
Abstract
Background and Aim:
Unilateral spatial neglect (UN) impairs patients’ ability to detect and respond to stimuli on the contralesional side, severely limiting functional recovery after right-hemispheric stroke. Neck muscle vibration (NMV) has been shown to be a bottom-up, proprioceptive intervention to modulate spatial neglect. Although preliminary studies found promising effects, the isolated efficacy of NMV for neglect rehabilitation has not yet been tested in a randomized, blinded controlled trial. This study aimed to evaluate whether NMV alone improves neglect symptoms and activities of daily living (ADL).
Methods:
Twenty patients with right-hemispheric stroke and UN were randomly assigned to receive either active or placebo NMV (combined, but not simultaneously with computer-based training) over 2 weeks (5 sessions/week, 20 minutes/day). In the computer training, the placebo NMV group completed neglect-specific modules (standard neglect therapy [SNT], e.g., visual exploration training), while the active NMV group performed only general cognitive tasks unrelated to neglect. This allowed the isolated effect of NMV to be examined. Assessments included standard neglect diagnostics (e.g., Letter Cancellation), the Free Exploration Test (FET), and 2 ADL-based measures (NET, CBS), conducted before, immediately after, and (NMV group only) 1 month post-treatment.
Results:
The active NMV group showed significant improvements in 3 of 4 standard neglect tests, exploration behavior (FET), and ADL performance, with effects remaining stable at 1-month follow-up. The SNT group with placebo NMV showed comparable gains in ADL outcomes but improved in 1 standard neglect test only. Between-group analyses revealed no statistically significant differences, suggesting similar efficacy of both interventions.
Conclusion:
NMV alone yields clinically meaningful and lasting improvements in neglect symptoms and ADL, comparable to SNT. Its passive nature makes it a promising tool, particularly for early rehabilitation.
Keywords
Introduction
Unilateral spatial neglect (UN) is a neurological disorder that typically occurs following right-hemispheric brain damage. It is estimated to affect approximately 30% of stroke patients. 1 The underlying lesions usually involve regions of the perisylvian network, which plays a crucial role in spatial orientation in the right hemisphere. 2 Damage to this network in patients with UN manifests as a strong continuing rightward orientation combined with neglect of the left side. These symptoms are associated with more severe motor deficits and delayed rehabilitation, 3 ultimately reducing patients’ ability to perform activities of daily living and negatively impacting their quality of life in the long term.4,5
There are 3 main therapeutic approaches for treating UN: top-down interventions, which focus on cognitive control of exploratory behavior; neuromodulatory techniques, which aim to inhibit or activate specific cortical networks; and bottom-up interventions, which use sensory stimulation to modulate altered spatial representation.6 -8 Bottom-up approaches have the advantage of being largely independent of any cognitive and attentional deficits associated with spatial neglect 7 and do not require the patients to have insight into their condition in order to consciously cooperate.6,8
Neck muscle vibration (NMV) is a bottom-up intervention that was extensively studied in the 1990s and early 2000s.9,10 Research has shown that left-sided NMV can modulate spatial representation in both healthy individuals and patients with UN. The effects of NMV result from the stimulation of muscle spindle afferents, which are thought to induce a reorganization of egocentric spatial reference systems in the brain, typically in the direction contralateral to the site of vibration.11 -14 Specifically, studies have demonstrated a significant expansion of the explored visual space toward the contralesional side following left-sided NMV 15 combined with a leftward shift in the perceived straight-ahead (SSA) orientation.12,16 This shift facilitates improved perception and exploration of the neglected space. These effects cannot be explained solely by a general increase in arousal, as other forms of sensory stimulation, such as electrical stimulation, do not produce comparable results.17,18
Previous studies have evaluated NMV in repeated application scenarios.14,19 -21 Johannsen et al 19 examined 6 patients with neglect and found that a 20-minute daily NMV intervention over 2 weeks led to long-lasting symptom improvements, detectable up to 1.4 years after treatment. Kamada et al 20 investigated 11 patients and reported that just 5 minutes of NMV before occupational therapy sessions over 2 weeks resulted in significant and stable improvements, persisting for up to 2 weeks post-treatment. The combination of neck muscle vibration and voluntary arm movements has also been tested successfully—but so far only in a single case. 21 Schindler et al. 14 conducted a crossover study with 20 neglect patients to compare active exploration training with simultaneous NMV against exploration training alone. Both interventions consisted of 15 sessions of 45 minutes each. The combined treatment led to significant and sustained improvements lasting up to 2 months, with visible benefits in activities of daily living.
Despite these promising findings, no randomized controlled trial (RCT) has yet been conducted to evaluate the isolated efficacy of NMV. Previous studies either lacked a control group or combined NMV with other therapeutic approaches to treat spatial neglect, making it difficult to determine the specific effects of NVM. This gap in evidence will be addressed by the present study, which, for the first time, investigates the standalone effectiveness of NMV on neglect symptoms in a randomized, controlled, and blinded study design.
Materials and Methods
The study was preregistered in the WHO-approved public trial registry “German Clinical Trials Register” (DRKS-ID: DRKS00032376).
