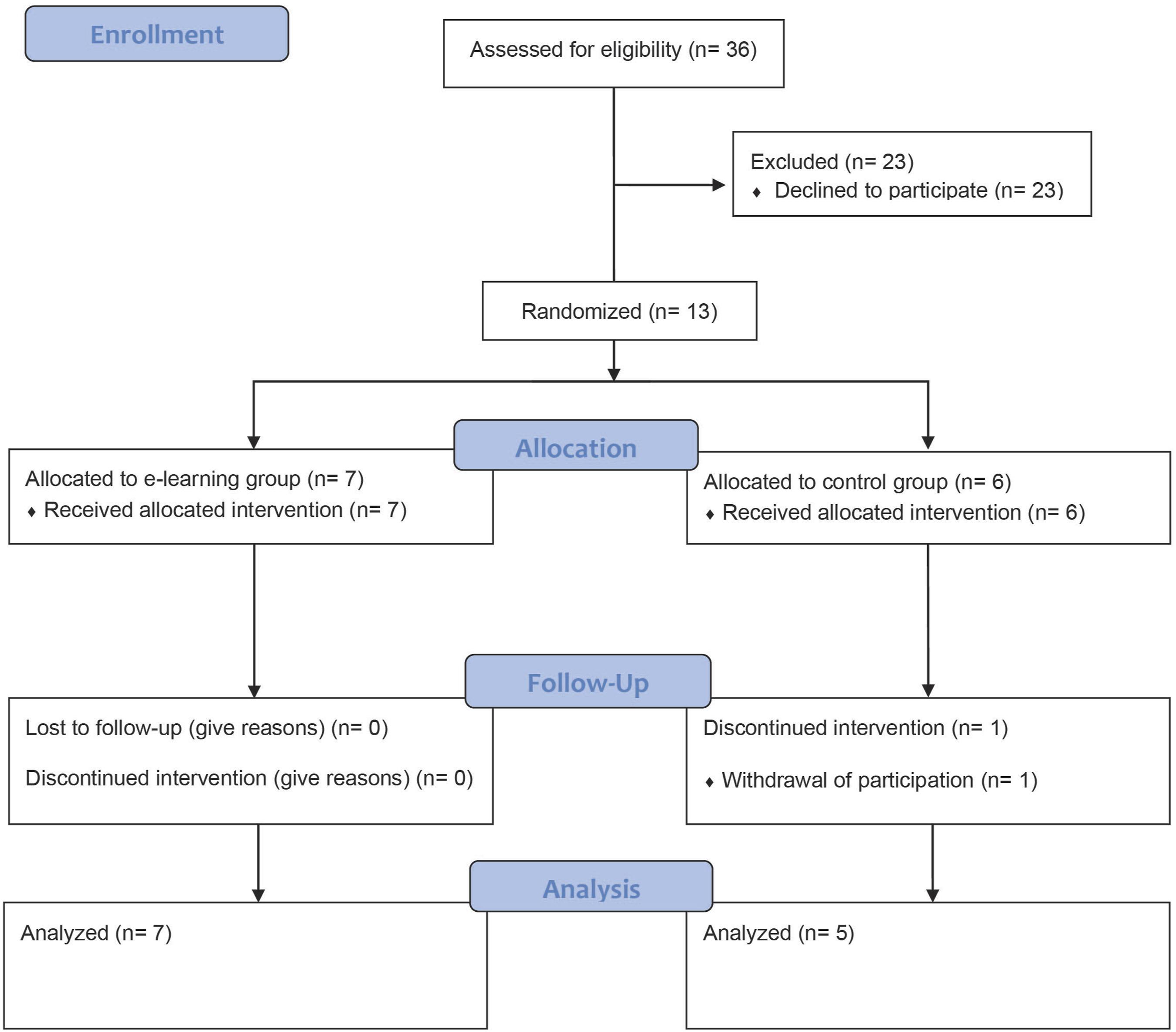
Development of E-Learning Module
We used the ADDIE (Analysis, Design, Develop, Implement, Evaluate) framework 17 under the guidance of an expert instructional designer in e-learning and education technology to design this program. In the Analysis phase, educational needs were defined by a panel of experienced surgeons to improve the skills and knowledge of chest tube insertion. For content, we included four subunits: indications and contraindications, preparation, procedure, and complications. The ATLS course guidelines were selected as the base for the content because McGill University’s Department of Surgery has been offering ATLS courses regularly and the instruction mode is familiar to study participants.
In the Design phase, specific, measurable, achievable, relevant, and time-bound learning objectives 18 were drafted. These include, the participant will be able to: (1) explain the indications/contraindications for chest tube insertion, (2) prepare the appropriate equipment for the procedure, (3) demonstrate the procedure in the simulation environment, (4) identify potential complications of the procedure.
In the Development phase, the didactic content of four subunits to cover the learning objectives was developed to achieve learner-centered learning through interactions between the module and learners. In contrast to traditional lectures, the e-module was designed to encourage learners to obtain didactic information by clicking or hovering over graphics. In addition, quizzes were included at the end of each subunit as a knowledge check. Multimedia materials, graphics, and animations were included to illustrate the physiopathology of conditions for which chest tubes are indicated, necessary equipment, etc. Additionally, a narrated video was created to show step-by-step instructions. Each subunit was designed to be completed within three to 6 minutes to allow learners to learn at their own pace (segmentation) 11 and access the module as many times as they wanted during the period prior to the simulation event. The Implementation and Evaluation phases were the main body of the study to facilitate the teaching program and evaluate learning outcomes. Details are provided in Experimental Design and Assessment.
