
Abstract
Objective: Severe pain and other symptoms in complex regional pain syndrome (CRPS), such as allodynia and hyperalgesia, are associated with abnormal resting-state brain network activity. No studies to date have examined resting-state brain networks in CRPS patients using electroencephalography (EEG), which can clarify the temporal dynamics of brain networks. Methods: We conducted microstate analysis using resting-state EEG signals to prospectively reveal direct correlations with pain intensity in CRPS patients (n = 17). Five microstate topographies were fitted back to individual CRPS patients’ EEG data, and temporal microstate measures were subsequently calculated. Results: Our results revealed five distinct microstates, termed microstates A to E, from resting EEG data in patients with CRPS. Microstates C, D and E were significantly correlated with pain intensity before pain treatment. Particularly, microstates D and E were significantly improved together with pain alleviation after pain treatment. As microstates D and E in the present study have previously been related to attentional networks and the default mode network, improvement in these networks might be related to pain relief in CRPS patients. Conclusions: The functional alterations of these brain networks affected the pain intensity of CRPS patients. Therefore, EEG microstate analyses may be used to identify surrogate markers for pain intensity.
Keywords
Introduction
Complex regional pain syndrome (CRPS) is characterized by severe pain and other painful symptoms, such as allodynia and hyperalgesia. 1 CRPS type 1, which involves covert nerve damage, is considered one of the most common nociplastic pain diseases. 2 The identification of not only pain but also co-morbidities is essential for diagnosing nociplastic pain, and CRPS patients have been reported to have comorbidities, such as visuospatial representation impairments and affective disorders.3,4 Recent studies using functional magnetic resonance imaging (fMRI) have revealed that the pain severity of CRPS patients is associated with a maladaptive central nervous system. 1 In particular, large-scale brain network abnormalities in CRPS patients have received considerable attention,5,6,7 owing to the correlation between the activity of these networks at rest and pain intensity in CRPS patients. 8 The temporal resolution of fMRI is not always compatible with the speed of human information processing, whereas electroencephalography (EEG) can determine spatial patterns during the resting state at a significantly shorter timescale than fMRI, although the spatial resolution of EEG is lower than that of fMRI. 9 With this advantage of EEG, microstate analysis has enabled observations of large-scale brain networks during the resting state. 10 In this analysis, EEG activity is segmented into arbitrary areas of scalp electrical topographies over certain time periods (eg, 60-120 ms). The segmented topographies remain temporally stable but dynamically change into different states in which the topographies become stable again (ie, quasi-stable states). 11 These discrete epochs of topographic stability are referred to as “microstates.”. 11 Four or five specific microstates have been proposed to explain most of the global variance of EEG signals. 11 Previous studies have reported abnormalities of temporal microstate characteristics in various neuropsychiatric disorders. 11 Moreover, several studies have reported abnormalities of temporal microstate characteristics in patients with chronic low back pain, fibromyalgia, and phantom limb pain.12,13,14 For example, temporal characteristics, such as the duration of one microstate, were shown to be decreased in chronic low back pain patients. 12 However, there have not been any studies that have analyzed EEG microstates in patients with CRPS.
Therefore, we first conducted EEG microstate analysis in CRPS patients and investigated the association between the temporal measurements of EEG microstates and pain intensity. Subsequently, we investigated changes in EEG microstates after clinical treatment for CRPS.
Methods
Participants
