
Abstract
We examined whether number of prism adaptation treatment (PAT) sessions in regular clinical practice would predict spatial neglect (SN) improvement and rehabilitation outcomes. We reviewed clinical records from 16 U.S. rehabilitation hospitals where neurological patients were assessed for SN using the Catherine Bergego Scale (CBS) and if SN was detected, and may have received PAT. Multiple linear regression was used to predict CBS Change (indicating SN improvement) in 520 patients who received PAT while considering age, sex, diagnosis, time post diagnosis, CBS at baseline, neglected side of space, and length of stay. Another set of regression models including the same variables and adding Function Independent Measure (FIM®) at admission was used to predict FIM Gains (indicating rehabilitation outcomes) in 1720 patients receiving PAT or not. We found that greater number of PAT sessions predicted greater CBS Change, especially in patients with moderate-to-severe neglect. Number of PAT sessions also positively correlated with Total FIM, Motor FIM, and Cognitive FIM Gains regardless of SN severity classification at baseline. Furthermore, number of PAT sessions predicted CBS Change and FIM Gains among patients completing ≤8 PAT sessions but not among patients with ≥8 sessions, who however, showed greater CBS Change with increased PAT frequency (i.e., fewer days between two consecutive sessions). Receiving more once-daily PAT sessions predicted greater improvement in SN and rehabilitation outcomes. Receiving PAT at a higher frequency for 8 or more sessions predicted better SN improvement. Thus, dosage matters. The study provides practice-based evidence that PAT is appropriate for inpatient rehabilitation.
Keywords
Introduction
Among stroke survivors in the acute and subacute inpatient settings, approximately 30% have spatial neglect (SN), which is more common after right brain damage than left brain damage. 1 SN can occur after other types of brain injuries as well. 2,3 SN results from damage to the neural networks critical to the processing of spatial information and attentional control. 4,5 The syndrome typically renders abnormal bias toward the space ipsilateral to the injured cerebral hemisphere, and hence, affected individuals pay insufficient or no attention to the contralesional side of space, which cannot be attributed to primary sensory or motor defects. 6,7 Decades of research has consistently demonstrated the negative impact of SN on rehabilitation outcomes. 8 -11
Prism adaptation treatment (PAT; for detailed treatment procedures and mechanisms, see recent reviews) 12 -15 is promising in reducing SN symptoms and improving functional outcomes. 16,17 We conducted a retrospective, matched control study (N = 312) 18 that demonstrated the effectiveness of PAT when embedded in occupational therapy practice on inpatient rehabilitation outcomes. In the study, PAT involved utilization of 20-diopter lenses (shifting the visual field for 11.4°) for 8–12 once-daily sessions, and this regimen was associated with greater rehabilitation outcomes at discharge compared to no PAT. 18 However, randomized controlled trials (RCTs) using similar strength of prism lens have showed mixed results, which could reflect differences in treatment intensity or outcome measures utilized. Some RCTs delivered the treatment 2 times a day, 5 days a week over two weeks, and resulted in improved SN 19 and rehabilitation outcomes. 20 Others had 10 sessions, one session a day, over two weeks, and showed improved SN 21,22 but no additional benefits to inpatient rehabilitation. 23,24 Trials examining reduced PAT dosage (e.g., one session a day over 4 days 25 or 1–2 sessions over 7–12 days) 26 have shown limited effects on some but not all neuropsychological test performances. This may account for the inconsistencies of recent meta-analyses. 27,28 In general, there is uncertainty about both the optimal and minimally necessary PAT dosage, that is, the number of PAT sessions, to improve outcomes.
To gain insight of the relationship between PAT dosage and outcomes, the present study examined data gathered through regular clinical practice (i.e., clinical records) in 16 rehabilitation hospitals that participated in a large-scale implementation project for improving SN care of patients with brain injury (for details about the overarching project, see Hreha et al.) 29 It is important to note that clinical records can provide practice-based evidence, which differs from evidence generated from prospective RCTs and has inherent limitations such as no blinding (i.e., the same therapists or colleagues on the same therapy team assessing and treating the same patients), no randomization or allocation concealment procedures assigning patients to control conditions, and a great heterogeneity of the sample. Nonetheless, as demonstrated in the matched, controlled study described above, 18 data based on clinical records can help answer certain questions and generate new research questions.
In the overarching implementation project, 29 therapists were encouraged to assess all neurological patients under their care, with the understanding that SN can occur after different types of brain injury, using the Catherine Bergego Scale (CBS) via the Kessler Foundation Neglect Assessment Process (KF-NAP®). 30,31 Therapists were encouraged to deliver PAT following the Kessler Foundation Prism Adaptation Treatment (KF-PAT®) protocol 13,22 when SN was detected. The primary goal was to train all participating therapists in integrating both KF-NAP and KF-PAT in their practice. The implementation process, which was a researcher–clinician collaboration, resulted in clinically feasible instructions for therapists. Therapists were instructed to assess patients with the CBS via KF-NAP within 4–5 days of hospital admission and, for those that received PAT, again prior to discharge. Patients who did not receive PAT were not re-evaluated using the CBS via KF-NAP at time of discharge.