Assessment
To assess the theoretical knowledge of the procedure, surgery and education experts created two tests (pre- and post-tests) comprised of 15-item multiple-choice questions. Questions in the pre- and post-tests were different, but the content area and difficulty level were designed to be similar.
Skill performance was assessed by two blinded to the allocation experienced surgeons not involved in the formal evaluation of residents. Assessors used a Modified Objective Structured Assessment of Technical Skills (OSATS), validated in previous studies. 19 The OSATS consists of a Global Rating Scale of 10-items, where 1 represents the poorest level of performance and 5 is considered the best performance; the items evaluate the location of the incision, subcutaneous dissection, intercostal dissection, instrument handling during dissection, digital exploration of the pleural cavity, handling of the drainage tube, insertion of the drainage tube, estimation of the intracorporeal drain length, the economy of time and movement, and degree of assistance or coaching. In addition to these items, we added one additional item related to the fixation of the tube to the skin. In total, eleven steps of the procedure were evaluated (Supplemental material). The mean scores from the two assessors were calculated, and a total score of 44 or more out of 55 was defined as proficiency level.
In addition to knowledge tests, after the simulation we asked participants to evaluate usability and cognitive load. Usability was assessed by a questionnaire composed of 6 questions for the three domains of usability: effectiveness, efficiency, and satisfaction, using a 5-point Likert scale, where 1 represents “strongly disagree” and 5 “strongly agree.” This questionnaire was developed referring to a recently developed questionnaire for evaluation of usability of blended learning. 20 Cognitive load was evaluated using Lepink’s scale, a 10-item questionnaire based on a 0-10 Likert scale, where 0 represents “not at all the case” and 10 is considered “completely the case.” The questionnaire comprised three items for intrinsic, three items for extraneous, and four items for the germane cognitive load. 21 Although the intrinsic cognitive load is generally expected to be unchanged by instruction, teaching materials with smaller extrinsic cognitive load and greater germane cognitive load are considered optimal for learning.10-12,21,22 The mean scores for each type of cognitive load were calculated and compared between groups. At the end of the post-survey, participants were asked to provide their opinion about the course materials and provide suggestions for improvement through open-ended questions.
Statistics
Quantitative data analysis was used to examine scores from knowledge tests, technical skills, and Likert scales. Numerical data are reported as median and range. Between-group comparisons of the scores for knowledge, skills, and survey questions were performed using non-parametric tests (Wilcoxon test), and scores at baseline and after intervention within subjects were compared using Wilcoxon signed rank test. Categorical data were evaluated using Pearson’s chi square test. Inter-rater reliability was assessed by intraclass correlation coefficient using Microsoft Excel 2016 (Microsoft, Corp, Redmond, WA), and other data were statistically evaluated using JMP Pro 15 (SAS Institute, Inc, Cary, NC) and P values for comparisons are reported. Descriptive analysis was used to explore residents’ attitudes towards the teaching materials.
Results
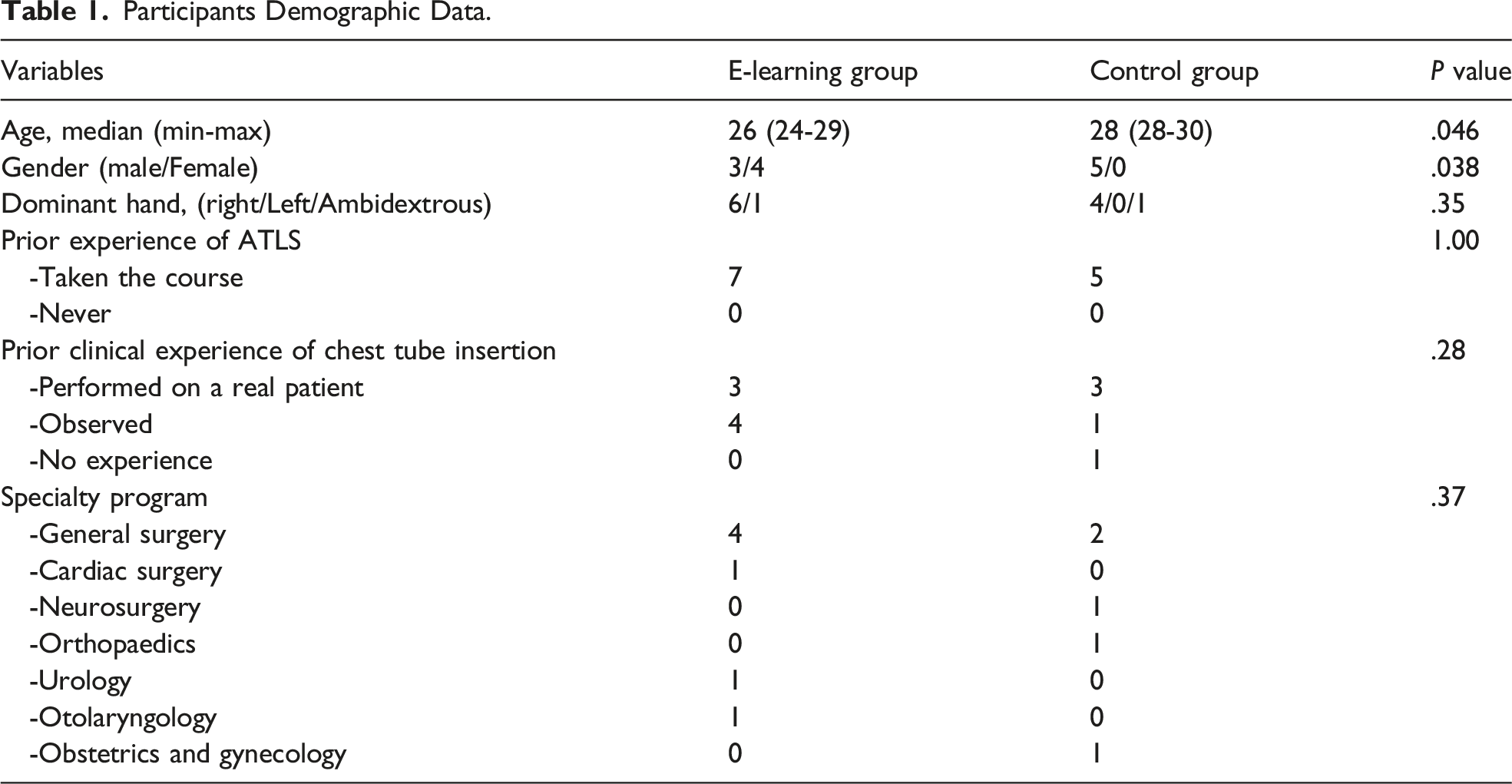
Participants Demographic Data.