Outpatients with CRPS were recruited from the Department of Hand Surgery, Nagoya University. Inclusion criteria were as follows: (i) males and females over 20 years of age; and (ii) fulfill the CRPS diagnostic criteria described below. Diagnostic criteria were based on the comprehensive Diagnostic Criteria for CRPS in the Japanese Population, 15 which is largely consistent with the Budapest criteria for diagnosing CRPS for international patients. 16 Patients with a clinical history of CRPS with scores of 3 or more in both objective and subjective assessments of trophic change, decreased range of motion, abnormal pain processing, sudomotor activity, and edema were included. Exclusion criteria were as follows: (i) patients lacking the capacity to give voluntary consent; (ii) patients unable to obtain written consent; (iii) patients deemed inappropriate by the physician in charge; (iv) patients with CRPS-specific dystonia causing EEG noise. Seventeen patients with CRPS (male: five patients, female: 12 patients) participated in this prospective cohort study (mean age 52 years, range 17-86 years). The cause of CRPS in the patients were as follows: two cases of incision wounds of the hand, four cases of laceration of the hand, one case of infusion in the forearm, one case of seronegative arthritis, one case of dislocation of the shoulder, one case of carpal tunnel syndrome surgery, one case of postoperative resection of subcutaneous soft tissue mass, two cases of amputation of one finger, one case of distal radius fracture, one case of triangular fibrocartilage complex injury, one case of ankle sprain, and one case of unknown etiology. The patients had already recovered from the primary (ie, underlying) cause of the CRPS when their EEGs were recorded, and therefore, musculoskeletal defects likely had no direct impact on the pain score or EEG activity. Patients received standard CRPS treatment (eg, medication, rehabilitation, and cognitive behavioral therapy). For rehabilitation, exercise-based rehabilitation was conducted in the hospital or at the patient's home. For cognitive behavioral therapy, the physician or psychologist aimed to improve the patient's negative thoughts and emotions surrounding the pain. All patients had been taking one or a combination of medications before and during treatment, such as pregabalin, pitavastatin calcium hydrate, loxoprofen sodium hydrate, salazosulfapyridine, etizolam, tramadol hydrochloride acetaminophen, duloxetine hydrochloride, celecoxib, lansoprazole, tranilast, rabeprazole sodium, estradiol, ramelteon, mecobalamin, gabapentin, teprenone, efinaconazole, fentanyl, zopiclone, ketoprofen, olopatadine hydrochloride, bepotastine besilate, and amitriptyline hydrochloride. For each CRPS patient, the physician tailored the therapy according to the comorbidities or medical history, such as high cholesterol, cataracts and mental disorder. As mentioned in limitation section, various medications and comorbidities can impact EEG findings (see Limitations section). However, we could not control the use of medications for ethical reasons. The ethics committee approved the study protocol, and written informed consent was obtained from each participant prior to participation in the study. Patients’ subjective pain intensity was assessed using the visual analogue scale (VAS), which was scored from 0 to 100 (0 = no pain; 100 = worst pain imaginable) on the same day as the EEG recordings before and after treatment. All patients underwent EEG. Thirteen patients returned for follow-up after approximately 6 months of treatment. Four patients did not consent to undergo EEG measurements for personal reasons. Figure 1 illustrates the above procedures.
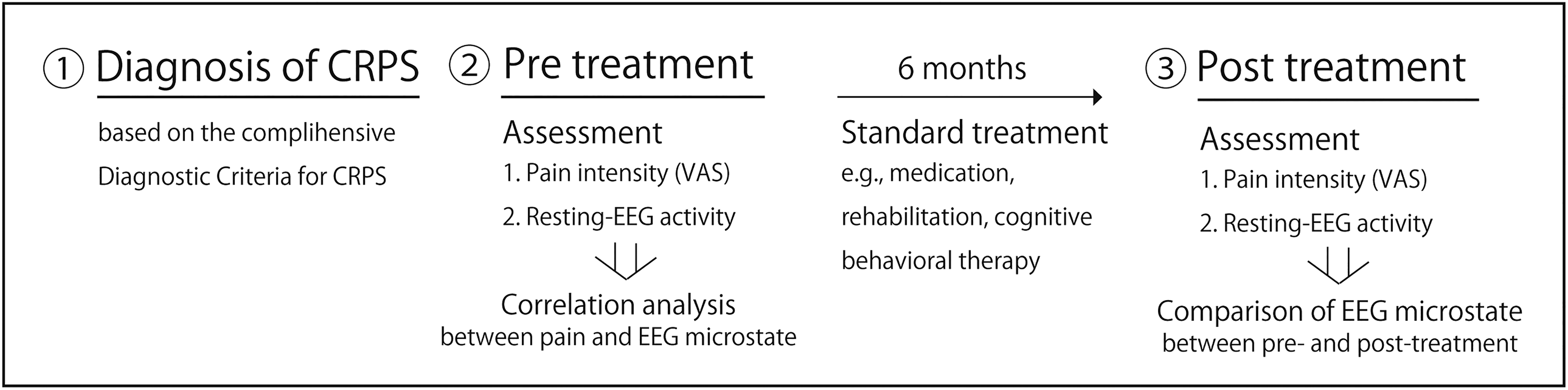
Schematic of the study procedure.
EEG Recording
Eyes-closed EEG signals were recorded for 60 s using an EEG system (Nihon Koden Co., Tokyo, Japan) after EEG waves achieved a stable state by a blinded clinical laboratory technician in a soundproof and dimly lit clinical laboratory. The EEG technician was a different person from the one who diagnosed CRPS and assessed the pain score. During the recording of EEG data, CRPS patients lay on a bed. The duration of EEG measurement was shorter than in other EEG studies to minimize patient burden because CRPS patients have severe pain. Given that each microstate lasts tens to hundreds of milliseconds,17,18 the shorter EEG measurement duration is likely not a major problem. Indeed, several previous studies performed microstate analysis using resting EEG data of less than 1 min.19,20 Data were recorded on 19 electrodes positioned according to the international 10-20 system (Fp1, Fp2, F3, F4, C3, C4, P3, P4, O1, O2, F7, F8, T3, T4, T5, T6, Fz, Cz, Pz). All EEG electrodes were referenced to the electrode placed on the earlobe. Data were sampled at a frequency of 1000 Hz.
