
Abstract
Background
Stroke is one of the leading causes of chronic disability worldwide. Sensorimotor recovery relies on principles of motor learning for the improvement of movement and sensorimotor function after stroke. Motor learning engages several cognitive processes to effectively learn and retain new motor skills. However, cognitive impairments are common and often coexist with motor impairments after stroke. The specific relationships between poststroke cognitive impairments and motor learning have not been determined.
Objectives
To summarize the existing evidence related to cognitive impairments and motor learning after stroke. Specific goals were to determine: (1) how motor learning is studied in individuals with poststroke cognitive impairments; (2) how cognitive impairments are assessed; (3) which cognitive domains impact motor learning.
Results
Over 400 studies were screened for specific inclusion criteria and 19 studies that related poststroke cognitive impairments to motor learning were included. Studies used a wide variety of experimental designs, sample sizes, and measures for cognitive evaluation. Cognitive impairments impacting motor improvement and learning capacity after stroke were reported in all but 4 studies. The most common domains impacting motor learning were attention, executive function, and memory.
Conclusion
Detailed cognitive assessments, retention testing, and a combination of clinical and kinematic outcomes are recommended for future studies. The presence of specific cognitive impairments measured with sensitive instruments should be considered when designing effective training interventions for patients with stroke to maximize sensorimotor recovery.
Background
Each year, ~12.2 million people worldwide suffer stroke 1 and 55% to 75% experience persistent sensorimotor deficits (ie, >6 months post-stroke 2 ). Sensorimotor recovery relies on the inherent plasticity of the nervous system.3,4 At the behavioral or task level, motor recovery refers to the return of movement patterns present before injury, while motor compensation involves alternative movement patterns for task accomplishment. 5 Sensorimotor recovery relies on motor learning principles such as repetitive goal-directed practice, use of sensory information to adapt and form new movement patterns related to the task and the environment,4,6,7 and the manipulation of task difficulty according to motor skill level. Recovery has also been linked to individual cognitive capacity, 8 but details about the relationship between motor learning and cognition still need elucidation.
In addition to sensorimotor deficits, ~65% to 70% of stroke survivors have cognitive deficits. 9 Motor learning and cognition engage many inter-related neural components.10,11 Cognitive processes important to adapt movements to changes in task and environmental conditions 4 include sensory information interpretation, 12 response selection (executive function), 13 direction and maintenance of attention, 14 and memory.15,16
Executive function deficits affect planning, initiation of goal-directed activities, and problem-solving related to task or environmental changes.4,17 Attention deficits may decrease mental flexibility, impair concentration, and affect processing information from multiple sources (ie, dual-tasking). 18 Memory problems may affect intake, storage, and retrieval of information, such as using feedback to adapt subsequent movements. 19
Cognitive impairments may hinder motor learning by diminishing error perception and movement pattern adaptation.20,21 Motor learning involves 3 phases: acquisition, retention, and transfer. 13 Acquisition is the initial period of skill practice. “Strategic” or “cognitive” learning occurs early in acquisition and is characterized by rapid performance improvement. “Consolidation” occurs later as newly learned motor skill becomes stable. 22 Cognitive learning involves the dorsolateral prefrontal cortex and posterior parietal cortex (PPC), while consolidation is mediated through a corticostriatal loop involving the striatum and supplementary motor areas. 23 Changes in motor behavior at the end of acquisition characterize motor improvement. Retention, or the automization phase, 22 requires demonstration of the new motor skill after a delay without further practice and is related to increased activity in primary motor cortex, premotor cortex, and the PPC. 23 Retention testing can reveal whether long-term or permanent changes in motor behavior due to training have occurred 24 and is essential to motor learning studies. 13 In the absence of retention testing, investigators can only identify changes in motor behavior, not whether motor learning has occurred. The transfer test evaluates the generalizability of newly learned skills and identifies if skills can be applied in a different context than that practiced during acquisition. 24 Successful performance of the learned motor skill at retention and transfer characterizes motor learning.
Motor learning can be classified as explicit or implicit. Explicit learning is conscious, requires declarative knowledge, and can be tested through recall or recognition. 4 It relies on feedback about desired motor behavioral changes brought to conscious awareness of the learner. Implicit learning is unconscious and characterized by motor skill automaticity. It relies on the provision of feedback about the result of the movement from which learners can adapt behaviors to improve subsequent movements. Determination of the most appropriate type of motor learning for people with cognitive deficits requires an understanding of the cognitive demands of explicit and implicit learning. While both explicit and implicit learning involve memory and executive function,25,26 explicit learning requires additional attentional resources. 27
Motor learning can be quantified by improvements in functional outcome measures including kinematics/kinetics (ie, endpoint performance, movement quality, and force) and clinical scales. 5 Endpoint performance is described by trajectory speed, precision, and straightness, while movement quality is described by individual joint and segment (ie, trunk) ranges, spatial and temporal inter-joint coordination, and muscle activation patterns.5,28
Previous reviews have focused on post-stroke cognitive impairments,21,29 cognitive rehabilitation, 30 and the relationship between cognitive impairments and motor recovery. 31 However, the relationship between cognitive impairments and responsiveness to training has been poorly studied, and the use of brief screening tools has been criticized as being insufficient to identify subtle cognitive impairments.21,29 Previously, in a small number of studies (n = 6), significant associations were found between executive function/attention and arm motor recovery. 31 Clarification of the role of cognitive deficits in recovery and relearning of motor skills was recommended, particularly related to specific types of motor learning and feedback. Therefore, the objective of this review was to determine the effect of cognitive impairments on motor learning in people with stroke. A scoping review was done to chart and synthesize the existing motor learning literature, as well as to identify gaps in knowledge for future studies. 32 A scoping, instead of a systematic review, was chosen because of the small number of studies in the literature. Specific goals were to determine: (1) how motor learning is studied in individuals with post-stroke cognitive impairments; (2) how cognitive impairments are assessed; (3) which cognitive domains impact motor learning. A better understanding of the role of cognitive impairments after stroke on motor learning may have practical implications for rehabilitative practice to improve sensorimotor recovery.