Cognitive Load
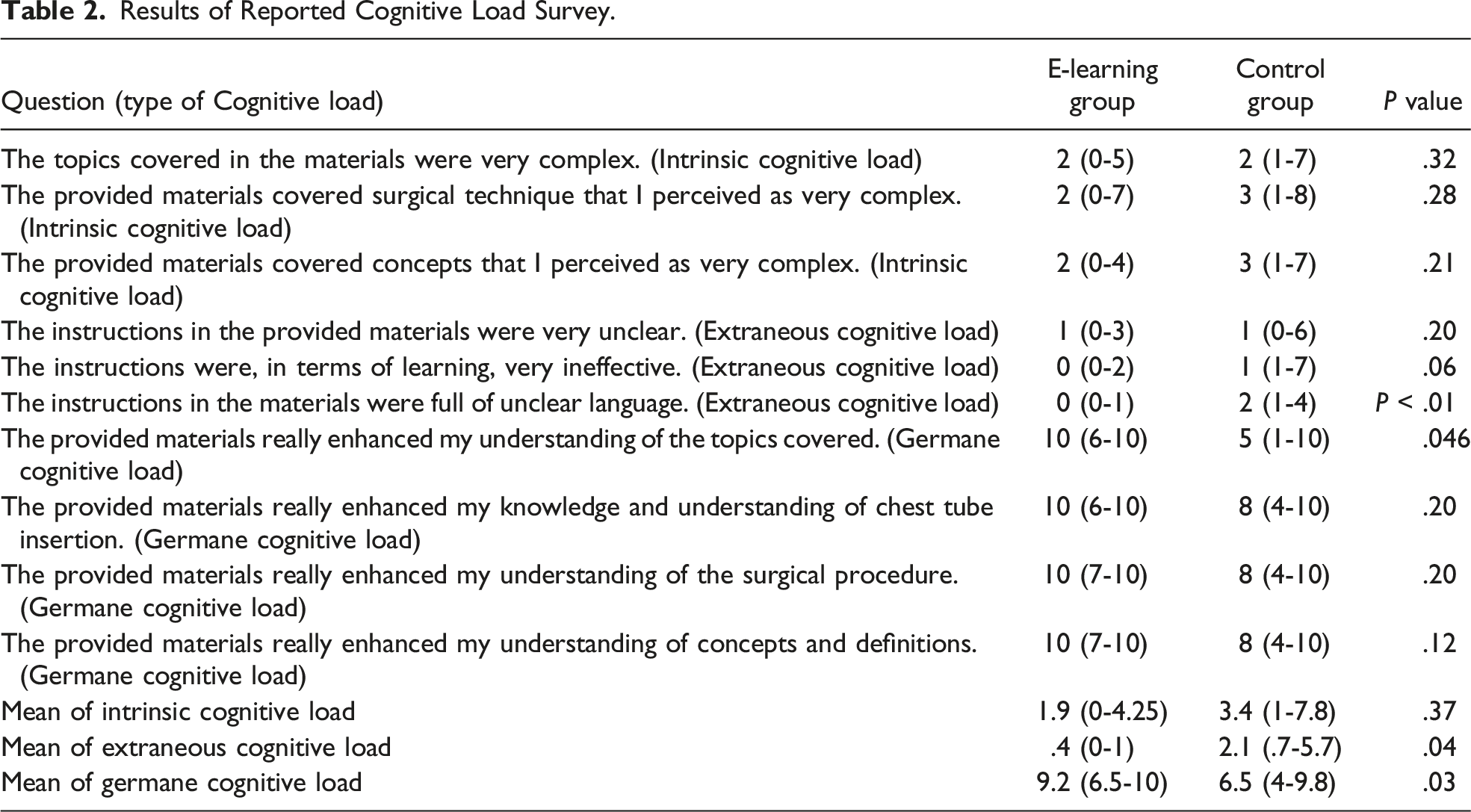
Results of Reported Cognitive Load Survey.
