
Abstract
Background
High intensity interval training (HIIT) is a mode of aerobic exercise that can increase neurotrophin concentration, improve cardiovascular health, and enhance recovery post-stroke. However, HIIT is not commonly prescribed in stroke rehabilitation. Exploring the clinical utility of, and barriers and facilitators to, HIIT is necessary to optimize clinical use.
Objective
To identify perceptions of HIIT from people with stroke and health professionals working in stroke rehabilitation.
Methods
People with stroke and health professionals in Australia were invited to participate in an online questionnaire. Participants were further invited to complete a one-on-one semi-structured interview. A Framework Analysis approach was applied to identify key themes.
Results
Twenty-six people with stroke (mean ± standard deviation = 49.2 ± 60.6 months post-stroke, 57.7% female) and 37 health professionals (2 medical and 35 allied health) completed questionnaires. Ten people with stroke (5 female) and 8 allied health professionals completed an interview. Aerobic exercise was not considered a priority after stroke, though participants were interested in HIIT. People with stroke reported a lack of understanding of the benefits of HIIT and use of the term “high intensity” as barriers to participation. Facilitators included education about safety of HIIT and referral to health professionals. Health professionals reported a lack of knowledge of HIIT prescription parameters and participant motivation as barriers to prescription. Facilitators included education of HIIT prescription and benefits and appropriate screening prior to commencement.
Conclusions
People with stroke and health professionals are interested in HIIT after stroke. Increasing knowledge and confidence to participate in, and prescribe HIIT, may increase clinical use.
Keywords
Introduction
Reduced participation in exercise is a strong predictor of future stroke1 -3 and is associated with poor heart health and cardiovascular function. 3 Aerobic exercise promotes cardioprotective effects to reduce the risk of cardiovascular events such as subsequent stroke, 4 and is recommended as part of comprehensive stroke rehabilitation 5 and secondary stroke prevention. 6 High intensity aerobic exercise may reduce the risk of stroke by approximately 27%. 7 Despite this, many people with stroke do not meet exercise recommendations, creating a cycle of deconditioning, decreased function, and increased risk of cardiovascular events (eg, secondary stroke). 6
High Intensity Interval Training (HIIT) is characterized by alternating bouts of high and low intensity aerobic exercise. 8 Preliminary evidence suggests HIIT is a safe and feasible intervention for people with stroke, with few serious adverse events reported for appropriately screened participants (ie, ≥3 months post-stroke, able to walk independently, no diagnosis of unstable cardiac conditions).9 -12 Two symptomatic hypotensive events have been reported pertaining to HIIT, possibly associated with participant dehydration and malnourishment, mitigated with education on hydration and nourishment, and limiting exercise intensity. 13
The use of HIIT facilitates larger increases in cardiorespiratory fitness and walking speed compared to moderate intensity continuous aerobic exercise.14,15 HIIT can also increase the concentration of neurotrophins within the body associated with increased neuroplasticity, which may improve functional outcomes post-stroke. 16 In addition, when completed in close temporal proximity to skill training (eg, 30 minutes before or after), the use of HIIT may facilitate greater motor skill retention than skill training alone. 17
Barriers to participation in exercise following stroke have been extensively explored. Barriers such as motor impairments, fatigue, 18 lack of social support, 19 low exercise self-efficacy, 20 and fear of injury or damaging health21,22 are commonly reported by people with stroke. Support from qualified professionals, 23 education about the benefits of exercise,20,23 increased social support, and engagement in activities enjoyed prior to stroke 24 may assist in overcoming barriers to exercise participation post-stroke. From the perspective of health professionals, barriers to exercise prescription include insufficient knowledge and/or skills for safe exercise prescription,6,25 an inability to supervise exercise, lack of suitable equipment, 26 unfamiliarity with post-stroke exercise guidelines, and low prioritization of aerobic exercise. 25 Evidence-based guidelines for pre-screening and exercise prescription, appropriate monitoring of participants during exercise sessions, and further professional development for health professionals may facilitate aerobic exercise prescription for people with stroke. 25 However, it is unclear if these perceptions are applicable to HIIT, or if other barriers and facilitators exist. It is suggested that the increased intensity of HIIT may increase concern of potential orthopedic injury or cardiovascular event.27,28 This study aims to identify perceptions of HIIT post-stroke from the perspectives of people with stroke and health professionals, respectively.
Methods
An exploratory cross-sectional mixed-methods study was used to gain insights into the perceptions of HIIT after stroke using a co-designed questionnaire and semi-structured interview. Ethics approval was obtained from Australian Catholic University Human Research Ethics Committee (2022-2702H).
Participants
People with stroke and health professionals who work with people with stroke were recruited for this study via social media (eg, Twitter/X, LinkedIn, and Facebook) and professional networks of the research team. Due to the residual impact of the coronavirus disease pandemic on research in Australia 29 and limited face-to-face access with participants, a sample of convenience recruited through online strategies was used. Previous quantitative studies exploring barriers to exercise after stroke recruited 50 people with stroke 22 and an average of 123 health professioanls. 6 Qualitative research reached thematic saturation with 13 people with stroke 24 and 10 health professional focus groups (approximately 40 participants). 30
To be eligible for inclusion people needed to: (1) have a diagnosis of single or multiple ischemic and/or hemorrhagic stroke or be qualified health professionals with experience working with people with stroke, (2) be aged ≥18 years, (3) live in Australia, and (4) understand written and verbal English language.
Procedure
All participants completed an online questionnaire via REDCap between 28 March 2023 to 14 September 2023. A subset of participants completed a one-on-one semi-structured interview via Zoom to further explore the perceptions of HIIT after stroke. After completing the questionnaire, all participants were invited to complete an expression of interest form for the semi-structured interview. Responses of the expression of interest form were not linked to questionnaire responses to ensure anonymity of the questionnaire.
