
Abstract
Background
Stroke survivors are one of the largest consumer groups of rehabilitation services. Despite improvement in daily activities while in inpatient rehabilitation, many have difficulty performing daily activities at home after discharge. The difference in performance between a standard clinical context and at home is poorly understood.
Objective
To better understand differences in activity performance during transition from inpatient rehabilitation facility (IRF) to home, we examined daily activity performance scores from 2 different environments (IRF and home) at the same time point (discharge).
Methods
This was a cross-sectional analysis using baseline data from a randomized controlled trial. Participants were stroke survivors aged ≥50 who planned to discharge home from the IRF. The Functional Independence Measure and Section GG codes (both converted to International Classification of Functioning, Disability, and Health scores) were conducted per protocol first at home and then in the IRF at discharge (≤3 days apart, order not randomized).
Results
Among 57 participants, activity scores at home were significantly worse than scores at IRF discharge. Over 40% of participants had discharge scores indicating no-to-mild impairment for shower/tub transfer, walking, and going up/down stairs, while home visit scores indicated moderate-to-complete impairment for those activities. The greatest differences in scores were for shower/tub transfer (median difference 1.5, 95% CI 1.00-2.00) and going up/down stairs (median difference 1.50, 95% CI 1.00-2.00).
Conclusion
The environment plays an important role in stroke survivors’ functioning at home. Future studies should further examine how the environment impacts activity performance upon returning home following stroke.
Introduction
Stroke is a leading cause of long-term disability in the US, with over 795 000 people experiencing a stroke each year. 1 Approximately two-thirds of stroke survivors experience motor or sensory impairments, difficulties with language, impaired cognition, increased depression and anxiety, or emotional lability, which can lead to difficulties completing daily activities in the home and community.2,3 Stroke survivors are one of the largest consumer groups of post-acute rehabilitation services, with approximately 25% of stroke survivors discharging to an inpatient rehabilitation facility (IRF) to improve their daily activity performance and community participation.4-6 The goal of an IRF is to improve independence in activities of daily living (ADLs; eg, walking, going up and down stairs, and bathing).5,7-9 Stroke survivors who are more independent in daily activities are more likely to discharge home rather than a long-term care facility, with the expectation that higher levels of independence in daily activities in the IRF would translate similarly to greater independence at home.9,10
Despite progress made in performing daily activities while in an IRF, many stroke survivors have difficulty with the transition home after discharge. Stroke survivors report having difficulty completing activities at home, and their caregivers often feel ill-prepared to support them. 11 Some stroke survivors report returning home and waiting 6 to 12 months before resuming daily activities such as bathing, getting dressed, and cooking. 12 For those who do resume their daily activities, over 50% still report difficulty at 1 year, which can lead to poor outcomes such as falls and rehospitalization.13,14 Within the field of rehabilitation, the measurement of functioning has been dominated by measures of capacity. Capacity is defined as what is possible in an ideal situation15,16 as opposed to the enacted or lived experience, in this case daily participation in the individual’s own home environment. Therapists in rehabilitation generally conduct gold-standard performance-based assessments of daily activities in the rehabilitation facility. Often, because of administrative barriers, therapists are not able to conduct performance-based assessments in an individual’s home prior to discharge. The difference in performance-based daily activity assessments conducted in the IRF compared to the home environment is unknown. The discordance between what an individual can do in a standard clinical context compared to what they could do at home with potentially high levels of environmental barriers is poorly understood but could explain the challenge many survivors have transitioning home after rehabilitation.
To address this gap in our understanding of the influence of difference in environment on performance-based ADL assessment during the transition home from IRF, we examined the daily performance of stroke survivors at the time of discharge from an IRF in the facility and also in the home. We hypothesized that there would be a difference between capacity scores (measured in a standard environment) and participation scores (measured in the real world).
Methods
Design
In this cross-sectional study, we capitalized on data collected as a part of an ongoing randomized controlled trial (RCT), the Community Participation Transition After Stroke (COMPASS) study. 17 COMPASS examines the efficacy and safety of a rehabilitation program designed to reduce barriers to independent living in the community for stroke survivors during the transition from an IRF to home. All study procedures were approved by the Human Research Protection Office at Washington University in St. Louis (IRB# 201705047), and all participants provided written informed consent.
Participants
Inclusion criteria for the RCT were used for this sub-study. Participants were recruited while inpatient at an IRF in St. Louis, Missouri. Participants were included if they were 50 years of age or older, diagnosed with an acute ischemic stroke or intracerebral hemorrhage, independent in ADLs prior to stroke (premorbid Modified Rankin Scale score ≤2 18 ), and planned to discharge home (determined by conversations with the IRF case manager or therapy team). Participants were excluded if they had a life expectancy of less than 6 months, had significant cognitive impairment (Short Blessed Test score >10 19 ), had moderate-to-severe aphasia (National Institutes of Health Stroke Scale best language score of ≥2 20 ) indicating communication problems that could prevent study completion, lived more than 60 miles from St. Louis, or planned to discharge to an institutional setting. A total of 185 participants were randomized to treatment (n = 85) or control (n = 100).