Participants
Twenty consecutively admitted patients with right-sided stroke and spatial neglect participated after the exclusion of 5 patients, 1 who was transferred to another hospital and 4 because of spontaneous remission after 1 week. A priori sample size estimation is described in the Supplemental Material. Patients were recruited from 2 different rehabilitation facilities (Schmieder-Klinik, Stuttgart-Gerlingen, Germany [n = 17 patients], Neurological Rehabilitation Center Quellenhof, Sana Kliniken AG, Bad Wildbad, Germany [n = 3 patients]) and were randomly assigned to 2 groups (n = 10 each) who received either active NMV or placebo NMV (combined, but not simultaneously with computer-based training). In the computer-based training, the placebo NVM group completed neglect-specific modules (standard neglect therapy [SNT] with, e.g., visual exploration training etc.), while the active NMV group performed only general cognitive tasks, not related to spatial neglect (see below). Simple randomization was performed using a time criterion 22 : the first 10 patients admitted to any of the 2 participating rehabilitation facilities were assigned to the active NMV group and the next 10 patients admitted to any of the 2 rehabilitation facilities to the SNT with placebo NMV group. Demographic and clinical details are given in Table 1. Structural imaging was acquired by computed tomography as part of the clinical routine procedure carried out for all stroke patients in the acute phase at stroke-onset. Patients with tumors or patients in whom scans did not reveal any clear lesions were not included. All participants gave their informed consent to participate in the study, which was conducted in accordance with the ethical standards of the 1964 Declaration of Helsinki.
Demographic and Clinical Data of all 20 Right Brain Damaged Neglect Patients.
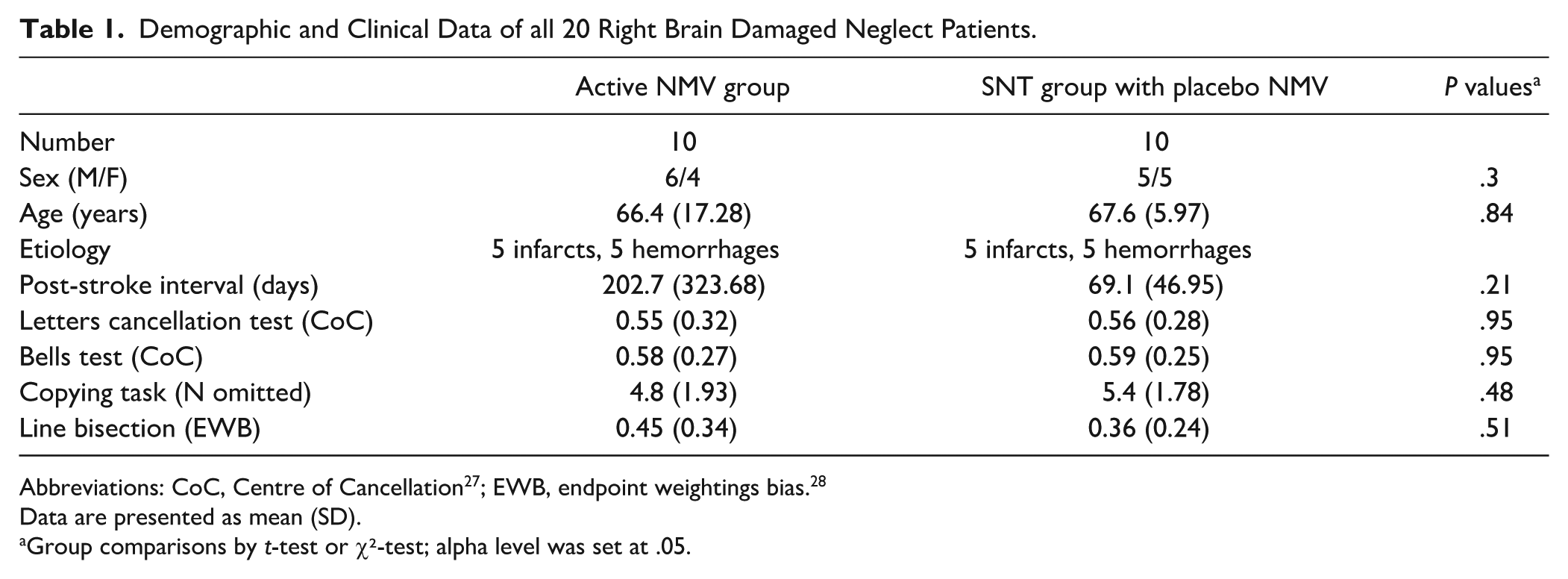
Data are presented as mean (SD).
Group comparisons by t-test or χ²-test; alpha level was set at .05.
The inclusion criterion for this study was the presence of spatial neglect as a result of brain damage caused by right hemispheric stroke. In addition to clinical behavioral observations, diagnostic criteria had to be met in at least 2 of the following 4 neglect tests: The Letter Cancellation Test, 23 the Bells Test, 24 a Copying Task, 25 and a Line Bisection Task. 26 All 4 neglect tests were performed on a Samsung S7+ tablet with screen dimensions 285 × 185 mm. The severity of spatial neglect in the cancellation tasks was determined by calculating the center of gravity of the target stimuli marked in the search fields, that is, the Center of Cancellation (CoC 27 ; A CoC value ≥ 0.08 indicated left-sided spatial neglect. 27 The Copying Task consisted of a complex scene consisting of 4 objects (fence, car, house, tree), points were assigned based on missing details or whole objects. One point was given for a missing detail, 2 for a whole object. The maximum number of points is therefore 8. A score higher than 1 (i.e., >12.5% omissions) indicated spatial neglect. 25 In the Line Bisection Task, 26 patients were presented with 4 different line lengths 8 times each, that is, 32 lines in total. The cut-off value for spatial neglect was defined as an “endpoint weightings bias (EWB)” value ≥ 0.07. 28
Procedure
Intervention
Both groups, the active NMV group and the SNT group with placebo NMV, received daily 20-minute vibration sessions over a period of 2 weeks (5 sessions per week). The vibration was applied using a handheld device (NOVAFON®, version: Novafon Power 2) equipped with a flat disk (diameter: 2.8 cm), which was placed on the left posterior neck muscles (Figure 1A). The active NMV group received vibration at 100 Hz with an amplitude of 2.8 mm, whereas the placebo NMV group received an ineffective vibration with an amplitude of <0.09 mm, applied at the same neck region (Figure 1A). To ensure blinding, the placebo device was identical in appearance to the active device. The vibration of the placebo device was rendered ineffective by reducing the amplitude, thus making these oscillations barely perceptible at the skin surface and therefore unlikely to produce passive transmission effects to the underlying musculature. This allowed a comparable humming sound to be maintained and provided mild sensory stimulation, ensuring that participants perceived a similar experience in both groups. The participating patients were not informed about which group (active or placebo NMV) they were assigned to.