Microstate Analysis
Microstate analysis was performed using MATLAB (MathWorks, Natick, MA) and the Microstate EEGlab toolbox [Microstate EEGlab toolbox: An introductory guide 2018]. Before conducting the microstate analysis, EEG data were band-pass filtered between 1 and 40 Hz and downsampled to 125 Hz in line with a previous study. 12 If muscle/ocular noises were detected on visual inspection, they were removed using independent component analysis (ICA). There were no electrodes that required interpolation, and none of the EEG data were excluded. The microstate analysis involved the well-established two-step clustering procedure using a modified k-means algorithm. 11
In the first step, a modified k-means method was used to generate unique clusters of EEG topographies at the individual level. The EEG topographies of each participant were clusters based on global field power (GFP) peaks given that the topographies of GFP peaks are considered discrete microstates. 22 In the second step, k-means clustering was performed at the group level using the EEG topographies of CRPS patients before treatment, where the concatenated individual topographies obtained in the first step were clustered. We then categorized the microstate topographies into five categories (A–E) (Figure 1), which were similar to those reported previously.11,12 The five CRPS-dominant microstate topographies were then fitted to each individual's EEG data before and after treatment to calculate the following temporal microstate measures: mean duration (ms), time coverage (ratio), frequency of occurrence (microstate/s), and global explained variance (GEV; ratio). Mean duration is the average time (in ms) during which a microstate persists before transitioning to a different microstate. Time coverage is the ratio of the total time that a microstate is present. Frequency of occurrence is the number of times that a microstate recurs every second. GEV is the ratio of global variance that is explained by every microstate.
Statistical Analysis
The associations between pain intensity and temporal microstate measures in 17 participants before treatment were analyzed. Generalized linear model (GLM) analysis was performed to assess the association between pain intensity and temporal microstate measures. We used the Bayesian method to enable reasonable estimation even when using a small sample size and applied Markov chain Monte Carlo (MCMC) fitting of the GLM 23 using the pain intensity and temporal microstate measures as fixed effects. MCMC is a method used to generate a sample with a distribution characteristic that matches the posterior distribution of the Markov chain using the Bayesian method and to calculate an estimated value of the objective variable. To check the modeling assumption, we used the Rhat value. A Rhat value of < 1.1 for all parameters indicates a good estimation of the model. 23 In addition, all credible intervals (CI) were provided as 95% CIs, and we tested their statistical significance. The statistical analyses were performed in R ver. 4.2.1.
For the comparison of temporal microstate measures between pre- and post-treatment, we used data from CRPS patients (N = 13) who underwent follow-up EEG recording after approximately 6 months of treatment. The Bayesian approach using MCMC was also used for the comparisons, and significance was tested using 95% CIs. Statistical analyses were performed in R, ver. 4.2.1.
Results
Microstates in Patients with CPRS
CRPS-dominant microstate topographies are shown in Figure 2. Microstate maps A and B display the left and right directions, maps C and E display the anterior-posterior directions, and map D shows the central maximum. Note that polarity (black) is ignored in the microstate analysis. 24 The sum of five microstates accounted for 63.4% of the GEV. Each temporal microstate measure (eg, mean duration (ms), time coverage (ratio)) in CRPS patients is given in Table 2.
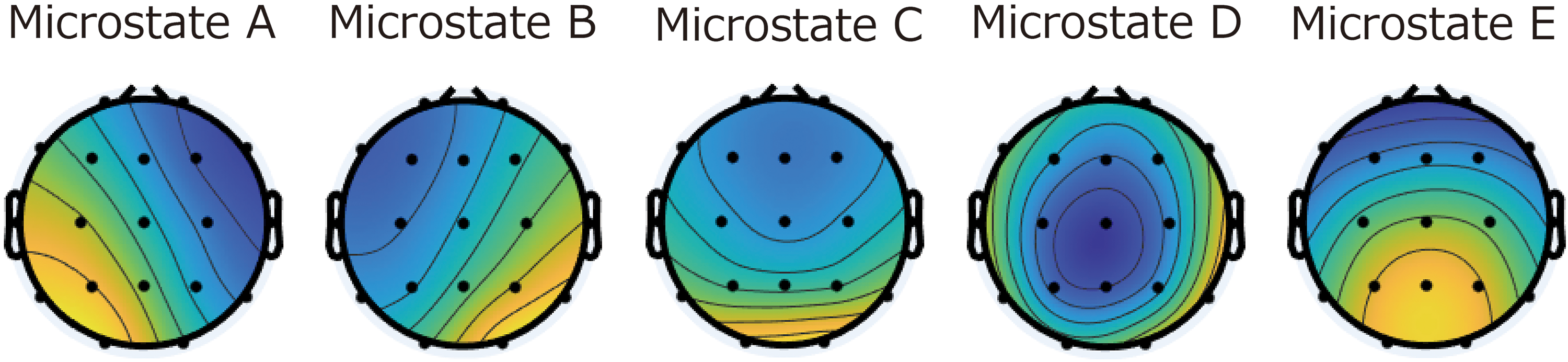
Microstate topographies five microstate topographies were defined in complex regional pain syndrome patients. Each microstate is labeled A to E.