Methods
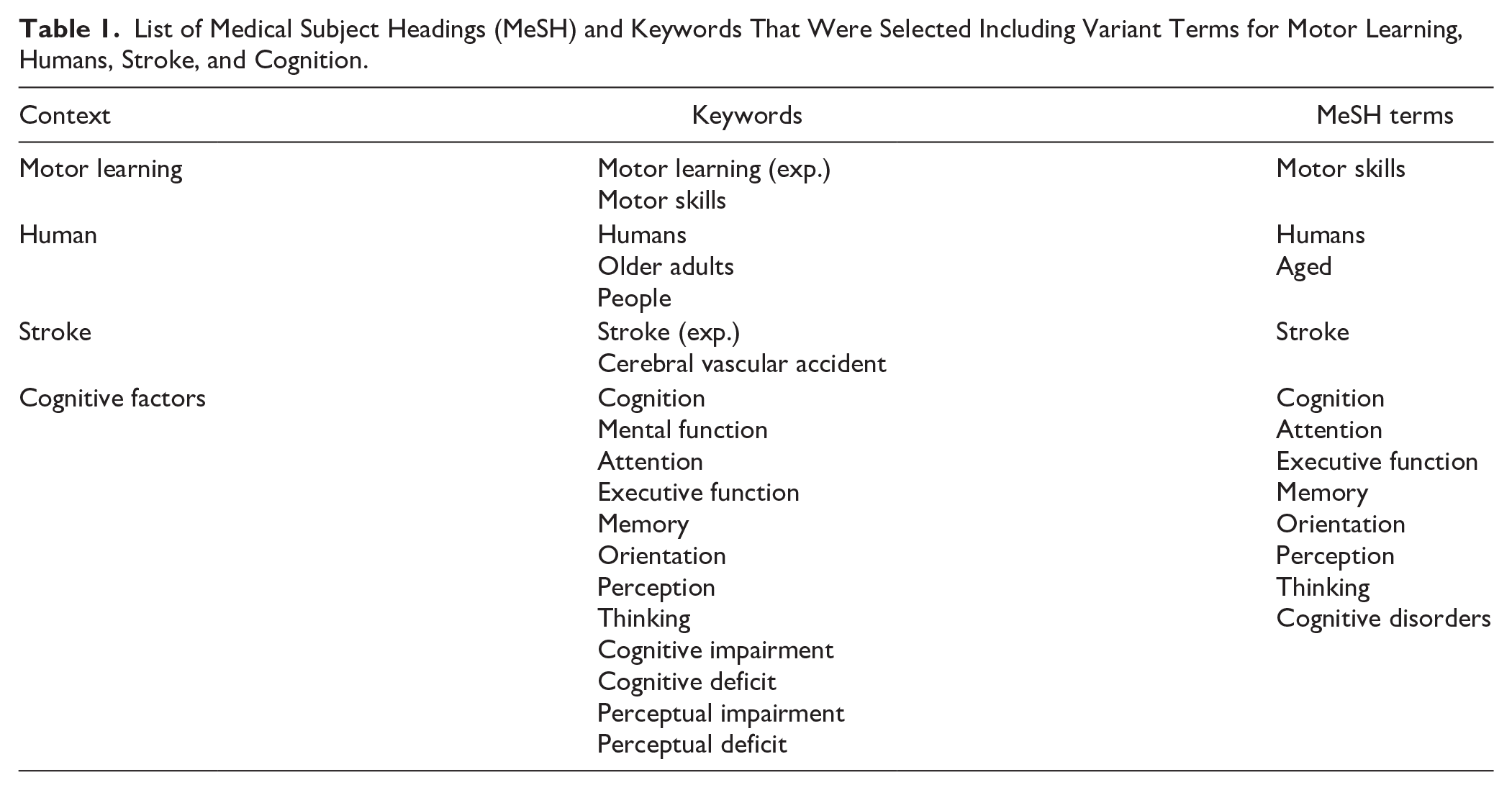
The review was conducted using the checklist for the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR 33 ), and guidelines proposed by Arksey and O’Malley, 34 Levac et al, 35 and Peters et al. 36 Literature from 4 databases up to July 2024 were searched: MEDLINE (1946-2024), Embase (1966-2024), Embase Classic (1947-2024), and PsycINFO (1967-2024; Table 1). After duplicate removal, 2 reviewers (CR, MCCL) selected studies meeting inclusion criteria based on title and abstract screening. A third reviewer (MFL) resolved conflicts, if present. Studies were included if they: (1) declared or implied that they investigated the relationship between cognitive impairments and motor learning; (2) were in English; (3) included a stroke group; (4) used a motor learning task; (5) included a control group; and (6) included a quantifiable clinical test of cognition. Studies were excluded if they: (1) involved pediatric patients; (2) included non-human participants; (3) were book chapters, dissertations, protocols, reviews, conference papers, abstracts, or case studies. Two authors (CR and KD) extracted relevant information from the studies.
List of Medical Subject Headings (MeSH) and Keywords That Were Selected Including Variant Terms for Motor Learning, Humans, Stroke, and Cognition.
One author (CR) independently evaluated the risk of bias of each study using the Newcastle-Ottawa Scale (NOS 37 ) and the Risk of Bias2 (RoB2) Tool. 38 The NOS assesses the quality of non-randomized studies in terms of design, content, and ease of use. where a score of 0 to 4 indicates a high risk of bias, and 5-6 and 7-9 refer to moderate or low risk of bias, respectively. 39 RoB2 assesses the quality of randomized trials in 5 domains: (1) randomization; (2) deviations from the intended intervention; (3) missing outcomes; (4) outcome measurement; and (5) results. 40 Studies classified with a low risk of bias must have a low rating in all domains, whereas studies classified as having some concern or a high risk of bias should have a concern or high risk in at least 1 domain, respectively. 38
Results
Search Results
Of the 450 studies identified, 334 were removed during duplicate screening, 32 by title screening, 53 by abstract screening, and 17 by full-text screening. Five studies were added to full-text screening through reference screening, resulting in 19 studies (Figure 1).