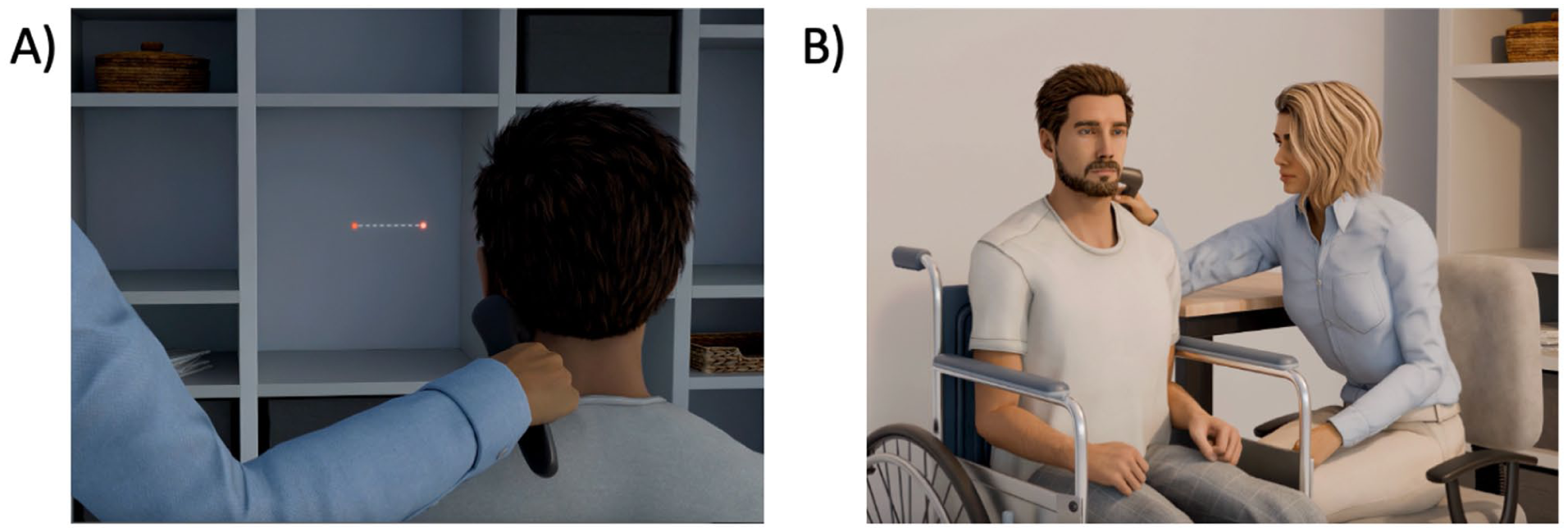
(A) Determination of the correct vibrator position in the active NMV group. The optimal position was identified as the location where the patient experienced—in dimmed lighting—the strongest illusion of a horizontal displacement of a centrally presented stationary red light toward the right side. (B) Setup for vibration of left posterior neck muscles in both the active NMV group as well the placebo NMV group during the treatment sessions.
In all patients, the vibrator was positioned within a palpable depression in the left dorsolateral neck region. Based on anatomical orientation, this site corresponds to the upper part of the so-called “posterior triangle of the neck,” that is, the area of the depression between the left sternocleidomastoid muscle and the upper, descending part of the left trapezius muscle. In the active NMV group, exact positioning of the vibration device within that region was further individually adjusted to maximize the vibration-induced shift in the perceived body midline. To determine the optimal placement, adjustments were made in dimmed lighting until the subject experienced the strongest illusion of a rightward horizontal displacement of a centrally presented stationary red light (cf. Figure 1A). Of the ten patients in the active NMV group, 5 reported experiencing such a kinesthetic illusion of the centrally presented light stimulus. Once the ideal location was identified, it was marked with a permanent marker to ensure consistent placement during subsequent treatment sessions, which were conducted under normal lighting conditions (cf. Figure 1B).
In addition, both groups (active and placebo NMV) received standard computer-based cognitive training of the respective rehabilitation institution, as part of the neuropsychological rehabilitation program. This consisted in both facilities of 5 training sessions per week, each session lasted about 25 minutes. The experimental NMV group received this training without any neglect-specific modules, while this training in the placebo NMV group included either neglect-specific computer training modules or individual therapy sessions focusing on smooth pursuit eye movement training and visual exploration therapy. For smooth pursuit eye movement training, control patients were presented with clouds of dots on a computer screen that moved slowly at 5 to 10°/s from the ipsilesional to the contralesional side. Patients were instructed to follow the moving dots with their eyes. For visual exploration therapy, patients completed reading and copying tasks, image descriptions, and search tasks, all of which required them to actively orient toward their contralesional side.