Procedures
Details of the study have been published. 17 In brief, all study participants completed a home visit while in the IRF. Participants traveled to their home with a study occupational therapist. The occupational therapist rated the participant’s level of independence in completing daily activities in the home and made recommendations for home modifications for those randomized to the intervention group. For this study, we selected participants with home visits completed within 3 days of discharge, the same timeframe during which IRF staff occupational and physical therapists rated participants’ levels of independence in daily activities in the IRF as part of standard discharge procedures. The IRF discharge assessment occurred either on the day of discharge or the day prior. The similar timeframe provided an opportunity to explore the difference in performance-based daily activity assessments in the home versus the IRF. The order of the assessments in this study was not randomized. The standardized protocol specified that home visit assessments be conducted prior to IRF discharge assessments.
Measures
Basic demographic information, including age, gender, race, years of education, comorbid conditions (including depression), and type of stroke, were collected. Level of independence in performing daily activities was assessed using The Functional Independence Measure (FIM™). The FIM is a widely used and reliable measure to assess daily activity performance in acute and post-acute care settings among individuals with disability. The FIM measures self-care, sphincter control, transfers, locomotion, communication, and social cognition. 21 FIM scores range from 7, indicating complete independence with the activity, to 1, indicating the need for total assistance to complete the activity. All IRFs are required by the Centers for Medicare and Medicaid Services to use a standardized assessment battery, which, at the beginning of our data collection (January of 2018), included the FIM to measure daily activity performance.
In October 2019, the Centers for Medicare and Medicaid Services replaced the FIM items with Section GG codes as the mandated standardized measure to assess level of independence in self-care activities and mobility in IRFs. 22 Using Section GG, occupational and physical therapists score each self-care and mobility activity using a 6-point Likert rating scale to reflect the patient’s level of independence in daily activities based on the type and amount of assistance provided. Scores range from 6, independent and no help needed to complete the activity, to 1, dependent requiring 100% of the effort required to complete the activity. From October 2019, the IRF staff occupational and physical therapists used the Section GG codes to rate patients’ functional performance, while the study occupational therapists continued using the FIM to remain consistent with the study protocol. Data were collected from January 2018 until March 2020, when the trial was paused due to the coronavirus disease-2019 (COVID-19) pandemic and after which home visits had to be modified. During the period of data collection before COVID-19, 83% of participants were assessed using the FIM, and 17% were assessed using Section GG codes at IRF discharge.
Rater Training
Study occupational therapists were trained to administer the FIM using the standardized training program. All study occupational therapists passed the initial examination and were re-credentialed every 2 years. IRF occupational and physical therapists hired prior to October 2019 completed an initial FIM training and were recertified annually. After 2019, all IRF occupational and physical therapists complete GG training and are recertified every 2 years. The average years of experience for study occupational therapists was 12.0, and the average years of experience for IRF occupational and physical therapists was 11.8.
Measurement Crosswalk
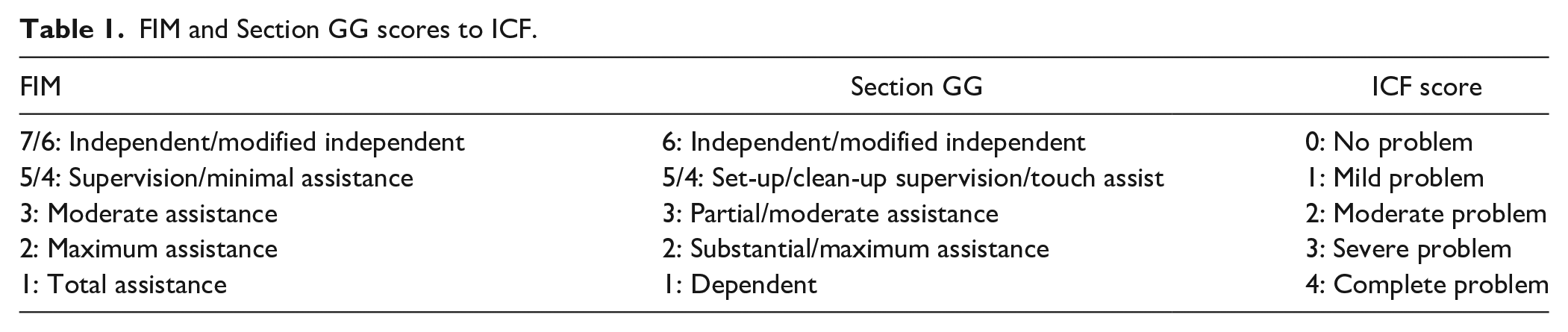
A key study 23 that examined similarities and differences between clinician-observed scores in Section GG and FIM for the same IRF patient highlighted important differences between how independence is scored. For example, patients were scored more frequently as independent using Section GG relative to FIM, because patients are considered independent in Section GG even if using assistive devices. To address these coding discrepancies, we used the International Classification of Functioning, Disability, and Health (ICF) to crosswalk the scores of the FIM and Section GG codes into a common scoring scale. The ICF uses a generic qualifier scale to describe the extent of limitation to participation in daily activities and has been used successfully to create a common language for comparison across measurements when scoring scales differ.15,24 While there is a loss of precision associated with this approach (reducing it to a 5-point scale), it was employed to address the differences in measurement identified by Li et al. 23
To create the crosswalk, overlapping items were identified. These included self-care items of eating, grooming, toileting, bathing, upper body dressing, and lower body dressing, as well as mobility items of bed/chair transfer, toilet transfer, shower/tub transfer, walking 150 ft, and going up and down 12 steps. Next, the FIM and Section GG scales were converted into ICF qualifiers using the ICF manual. A consensus conference with IRF therapists was held. Two IRF occupational therapists were asked to code a set of sample cases (1 case with FIM scores and 1 with Section GG scores) into ICF qualifiers. After consensus was reached on all scores, the scale was finalized (Table 1).