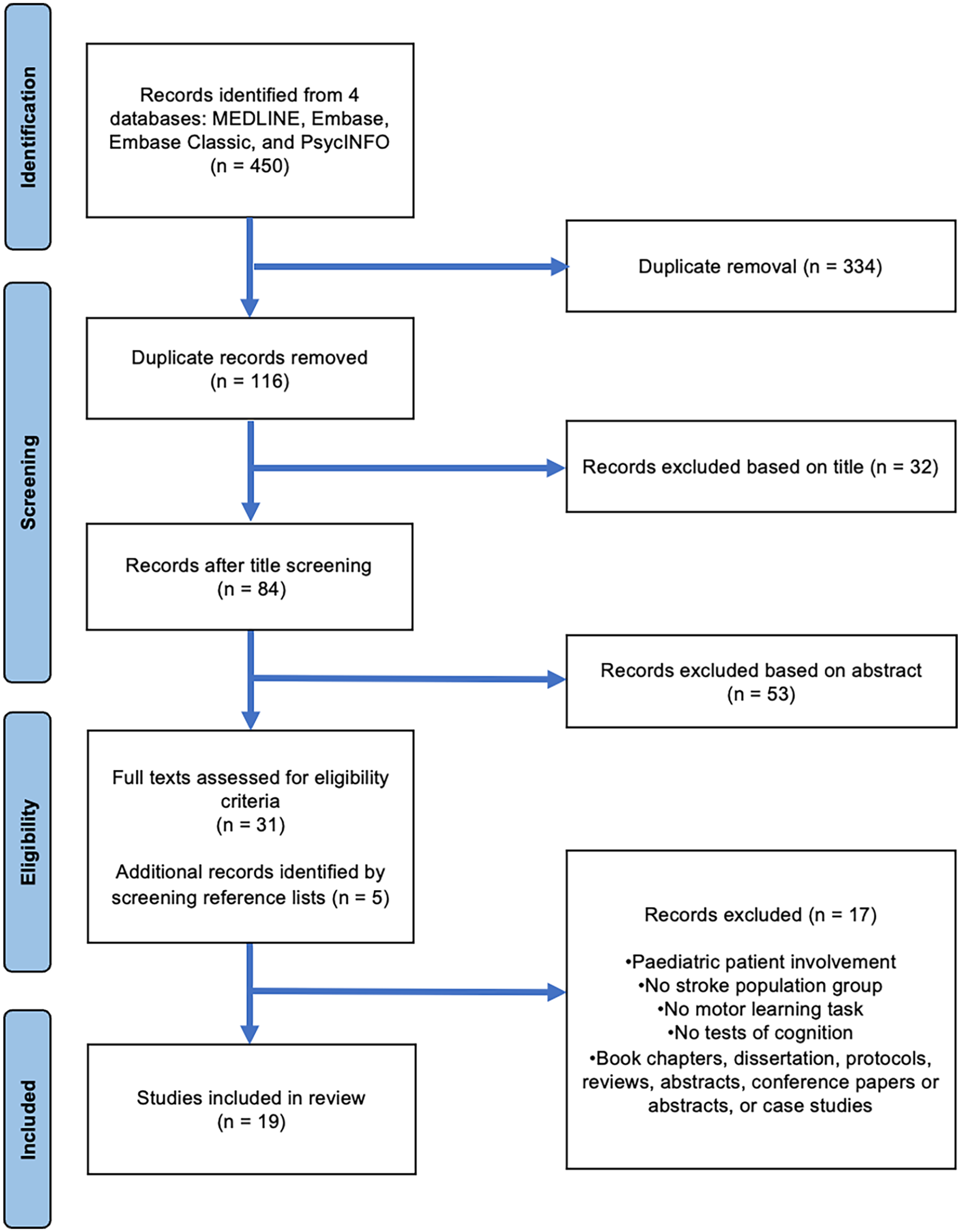
PRISMA flowchart describing the study selection process.
Characteristics of Selected Studies
Among the 19 selected studies, 7 had pre-post designs,41 -47 7 were randomized control trials (RCT),20,48 -53 3 were cross-sectional studies,54 -56 1 was a non-randomized control trial, 57 and 1 was a randomized crossover study. 58 Two studies were pilot studies.45,57 A total of 440 patients with stroke were included and sample sizes ranged from 9 to 59 subjects. Stroke chronicity varied from 6 days to 3.9 years poststroke (Table 2).
Demographic Information of Participants in Selected Studies.
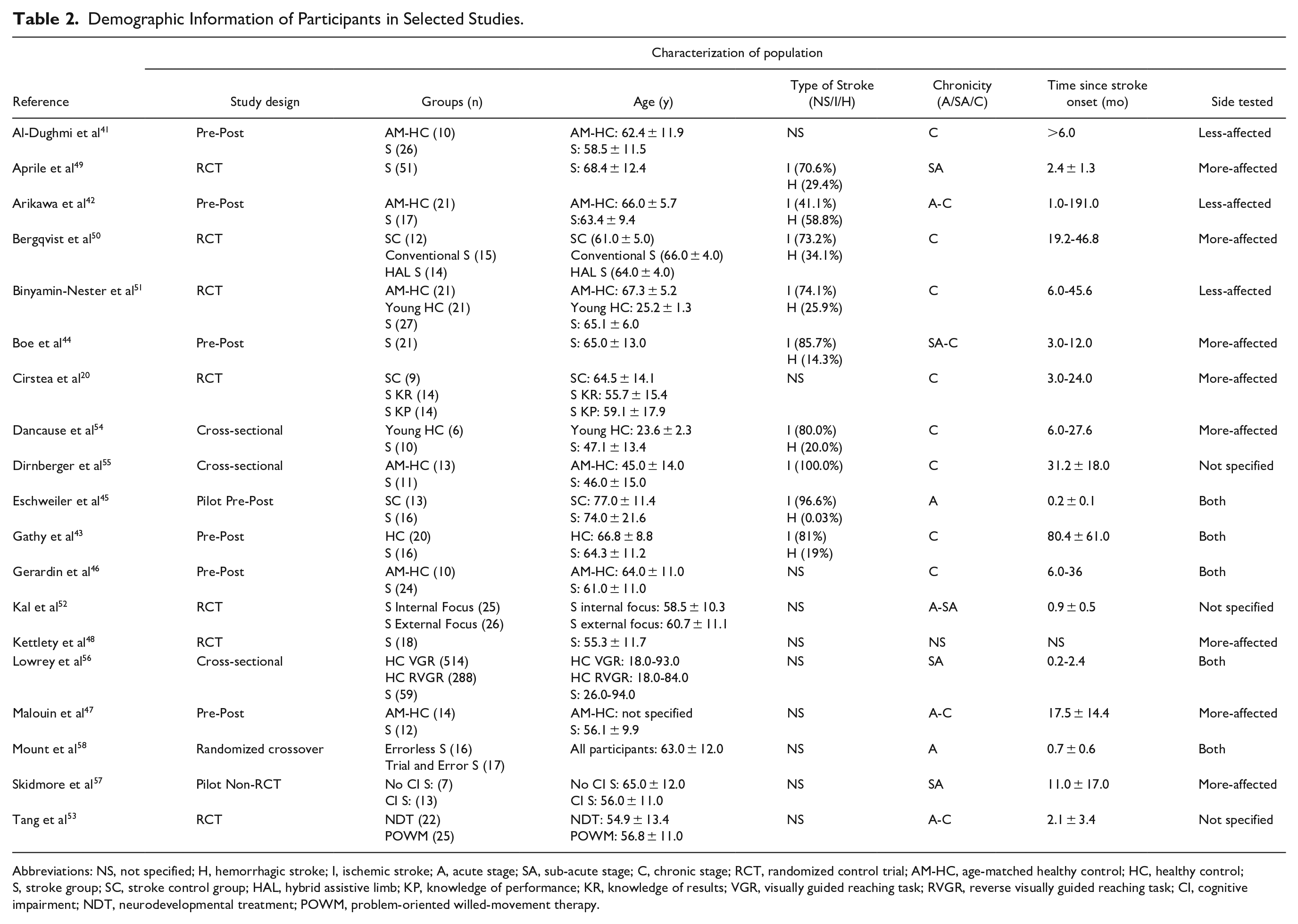
Abbreviations: NS, not specified; H, hemorrhagic stroke; I, ischemic stroke; A, acute stage; SA, sub-acute stage; C, chronic stage; RCT, randomized control trial; AM-HC, age-matched healthy control; HC, healthy control; S, stroke group; SC, stroke control group; HAL, hybrid assistive limb; KP, knowledge of performance; KR, knowledge of results; VGR, visually guided reaching task; RVGR, reverse visually guided reaching task; CI, cognitive impairment; NDT, neurodevelopmental treatment; POWM, problem-oriented willed-movement therapy.