Two separate questionnaires were used, 1 for people with stroke and 1 for health professionals. An initial draft of both questionnaires were developed following review of existing literature exploring barriers and facilitators to non-HIIT exercise and/or physical activity after stroke18,26,31,32 and interview findings of 12 people with stroke who completed a HIIT program. 33 Draft questionnaires were then put to a panel of lived experts (ie, 4 people with stroke, and 2 health professionals with experience working with stroke) for comment, clarification, and amendment. Questionnaires included the following description of HIIT, “High Intensity Interval (HIIT) sessions; are a form of heart health exercise involving alternating brief bouts of higher effort exercise and lighter effort exercise, 8 in total; can last from just a few minutes up to about 30 minutes; are individualized to your fitness and interests; and can be done on a bike (legs or arms), treadmill, boxing, and in many more ways.” A graphic was provided to depict the alternating intensities utilized in a HIIT session (Figure 1 in Supplemental Files 1 and 2). Closed and Likert-type questions were included to provide information about barriers and facilitators to the participation in, and prescription of, HIIT after stroke (Supplemental Files 1 and 2). Semi-structured interview scripts were developed by the research team, in consultation with a psychologist and a qualitative researcher, comprising open-ended questions and 1 to 10 rating scales to extend upon topics covered in the questionnaires and facilitate conversation (Supplemental Files 3 and 4).
Data Analysis
Questionnaire data were downloaded from REDCap, and imported into Statistical Package for Social Science (SPSS) for analysis (IBM SPSS Statistics, version 29.0.1.0). Participant demographic data are presented as mean and standard deviation (SD), and percentages where appropriate. Questionnaire responses are presented as frequency and percentage. Semi-structured interviews were recorded on Zoom and transcripts were developed in Microsoft Word Online. Transcripts were checked verbatim against recordings and analyzed by 2 independent assessors using the Framework Analysis approach, 34 using NVivo (Lumivero NVivo, 14). The Framework Analysis approach was implemented due to its common use for semi-structured interviews and provision of clear steps to provide output. 35 Briefly, 2 independent assessors read the transcripts and identified a thematic framework by developing codes organized into categories. 34 Following analysis of all transcripts, data were entered into a spreadsheet containing codes and cases 34 and approved by both assessors. Discrepancies were moderated by a third independent assessor if required. Synthesized member checking, whereby all participants were emailed a summary of the results and asked to provide feedback, was undertaken. 36 Any feedback provided (ie, naming of themes or choice of quotes) were then discussed with the research team with amendments made accordingly and the synthesized member checking process completed again. Interview data are presented as themes, with quotes provided by people with stroke and health professionals.
Results
Participants
Thirty-two people with stroke commenced the online questionnaire, of which 26 (81%) completed the full questionnaire and were included in the analysis (Table 1). Questionnaire participants were on average 49.23 (SD = 60.66) months post-stroke, 57.7% participants were female, and 84.6% experienced at least 1 impairment after stroke. A subset of 10 people with stroke participated in a one-on-one, online semi-structured interview (Table 1). Interview participants were on average 39.30 (SD = 24.87) months post-stroke, 5 were female (50%), and 90% of participants reported at least 1 impairment. Two (20%) people with stroke reported never completing HIIT. One (10%) participant reported completing HIIT pre-stroke only, 3 (30%) participants reported completing HIIT post-stroke only, and 4 (40%) participants reported completing HIIT pre- and post-stroke.
People With Stroke Participant Demographics.
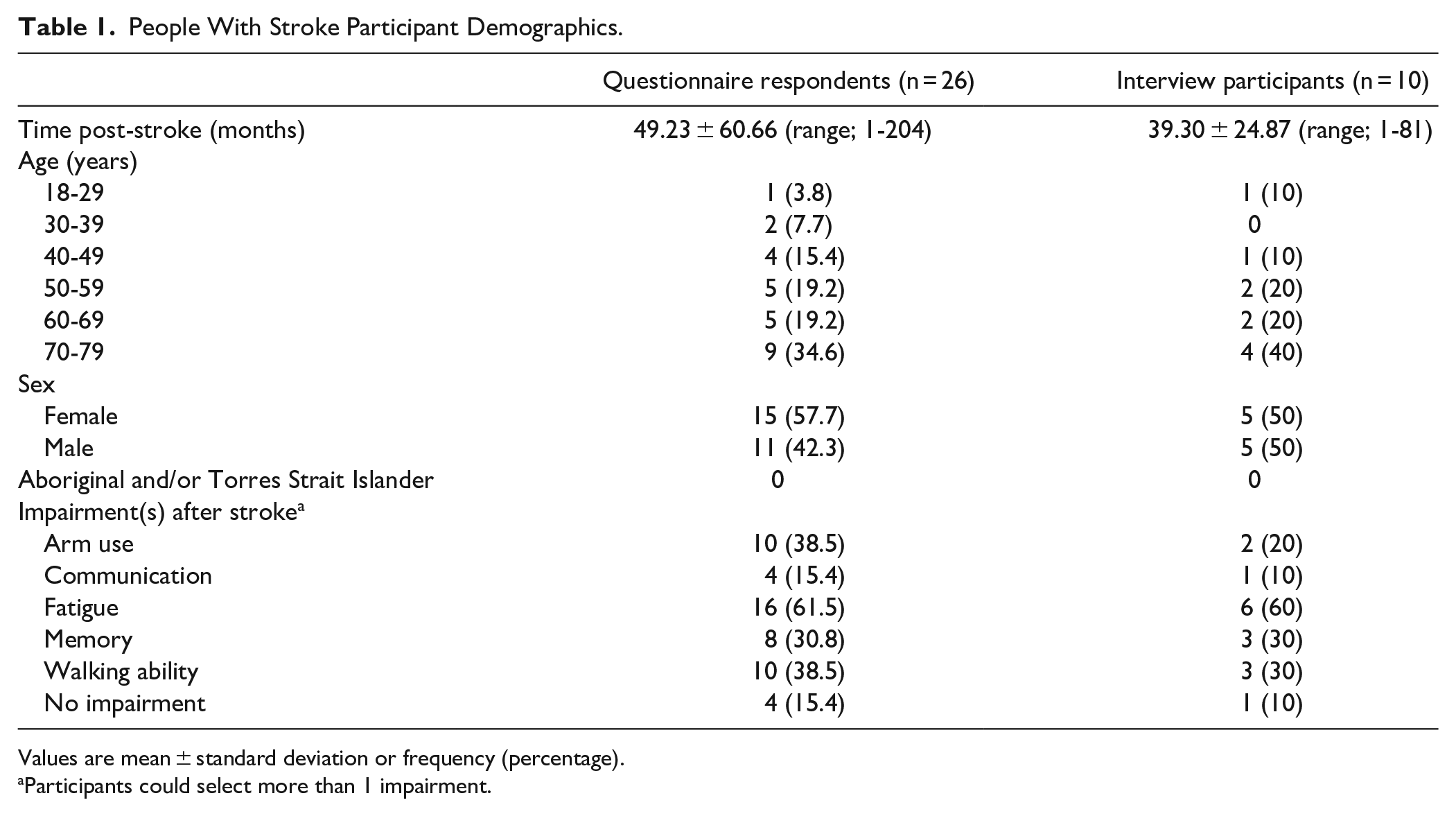
Values are mean ± standard deviation or frequency (percentage).