FIM and Section GG scores to ICF.
Statistical Analysis
All data from each participant’s home visit and FIM/Section GG discharge scores from the IRF were entered into a secure, web-based online database, Research Electronic Data Capture. 25 FIM and Section GG scores were converted to ICF scores as described previously. In addition, a total ICF score for each participant for each assessment location (IRF and home) was created using the average of the ICF scores across the 11 activities. Before averaging across activities, we first checked the internal consistency of the ICF items for each assessment location (all Cronbach’s alpha ≥.90).
Participant demographic and baseline characteristics were reported with descriptive statistics for continuous variables, summarized by mean and standard deviation, and categorical variables, summarized by frequency distribution. Distributions of ICF scores for each activity and the average composite ICF score at the home visit evaluation were compared with discharge IRF ICF scores using Wilcoxon signed-rank tests. P values along with Hodges–Lehmann median differences and 95% confidence intervals are provided. A P value <.05 was considered statistically significant. Effect sizes were calculated by dividing the Z statistic by the square root of N and interpreted as 0.1 to <0.3 for a small effect, 0.3 to <0.5 for a moderate effect, and ≥0.5 for a large effect. 26 Using the average score across activities, a linear mixed effects model appropriate for repeated measures data was run using SAS PROC MIXED with a compound symmetry covariance structure. Location of assessment (home vs IRF discharge) was the predictor of interest, and we adjusted for covariates known to be associated with decreased clinical outcomes, including ICF score at admission, age, living situation (ie, living alone or with others), score on the Geriatric Depression Scale Short Form (GDS-SF), 27 and number of comorbid conditions. Finally, the discordances between home and IRF discharge scores were described by classifying scores into 2 categories using a clinically meaningful cutoff ICF score of 2, where <2 indicates no-to-mild impairment and ≥2 indicates moderate-to-complete impairment.
We restricted our analysis to participants whose home assessments were completed within 3 days of discharge (n = 57) to allow for comparison with IRF discharge scores, which are collected during the same timeframe. Data analysis was performed using IBM SPSS Statistics version 27 (IBM Corp., Armonk, NY, USA) and SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). Missing data for assessments was minimal (eg, 1 or 2 participants with missing data for some activities); participants with missing data were excluded from analysis. Analytic sample sizes for each activity are provided in the tables.
Results
Participant Characteristics
The flow of participants for this study is shown in Figure 1. For this cross-sectional study, 85 of the 185 participants randomized for the trial were excluded from the analysis because their home visit was completed using modified procedures due to the ongoing COVID-19 pandemic. An additional 43 were excluded because their home visit was more than 3 days before IRF discharge; thus, the time points were not comparable. The remaining 57 participants were included in this analysis.
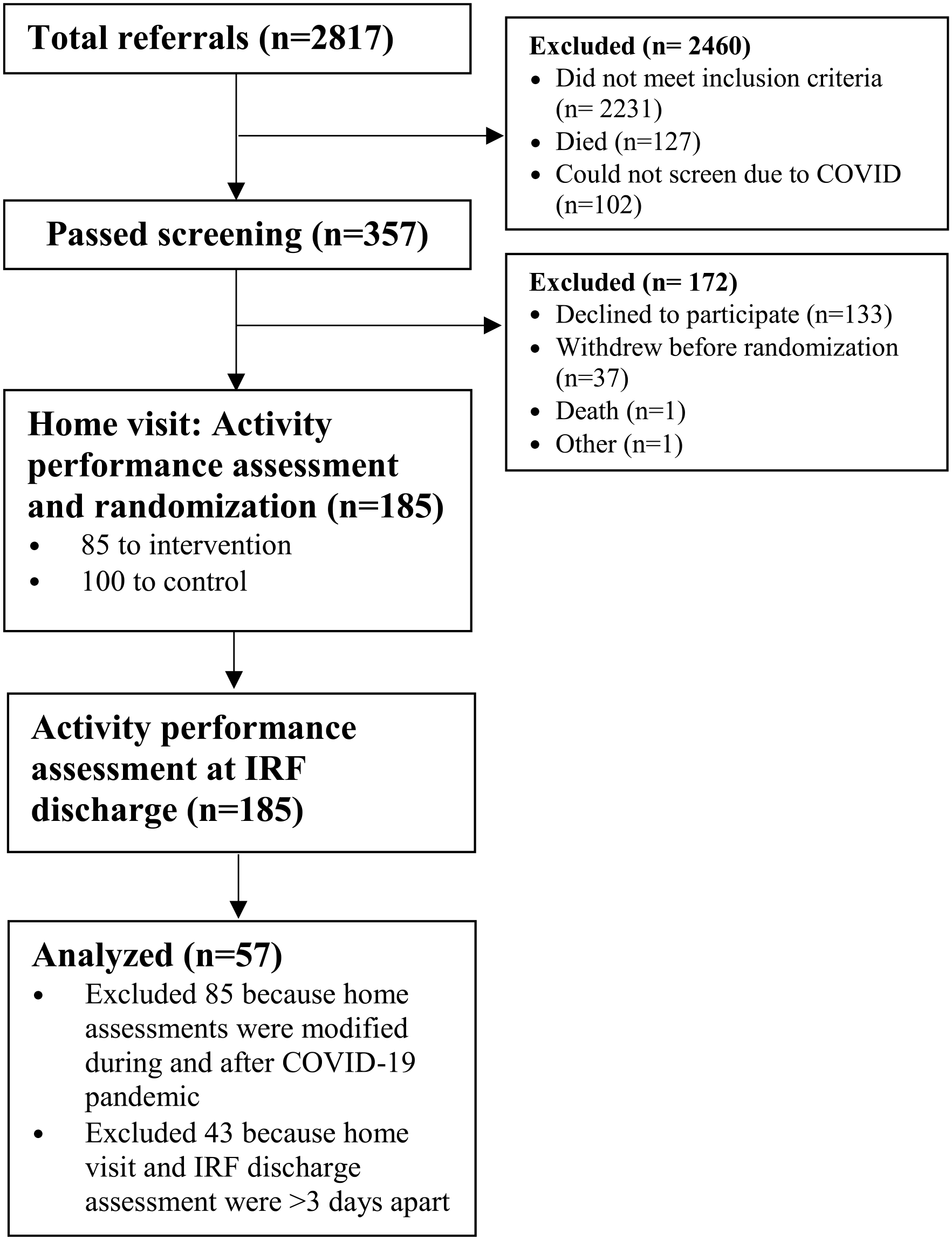
Participant flow chart.