Association Between Temporal Microstate Measures and Pain Intensity
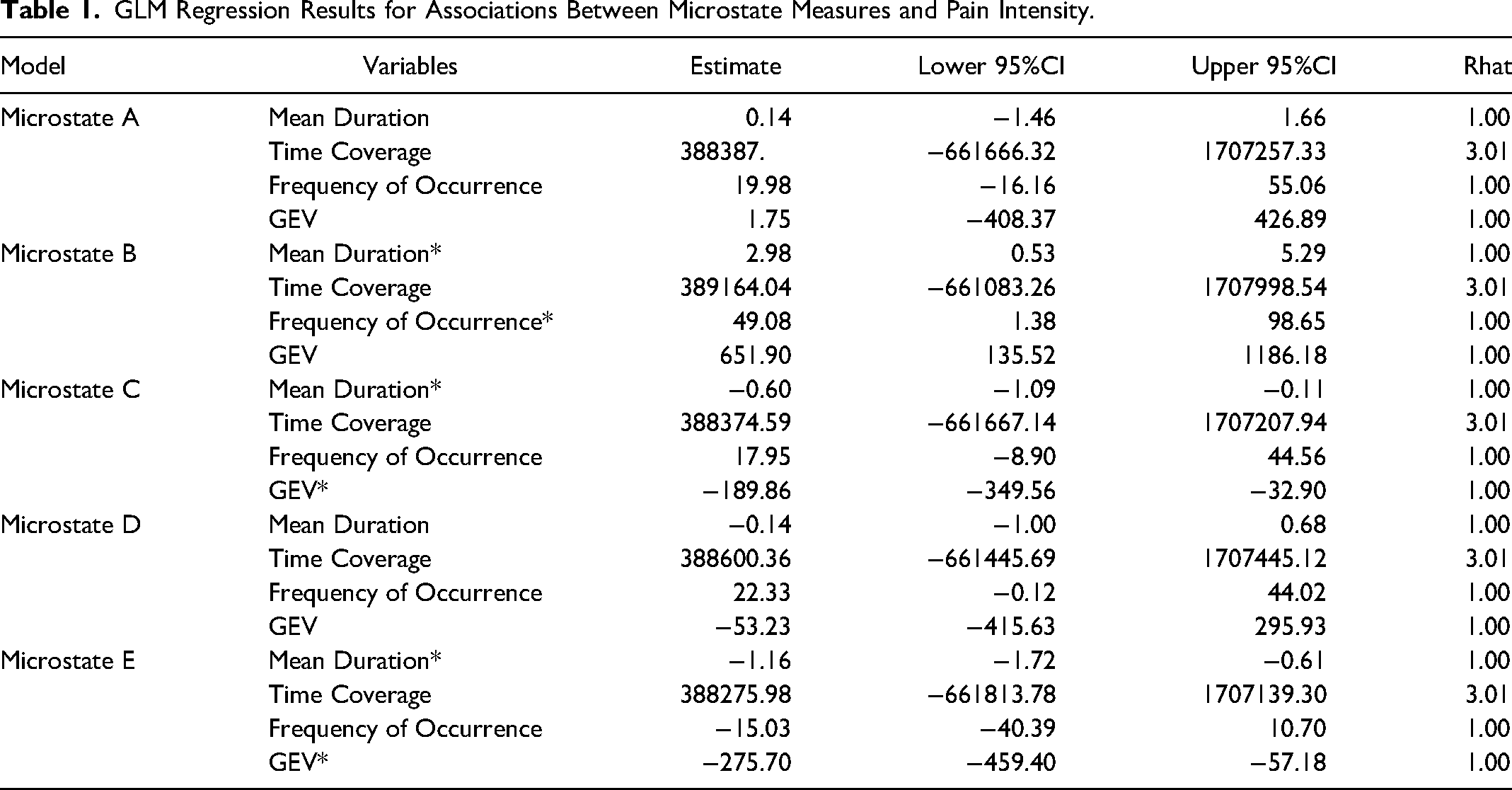
The scatter plot and results of the association analysis between microstate measures and pain intensity are shown in Figure 3 and Table 1. In the microstate B model, mean duration and frequency of occurrence were positively associated with pain intensity. In the microstate C and E models, mean duration and GEV were negatively associated with pain intensity. No significant correlations were observed between pain intensity and microstate A or D.