Participants could select more than 1 impairment.
Forty-four health professionals commenced the online questionnaire, of which 37 (84%) completed the full questionnaire and were included in the analysis (Table 2). Most questionnaire participants were physiotherapists (59.5%) or exercise physiologists (32.4%) with more than 1 year of clinical experience (97.3%). Eight health professionals participated in a one-on-one, semi-structured interview (Table 2). Six (75%) interviewees were physiotherapists, 75% of interviewees worked with people with stroke during the subacute phase of stroke recovery, while all worked with people with stroke in the chronic phase of stroke recovery.
Health Professional Participant Demographics.

Values are mean ± standard deviation or frequency (percentage).
Participants could select more than 1 impairment.
Questionnaire Results
Thirteen (50%) people with stroke that completed the online questionnaire reported participating in HIIT previously (ie, before and/or after stroke), and 19 (73.1%) respondents expressed an interest in participating in HIIT. Following stroke, 10 (39%) participants reported a walking impairment, with 6 (23%) reporting the use of a walking aid for ambulation. Ten (39%) reported an upper limb impairment, 8 (31%) reported a memory impairment, 4 (15%) reported a communication impairment, and 16 (62%) reported post-stroke fatigue.
A lack of knowledge about the benefits of HIIT, and a lack of support from other people with stroke and health professionals were the most reported barriers to participation in HIIT by people with stroke (Figure 1). The most reported facilitators to HIIT participation included supervision by a trained professional during sessions and being educated on the safety, benefits, and personalization of HIIT (Figure 2).
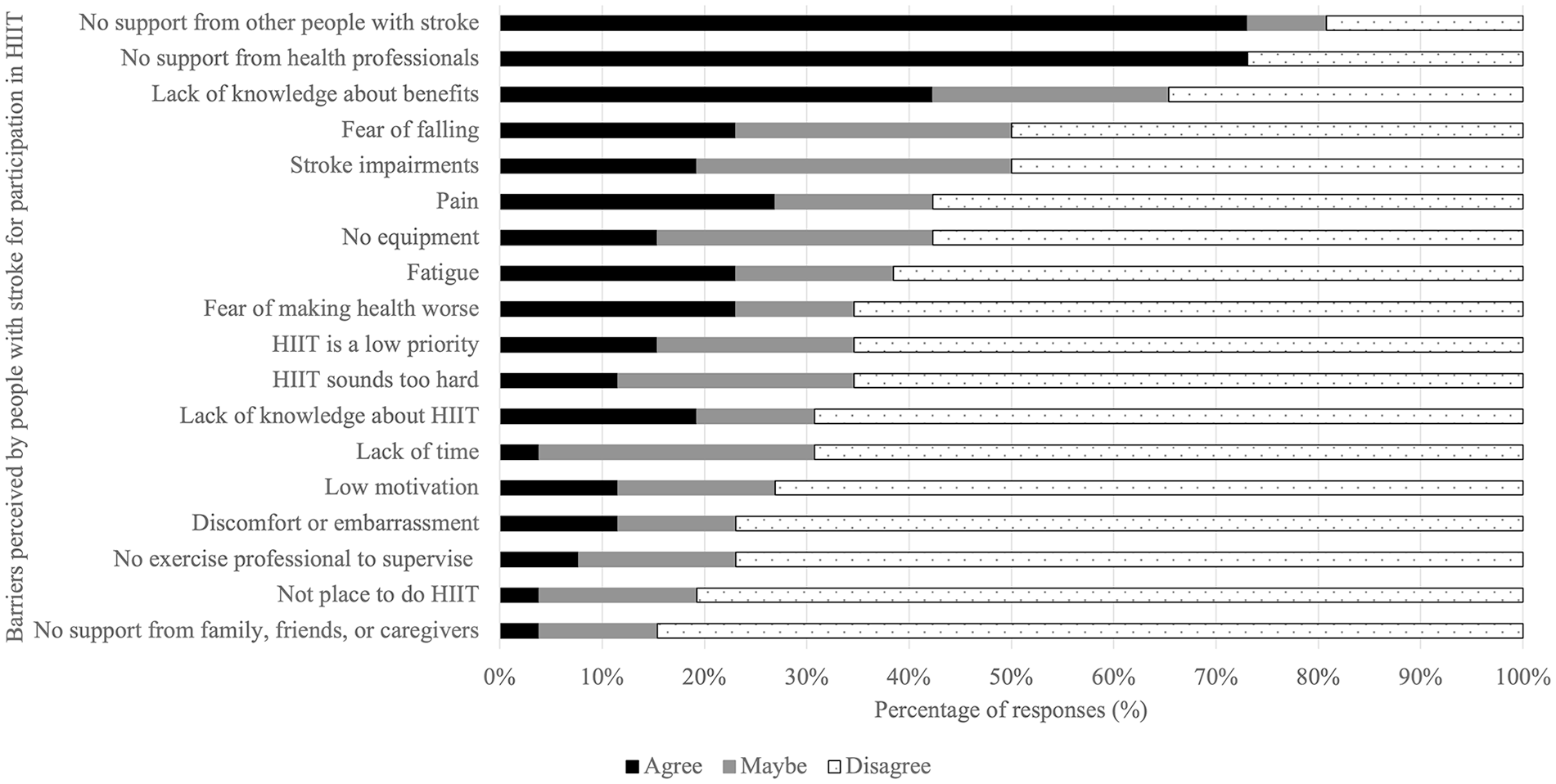
Barriers perceived by people with stroke for participation in HIIT by questionnaire.