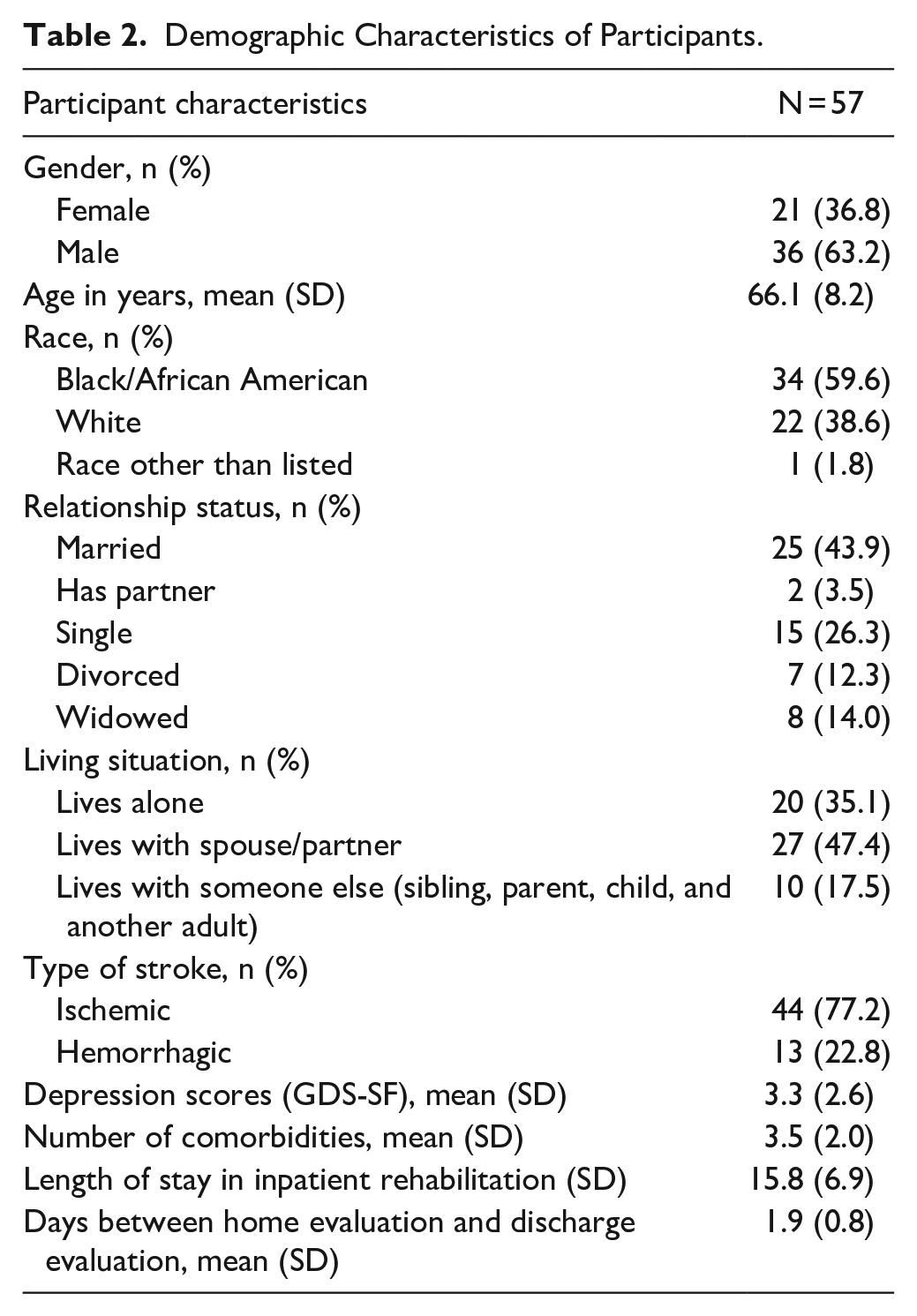
Characteristics of the 57 participants whose home visit was completed ≤3 days before discharge are shown in Table 2. Over half were male and Black, with an average age of 66.1 years (SD = 8.2). Most participants had an ischemic stroke (77.2%), had 3.5 comorbidities, and had few depressive symptoms. The average length of stay in the IRF was 15.8 days (SD 6.9), with longer stays being due to hospital readmissions or extension of IRF stay using private funds. The average number of days between the home visit and IRF discharge evaluation was 1.9 (SD = 0.8, range = 0-3). All home visit assessments were conducted prior to IRF assessments.