Assessment of Treatment Effects
A comparison of the active NMV group against the SNT group with placebo NMV allowed to directly compare the effect of pure NMV therapy against the effect of standard neglect therapy. Before and after the intervention, both groups underwent a total of 4 examinations (cf. Figure 2) using the 4 diagnostic neglect tests described above (Letter Cancellation, Bells Test, Copying Task, Line Bisection Task), as well as the Free Exploration Test (FET 29 ;), everyday tasks from the German version of the Behavioral Inattention Test (BIT, German version: Neglect Test (NET 30 ), and the Catherine Bergego Scale (CBS 31 ). Two of the 5 diagnostic assessments were conducted before the start of the intervention to account for spontaneous recovery (Figure 2; E1 and E2), with a time interval of 1 week between them. After completing the intervention, both patient groups underwent 2 additional assessments: immediately after the training and 1-week post-training (Figure 2; E3 and E4). Additionally, the active NMV group received a fifth follow-up assessment 1 month after completing the training (Figure 1; E5).
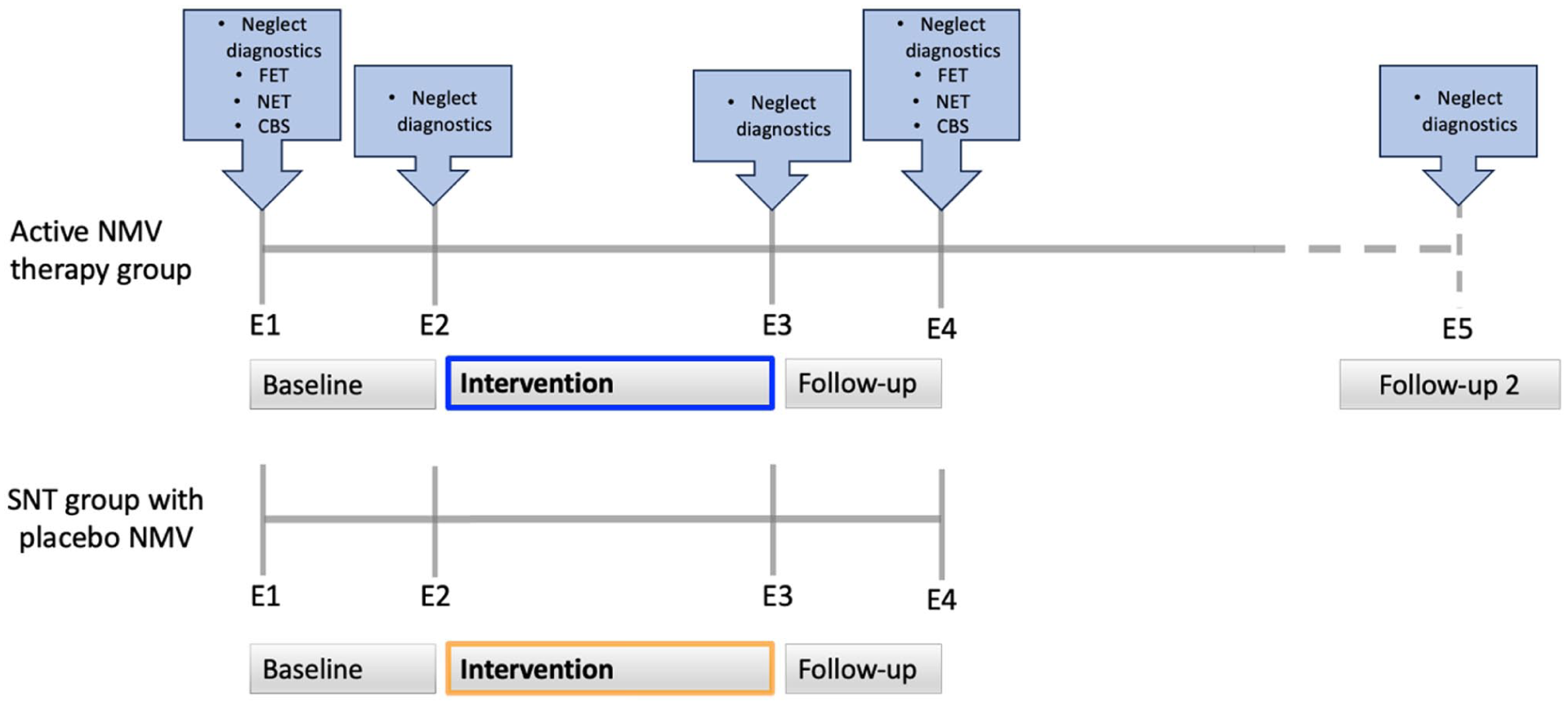
Experimental design. Four diagnostic examinations (E1 to E4) were conducted in both groups: 2 before therapy (E1, E2; 1 week apart), 1 immediately after the 2-week intervention (E3), and 1 follow-up 1 week later (E4). An additional follow-up (E5) was conducted 1 month after therapy in the active NMV group only. The 4 standard neglect tests (Letter Cancellation, Bells Test, Copying Task, Line Bisection Task), were applied at all time points; FET, NET, and CBS were assessed at E1 and E4.