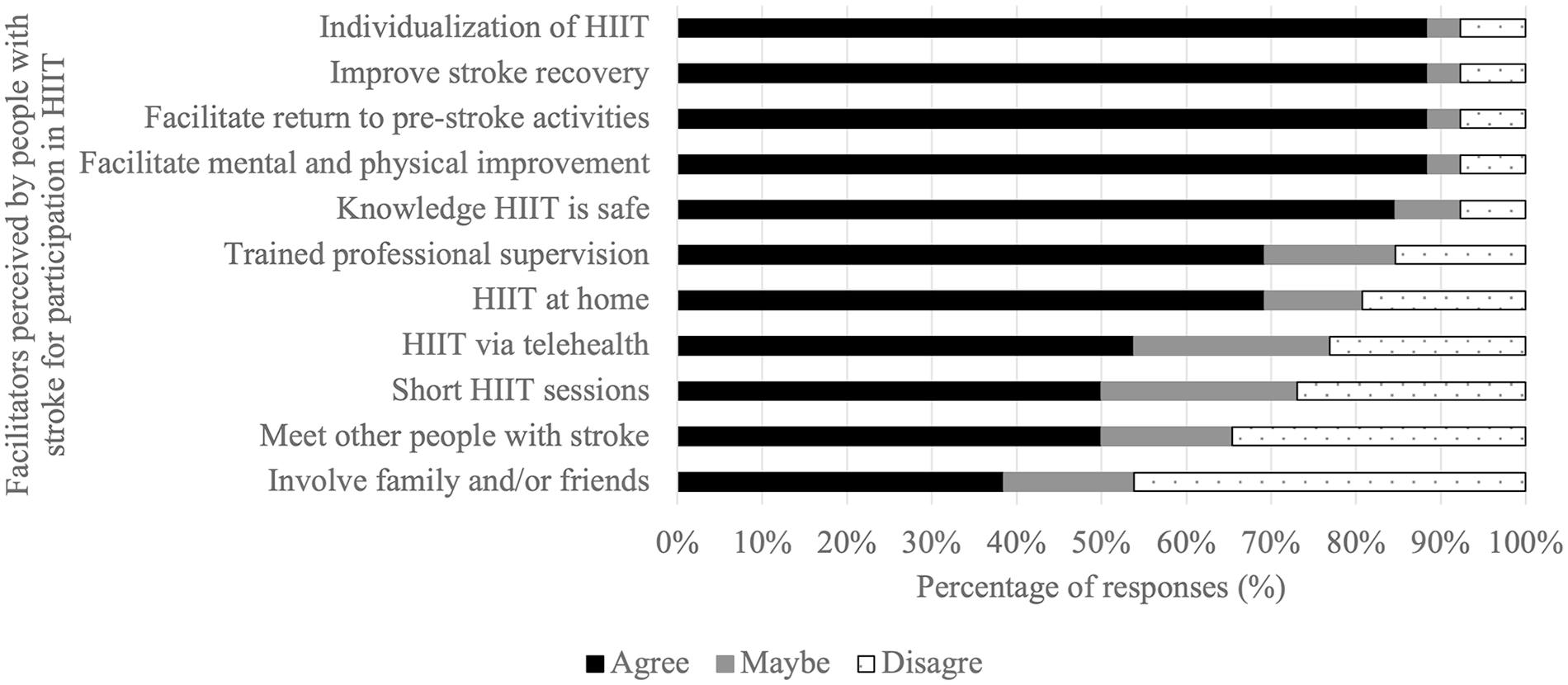
Facilitators perceived by people with stroke for participation in HIIT by questionnaire.
Twenty-seven (73%) health professionals reported they recommend and/or prescribe HIIT to people with stroke, and 23 (62.2%) reported confidence in their ability to prescribe HIIT. A lack of knowledge regarding when to commence HIIT post-stroke (ie, phase of stroke) and how to personalize HIIT to the person with stroke (eg, impairment and goals), as well as the varied motivation and fatigue of the person with stroke were the most reported barriers to the recommendation/prescription of HIIT by health professionals (Figure 3). The most reported facilitators to HIIT recommendation/prescription included being educated about the prescription and benefits of HIIT, being able to supervise people with stroke during exercise sessions, and appropriate screening prior to the commencement of HIIT (Figure 4).