Demographic Characteristics of Participants.
Outcomes
During the IRF stay, functional outcome scores improved as expected from admission to discharge for all activities (all P < .001). However, scores for all activities at the home visit were significantly higher than at IRF discharge, indicating greater impairment in daily activities at home compared to in the IRF (Table 3 and Figure 2). The greatest differences were observed for shower/tub transfers and going up and down stairs. The smallest difference between home and IRF discharge scores was for toileting. Effect sizes were large (≥0.6) for almost all activities, except for toileting, which had a moderate effect size (0.4).
Converted Scores at Home Visit and IRF
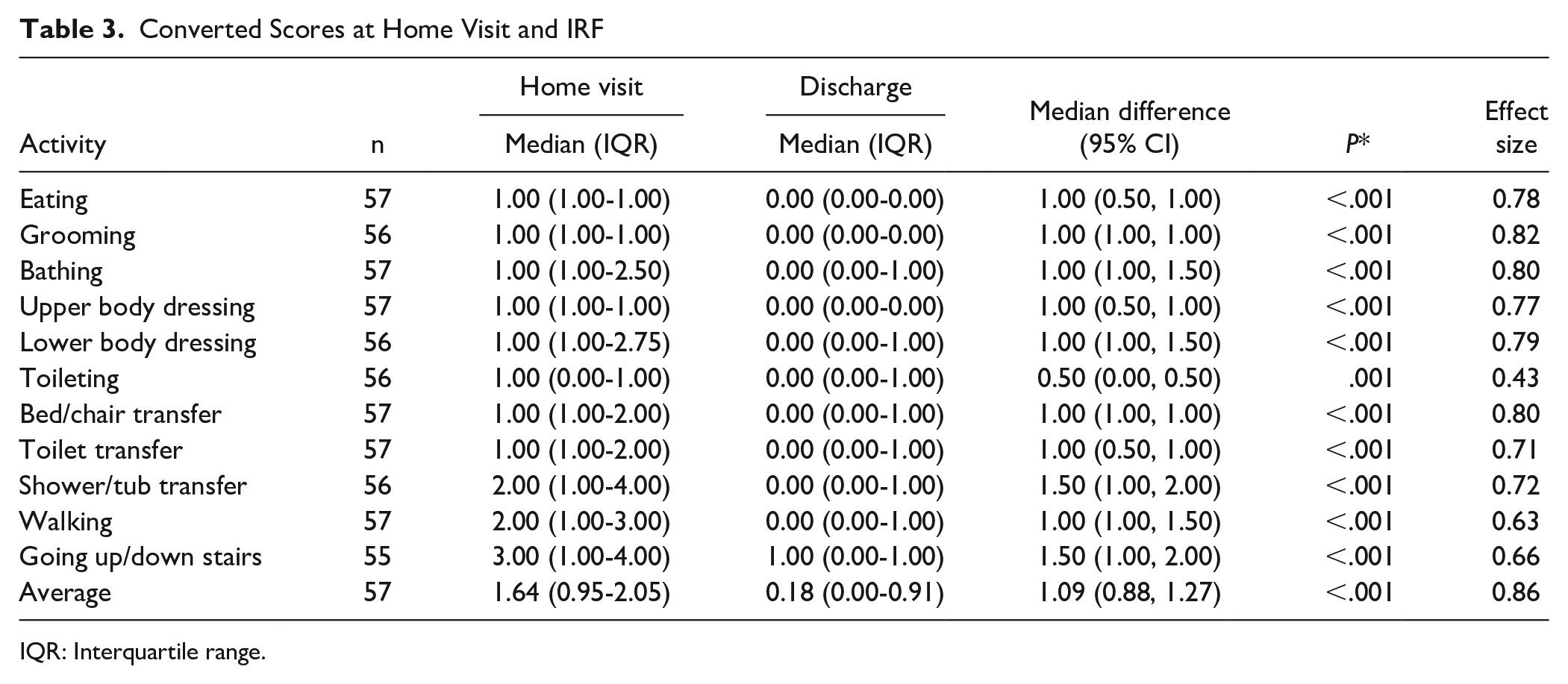
IQR: Interquartile range.