Out of the 17 BIT/NET tasks, 9 are designed to assess activities of daily living (ADL). To assess ADL in the present study, we included 8 of these ADL tasks; the task requiring manual adjustment of a clock was excluded, as it demands intact bilateral hand function and would have been confounded by patients’ hemiparesis. The selected tasks included reading a newspaper article, writing an address, describing a picture of a meal, a sink, and a room, reading a menu, and reading both a digital and an analog clock. As a second method for assessing ADL, the Catherine Bergego Scale (CBS) was conducted as an observer-rated assessment. The CBS evaluates functional impairments in personal care, spatial exploration, and navigation, based on observations made by caregivers or healthcare professionals. It consists of 10 items, each rated on a 4-point scale (0–3), with higher scores indicating greater neglect severity. The maximum total score is 30, reflecting the overall impact of neglect on daily activities. According to Azouvi et al 31 the CBS score is used to classify neglect severity as follows: 0 = no behavioral neglect, 1–10 = mild behavioral neglect, 11–20 = moderate behavioral neglect, 21–30 = severe behavioral neglect. The 2 ADL tests NET and CBS were carried out at time points E1 and E4, since changes in ADL are expected to evolve more slowly. In particular, observer ratings require a certain time interval to reliably capture functional improvements. 32 In addition to the ADL tests, a further test for spatial neglect was applied at these time points. The FET is an exploration task performed on a Samsung S7+ tablet. 29 During the familiarization phase, patients were required to locate a virtual origami bird in real space, which was augmented into the environment via the tablet’s rear camera. In the subsequent test phase, patients were asked to search for the bird again, even though it had not been hidden. The patients’ exploratory movements were recorded for 30 seconds, and the average horizontal exploration movement was measured. Values exceeding 9° indicate the presence of spatial neglect. The decision to conduct the FET at only 2 time points (E1 and E4) was due to time constraints and economic considerations within the rehabilitation setting, as therapy sessions were tightly scheduled and testing time was limited. The 4 traditional neglect tests (Letter Cancellation Test, Bells Test, Copying Task, Line Bisection Task) were prioritized for repeated administration at every assessment point to ensure comparability with previous studies that have widely used these standard assessments.
Statistical Analyses
Statistical analyses were conducted using SPSS (Version 28.0). Group differences at baseline were examined using t-tests and chi-square tests. To assess within-group treatment effects, paired t-tests (baseline vs. post-intervention) were performed with Bonferroni correction (α = .017). Between-group effects were analyzed using ANCOVAs with baseline performance as a potential covariate. Additionally, linear mixed models (LMMs) were applied to account for the correlation of repeated measures within subjects and to handle missing data, thereby providing a complementary validation of the results. Significance level was set at P < .05 (2-tailed).
Results
The potential confounding variables age, sex, post-stroke interval, and neglect diagnostic test performance at baseline did not significantly differ between the active NMV group and the SNT group with placebo NMV (Table 1) and therefore were not included in further analyses. Figure 3 provides an overview of the results for both the active NMV group and the SNT group with placebo NMV across all diagnostic examinations for the 4 diagnostic neglect tests. In both groups, no significant differences were found between the measurement time points E1 and E2 for any of the 4 neglect tests (active NMV group: dependent t tests for all 4 neglect tests: P > 0.2; SNT group with placebo NMV: for all 4 neglect tests: P > 0.4). This suggests that spontaneous remission was unlikely to account for possible improvements observed after starting the intervention. For the subsequent analyses, we averaged the 2 measurements obtained at time points E1 and E2 into a single (“baseline”) variable, separately for each of the 4 diagnostic neglect tests.
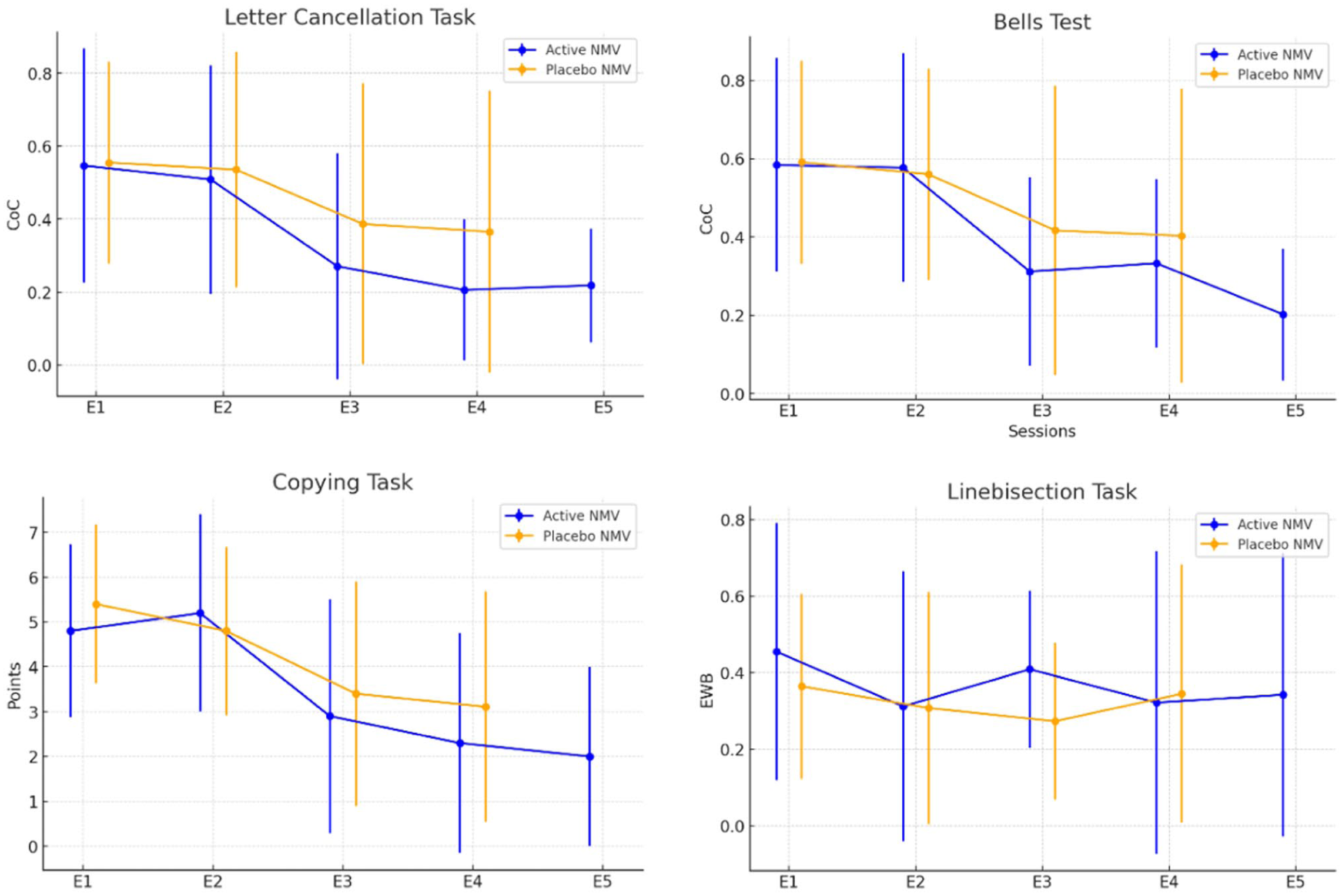
Results in the Letter Cancellation Task, Bells Test, Copying-Task, and Line bisection Task for the active NMV group (blue) and the SNT with placebo NMV (orange) over the different diagnostic examination time points (E1 to E5). Displayed are group means with standard error bars.