Methodological Quality
Tables 3 and 4 describe the methodological quality of the included studies. Based on the NOS, none of the non-randomized studies had high risk of bias. Three studies had a moderate risk, and the remaining 9 had a low risk. Based on the RoB2, 1 study had a high risk of bias, 1 study had some concerns, and the remaining 4 RCTs had a low risk.
Methodological Quality of Selected Studies Based on the Newcastle-Ottawa Scale (NOS).
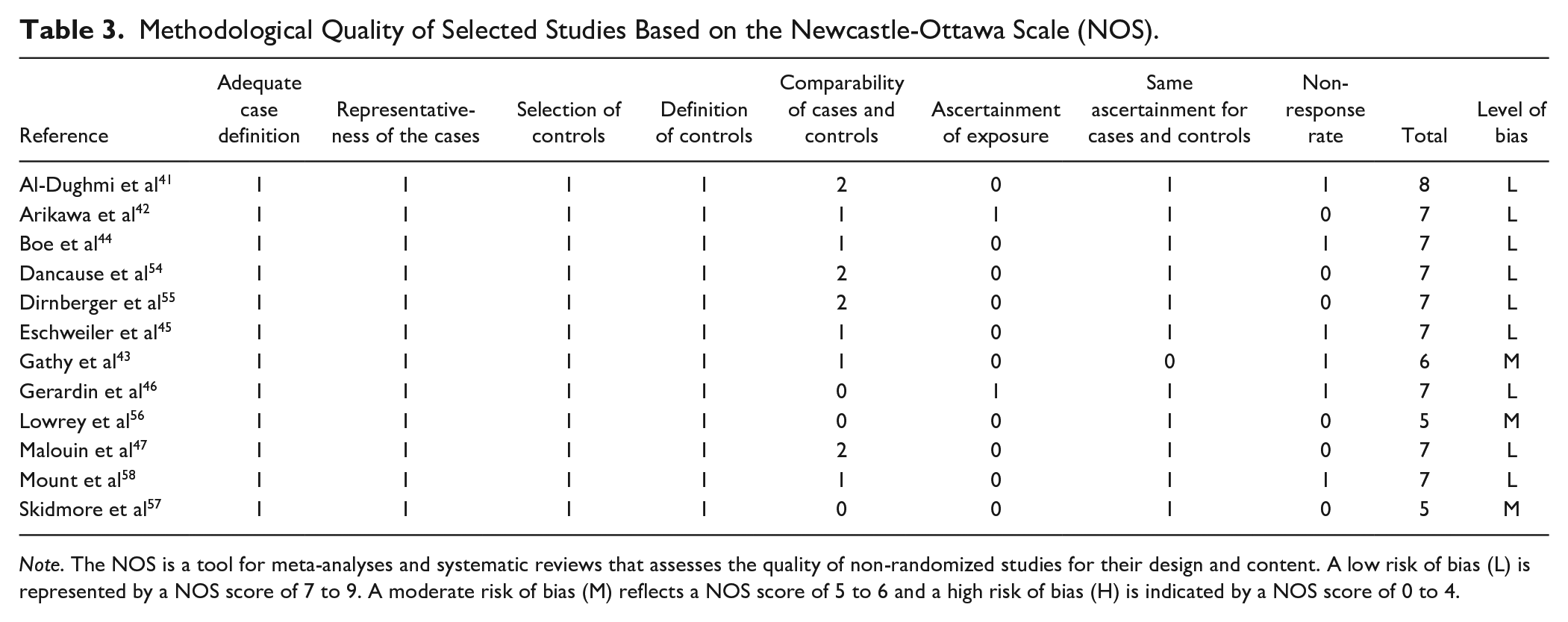
Note. The NOS is a tool for meta-analyses and systematic reviews that assesses the quality of non-randomized studies for their design and content. A low risk of bias (L) is represented by a NOS score of 7 to 9. A moderate risk of bias (M) reflects a NOS score of 5 to 6 and a high risk of bias (H) is indicated by a NOS score of 0 to 4.
Methodological Quality of Selected Studies Based on the Risk of Bias 2 (RoB 2) Tool.
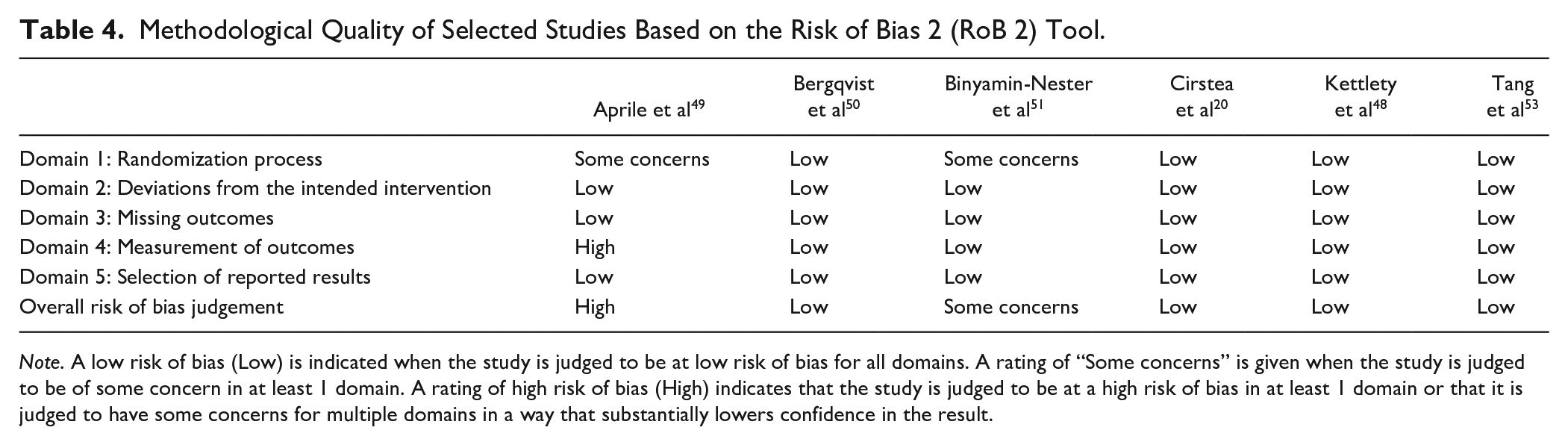
Note. A low risk of bias (Low) is indicated when the study is judged to be at low risk of bias for all domains. A rating of “Some concerns” is given when the study is judged to be of some concern in at least 1 domain. A rating of high risk of bias (High) indicates that the study is judged to be at a high risk of bias in at least 1 domain or that it is judged to have some concerns for multiple domains in a way that substantially lowers confidence in the result.
Methodologies Used for Studying Motor Learning in Individuals With Post-Stroke Cognitive Impairments
Nine studies addressed motor improvement since they did not include a retention or transfer test43,45,46,48,49,53 -56 and 10 were true motor learning studies.20,41,42,44,47,50 -52,57,58 Amongst the 9 motor improvement studies, 4 examined implicit,43,46,57,58 and 5 examined explicit learning45,47,48,53,54 (Table 5). Amongst the 10 motor learning studies, 2 examined implicit,41,52 and 4 examined explicit learning.44,47,50,57 The remaining 4 studies examined both implicit and explicit learning20,42,51,58 (Table 5).