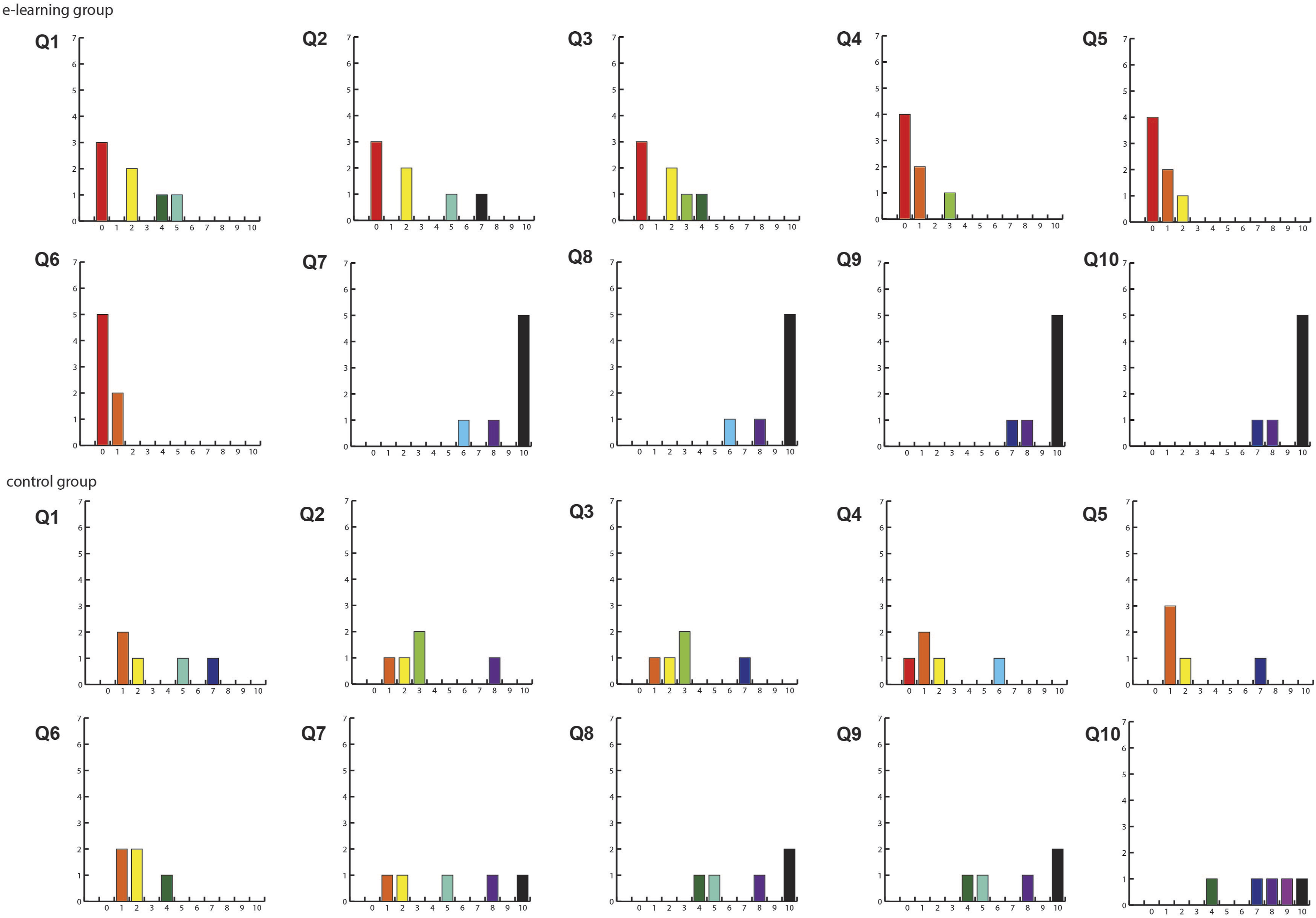
Cognitive load survey results. X axis shows value, and y axis shows 11-point Likert scale: 0 means not at all the case, and 10 means completely the case. Q1: The topics covered in the materials were very complex (Intrinsic cognitive load). Q2: The provided materials covered surgical technique that I perceived as very complex (Intrinsic cognitive load). Q3: The provided materials covered concepts that I perceived as very complex (Intrinsic cognitive load). Q4: The instructions in the provided materials were very unclear (Extraneous cognitive load). Q5: The instructions were, in terms of learning, very ineffective (Extraneous cognitive load). Q6: The instructions in the module were full of unclear language (Extraneous cognitive load). Q7: The provided materials really enhanced my understanding of the topics covered (Germane cognitive load). Q8: The provided materials really enhanced my knowledge and understanding of chest tube insertion (Germane cognitive load). Q9: The provided materials really enhanced my understanding of the surgical procedure covered (Germane cognitive load). Q10: The provided materials really enhanced my understanding of concepts and definitions (Germane cognitive load).
Usability
Results of Reported Usability From the Survey.