Treatment Effects in Diagnostic Tests of Spatial Neglect
To assess treatment effects within each group, we conducted pairwise t-tests with a Bonferroni-corrected significance level of P < .017 for pre- and post-intervention comparisons. For the 4 diagnostic neglect tests (Letter Cancellation Task, Bells Test, Copying Task, and Line Bisection Task), pairwise t-test compared “baseline” (average of E1 and E2) with E3. The results revealed significant improvements in 3 out of the 4 neglect tests in the active NMV group, whereas the placebo NMV group showed a significant change in 1 of the 4 neglect tests, namely the copying task (see Table 2). To investigate whether or not the experience of a visual illusion prior to stimulation influenced treatment outcomes, we also performed independent-samples t-tests on difference scores (“baseline” to E3) within the active NMV group for each of the 4 conventional neglect tests. Results revealed no significant differences (all P > 0.124).
Treatment Effects for the Active NMV Group and the STN Group With Placebo NMV.
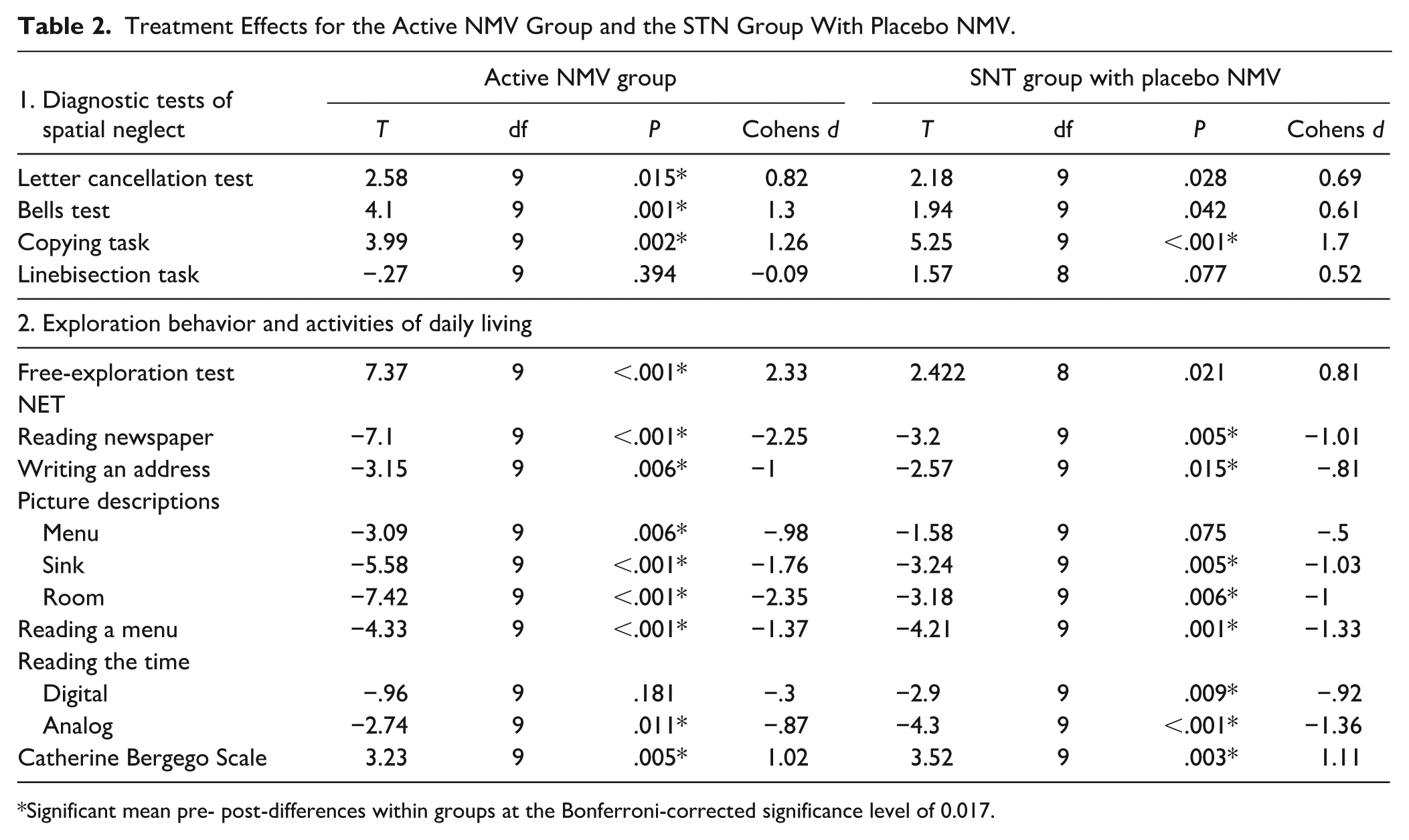
Significant mean pre- post-differences within groups at the Bonferroni-corrected significance level of 0.017.