Characteristics of Selected Studies: Methodological Design and Outcome Measures.
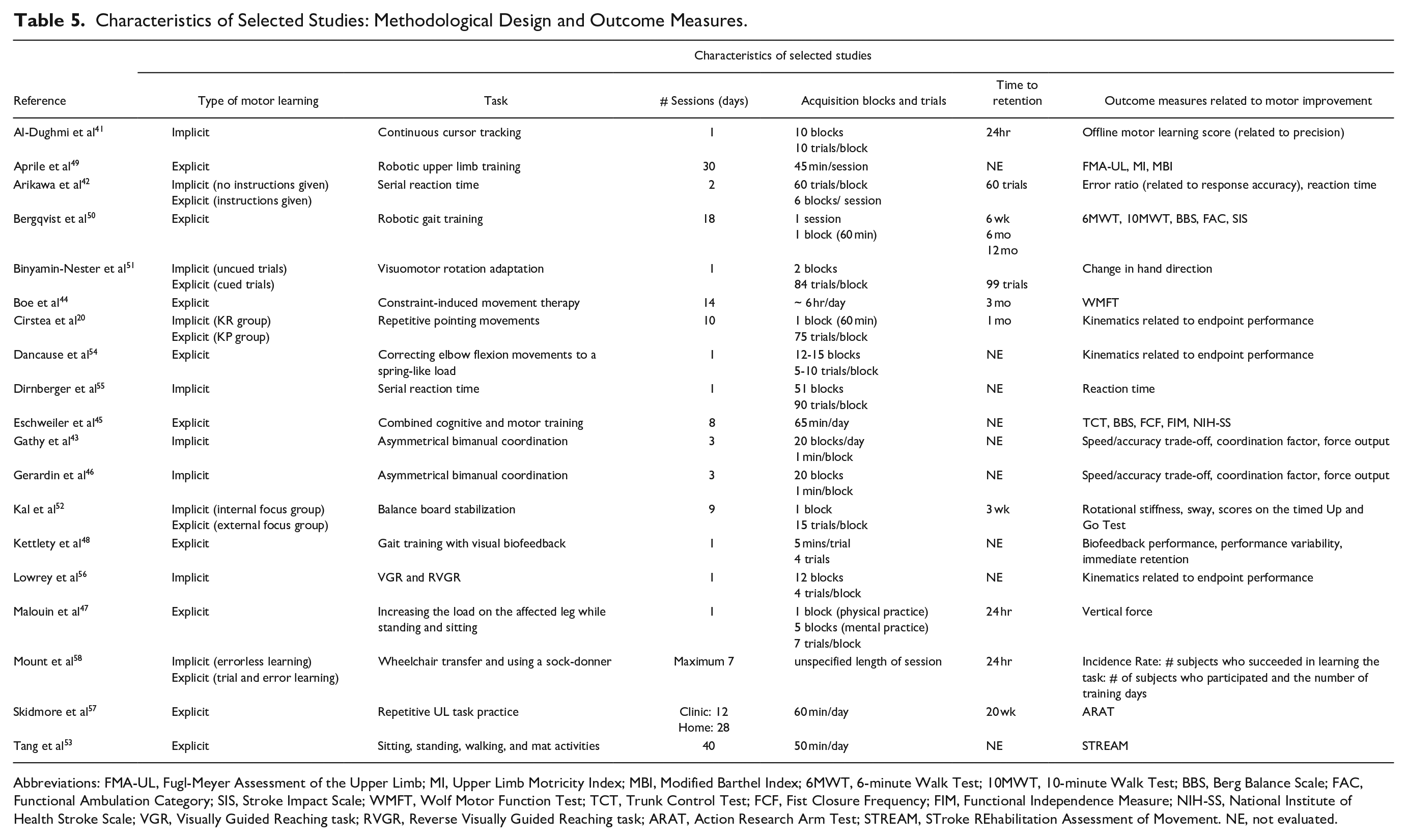
Abbreviations: FMA-UL, Fugl-Meyer Assessment of the Upper Limb; MI, Upper Limb Motricity Index; MBI, Modified Barthel Index; 6MWT, 6-minute Walk Test; 10MWT, 10-minute Walk Test; BBS, Berg Balance Scale; FAC, Functional Ambulation Category; SIS, Stroke Impact Scale; WMFT, Wolf Motor Function Test; TCT, Trunk Control Test; FCF, Fist Closure Frequency; FIM, Functional Independence Measure; NIH-SS, National Institute of Health Stroke Scale; VGR, Visually Guided Reaching task; RVGR, Reverse Visually Guided Reaching task; ARAT, Action Research Arm Test; STREAM, STroke REhabilitation Assessment of Movement. NE, not evaluated.
Motor Task
Four motor improvement studies used a virtual environment to practice serial reaction time, 55 asymmetrical bimanual coordination,43,46 or visually guided reaching, 56 and 1 study evaluated elbow flexion error corrections. 54 In 4 other motor improvement studies, training involved a novel approach such as robotic upper limb training, 49 combined cognitive and motor training, 45 problem-oriented willed-movement therapy, 53 or gait training with visual biofeedback. 48
Three motor learning studies included a motor task in a virtual environment in which participants practiced a serial reaction time, 42 continuous cursor tracking 41 or visuomotor rotation adaptation tasks. 51 Seven studies required participants to practice different activities including robotic gait training, 50 repetitive reaching,20,44,57 balance board stabilization, 52 affected leg loading, 47 wheelchair transfers, and using a sock-donner. 58
Outcome Measures
In all motor improvement studies, all patients improved in the motor task, regardless of cognitive status. Six studies used endpoint kinematic measures43,46,48,54 -56 and 3 used clinical scores to describe motor improvement.45,49,53
Four motor learning studies evaluated endpoint kinematics derived from motion analysis technology 20 or the training program,41,42,51 while 2 evaluated force output.47,52 One study used a ratio describing successful learning 58 and 3 reported clinical scores.44,50,57
Acquisition
Four motor improvement studies consisted of 1 practice day,48,54 -56 while in the remaining studies, practice ranged from 3 to 40 days.43,45,49,52 Although 7 studies specified the type and delivery of feedback used,43,46,48,49,51,54,56 none compared different feedback types.
Four motor learning studies involved 1 practice day.41,42,47,51 The remaining 6 studies included 7 to 40 practice days.20,44,50,52,57,58 Three studies specified how feedback was delivered, 58 and 2 of these compared effects of different feedback types on motor learning.20,52 Motor and clinical improvements after reaching training with Knowledge of Performance (KP) feedback about upper limb movement patterns were related to better memory, mental flexibility, and planning. 20 However, all patients with stroke, regardless of cognitive status, benefitted from Knowledge of Results (KR) feedback about reaching precision. Similarly, patients with severe attention deficits training on a balance board task benefitted more from KR feedback about movement outcome than KP feedback on movement patterns.