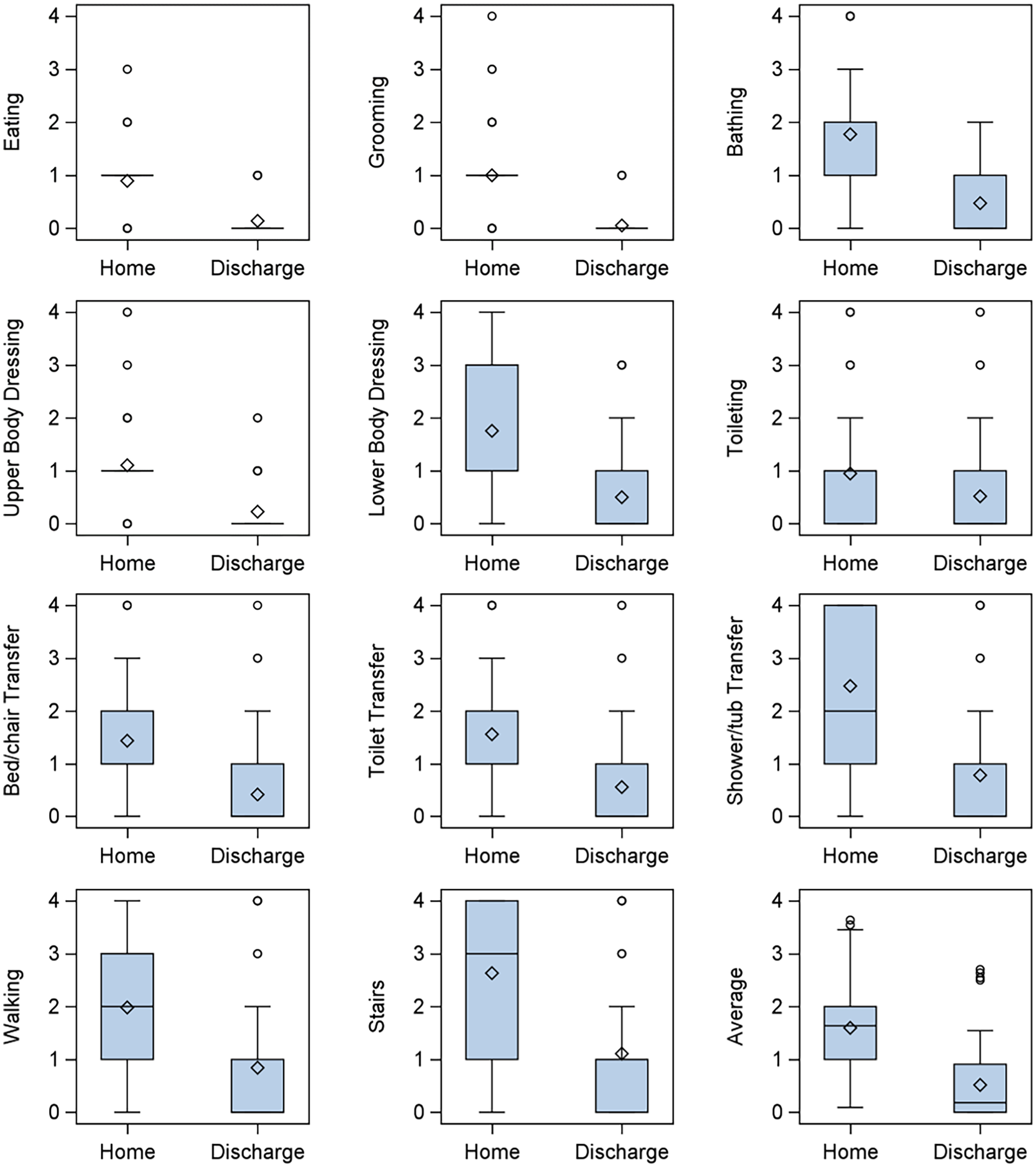
Boxplots of ICF scores at home evaluation versus discharge evaluation. ICF scores for all activities were significantly higher at home evaluation than discharge (all P ≤ .001).
Using average scores across all activities, the median difference between the home assessment and the IRF discharge assessment was 1.09 (95% CI 0.88-1.27). A linear mixed model for repeated measures was used to compare the average score across all activities at home with the IRF discharge assessment, adjusting for the average rating at admission, age, living situation, depression score, and number of comorbidities. Results from this model similarly showed a significantly greater average score at home versus IRF discharge (β = 1.08, 95% CI 0.91-1.26).
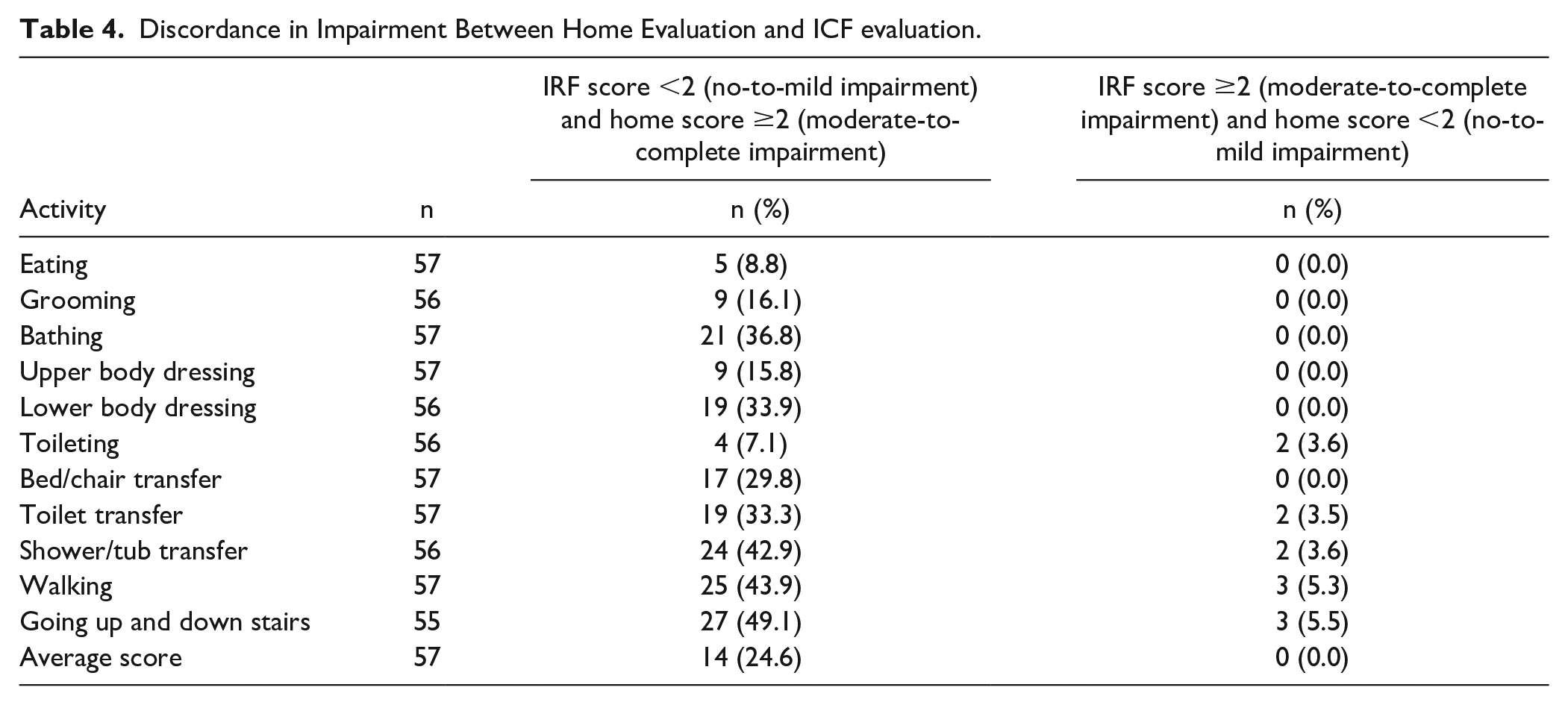
Table 4 shows the discordance between home and IRF discharge scores when classifying ICF scores into 2 clinically meaningful categories (no-to-mild impairment, moderate-to-severe impairment). Results indicate that this discordance between home and discharge scores is quite high for some activities. For example, over one-third of participants had a discharge score indicating no-to-mild impairment, but the home visit score indicated moderate-to-complete impairment for bathing, lower body dressing, and toilet transfer. Over 40% of participants had a discharge score indicating no-to-mild impairment, but the home visit score indicated moderate-to-complete impairment for shower/tub transfer, walking, and going up and down stairs. There were very few discordances in the other direction (ie, the home visit score indicated no-to-mild impairment while the discharge score indicated moderate-to-complete impairment).
Discordance in Impairment Between Home Evaluation and ICF evaluation.
Discussion
Our findings shed light on the influence of the environment on capacity-based assessments conducted in standard clinical settings versus the home. Rehabilitation therapists typically conduct gold-standard performance-based assessments within the controlled confines of the rehabilitation facility, making it challenging to ascertain how well these assessments reflect real-world performance in the home. This study, using baseline data from a larger RCT, sought to determine if there was discordance observed between what an individual can do in the clinical context compared with what they can accomplish at home.