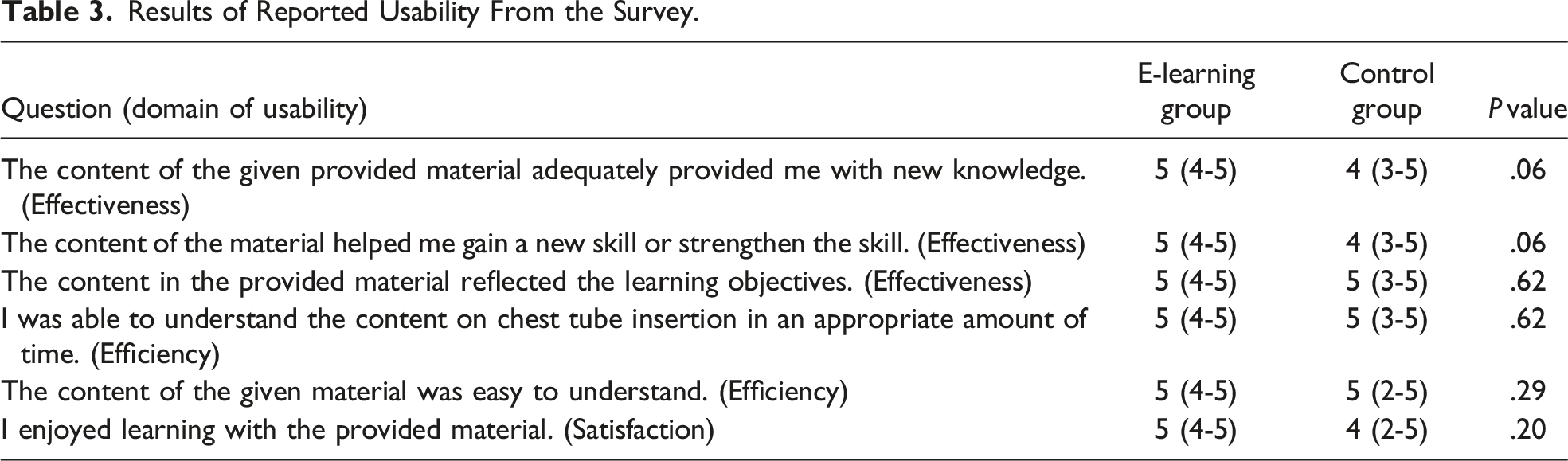
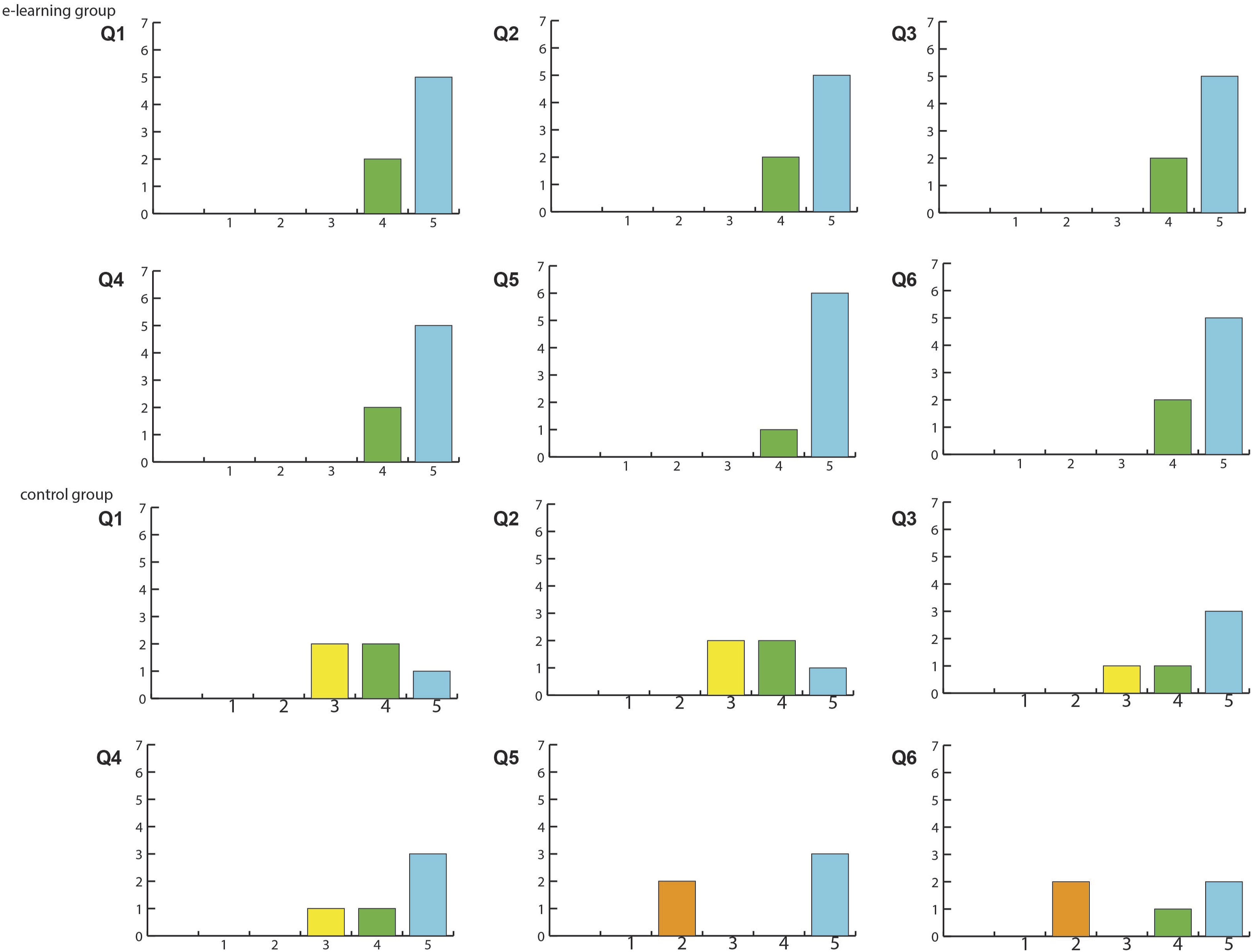
Usability survey results. X axis shows value, and y axis shows 5-point Likert scale: 1 means strongly disagree, and 5 means strongly agree. Q1: The content of the given provided material adequately provided me with new knowledge (Effectiveness). Q2: The content of the material helped me gain a new skill or strengthen the skill (Effectiveness). Q3: The content in the provided material reflected the learning objectives (Effectiveness). Q4: I was able to understand the content on chest tube insertion in an appropriate amount of time (Efficiency). Q5: The content of the given material was easy to understand (Efficiency). Q6: I enjoyed learning with the provided material (Satisfaction).