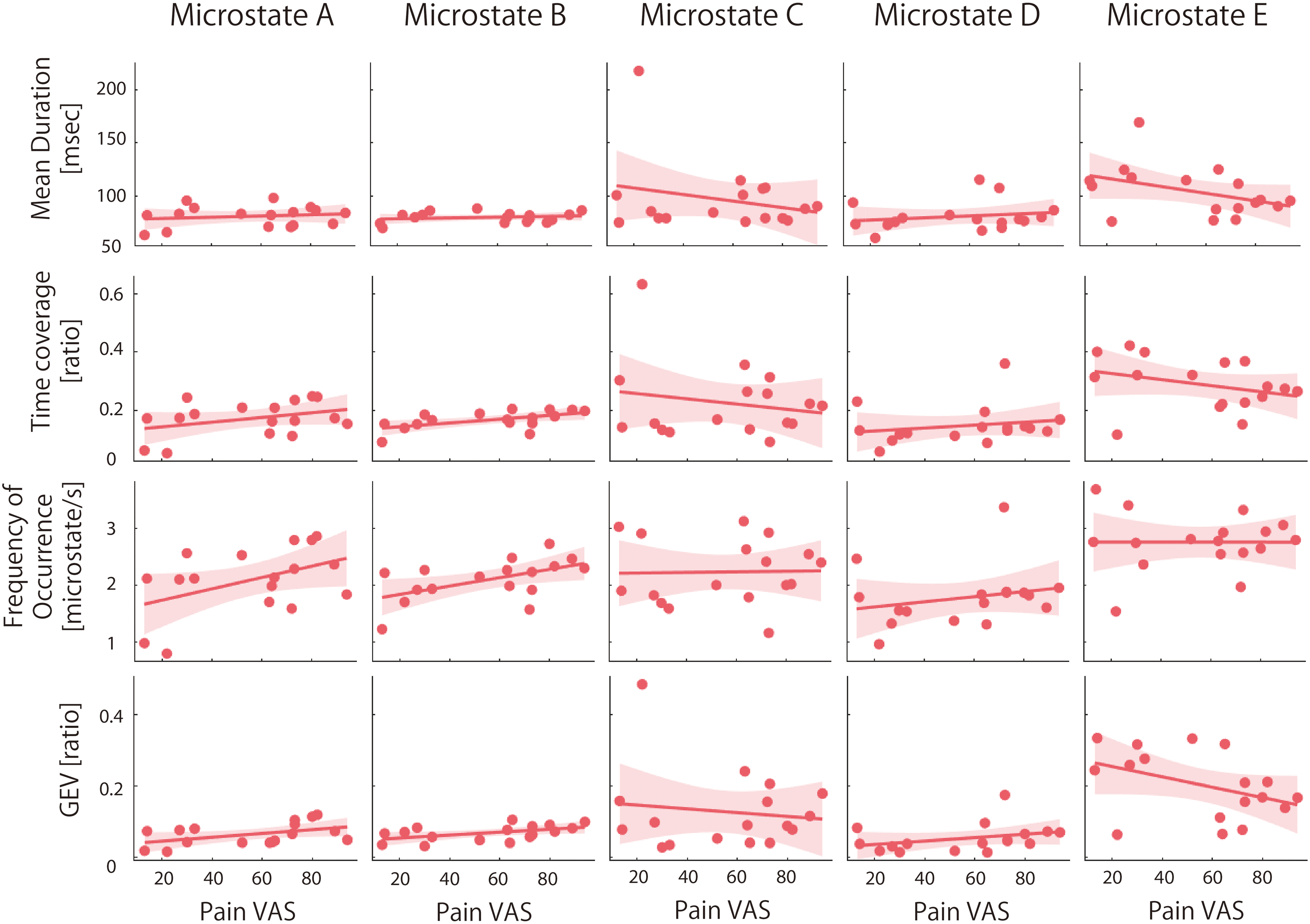
Scatter plot of each temporal microstate measure and pain intensity (visual analogue scale score) in complex regional pain syndrome patients mean duration, time coverage, frequency of occurrence, and global explained variance of each microstate were calculated as temporal microstate characteristics. Filled black indicates a significant association between temporal microstate measures and pain intensity.
GLM Regression Results for Associations Between Microstate Measures and Pain Intensity.