To address this knowledge gap and explore the impact of the environment on performance-based daily activity assessments during the transition from IRF to home, our study examined the daily performance of stroke survivors both within the IRF and in their home environment near the time of discharge. We hypothesized that there would be a significant difference between capacity scores measured in the standard clinical environment and participation scores measured in the real-world setting. Our findings support this hypothesis, revealing that performance was significantly more impaired at home than within the IRF.
It is noteworthy that the discrepancies in performance between the clinical setting and the home environment were most pronounced in specific activities, such as stair climbing and shower/tub transfers (with a difference of nearly 2 points), while being relatively minimal for toileting (with a difference of only 0.5). The differences in observed effect sizes adds support to our hypothesis. Stairways and shower areas are inherently more variable in design and accessibility from one’s clinical rehabilitation environment to their home setting. These areas can be subject to architectural differences, space constraints, and safety modifications, all of which can significantly impact an individual’s ability to perform daily activities. In contrast, toileting activities tend to be more standardized, with fewer environmental variations that could explain the observed differences. This contrast in the discordance between these specific ADLs underscores the importance of considering the real-world variability in home environments when designing and implementing stroke rehabilitation interventions.
The differences in performance we observed between clinical and home settings lend support to the ICF model, which posits that an individual’s functioning and disability are not solely determined by their health condition but are influenced by environmental factors. Our findings illustrate how the environment can act as both a facilitator and a barrier to individuals’ participation in daily activities. Emphasizing the environmental component within the ICF framework is crucial for refining rehabilitation strategies, as it underscores the importance of tailoring interventions to address the unique challenges presented by each individual’s home environment. Most homes in the US have an average of 4.7 to 10.7 environmental barriers that can impact one’s ability to complete daily activities independently.28,29 These findings suggest that barriers in the home environment may be a reason for decreased daily activity performance for stroke survivors in this study.