Theoretical Knowledge
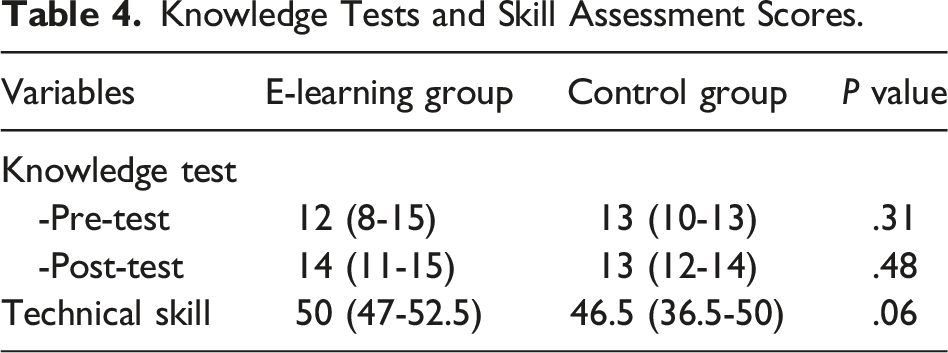
Overall, all participants showed significant improvement from pre-test to post-test (P = .008). The median score for the pre-test in the e-learning group was 12 (range: 8-15, 95% CI: 9.5-13.6) and 13 (range: 10-13, 95% CI: 10.7-14.1) in the control group; there was no difference in baseline knowledge (P = .31). The median score in post-test was 14 (range: 11-15, 95% CI: 12.1-14.7) in the e-learning group and 13 (range: 12-14, 95% CI: 12.2-14.2) in the control group, and there was no difference in post-intervention knowledge (P = .48). When the scores in two tests were compared, the e-learning group showed a slight but significant improvement (P = .047), while the control group did not (P = .500) (Figure 4, Table 4). Knowledge tests scores. Knowledge Tests and Skill Assessment Scores.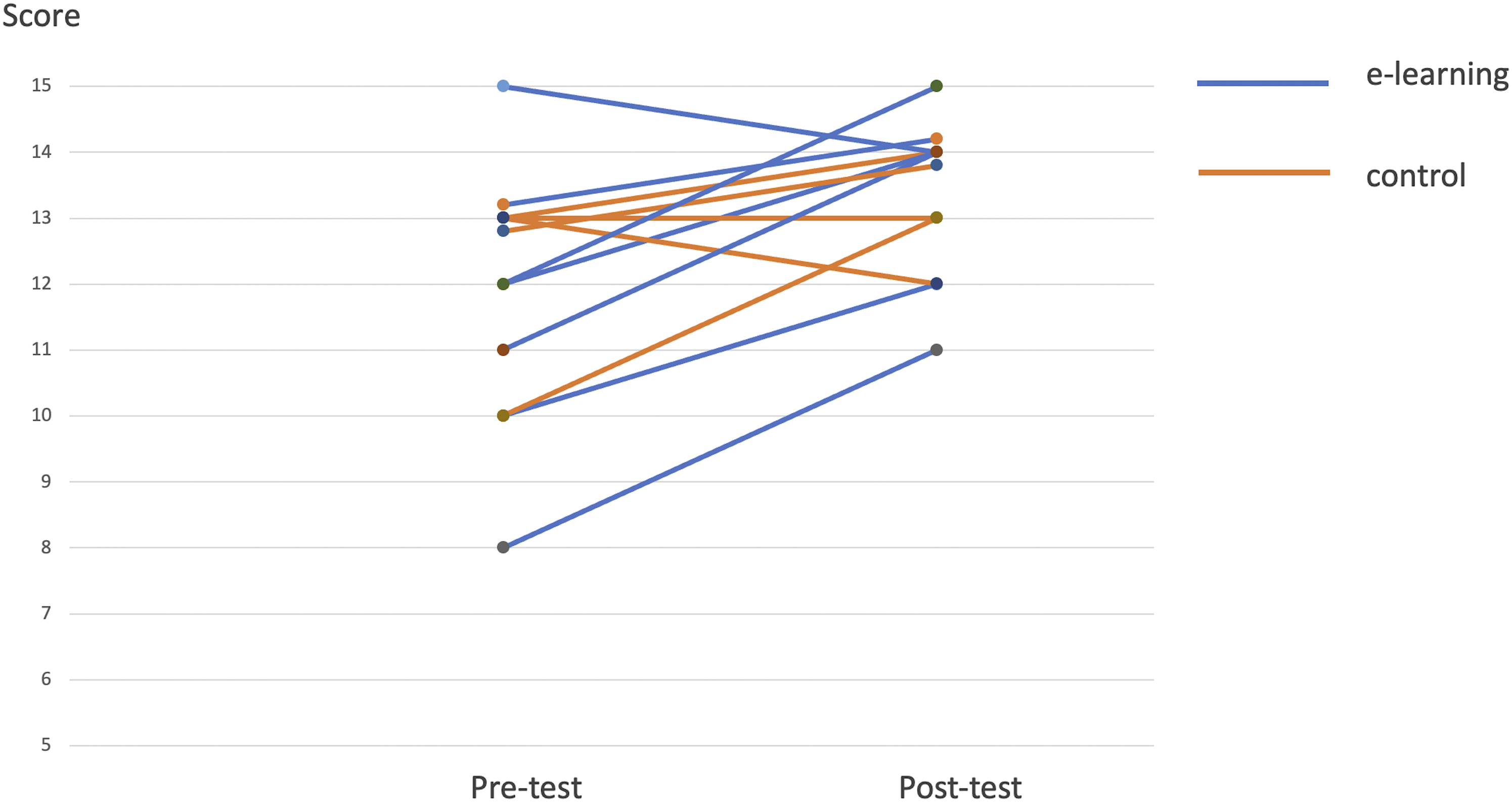
Technical Skill
The median score for technical skill performance was 50 (range: 47-52.5, 95% CI: 47.8-52.3) in the e-learning group vs 46.5 (range: 36.5-50, 95% CI: 13.2-61.4) in the control group (P = .06) (Table 4). Importantly, all residents (100%) in the e-learning group reached a proficient performance level in the technical skill assessment. In contrast, only three of five (60%) residents in the control group reached proficiency (Figure 5). Inter-rater reliability was fair at .38. Scatter plot of skill assessment scores. Score >= 44 was considered the proficiency level.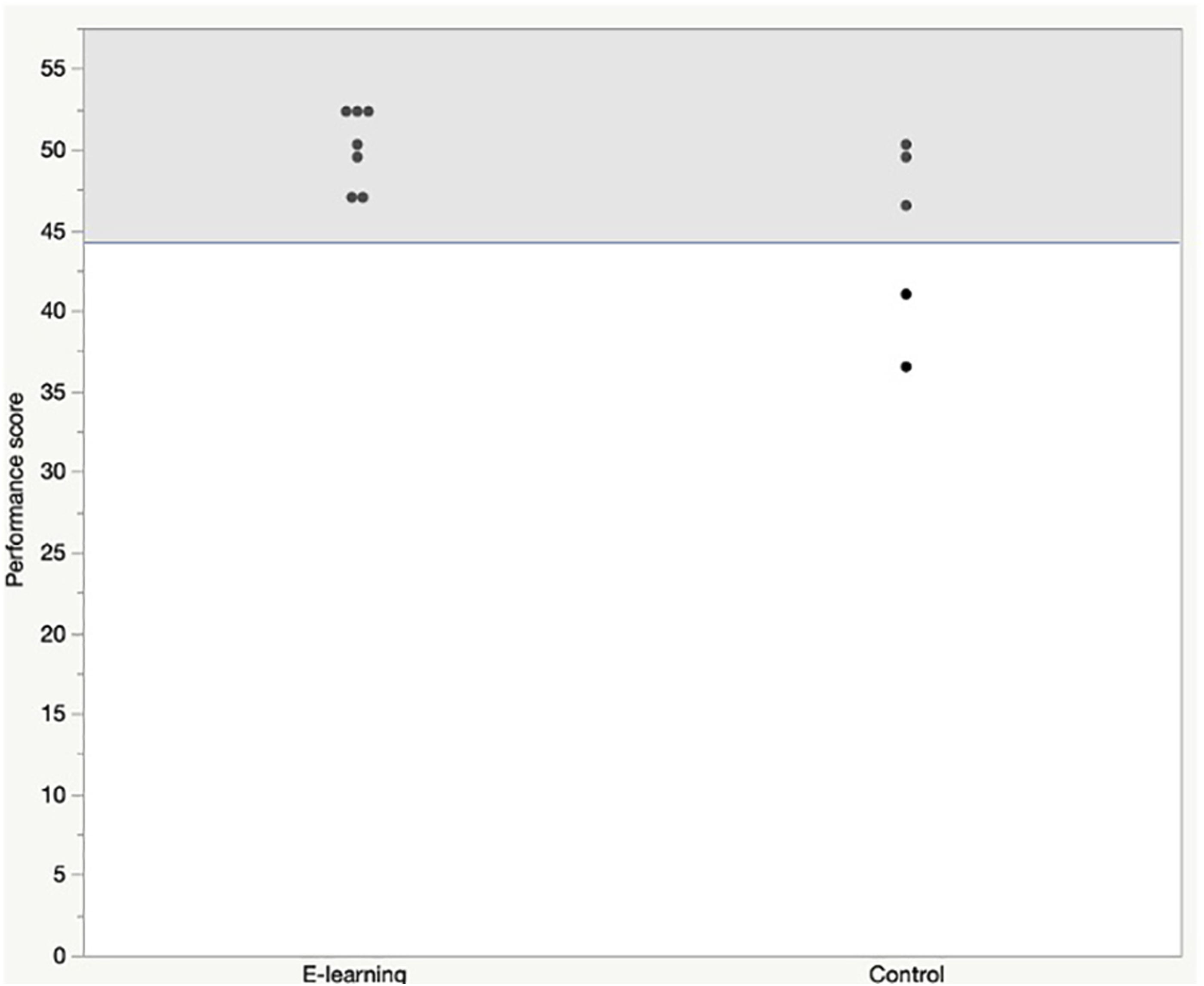
Attitudes and Feedback
Residents also provided free-text comments in the post-intervention survey. In the e-learning group, five residents (71%) liked the multimedia materials and suggested a voice-over for the didactic content and immediate quizzes as ways to improve the module. In the control group, three residents (60%) found the ATLS manual interesting because they were familiar with the material, and the graphics were good quality. Students suggested that more videos, interactive content, and reduced load would improve the educational experience.
Discussion
High complication rates for chest tube insertion have been seen even after simulation exposure and repeated procedure training has been recommended in order to reduce complications. 1 In the present study, we created and evaluated the addition of a new e-learning module aiming to optimally prepare junior surgical residents for in-person hands-on simulation training. We examined the logistics and feasibility of implementing this teaching program. In this blended learning program, the addition of newly developed e-learning module, was likely to improve residents’ knowledge and skills with optimized cognitive load and usability compared to standard reading materials only.