Comparison of Temporal Microstate Measures Between Before and After Treatment
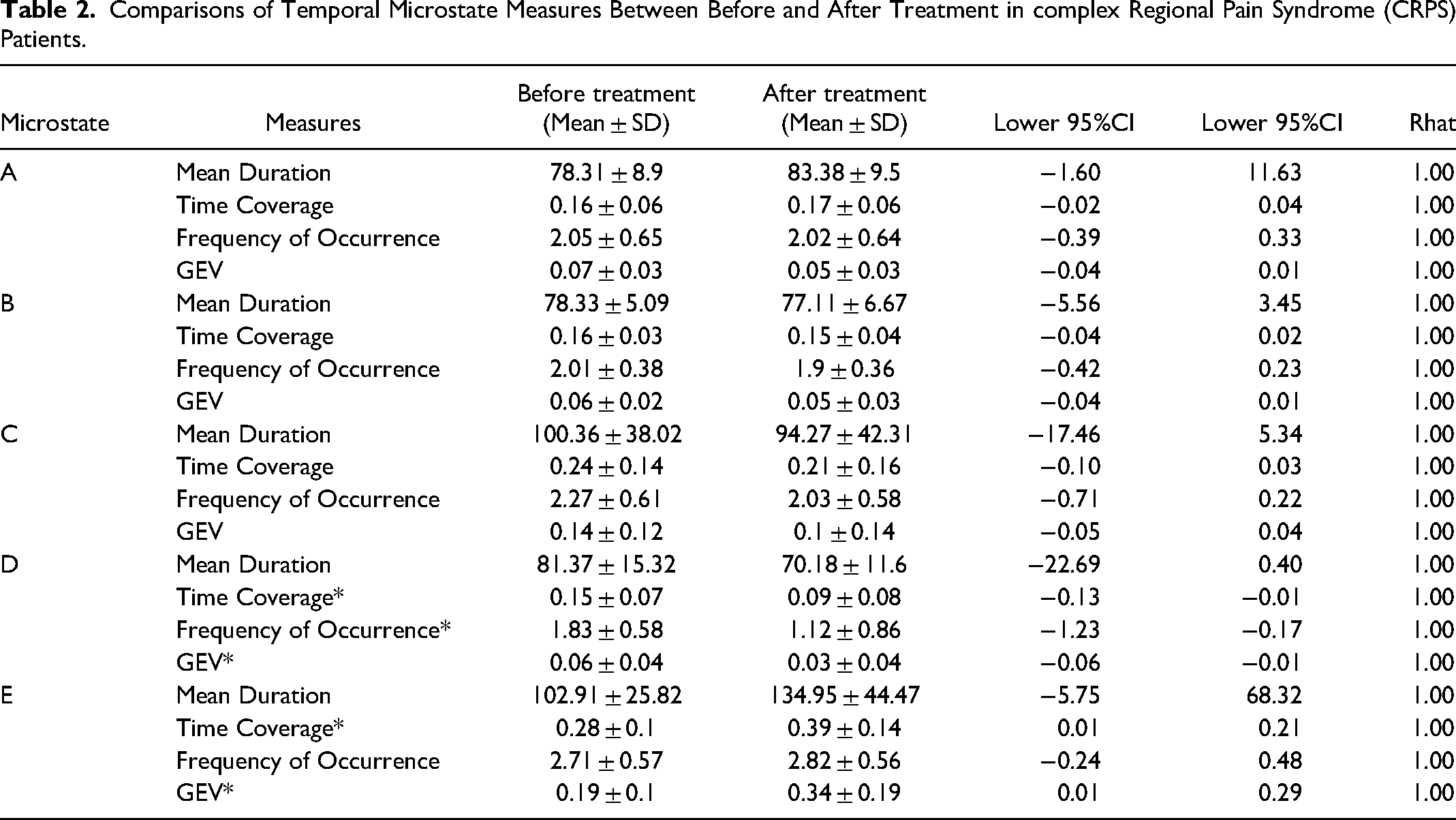
The temporal microstate measures before and after treatment in 13 CRPS patients are provided in Figure 4 and Table 2. The time coverage and GEV of microstate E significantly increased from before to after treatment. The time coverage, frequency of occurrence of the microstate, and GEV of microstate D significantly decreased from before to after treatment. The mean VAS scores before and after treatment were 51.3 ± 25.9 and 42.9 ± 9.3, respectively. The mean VAS scores before and after treatment were almost the same as in a previous study of CRPS patients. 25 Eight of the 13 CRPS patients experienced pain alleviation at the following rates: 21%–30% alleviation in three patients, 31%–40% alleviation in one patient, 41%–50% alleviation in three patients, and 51%–60% in one patient. Given that CRPS remained refractory 6 months later, 25 the treatment outcomes in the present study are reasonable. In addition, there was no serious complication of the present standard treatment. No significant changes were detected in microstates A, B, or C between before and after treatment.