Retention
Most motor learning studies had 1 follow-up (90%) while 1 study included 3 follow-up assessments (10%). 50 The time to the retention test was related to the acquisition phase duration, varying from a short 10-minute washout to 6 months post-acquisition.
Assessment of Post-Stroke Cognitive Impairments
Studies used a variety of reliable and valid cognitive measures (Table 6). Most motor improvement studies assessed multiple cognitive domains (55.0%), while the remaining 44.0% assessed global cognition with 1 assessment tool.46,49,53,56 The most frequently used tool was the Montreal Cognitive Assessment (MoCA; 50.0%), followed by the Mini Mental State Examination (MMSE; 25.0%), and the Oxford Cognitive Screening test (OCS; 25.0%).
Characteristics of Selected Studies: Cognitive Assessments and Relation to Motor Learning.
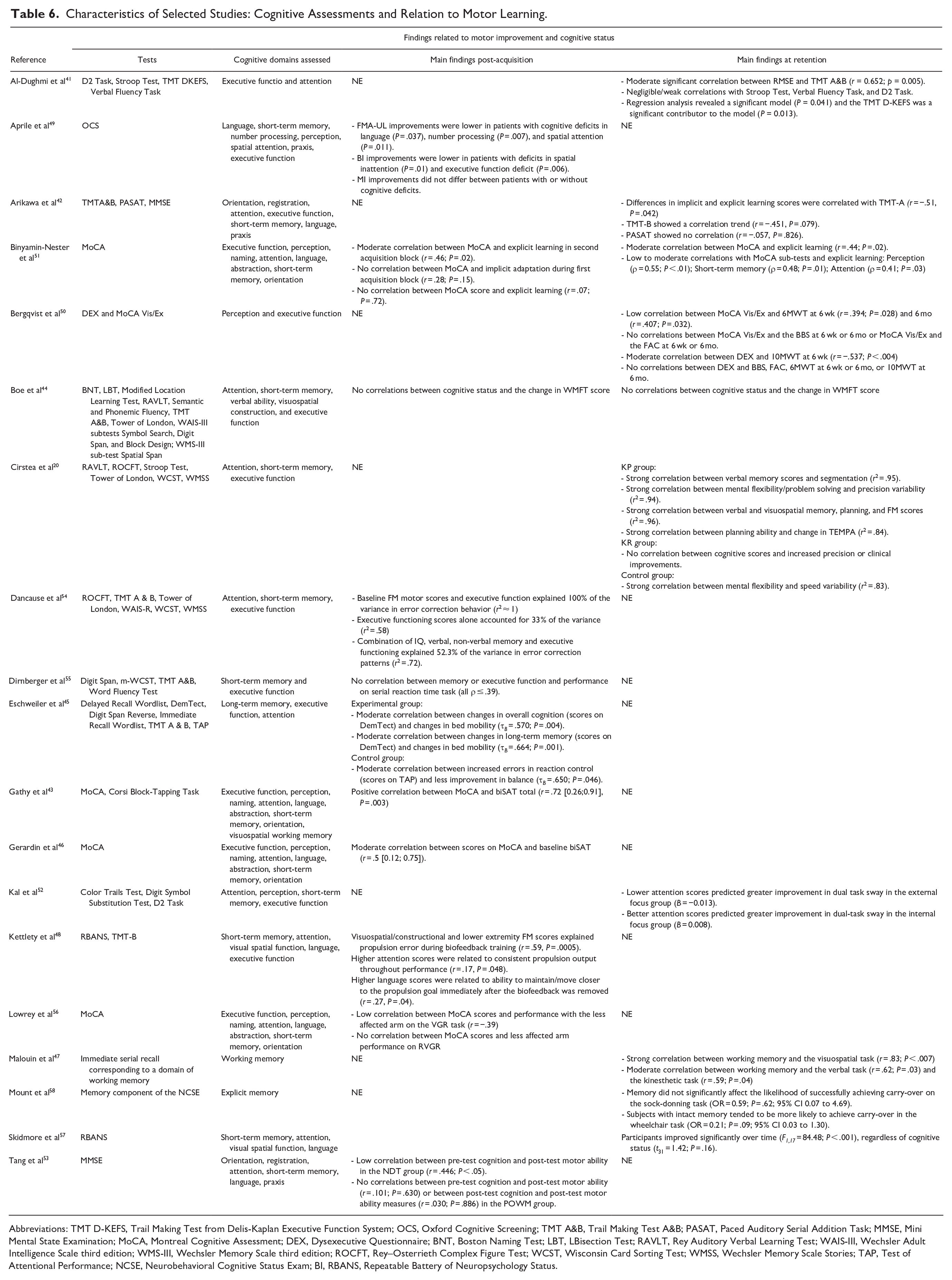
Abbreviations: TMT D-KEFS, Trail Making Test from Delis-Kaplan Executive Function System; OCS, Oxford Cognitive Screening; TMT A&B, Trail Making Test A&B; PASAT, Paced Auditory Serial Addition Task; MMSE, Mini Mental State Examination; MoCA, Montreal Cognitive Assessment; DEX, Dysexecutive Questionnaire; BNT, Boston Naming Test; LBT, LBisection Test; RAVLT, Rey Auditory Verbal Learning Test; WAIS-III, Wechsler Adult Intelligence Scale third edition; WMS-III, Wechsler Memory Scale third edition; ROCFT, Rey–Osterrieth Complex Figure Test; WCST, Wisconsin Card Sorting Test; WMSS, Wechsler Memory Scale Stories; TAP, Test of Attentional Performance; NCSE, Neurobehavioral Cognitive Status Exam; BI, RBANS, Repeatable Battery of Neuropsychology Status.
Most motor learning studies used a valid and reliable cognitive test battery to measure multiple cognitive domains (80%), while the remaining studies used either the MoCA 51 or a portion of the Neurobehavioral Cognitive Status Exam to test memory. 58
In all of the included studies, the cognitive domains assessed were executive function (eg, mental flexibility, planning, and problem-solving), attention (eg, processing speed, spatial attention, and reaction control), language, memory (eg, working, short-term, long-term, verbal, kinesthetic, and visuospatial), visuospatial perception, praxis, and orientation.
Cognitive Domains Impacting Post-Stroke Motor Improvement and Learning
Seven cognitive domains were examined across the studies (Table 6). Overall, memory was the most frequently assessed (89.5%), followed by attention (78.9%), and executive function (73.7%). Specific types of memory assessed, included short-term,20,42 -44,46,48,49,51,54 -57 long-term, 45 working, 47 and explicit. 58 Two studies focused specifically on memory,47,58 while the remaining studies included a variety of domains to encompass global cognition and included 2 to 6 cognitive domains.