Although additional research may be warranted to confirm our observed differences in stroke survivors’ functional abilities in IRF versus home, home visits can enable therapists to make tailored home modification recommendations based on performance in the stroke survivor’s real-world environment rather than relying on performance in an optimized setting. Although home visits prior to discharge have been recommended, 30 they are still not standard practice at many IRFs because of lack of time, productivity standards, and limited evidence supporting their effectiveness in improving discharge outcomes. 31 There is currently only low-to-moderate evidence that predischarge home visits improve patient outcomes,32-34 but it is possible that addressing barriers in the environment during home visits could be instrumental in adequately preparing stroke survivors for a successful transition home after stroke and lead to greater independence, fewer falls, and less reliance on caregivers.35-37 However, additional rigorous trials among stroke survivors are needed to examine whether home visits can in fact improve safety, participation, and independence after discharge from an IRF.
Our findings support previously published evidence that describes a decline in stroke survivors’ abilities to complete daily activities at home after discharge from inpatient rehabilitation.11,12 Our study further adds to the evidence by establishing a significant difference in performance scores between the 2 settings at discharge, which may be due to barriers in the home environment.
Limitations
It is important to interpret the findings of this study with caution. The study’s design, which leveraged an ongoing clinical trial, does introduce the possibility of measurement error. Notably, the distinction between FIM and Section GG codes presented a measurement challenge. While it is acknowledged that clinician-observed scores in Section GG and FIM tend to align, 23 there are inherent differences between the 2 assessment tools. Our approach to crosswalk the data using the ICF did involve some reduction in data precision, but it still allowed us to reconcile data from both scales effectively. Importantly, this reduction in precision did not diminish the observed effect. It appears that a genuine difference in performance exists between the standard clinical setting and the home environment.
Another potential limitation of this study is that the scoring of each participant was completed by multiple therapists (study and IRF). Although all therapists underwent standard training and certification for the FIM and Section GG, interrater reliability between the study occupational therapists and the IRF therapists is unknown. Despite the involvement of multiple therapists in scoring each participant, it is important to note that the FIM and Section GG assessments are standardized tests known for their high interrater reliability. 38 The potential variation introduced by different therapists is likely minimal. Because this was a secondary analysis of baseline data from a larger RCT, data were collected according to protocol, where the order of home and IRF assessments was not randomized; home assessments were completed at some point prior to IRF discharge. The study protocol did not control the dose or type of rehabilitation while in the IRF. However, we included participants whose home assessments were conducted within 3 days of discharge, allowing for comparison of assessments conducted within a similar timeframe. There could have been some natural recovery in this short timeframe, which may account for part of the difference in ability between home visit assessments and IRF assessments. Yet it is unlikely that the amount of natural recovery would have been as large as the differences observed in our study. In addition, our sample size was relatively small (n = 57) but did provide 80% power to detect an effect size of ≥0.39 in the Wilcoxon signed rank tests, and all observed effect sizes were large. However, a larger sample may provide more precise estimates of differences in scores between home and IRF assessments. Finally, our study included stroke survivors who were aged 50 years or older and independent in ADLs prior to their stroke; thus, findings may not be generalizable to stroke survivors who were younger or dependent in ADLs pre-stroke.
Conclusion
This exploratory study sheds light on the difference in capacity-based assessments routinely conducted within standard clinical settings versus the home environment. Our investigation explored the gap between clinical performance and real-world functioning in the home environment. Our findings provide evidence to support our hypothesis that performance in daily activities is significantly more impaired at home than within the structured setting of an IRF. Variations in effect sizes by activity underscore the influence of the home environment’s inherent variability.
More robust studies specifically designed to examine differences in stroke survivors’ abilities at home versus in IRF could help corroborate our findings and further inform practical application. However, given our findings, we believe the implementation of home visits prior to discharge to identify and address environmental barriers could better prepare stroke survivors for a successful transition home. The challenges encountered by stroke survivors transitioning from the clinic to the home emphasize the need for rehabilitation strategies that prepare individuals for the multifaceted demands of daily life beyond the controlled environment of the IRF. Home visits are not yet standard practice in many IRFs, often due to time and staffing constraints. Overcoming these barriers and addressing the challenges of the transition from IRF to home could prove instrumental in promoting greater independence.
Footnotes
Acknowledgements
We would like to express our gratitude to all of the participants who willingly contributed their time and effort to this study. Their dedication and cooperation played an integral role in the research process and made this study possible.
Author Contributions
Emily Somerville: Conceptualization; Data curation; Investigation; Methodology; Project administration; Supervision; Writing—original draft; Writing—review & editing. Gabrielle Blenden: Conceptualization; Investigation; Methodology; Writing—original draft; Writing—review & editing. Danielle Kretzer: Methodology; Resources; Writing—review & editing. Brianna Holden: Methodology; Writing—review & editing. Rebecca M.Bollinger: Conceptualization; Methodology; Writing—original draft; Writing—review & editing. Melissa J.Krauss: Data curation; Formal analysis; Methodology; Validation; Visualization; Writing—original draft; Writing—review & editing. Meghan Haxton: Investigation; Writing—review & editing. Noah Martin: Data curation; Formal analysis; Investigation; Visualization; Writing—original draft. Alexandre Carter: Conceptualization; Methodology; Writing—review & editing. Susan L.Stark: Conceptualization; Funding acquisition; Methodology; Writing—review & editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by National Institutes of Health’s Eunice Kennedy Shriver National Institute of Child Health & Human Development (NICHHD) and The National Center for Medical Rehabilitation Research (NCMRR), 1R01HD092398-01.
Clinical Trial Registration
Prospectively registered at clinicaltrials.gov, NCT03485820.