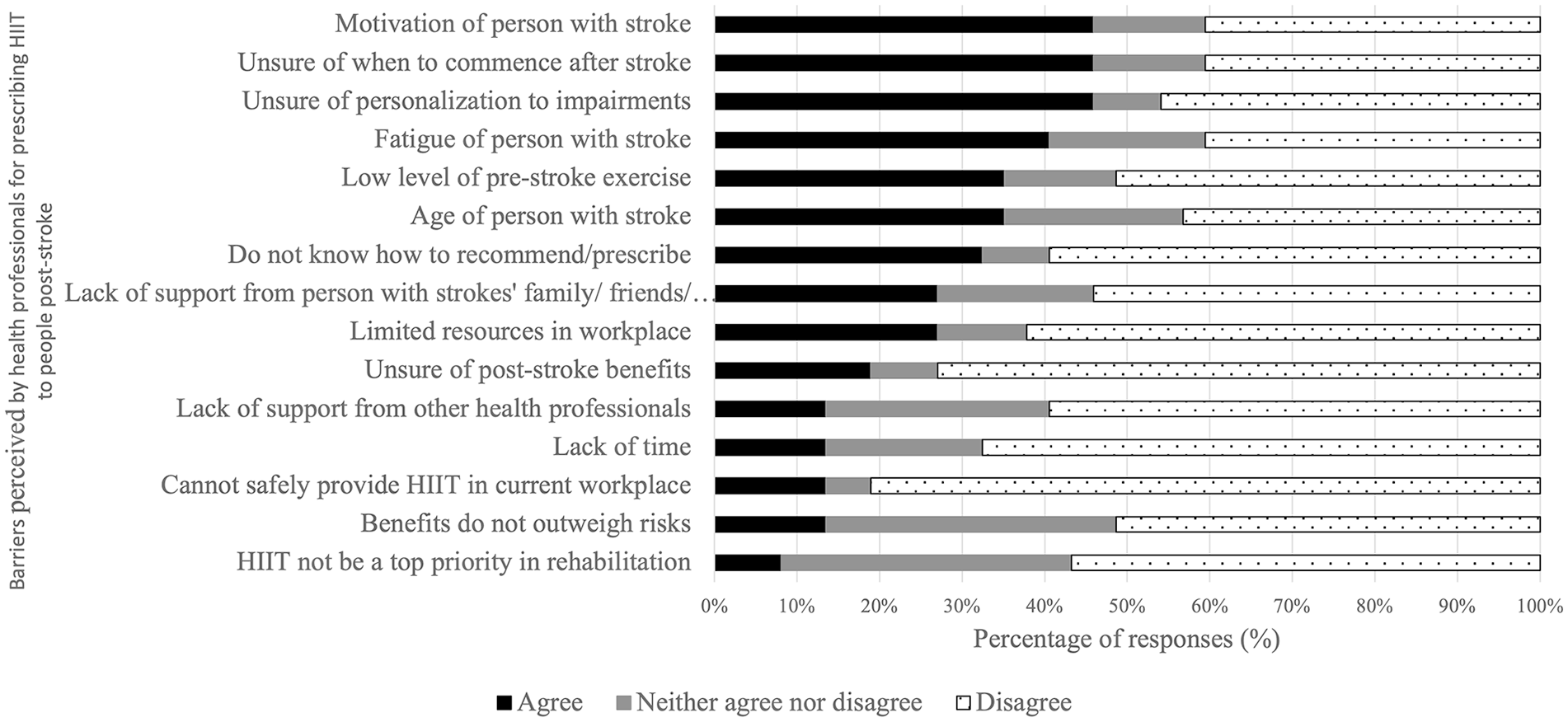
Barriers perceived by health professionals for prescribing HIIT to people post-stroke by questionnaire.
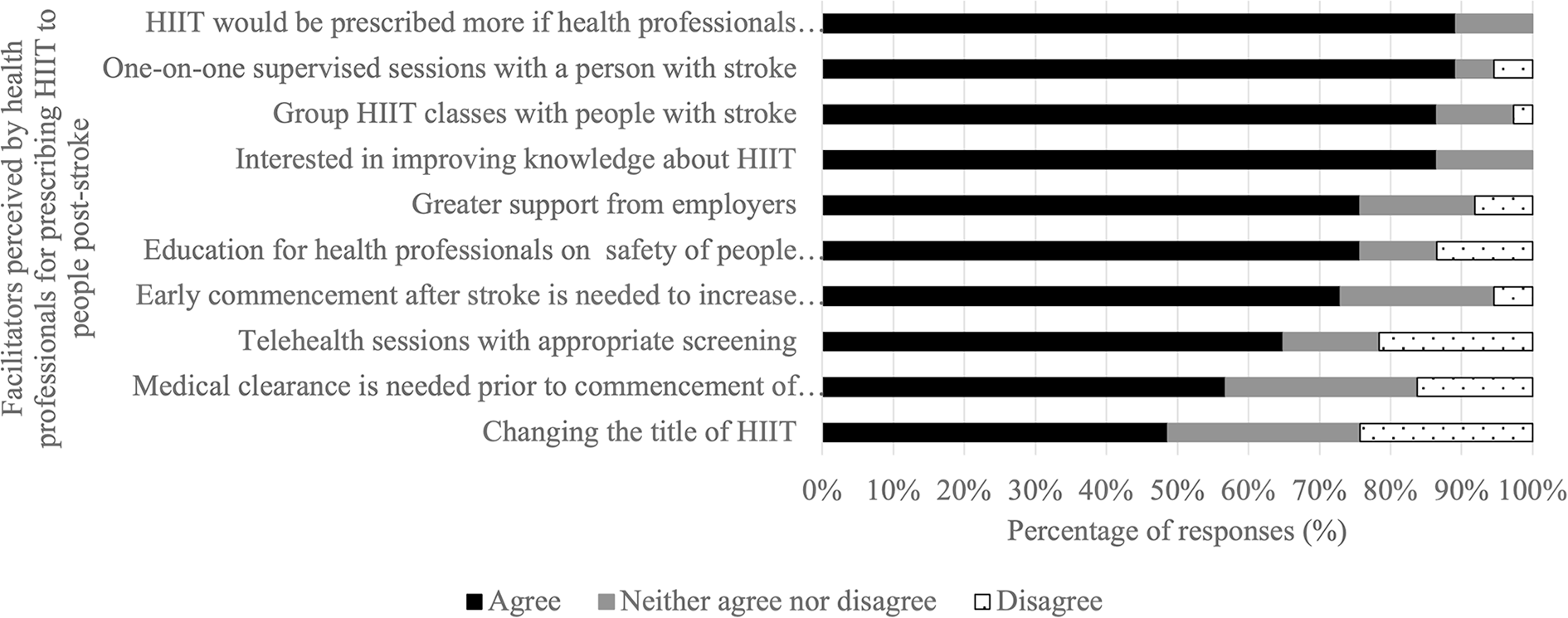
Facilitators perceived by health professionals for prescribing HIIT to people post-stroke by questionnaire.