Treatment Effects in Exploration Behavior and Activities of Daily Living (ADL)
In addition to the 4 diagnostic neglect tests, a significant improvement in exploratory behavior was also observed in the FET from E1 to E4 in the active NMV group; in contrast, the SNT group with placebo NMV showed no significant change in exploration behavior. Regarding the ADL test battery (NET), both groups exhibited significant improvements from E1 to E4 in 7 out of 8 tasks, as well as in the observer-rated CBS scale (see Table 2).
All statistical comparisons were conducted using paired t-tests before and after the intervention. According to the study design (see above), neglect diagnostic tests were compared between baseline and E3, while exploration behavior and ADL measures were compared between E1 and E4.
Development Over Time
To examine the stability of treatment effects, we conducted pairwise comparisons between consecutive time points within each group. Comparisons within the active NMV group revealed no significance difference between E3 and E4 for any of the 4 neglect tests (all P > .05) and no significant changes between E4 and the follow-up examination E5 (all P > .09). This suggests that the improvements achieved through NMV remained stable over time. Similarly, the SNT group with placebo NMV showed no significant difference between time points E3 and E4 for all 5 neglect tests (all P > 0.13).
Between-Group Effects
To examine whether the 2 groups differed from each other, a series of ANCOVAs were conducted in the first step, comparing “baseline” to E3 for the 4 neglect tests (Letter Cancellation Task, Bells Test, Copying Task, and Line Bisection Task) as well as the 2 time points before and after therapy for the FET and the ADL assessments (NET, CBS). For the NET, an averaged variable was computed across all 8 tests. The ANCOVAs revealed no significant group differences for any of the 4 neglect tests (Letter Cancellation Task: F(1,17) = 0.69, P = 0.42; Bells Test: F(1,17) = 1.08, P = 0.31; Copying Task: F(1,17) = 0, P = 0.99; and Line Bisection Task: F(1,16) = 1.33, P = 0.15). Similarly, there was no significant difference for the FET (F(1,16) = 0.31, P = 0.58) and the ADL assessments, including the averaged NET variable (F(1,17) = 0.12, P = 0.74) and CBS (F(1,17) = 0.98, P = 0.34). This indicates that both groups improved to a similar extent in terms of neglect severity, exploratory behavior, and everyday functioning, suggesting that the therapeutic effects were comparable across groups.
For complementary validation of these findings a secondary analysis, a linear mixed model (LMM) was applied to the 4 neglect tests at each time point (E1–E4), as this approach also effectively handles missing values. Missing values occurred only in a few individual cases due to specific circumstances. (In 1 case, the Line Bisection Task (E1–E4) was not completed because the patient was unable to perceive the line. Another patient was unavailable for testing at E1 for the FET due to an external appointment, which also prevented completion at E4. In a third case, all 4 neglect tests at E4 were not conducted because the patient experienced severe pain and opted for early termination.) The LMM analysis confirmed that the groups did not significantly differ at any of the test time points (E1–E4) for any of the 4 neglect tests (all P > 0.29).
Discussion
This randomized, controlled, and blinded trial examined the individual effects of neck muscle vibration (NMV) and standard neglect therapy (the latter consisting of active exploration training, the current “gold standard” in neglect rehabilitation8,33), and compared the 2 interventions. Both treatment approaches led to significant improvements of spatial neglect. While the active NMV group showed significant improvements in 3 out of 4 standard neglect tests (Letter Cancellation Task, Bells Test, Copying Task), the placebo NMV group exhibited improvement in one of these tests (Copying Task). Additionally, both groups demonstrated substantial gains in exploration activity and ADL performance, as measured by the Free Exploration Test (FET), the Neglect-Test (NET), and the Catherine Bergego Scale (CBS). Direct comparisons between the 2 groups revealed no statistically significant differences. Importantly, while both groups were re-assessed 1 week after therapy completion, the active NMV group underwent an additional follow-up 1-month post-treatment. Improvements in the active NMV group remained stable also over this longer time range.
Methodological and Clinical Context
A recent review by Duclos et al 9 characterized the research landscape on NMV in neglect as methodologically inconsistent and acknowledged that several studies were of lower quality. A central limitation identified was the absence of randomized controlled trials that isolated the effects of NMV. The present study addresses this gap; the randomized, controlled, and blinded trial found that NMV therapy leads to significant and stable improvements of spatial neglect.
Moreover, the present study addresses another deficit identified by Duclos et al, 9 namely the lack of ecologically valid outcome measures and the lacking of translational applicability. In fact, this aspect is of high clinical relevance, as persistent everyday functional limitations can remain even when core symptoms remit. 34 By using functionally relevant instruments (CBS, FET, subtests from the NET), our study demonstrated that NMV indeed induces not only improvements on diagnostic tasks but also meaningful functional changes in patients’ exploration activity and ADL performance. This aligns with prior findings by Schindler et al, 14 who applied NMV in patients with spatial neglect and found gains in reading performance and in a self-developed ADL observer questionnaire. Also, Kamada et al 20 reported improvements on the Japanese version of the Behavioral Inattention Test (BIT) which comprises 15 subtests—6 conventional neglect tests (e.g., line bisection, cancellation tasks) and 9 assessing activities of daily living (ADL).