Six motor improvement studies used correlations to determine if cognitive scores were related to motor ability,43,45,46,53,55,56 while 2 studies used multiple regression analysis.47,48 One study 49 directly compared scores on cognitive and clinical scales. Seven studies found significant relationships between cognitive status and motor performance.43,45,48,49,53,54,56 General cognitive status was related to improvement on a motor ability scale following neurodevelopmental treatment in patients with varying chronicity (MMSE × Stroke Rehabilitation Assessment of Movement: r = .47, P < .05 53 ). However, in the same study, MMSE scores were not related to motor improvement when training with problem-oriented willed-movement therapy (r = .10, P = .63 53 ). General cognitive status was also related to improved bed mobility in acute patients receiving combined cognitive and motor therapy (DemTect × Trunk Control Test [TCT]: t = 0.57, P = .004 45 ), improved performance on a visually-guided reaching task using the more-affected arm in sub-acute patients (MoCA: r = −.39, P < .05 56 ), and improved bimanual motor skill learning in chronic patients (MoCA: r = .72, P = .003 43 ) . Eschweiler et al 45 also determined that improvements in bed mobility were related to long-term memory (DemTect × TCT: t = 0.66, P = .001). Aprile et al 49 demonstrated that patients with sub-acute stroke and cognitive deficits had reduced gains in upper limb impairment scores (Fugl-Meyer Assessment of the Upper Limb [FMA-UL]) and activities of daily living and mobility (modified Barthel Index [mBI]) after robotic upper limb training compared to patients without cognitive deficits. Reduced gains were particularly prevalent in patients with deficits in spatial attention (mBI: P = .010; FMA-UL: P = .011), executive function (mBI: P = .006), language (FMA-UL: P = .037), and number writing (FMA-UL: P = .007). However, there were no differences between patients with and without cognitive impairments in improvements of muscle strength (OCS × Upper Limb Motricity Index: P = .133-0.886). Dancause et al 54 observed that chronic patients with moderate motor disability and executive function deficits used atypical movement strategies when correcting elbow flexion movement errors (Wisconsin Card Sorting Test & Tower of London × FMA-UL). Kettlety et al 48 noted that visuospatial/constructional skills, in combination with motor impairment, were associated with performance (repeatable battery of neuropsychology status [RBANS] × Fugl-Meyer Assessment of the Lower Limb × paretic leg propulsion error) during biofeedback training on a treadmill (r = .59, P = .0005) attention was associated with performance variability (RBANS × propulsion output: r = .17, P = .048), and language was related to use of visual biofeedback during the retention test (RBANS × propulsion maintenance: r = .27, P = .04). The remaining 2 motor improvement studies found no significant interactions between cognitive scores and changes in motor behavior in chronic patients.46,55
Four of the 10 motor learning studies42,44,47,51 used simple correlations to analyze the relationship between cognition and motor learning, while 5 used multiple regression analysis20,41,50,52,58 and Skidmore et al 57 directly compared performance in participants with and without cognitive deficits. 57 Eight studies found significant relationships between cognition and motor learning. Global cognition was related to motor learning in an explicit learning visuomotor rotation adaptation task in patients with chronic stroke (MoCA: r = .44, P = .020 51 ), while it was not related to changes in an implicit task (MoCA: r = .28, P = .150 51 ). Global cognition was also not related to performance after constraint-induced movement therapy 44 or robotic gait training 50 but was related to deficits on the 6-metre walk test after conventional gait training in chronic patients (MoCA: 6-week follow-up: r = .39, P = .028; 6-month follow-up: r = .41, P = .032 50 ). Executive function was related to motor learning during a continuous cursor tracking task in patients with chronic stroke (Trail-Making Test: r = .65, P = .013 41 ). Working memory was related to loading on the more-affected leg with mental imagery in patients with varying chronicity (visuospatial: r = .83, P < .007; verbal: r = .62, P = .03; kinesthetic: r = .59, P = .04 47 ). Differences in learning between implicit and explicit conditions were related to attention (TMT-A: r = −.51, P = .042), but not to executive function (TMT-B: r = −.45, P = .826 42 ) in a serial reaction time task.
Two motor learning studies found that cognitive deficits were related to decreased motor learning when training with movement quality-related feedback. Cirstea et al 20 found that decreased movement segmentation (r2 = .95) and decreased precision variability (r2 = .94) were related to verbal memory (b = 1.52) and executive function, specifically mental flexibility (b = −1.46) and planning (b = −0.65) in chronic stroke. Greater improvements in FMA-UL (r2 = .96, P < .050) and the Upper Extremity Function Test for the Elderly (TEMPA, r2 = .84, P < .050) were related to deficits in verbal (FMA-UL: b = −0.86) and visuospatial memory (FMA-UL: b = −1.85) and executive function (planning × FMA-UL: b = 0.71; planning × TEMPA: b = −0.88). Deficits in attention predicted motor performance with either an external or internal focus of attention (D2 Attention Test: Wald χ2 = 7.843, P = .049, external focus: b = −0.013, internal focus: b = 0.008) in acute patients. 52 The remaining 2 motor learning studies found no significant interactions between cognitive scores and changes in motor learning on any outcome measure in patients with varying chronicity.44,57
Overall, in the motor improvement studies, executive function49,54 and memory (short-term and verbal 54 and long-term 45 ) were most often related to motor improvement. In the motor learning studies, executive function20,41,50 and memory (verbal, 20 working, 47 and short-term 51 ) were most often related to motor learning. Attention was related to both motor improvement and learning.49,51,52,54 The specific cognitive domain that may impact or predict motor performance was not specified in 6 of the improvement/learning studies making it difficult to identify which cognitive domains influenced motor outcomes.
Discussion
Evidence of the association between cognitive impairments and motor learning after stroke is summarized. Most studies had a low risk of bias and studies used a variety of experimental designs, outcome measures, and motor tasks, with sample sizes ranging from 9 to 59 patients. The most common cognitive domains assessed were memory and executive function, with short-term memory evaluated most often. Overall, results suggest memory and executive function deficits impair motor learning, especially when the task involves intrinsic feedback. However, due to inconsistent motor learning experimental designs and small sample sizes, conclusions about motor learning should be considered preliminary.
Association Between Specific Cognitive Domains and Motor Learning
Six studies used general cognitive screening tools such as the MoCA and MMSE to identify cognitive deficits. Both tools screen for global cognition, although MoCA is more sensitive to detecting cognitive impairments than MMSE. 59 General screening tools are thought to be insufficiently detailed to provide insights about an individual’s specific cognitive impairments21,60 and should mainly be used to identify whether further diagnostic testing is indicated.
A few studies indicated that attention deficits contributed to motor learning difficulties related to recovery. A previous meta-analysis found a moderate association between sensorimotor recovery and executive function and a weak association between recovery and attention. 31 However, memory and recovery were not related. In contrast, there were strong associations between memory and improvement in arm activity scores based on clinical scales (eg, Hyndman et al 61 ). The discrepancy may be related to populations studied (ie, acute stroke 61 and chronic stroke 31 ).