Themes From Semi-structured Interviews
Analysis of interview transcripts identified 4 themes about the use of HIIT after stroke from the perspectives of people with stroke and health professionals.
Theme 1: “I Can Get Around and Walk Around the House and I Can Walk Around the Block If I Want To, [aerobic exercise] Just Becomes a Low Priority” (Person With Stroke 2)
Both people with stroke and health professionals indicated aerobic exercise is not a high priority during rehabilitation. Instead, functional recovery (ie, improving gait and balance), is considered of a higher priority, especially by the treating health professional:
It’s not my main priority (Person with stroke 2).
I was weak and I still am, so it’s important to do strength-based exercise (Person with stroke 7).
A very severe stroke, very disabled, then we’re focusing more on sit to stand, sitting balance (Health professional 3).
What are their priorities and how can I get them to engage with me as a therapist? Sitting down and saying, ‘Let’s do some cardiovascular fitness’, people may go, ‘No thanks, I’ll find a physio[therapist] who will look at my hand or look at my weak ankle’. [I’ve] got to be really selective (Health professional 6).
However, both groups consider HIIT a useful adjunct therapy due to the potential physical and mental benefits elicited:
If I do high intensity, I think it might speed up the nervous system (Person with stroke 2).
I want to reduce my risk of having a stroke for other health reasons in the future (Person with stroke 4).
Mental health improvements. . .potentially cognitive improve-ments (Health professional 1).
It’s good for your cardiovascular system. . .help prevent you from having a future stroke (Health professional 5).
Despite HIIT being considered beneficial after stroke, the health professionals interviewed highlighted the need for appropriate screening prior to the commencement of HIIT to increase safety of the participant:
There would be a ‘this is too early point’. . .if they’re not medically stable. And I think that would be a barrier to starting [HIIT] (Health professional 1).
The more acute they are, then medical clearance is needed (Health professional 7).
Theme 2: “I’m a Bit Concerned About the Word ‘High Intensity’” (Person With Stroke 1)
People with stroke and health professionals reported that the term ‘high intensity’ may be off-putting and limit participation in HIIT after stroke. The term was considered intimidating, especially to older people with stroke and/or those who were more apprehensive to exercise:
High intensity kind of excludes someone who thinks that they’re a little bit vulnerable (Person with stroke 2).
To somebody a bit older they’d be like, ‘Oh is this going to hurt?’ (Person with stroke 3).
I don’t sit down and say, ‘Alright, now we’re going to do some high intensity interval training’, because I feel that most of my patients would go, ‘You’re mad, you’ve lost the plot’ (Health professional 6).
Instead, a description of the HIIT intervention should be provided with emphasis on the use of intervals and highlighting the personalized nature of the intervention, that is, the intensity of the training is relative to each participant’s effort and fitness levels:
It might just be worded as ‘interval training’. ‘We’re working for on and off periods, fast and slow (Health professional 7).
I do think that slipping things in like [the intensity is relative to them] is a really good way to just like prove them wrong about some beliefs that they have (Health professional 8).
Theme 3: “Interdisciplinary Allied Health Would be Invaluable” (Health Professional 7)
Interview participants reported that referral to appropriate health professionals to prescribe HIIT interventions may increase participation. People with stroke did not express a preferred profession to deliver or supervise the intervention, while health professionals reported the need for a multidisciplinary approach:
As long as the health professional understood the challenges with each [person with stroke] (Person with stroke 1).
Physiotherapists and exercise physiologists can work together, discuss the patients together. . .the level of assistance needed or the ability of the patient (Health professional 3).
Health professionals consistently reported the importance of seeking medical clearance for people with stroke prior to commencing HIIT. However, a general lack of understanding of what HIIT is, the benefits of HIIT, and who HIIT is appropriate for, may restrict access to HIIT:
I think there’s also a disconnect with the medical professionals understanding [exercise intensity] (Health professional 7). My only concern with that is who’s going to be giving that medical clearance. . .[will they know] what high intensity interval training is and know that it’s safe (Health professional 8).
Theme 4: “You Just Need Perhaps a Bit of an Explanation as to What It is” (Person With Stroke 5)
Both groups identified education as necessary to increase the uptake and prescription of HIIT after stroke. Education for people with stroke should center around participant safety, particularly how the intervals will accommodate personal factors, such as comorbidities and post-stroke impairments:
The thing that scares me a bit is whether it’s safe enough for me to do it (Person with stroke 1).
It’s a fear of if I do that little intensive spurt I’m gonna crash and burn. So, it’s probably more the unknown (Person with stroke 4).
Who knows what they see in social media, Facebook or TikTok. . .they might have been misinformed. . .[health professionals] can explain to them, educate them what it actually involves. But also [that it is] personalized, so it’s related back to why it’s relevant to them (Health professional 3).
Education is quite important to let people know that this is safe, and you can do it (Health professional 4).
People with stroke want information about HIIT from educated and qualified professionals:
I’d have to be very trusting on what people would say and if they said it was good then I’d do it. If I read it on the back of the Kellogg’s packet, maybe I’d be a bit dubious (Person with stroke 3).
While only 1 health professional had training in the recommendation/delivery of HIIT, all health professionals recognized the need to upskill to incorporate HIIT into practice:
You have to be on board with it yourself and then your client’s going to be on board (Health professional 2).
The risks versus benefits analysis. . .type of screening to be done in addition to your typical screening. . .preferred mode of delivery. . .common medications that may be contraindicated (Health professional 7).