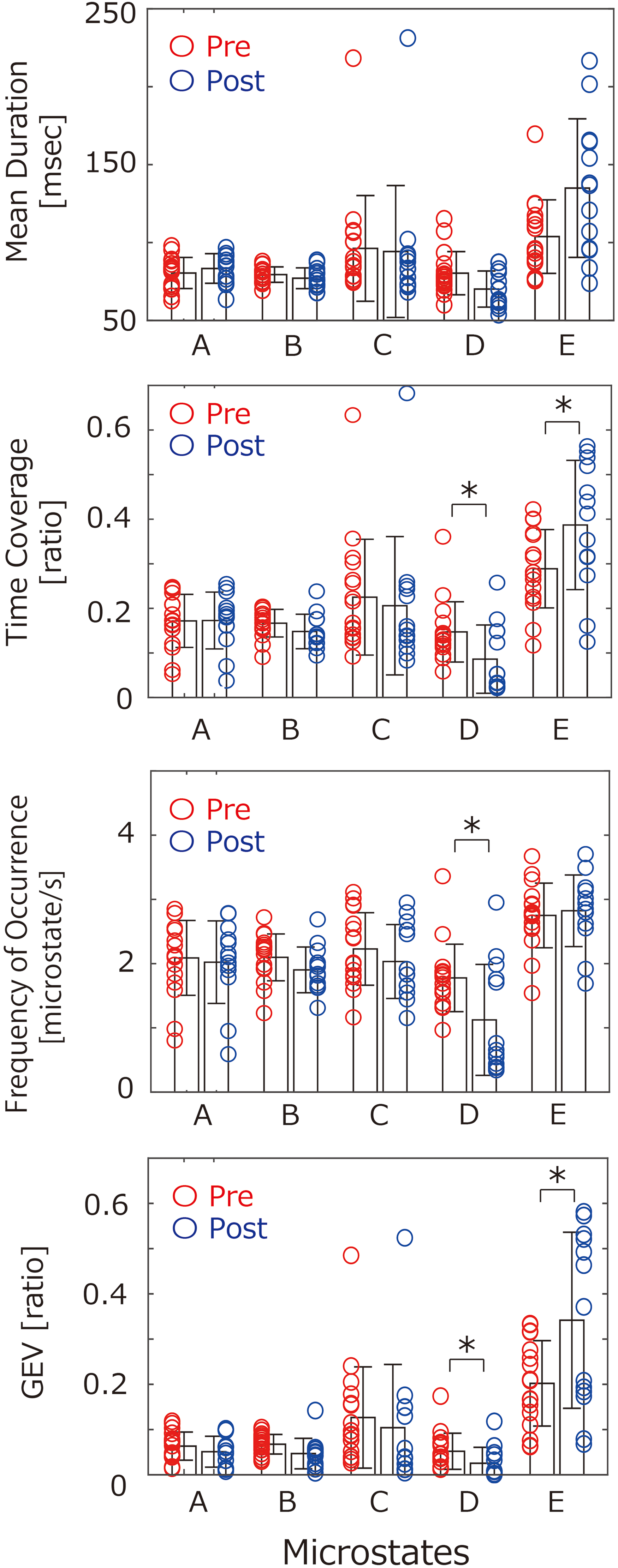
Comparisons of temporal microstate measures between pre- and post-treatment in complex regional pain syndrome (CRPS) patients dots on left side and dots on right side indicate temporal microstate measures before and after treatment, respectively, for each CRPS patient. *Significant change in temporal microstate measures from before to after treatment (p<0.05).
Comparisons of Temporal Microstate Measures Between Before and After Treatment in complex Regional Pain Syndrome (CRPS) Patients.
Discussion
The present CRPS-dominant microstate topographies were similar to those previously observed in healthy subjects and musculoskeletal pain patients,11,12 and the GEV value in the present study was similar to those reported in previous resting-state EEG studies.13,26,27 Thus, the EEG data in the present study are likely reliable. We revealed that the temporal measures of microstates B, C, and E were significantly associated with pain intensity in CRPS patients. Microstate B is thought to reflect visual networks.11,28 The visuo-spatial perception has been reported to be disturbed in CRPS patients.15,29,30 The disturbed visuospatial perception in CRPS is associated with pain severity.30−32 Furthermore, therapy for the visuospatial disturbance can alleviate pain in CRPS patients.31−33 Therefore, we possibly suggest that the association between microstate B and pain intensity reflects visuo-spatial dysfunction in CRPS patients. However, microstate B was not improved after decreasing pain intensity in the present study. It is plausible that the treatment procedure might account for this inconsistent result. In the present study, only standard analgesic treatments were prescribed for the CRPS patients, and these did not include procedures to improve visuospatial dysfunction such as adaptation to prism glasses.31,32,33 Furthermore, a previous study 32 found that the intensity of pain was not linearly correlated with the degree of visuospatial deviation. The patients witnessed an improvement in pain intensity after standard treatments, but without complete remission. Therefore, the microstate B abnormality might be sill observed after pain improvement. Future studies should investigate the ability of specific treatments to resolve microstate B and provide pain relief in CRPS patients.