Practical Relevance and Implementation Considerations
A major advantage of NMV is the passive application of the therapy from the patient’s point of view. Especially in the acute and subacute phases after stroke—when patients are often unable to engage in active exploration tasks or cognitive compensation strategies—such an intervention offers a valuable therapeutic approach. The fact that NMV requires no active participation of the patient and yet induces measurable functional improvements makes it an ideal building block especially (but not only) for early rehabilitation. 8
Importantly, our data suggest that the precise vibrator placement with the goal of inducing a visual illusion is (although desirable) not a prerequisite for clinical effectiveness. Of the 10 patients in the active NMV group, 5 reported experiencing such a kinesthetic illusion of the centrally presented light stimulus. Nevertheless, significant improvements in exploratory behavior occurred even in the absence of consciously perceived illusions. We did not find significant differences between those participants who did versus did not report perception of a visual illusion while searching for the exact placement of the vibrator. This finding aligns with previous reports indicating that NMV—despite successful manipulation of wanted behavior—produces a visual illusion of light spot displacement in only about 65% to 90% of subjects.11,12,16,18,35,36 With regard to this apparent inconsistency Seizova-Cajic and Sachtler 38 argued that the computation of the egocentric spatial reference frame by NMV takes place at a higher level of the visual system and is not based on the conscious perception of motion or on eye movements. Rather, proprioceptive signals from the neck muscles appear to be directly fed into multimodal areas—particularly within the parieto-temporal cortex—where they contribute to the spatial localization of objects in reference to own body. 37 Illusions resulting from this process can therefore remain unconscious, but still exert a functional influence. 38
The finding that the exact placement of the vibrator on the left posterior neck muscles is not a prerequisite for clinical efficacy, significantly lowers the practical barrier to clinical implementation and increases the accessibility of NMV in routine care. It appears that accurate placement of the vibrator, as implemented in our patient sample, is sufficient for clinical efficacy: the vibrator was positioned within a palpable depression in the left dorsolateral neck region. Based on anatomical orientation, this site corresponds to the upper part of the so-called “posterior triangle of the neck,” that is, the area of the depression between the left sternocleidomastoid muscle and the upper, descending part of the left trapezius muscle.
New Perspectives for Muscle Vibration in Neglect: Vibrating the Biceps Muscle
Interestingly, recent findings in healthy participants 16 have suggested that vibration of the right biceps muscle can induce a horizontal shift in SSA, similar in magnitude to that produced by left-sided NMV. This effect may stem from proprioceptive alterations in the limb-to-trunk signal. 16 Such findings open up novel therapeutic possibilities for patients with spatial neglect: the right biceps muscle could potentially be targeted in future vibratory interventions. Also, simultaneously vibrating the right biceps and the left posterior neck muscles may turn out a promising approach to enhance therapeutic effects. Previous studies have demonstrated that stimulating multiple proprioceptive and sensory input channels simultaneously—such as neck muscle vibration, physical trunk rotation, and vestibular stimulation—can have additive effects. These combined stimulations, which play a role in shaping egocentric spatial coordinate systems, have been shown to amplify shifts in SSA and lead to greater reductions in neglect symptoms.12,15,17,39
Also, the combination of bottom-up (e.g., left NMV, right biceps vibration) and top-down approaches (e.g., active exploration training) could possibly represent a suitable form for even better therapeutic success in neglect rehabilitation. Like Schindler et al 14 with using a combination of NMV with active exploration therapy, a recent single-case study by Ceyte et al 21 has suggested additive effects when NMV was combined with, for example, arm movements.
Limitations
A primary limitation of this study is the relatively small sample size, with 10 participants per group. Although this number aligns with previous NMV studies in the field and was supported by a power analysis based on expected effects, it limits the generalizability of the findings. Future studies with larger samples will be necessary to confirm the robustness of the observed within-group improvements and to detect potentially subtle between-group differences.
Conclusion and Outlook
The present study demonstrated that NMV, even when used in isolation, produces significant and lasting improvements in neglect symptoms and ADL-performance. The therapy is not only functionally relevant, but also easy to apply, passive in nature, and comparable in effect size to well-established approaches such as active exploration training. Moreover, it is a low-effort, non-invasive rehabilitation method that requires no active participation by the stroke patient and is therefore an ideal building block, especially (but not only) for early rehabilitation. In light of these findings, it seems imperative to integrate NMV more extensively into standard clinical practice and treatment guidelines.
Future research in NMV should focus on 3 key areas: (1) the (simultaneous) combination of NMV with top-down and/or other bottom-up therapy approaches (e.g., vibration of the biceps muscle), (2) the development of portable, hands-free NMV devices as such systems could be worn continuously during other therapies, and (3) the systematic investigation of dose–response relationships, including the optimal duration of stimulation. It remains an open question whether more frequent or prolonged application—for example, continuous stimulation during longer periods of the day—might yield even stronger effects.
Supplemental Material
sj-docx-1-nnr-10.1177_15459683251412287 – Supplemental material for A Blinded, Controlled Randomized Clinical Trial on the Efficacy of Neck Muscle Vibration in Patients with Post-Stroke Spatial Neglect
Supplemental material, sj-docx-1-nnr-10.1177_15459683251412287 for A Blinded, Controlled Randomized Clinical Trial on the Efficacy of Neck Muscle Vibration in Patients with Post-Stroke Spatial Neglect by Britta Stammler, Carina Thiel, Anne Lieb, Heike Meißner and Hans-Otto Karnath in Neurorehabilitation and Neural Repair
Footnotes
Acknowledgements
We would like to thank L. Müller, O. Roggon, and M. Wejt for their valuable contribution to data collection.
Author Contributions
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material for this article is available on the Neurorehabilitation & Neural Repair website along with the online version of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.