However, to allow multidisciplinary decision-making, discussions about the potential benefits of HIIT for people with stroke must be discussed with the wider stroke rehabilitation team:
So, I think there’s also a disconnect with the medical professionals also understanding that [HIIT is relative intensities] (Health professional 7) I do not trust on [the GP’s] ability to know what high intensity interval training is and know that it’s safe (Health professional 8).
This education may be delivered by exercise physiologists or physiotherapists experienced in the use of HIIT after stroke:
Deliver the presentation as part of an inservice (Health professional 3).
To facilitate the increase of the uptake and prescription of HIIT after stroke, further research into the benefits of HIIT is required. This is necessary to increase the evidence-base of HIIT to facilitate its inclusion in exercise recommendations for stroke rehabilitation:
It would be good if there was evidence out there for high intensity interval training (Health professional 5).
Need more research to change the evidence. . .Because it’s a live guideline, they review it with the evidence, they change [the recommendations]. . . (Health professional 3).
Discussion
In this mixed-methods study people with stroke and health professionals working with people with stroke reported HIIT is currently not a routine component of stroke rehabilitation. However, people with stroke and health professionals are interested in the inclusion of HIIT provided participant safety is assured. Participants in this study report patient and clinician education on the use of HIIT in clinical practice post-stroke as necessary to ensure the safety of people with stroke participating in HIIT interventions.
To the best knowledge of the research team, this is the first study to explore perceptions of HIIT amongst people with stroke and health professionals in Australia. The use of HIIT interventions following stroke has demonstrated improvements in cardiorespiratory fitness, walking speed,10,14,15,37 balance, 14 and fatigue 10 when compared to moderate intensity aerobic exercise. However, HIIT is not commonly recommended in clinical practice 9 and therefore exploration of barriers and facilitators to its clinical application is important. While the most reported barriers to HIIT in this study were not consistent with those reported for general exercise, some identified barriers and facilitators were consistent with those previously identified as barriers and facilitators to aerobic exercise after stroke.20,25 People with stroke who have engaged with HIIT enjoy the intervention and identified benefits in physical function and daily life which outweighed the hard work required from the intervention. 33 In the current study, people with stroke reported support from health professionals and greater education about HIIT and its proposed benefits as facilitators to greater engagement in HIIT, which aligns with existing evidence.20,23 Health professionals interviewed in this study were not averse to including high intensity interventions in clinical practice, however many were uncertain as to how to implement HIIT. Given aerobic exercise is not considered a high priority with respect to stroke rehabilitation research by people with stroke 38 and health professionals, 39 the emphasis placed on the use of HIIT for aerobic exercise training in this study may have impacted questionnaire engagement and responses. Additionally, health professionals within this study reported self-efficacy in delivering high intensity interventions may be increased with appropriate screening and monitoring of participants prior to, and during the intervention, respectively. 40
As reported by people with stroke and health professionals in this study, concerns about safety are a barrier to participation in HIIT. While safety concerns are not commonly reported as a barrier to engagement in aerobic exercise after stroke, 38 people with stroke that participated in this study raised concerns regarding comorbid status and increased anxiety with respect to the high intensity aspect of the HIIT intervention. Some exacerbation of comorbidities (eg, musculoskeletal pain) 10 and serious adverse events such as hypotension 13 have been reported previously. People with stroke have voiced concerns regarding exacerbation of health problems, stroke-related impairments, 21 and fear of falling41,42 as barriers to engagement in exercise post-stroke. Such concerns were not reported as barriers to HIIT by people with stroke in this study which may be associated with the longer time post-stroke and increased pre-stroke exercise behaviors of the participants in this study.
An array of personal and environmental factors may impact perceptions of exercise from people with stroke and health professionals. Presence of comorbidities (eg, cardiovascular or endocrine conditions),20,21 severity of post-stroke impairments (eg, physical and/or cognitive impairment),41,43 and the absence of a support system to facilitate engagement in exercise post-stroke20,44 may reduce a person with stroke’s willingness to engage in exercise, and therefore HIIT. Prior engagement in HIIT may affect the level of apprehension, confidence, and enjoyment a person with stroke feels toward participation in HIIT. 9 Availability of the equipment and time necessary to prescribe HIIT 31 may also impact a health professionals’ ability to implement HIIT, however this was not reported as potential barriers to prescription by the health professionals in this study.
Changing the terminology used by health professionals or even avoiding the phrase “high intensity” when discussing HIIT was identified as a potential facilitator of HIIT. This is a novel finding from this study. Both people with stroke and health professionals suggested the focus should be placed on the structure of the intervention, with the session comprising intervals of alternating easy and high effort and emphasizing that the high effort is relative to the capabilities of the participant and within what is deemed safe for them based on pre-exercise screening. Therefore, person-centered education about the personalization of HIIT accounting for stroke impairments, comorbidities, and fitness level, as well as appropriate monitoring strategies to be utilized during exercise sessions is warranted. 4
Health professionals identified a lack of knowledge and/or confidence in prescribing HIIT and being able to adapt or individualize the intervention to the person with stroke’s impairments in the current study. A lack of knowledge and/or confidence to prescribe exercise to people after stroke has previously been reported by health professionals working in stroke rehabilitation.25,26 Continued professional development 45 and refinement of safety criteria and assessment 4 are considered potential methods to increase health professionals’ confidence to prescribe HIIT to people with stroke. Therefore, clearer recommendations specific to HIIT prescription, especially for the prescription of interval intensity and duration, may increase the use of HIIT in clinical practice. Further research is needed to increase the understanding of the benefits of HIIT and how this intervention can be implemented for people with stroke in clinical practice. The development of educational material for targeted professional development courses, including safety considerations and prescription principles, is also needed to increase knowledge and self-efficacy of health professionals with the intervention. 40
Limitations
A small sample size was recruited for this study; however, this is the first study to include both population groups. An online platform (ie, REDCap) was used to increase the reach of the study, which may have resulted in lower response rates when compared to paper-based methods. 46 Convenience sampling was implemented which may have yielded a biased sample with limited diversity. Therefore it is unclear whether the findings are representative of the wider population, potentially limiting the generalizability of the findings. The severity of post-stroke impairments and subsequent reliance on others for assistance, 47 have previously been reported as barriers to exercise post-stroke. These barriers were not reported in the current study; however, this may be due to most participants being independently mobile, with high levels of exercise participation and enjoyment of exercise post-stroke reported within the sample.