In surgical education, the main targeted fields are knowledge acquisition, technical skills, or non-technical skills 5 with the primary aim is to provide a safer clinical care for patients. However, it is challenging for surgical trainees to engage in training programs while occupied with clinical duties. Surgical training requires residents to acquire a large amount of knowledge and procedural expertise; this is in the context of providing clinical service that is highly demanding. For this reason, learning interventions that optimized cognitive load with high usability are more likely to engage the learner and retain learning. According to cognitive load theory, instruction information is obtained separately via visual and audio channels and processed in working memory to construct and store the schema of instruction. However, because of the limited capacity of working memory, the theory emphasizes that factors not contributing to retention should be eliminated.9-12 Also, the theory posits that instructions using multimedia are helpful for information processing by stimulating two different sensory channels. It is reported that high cognitive load may negatively influence performance in medical and surgical simulation training.23,24 In this study, data revealed consistent intrinsic cognitive load between the two groups but smaller extraneous cognitive in the e-learning group. The result of intrinsic cognitive load reflects the participants’ homogeneous backgrounds and similar baseline attitudes towards the procedure. We also assume that extraneous cognitive load was reduced by multimedia and interactive presentations of the e-learning module as best practice of established learning principles, helping the information processing. Consequently, the mitigated extraneous cognitive load induced more significant germane cognitive load resulting in improved knowledge and technical skill due to efficient self-directed learning. It also should be noted that multimedia and interactive content, which were the main features of the e-learning module, were favored among residents in the e-learning group and requested by residents in the control group, as can be seen from the open-text comments.
In addition, in the usability survey, all participants in the e-learning group evaluated the module with high scores, while the evaluation in the control group varied widely. The usability survey in the present study did not show any statistical difference between the two groups. A possible explanation of the results is that the control group received the reading assignment via the same learning managing system as the e-learning group used. In terms of human-computer interaction, using the same platform for both groups may have impacted the residents’ perception of usability. Likewise, instructional design has been partly applied by selecting reading materials to allow all residents to achieve the same learning objectives as those of the e-learning module. These similarities may have minimized the differences in perceptions of usability between the groups.
Five (42%) residents from both groups showed excellent scores (>=80%) at baseline; therefore, there may be a ceiling effect of the tests limiting the opportunity to demonstrate learning progression. However, the results suggest that blended learning with the e-learning module is likely to improve trainees’ theoretical knowledge and technical skills to exceed thresholds that are difficult to reach with only one simulation training experience. We considered that the control group also experienced blended learning delivery by combining asynchronous learning with reading materials via the same online learning management system and synchronous simulation; thus, we assume the learning in the asynchronous component of the blended learning minimized the differences in knowledge and technical skill between the two groups. The durability of the learning effects and the translation of learning to clinical performance would be important to study in the future.
To our best knowledge, this is the first pilot study to demonstrate the effects of blended learning on knowledge, technical skill, and cognitive load. However, there are some limitations to this pilot study. First, it was not powered sufficiently to show small but significant differences. Although a sample size of 30 participants (or greater) was expected based on recommendations for pilot trial design, 25 the actual sample size was smaller due to the constraints imposed due to the COVID-19 pandemic. Second, the low inter-rater reliability may have affected the ability to discriminate differences in technical performance. This could have been improved by training the raters by using pre-recorded videos of performances to align ratings. Third, we did not assess the baseline skill performance for logistical reasons. Because this study was conducted as a pilot trial to investigate the feasibility of the newly developed e-learning module, we did not intervene during the hands-on simulation for ethical reasons in the pilot study. Coaching during the simulation part was done by an experienced instructor as per previously established course guidelines of the standard program; the instructor was blinded to the learners’ study group.
Conclusion
We developed an e-learning module for chest tube insertion as preparation for hands-on simulation training. The module was highly interactive and characterized by high-quality multimedia. In this blended learning, residents who prepared with this e-learning module showed significant improvement in knowledge and reached or exceeded the proficiency level of skill performance. The module also showed optimal cognitive load, and all residents highly rated its usability. Lessons learned from this pilot study will form the basis for providing high-quality procedural training. The principles from this study can be used to inform the development of future programs with education technology in surgery.
Supplemental Material
Supplemental Material - Teaching Chest Tube Insertion by Blended Learning: A Multi-Dimensional Analysis
Supplemental Material for Teaching Chest Tube Insertion by Blended Learning: A Multi-Dimensional Analysis by Junko Tokuno, MD, MSc, PhD, Sofia Valanci-Aroesty, MD, PhD, Hayaki Uchino, MD, MSc, Gabriela Ghitulescu, MD, Christian Sirois, MD, Pepa Kaneva, MSc, Gerald M. Fried, MD, and Tamara E. Carver, PhD in Surgical Innovation.
Footnotes
Acknowledgements
The authors would like to thank Dr. Linda Snell for her helpful discussions. We are also grateful to Dr. Jason Harley, Dr. Clarissa Hin-Hei Lau, Dr. Elif Bilgic, and Mr. Byunghoon "Tony" Ahn, for the advice for study design and statistical analysis. Finally, the authors thank Mr. Jeremy Levette and Mr. Fardad Jabbary, and all members of the EdTECH Office for their assistance in the development of the module.
Author Contributions
JT: conception and design, acquisition of data, analysis/interpretation, and writing article. SVA: acquisition of data, and writing of article, HU: acquisition of data, writing of article, PK: conception and design, writing of article, GG: conception and design, writing of article, CS: acquisition of data, GMF: conception and design, analysis/interpretation, critical review of article, and final approval of the article, and TEC: conception and design, analysis/interpretation, critical review of article, and final approval of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Satoko and Richard Ingram McGill Surgical Education Scholarship.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.