Microstate C and E, both of which reflect the default-mode network (DMN), were negatively associated with pain intensity of CRPS. Microstate C indicates involvement of the posterior DMN, including the precuneus and posterior cingulate cortex, while microstate E indicates involvement of the anterior DMN, including the medial prefrontal cortex and anterior cingulate cortex. 11 The DMN is generally activated when an individual enters a relaxed, introspective self-referencing mode or is engaged with thoughts unrelated to the external world. 34 In contrast, the DMN is deactivated by emotional factors (eg, depression and anxiety). 35 A previous study reported that the deactivation of the DMN is more profound when patients with chronic back pain or CRPS report higher pain intensity.8,36 Interestingly, the microstate E was increased alongside pain alleviation following treatment in the present study. Considering these, improvement of anterior DMN activity would be associated with pain alleviation. Indeed, the functional connectivity between the anterior DMN and the descending pain modulatory system can modulate pain by suppressing nociceptive signals ascending through the spinal cord and brainstem toward the brain.37,38 Our current findings are in line with a previous report that found that the normalization of the anterior DMN enhances antinociceptive signaling, thereby alleviating pain. 37 EEG temporal dynamic studies show that microstate D, which is considered to reflect activity of the attention network, is decreased in tandem with pain reduction following treatment. Studies on the relationship between attention and subjective pain experiences show that centering attention on pain increases its intensity. 39 A human brain imaging study revealed that pain-evoked brain activity in several cortical areas is increased when the subject focuses attention on the pain, compared with when the subject is distracted from the pain. 40 When the subject's attention is maintained on pain, the DMN is reportedly deactivated. 41 These observations suggest that a reduction in the activity of the attention network after pain alleviation may indicate a state in which the patient is no longer allocating excessive attention to the pain and has entered a relaxed introspective mode. This state might be associated with an increase in microstate E and a decrease in microstate D following pain improvement. For microstate A, notable outcomes were absent by both correlation analysis and comparative analysis. Microstate A is thought to reflect activity of auditory networks. 11 Aberrant microstate A has been documented in patients with schizophrenia 42 and panic disorder 43 who suffer from auditory sensory disturbances such as hallucinations. Given that the cohort of CRPS patients in this study did not present auditory sensory dysfunctions, an association of microstate A with pain intensity or alleviation of pain was not observed.
Limitation
First, although the Bayesian approach enables stable estimations even when using a small sample size, 44 further studies in a larger sample of CRPS patients are necessary to confirm our conclusions. CRPS is a rare disease, and patients are difficult to recruit; thus, data should be acquired via international collaboration. Second, we cannot deny completely the effect of difference in administered drugs on EEG data. Several antipsychotic medications45,46 and mental disorders47,48 can affect EEG microstates. For example, antipsychotic medications reportedly affect temporal microstate measures and spatial distribution of EEG topographies. 46 In the present study, although pharmacological interventions were not controlled for ethical reasons, the impact of medications on EEG microstates might be minimal because the CRPS patients did not have severe mental disorders (such as schizophrenia or panic disorder), as reported in previous studies, as well as the lack of pharmacological treatment for these conditions. Third, there has been only one study measured by both EEG and fMRI simultaneously, 27 which revealed associations between microstates and brain networks. The functional significance of each microstate is still a debatable issue, but several lines of previous studies49,50 investigating the computed brain network of each EEG microstate data demonstrated almost consistent results from recorded brain networks by fMRI. 27 Based on the present limited understanding of the microstates, our present findings should be interpreted as informative, but not definitive. Fourth, we could not control the treatment methods or medication because of ethical considerations. However, with a sufficient sample size, subgroup analysis by treatment method would be possible. Fifth, the duration of EEG acquisition was shorter than that of other EEG studies to minimize patient burden because CRPS patients have severe pain. Recording EEG for longer may provide more reliable results. Finally, we did not evaluate other components such as neuropathic pain and central sensitization in detail using questionnaires, quantitative sensory testing (QST) or electrophysiologic testing. Future studies should therefore address their role in CRPS.
Conclusion
Our EEG data revealed that several temporal microstate measures were associated with pain intensity in CRPS patients. Specifically, improvements in microstates D and E showed a link with pain via the alleviation of CRPS. Microstate analysis of EEG data, which is suitable for use in clinical settings, may offer surrogate markers for pain intensity in CRPS patients.
Footnotes
Acknowledgments
Author Contribution
Michihiro Osumi: Data analysis, Manuscript writing and Interpretation of data. Masahiko Sumitani: Manuscript writing and Interpretation of data. Katsuyuki Iwatsuki: Concept or design of the work and Data acquisition. Minoru Hoshiyama: Concept or design of the work and Data acquisition. Ryota Imai: Data analysis. Shu Morioka: Interpretation of data. Hitoshi Hirata: Concept or design of the work, Data acquisition and Interpretation of data. All authors satisfy the following. (i) Made a substantial contribution to the concept or design of the work; or acquisition, analysis or interpretation of data, (ii) Drafted the article or revised it critically for important intellectual content, (iii) Approved the version to be published, (iv) Each author should have participated sufficiently in the work to take public responsibility for appropriate portions of the content.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval Statement
The study was approved by the Ethics Committee of the Nagoya University Graduate School of Medicine and was conducted in accordance with the Declaration of Helsinki
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Japan Agency for Medical Research and Development (AMED) (grant number 17ek0610009h0003).