Health literacy of the individual, or the protection of family and friends 48 may also be barriers to exercise participation. Race or ethnic origins were not explored within this study; however this may be an important area of future research. The description and graphical representation of HIIT was developed by the research team in conjunction with lived experts. This was a broad description with a wide variation in interval durations and intensities that may be shorter than conventional HIIT, 27 such that participants’ understanding or perceptions of the intervention may have been impacted.
Bias was demonstrated toward allied health professionals with expertise in exercise prescription (ie, exercise physiologists and physiotherapists) despite attempts to recruit through medical networks, however this appears to be common within the literature as these are typically the professions providing exercise interventions in healthcare.25,49 While all health professionals who work with stroke were targeted due to a multidisciplinary stroke rehabilitation approach being recommended, 49 the inclusion of non-exercise specializations (eg, medical professionals) may have provided different perspectives. Approximately 3-quarters of health professionals reported having previously prescribed HIIT to people with stroke which may have further skewed the perceptions voiced within this study. The confidence of the health professional in their ability to facilitate person-centered exercise,6,41 and their belief in the value of the intervention 50 may also impact a health professionals’ ability to implement HIIT. These factors were not explicitly explored within this study; therefore, conclusions cannot be made regarding the effect of these factors on the participants’ perspective of HIIT.
Future Research Directions
To improve the generalizability of this research, future studies could expand the sample to increase representation of the heterogenous stroke and health professional community. It is recommended that people with stroke of different ages, stages of recovery, with varied previous engagement in, and preferences for, exercise including HIIT (ie, with and without experience in HIIT), different levels of physical and cognitive impairment, as examples, be included in future research. Similarly, medical and health professionals with a differing scope of practice, experience level, and expertise with exercise are required to support the development of strategies to increase the clinical utility, acceptability, and uptake of HIIT in clinical practice. Future research should explore the potential ways to implement the facilitators to HIIT identified in this study in clinical practice.
Conclusion
The findings of this study suggest that people with stroke and health professionals who work with people with stroke are interested in HIIT. Yet HIIT is rarely utilized in clinical practice. Additional research is required to explore safety procedures, the benefits of HIIT after stroke, and facilitate the development of participant and provider education to optimize HIIT participation and prescription. While HIIT is not included in clinical guidelines,4,50 HIIT shows promise as an intervention to improve functional outcomes. High quality randomized controlled trials are needed to optimize the dosage, effectiveness, and timing of HIIT delivery post-stroke to allow for integration into clinical guidelines.
Supplemental Material
sj-docx-1-nnr-10.1177_15459683251317185 – Supplemental material for High Intensity Interval Training POst-STroke (HIIT-POST): Perspectives of People Living With Stroke and Health Professionals
Supplemental material, sj-docx-1-nnr-10.1177_15459683251317185 for High Intensity Interval Training POst-STroke (HIIT-POST): Perspectives of People Living With Stroke and Health Professionals by Sarah K. Ashcroft, Liam Johnson, Suzanne S. Kuys and Angelica G. Thompson-Butel in Neurorehabilitation and Neural Repair
Supplemental Material
sj-docx-2-nnr-10.1177_15459683251317185 – Supplemental material for High Intensity Interval Training POst-STroke (HIIT-POST): Perspectives of People Living With Stroke and Health Professionals
Supplemental material, sj-docx-2-nnr-10.1177_15459683251317185 for High Intensity Interval Training POst-STroke (HIIT-POST): Perspectives of People Living With Stroke and Health Professionals by Sarah K. Ashcroft, Liam Johnson, Suzanne S. Kuys and Angelica G. Thompson-Butel in Neurorehabilitation and Neural Repair
Supplemental Material
sj-docx-3-nnr-10.1177_15459683251317185 – Supplemental material for High Intensity Interval Training POst-STroke (HIIT-POST): Perspectives of People Living With Stroke and Health Professionals
Supplemental material, sj-docx-3-nnr-10.1177_15459683251317185 for High Intensity Interval Training POst-STroke (HIIT-POST): Perspectives of People Living With Stroke and Health Professionals by Sarah K. Ashcroft, Liam Johnson, Suzanne S. Kuys and Angelica G. Thompson-Butel in Neurorehabilitation and Neural Repair
Supplemental Material
sj-docx-4-nnr-10.1177_15459683251317185 – Supplemental material for High Intensity Interval Training POst-STroke (HIIT-POST): Perspectives of People Living With Stroke and Health Professionals
Supplemental material, sj-docx-4-nnr-10.1177_15459683251317185 for High Intensity Interval Training POst-STroke (HIIT-POST): Perspectives of People Living With Stroke and Health Professionals by Sarah K. Ashcroft, Liam Johnson, Suzanne S. Kuys and Angelica G. Thompson-Butel in Neurorehabilitation and Neural Repair
Footnotes
Acknowledgements
The authors would like to thank the participants of this study. The authors would also like to thank Saran Chamberlain, Clive Kempson, Letisha Living, Terence Polkinghorn, Justine Stynes, Danielle Hassarati, and David Peng for their contributions to the development of the questionnaire and semi-structured interview script. The authors would also like to thank Samantha Walsh and Stephanie Frade for their assistance in the conduct and analysis of the semi-structured interviews, respectively.
Author contributions
SKA: Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Project administration; Validation; Writing—original draft; and Writing—review & editing. LJ: Conceptualization; Methodology; Supervision; and Writing—review & editing. SSK: Conceptualization; Methodology; Supervision; and Writing—review & editing. AGT-B: Conceptualization; Methodology; Supervision; and Writing—review & editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplementary material for this article is available on the Neurorehabilitation & Neural Repair website along with the online version of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.