Studies that found no relationships between cognitive status and motor learning used scores on clinical scales to identify learning (eg, Wolf Motor Function Test [WMFT] 44 and Action Research Arm Test [ARAT] 57 ). Both WMFT and ARAT are valid and reliable upper limb activity scales. However, they do not specifically differentiate between true motor recovery and compensations since scores are mostly based on task success, without accounting for movement quality. 28 Kinematics objectively measure changes in movement patterns that can identify movement quality,62,63 and may be more sensitive to detecting associations between cognition and motor learning. 20 However, movement quality indicators were absent from the reviewed studies. In a conference proceeding, Subramanian et al 64 examined the influence of post-stroke cognitive impairments on the use of motor-related feedback to improve reaching in a 3D virtual environment and a similar physical environment. Patients with stroke in the physical group with better memory and problem-solving improved endpoint movement speed, shoulder flexion, and elbow extension ranges while pointing to a target. Improvements in endpoint and movement quality outcomes were related to better visuospatial memory, problem-solving, and cognitive flexibility.
Two studies did not find any relationship between cognitive status and motor improvement using reaction times 55 or speed/accuracy trade-off of a reaching movement. 46 However, these studies did not measure improvements on clinical scales, making it difficult to relate kinematic outcomes to functional improvements.
Motor Outcomes
Most studies used reliable and valid clinical scales to measure motor improvement during acquisition. Studies that reported kinematic variables focused only on endpoint performance without characterizing limb movement patterns. Thus, they did not distinguish between true motor recovery and compensation at the movement quality level.5,28 Future studies should focus on this distinction, since improving movement with motor compensations can lead to learned disuse or reinforcement of undesirable movement patterns that may interfere with true motor recovery. 65
Types of Motor Learning
Most studies used either implicit or explicit learning, while 5 studies incorporated both types of learning. These studies found that deficits in attention, 42 executive function and memory, 20 or global cognition indicated by a low MoCA score 51 were related to the use of explicit, but not implicit learning. These results are consistent with previous studies66,67 that suggested that explicit information impeded motor learning in post-stroke patients with cognitive deficits, while patients were able to retain the learned motor skill longer when acquired implicitly.
The patients in the included studies generally had cortical/sub-cortical stroke. Specific types of learning can be impacted by lesions in different brain areas (eg, basal ganglia for implicit learning67,68). For example, patients with stroke affecting different brain areas and cognitive processes may have difficulty with implicit learning when explicit instructions are provided.67,68
Feedback
Less than half of the included studies specified the type and delivery of feedback used during training. This is important because there is a variety of feedback types available to optimize motor learning. 69 Consideration of the type and delivery of feedback is necessary since cognitive impairments may affect the ability to detect and integrate new movement information as changes in the task or environment arise 20 and to store and retrieve relevant information. 54 This may be especially prevalent in those with deficits related to short-term memory. 70 Kal et al 52 found that patients with lower attention scores had greater improvements in task performance when extrinsic feedback was provided, while patients with better attention scores benefitted more from intrinsic feedback.
Individuals with post-stroke cognitive impairments, particularly in short-term memory and attention, may benefit more from extrinsic feedback to learn a new motor task. 71 This and previous sections suggest that motor learning studies should consider lesion location as well as the type of learning and feedback to provide a better understanding of the relationship between lesion location, cognitive deficits, and motor learning. 72
Retention Testing
Studies used a variety of delays for retention testing (ie, next day41,47,58 to 6 months 50 ). The extent to which the learner retains improvement over the retention interval reflects the strength of learning and motor skill memory. 73 Retention and transfer tests should be conducted at least 24 hours after practice for motor memory consolidation. 24 If retention and transfer tests are conducted too early, increased fatigue and decreased motivation may affect results.
Generally, motor learning studies found that patients with post-stroke cognitive impairments particularly with explicit learning and using intrinsic feedback had fewer training gains compared to those without cognitive impairments. Although the included studies purported to measure motor learning, only 10 of 19 studies used retention testing such that information about the effectiveness of learning should be interpreted with caution.43,45,46,48,49,53 -56
Clinical Implications
Executive function and memory were related to functional motor performance in most studies. Cognitive impairments after stroke can profoundly influence the effectiveness of sensorimotor training and quality of life. 74 The ability to understand and remember instructions, plan and initiate self-directed activities, and solve problems is impacted by cognitive impairments. Individualized treatment interventions considering the patient’s cognitive deficits may improve intervention effectiveness. A detailed cognitive assessment can inform clinicians how to instruct their patient during training. For example, patients with memory deficits may struggle with a task requiring multiple sources of information. In addition, based on age-related declines in working memory, patients may have difficulty maintaining and manipulating information from a complicated motor task. 75 Our results suggest that patients with cognitive deficits may benefit more from training using implicit learning and that the most effective feedback delivery may differ for people with different cognitive deficits. For example, memory and executive function scores correlated with using KP feedback to improve motor and clinical scores in people with chronic stroke. 20 These cognitive processes are likely important for integrating movement-related information to adapt movements to task constraints. Therefore, patients with executive function and/or memory deficits would likely have problems using KP feedback for motor learning. However, there were no correlations between cognitive scores and improvements in endpoint precision which may be related to KR feedback requiring fewer cognitive resources. 20 This suggests that clinicians should consider emphasizing KR over KP feedback for motor learning in post-stroke individuals with cognitive impairments.
Limitations
While the results shed light on which cognitive impairments impact motor learning after stroke, recommendations should be carefully considered due to the small number of included studies and the variability in methodologies. Several studies had small sample sizes (Table 2), making it difficult to interpret results. Furthermore, few studies used retention testing making it difficult to generalize results to the greater stroke population. We did not compare motor learning in patients of different genders or having different levels of chronicity, separately for the affected versus unaffected limb, the upper and lower limbs, or tasks involving different levels of cognitive load. The suggestion that more visuospatial cognitive resources may be required for upper limb training 21 requires further investigation. Other limitations are that the protocol was not prospectively registered, and that risk of bias assessments were evaluated by only 1 author.
Directions for Future Research
A better understanding of the relationship between cognition and motor learning after stroke is fundamental for improving sensorimotor recovery. Cognitive status and study design should be considered when designing interventions for sensorimotor recovery in people with stroke. Future studies should consider experimental designs with retention testing, using a combination of outcome measures including clinical scales and kinematics/kinetics, different cognitive loads on learning, and identification of specific cognitive impairments. As well, studies on the use of KR versus KP feedback may inform clinicians about how to provide feedback during training interventions for patients with cognitive deficits. Further studies about implicit learning and feedback related to endpoint movement (KR) or movement quality (KP) are needed to fully understand the relationship between the provision of KR versus KP feedback and motor learning for patients with post-stroke cognitive deficits.
Footnotes
Acknowledgements
We would like to thank Maria do Carmo Correia de Lima for her help in conducting the literature search and initial screening process.
Author Contributions
Caroline M. Rajda: Conceptualization; Data curation; Formal analysis; Methodology; Resources; Writing—original draft; Writing—review & editing. Katrina Desabrais: Formal analysis; Writing—review & editing. Mindy F. Levin: Conceptualization; Formal analysis; Methodology; Project administration; Resources; Supervision; Validation; Writing—review & editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.