Therapists were also instructed to provide 10 once-daily sessions of PAT during patients’ stay. While this has become the standard procedure in recent RCTs, 21 -24 the regimen may not be easily implemented clinically, especially in U.S. rehabilitation hospitals. 32 Among 2019 Medicare beneficiaries, for example, the average length of stay (LOS) is 17, 16, and 15 days for patients with stroke, traumatic brain injury, and non-traumatic brain injury, respectively. 33 Even if patients are evaluated for SN within the first few days of admission, there may be less than 10 full treatment days for a therapist to provide PAT daily. Thus, we acknowledged the challenge and provided suggestions regarding management of time and resources. Ultimately therapists used their discretion when providing care and services to their patients. All the activities executed and documented were part of clinical practice.
Based on the clinical records available from the overarching implementation project, the present study examined the hypothesis that greater PAT dosage (i.e., number of PAT sessions) would predict better SN improvement and rehabilitation outcomes in patients with mild, moderate, or severe SN.
Methods
Included Patients
The overarching implementation project included 16 rehabilitation hospitals across 11 different states in the US through a collaborative agreement. The agreement included that occupational therapists in the participating hospitals would be trained in both the KF-NAP and KF-PAT and that the hospitals would share de-identified clinical information with the research center. The project was approved by the Institutional Review Board (IRB) of the research center and a hospital’s local IRB if available. No consent forms were collected from individual patients due to the nature of the present study, that is, review of clinical records and retrospective analyses. We reviewed the records of patients who were assessed using the CBS via KF-NAP from April 2016 to November 2020.
For the purpose of the present study, we included patients (1) whose CBS > 0, indicating the presence of SN, (2) who, if treated with PAT, had a documented number of PAT sessions, and (3) whose outcomes were assessed before and after PAT using either the CBS or the Functional Independence Measure (FIM®).
Outcome Measures
Spatial neglect improvement was measured using the change score of the CBS from baseline to after PAT (i.e., CBS Change). The CBS measures functional deficits specific to SN. 31,34 The KF-NAP is a standardized method for using the CBS in 10 categories of behaviors during daily activities, which includes gaze orientation, limb awareness, auditory attention, personal belongs, dressing, grooming, navigation, collisions, meals, and cleaning after meals. 30 Each item is scored from 0 (no neglect) to 3 (severe neglect). The final score ranges from 0 to 30, calculated with the formula: (sum score ÷ number of scored items) × 10. 34 The level of SN severity was classified as mild (CBS = 1–10), moderate (CBS = 11–20), or severe (CBS = 21–30). 34 In the present study, CBS Change = CBS score at baseline–CBS score after PAT, and a positive value of CBS Change indicated SN improvement.
Rehabilitation outcomes were measured using the change scores of the FIM from admission to discharge (i.e., Total, Motor, and Cognitive FIM Gains). The FIM consists of 6 self-care items, 2 sphincter control items, 3 transfer items, 2 locomotion items, and 5 cognitive items. The cognitive items form the Cognitive FIM Subscale and the other 4 categories with a total of 13 items form the Motor FIM Subscale. Each item was scored 0 (activity did not occur) to 7 (complete independence) at admission, and 1 (total assistance) to 7 at discharge. 35 FIM was the standard for measuring inpatient rehabilitation outcomes in the U.S. until September 2019. Thus, FIM scores were available in the records collected prior to that time.
PAT
The treatment procedures were detailed elsewhere. 13,22 In short, patients wore goggles fitted with 20-diopter prism lenses that shift the visual field 11.4 degrees of visual angle to the right (used for left-sided neglect) or the left (used for right-sided neglect) and used a pen to mark the center of a 24 cm line or a 1 cm diameter circle. Each stimulus (a line or circle) was placed at body midline or in left or right space (32 cm to the side of body midline). Patients performed the task beneath a shelf that blocked their view of the initial part of the arm movement but allowed them to view the stimulus and approximately the latter third of their hand-path. Patients completed all 30 lines and 30 circles, or until 20 minutes had elapsed. The 20-minute limit was created to fit within the typical 45-minute occupational therapy session in the US inpatient rehabilitation care.
Analysis Methods
All the analyses were performed using STATA/SE 16.1. 1 We described patient characteristics using median (IQR) for continuous variables, and counts (%) for categorical variables. We examined the impact of PAT dosage (i.e., number of PAT sessions) on SN improvement (CBS Change) and rehabilitation outcomes (FIM Gains) using multiple linear regression analysis. We minimized confounding effects of LOS on the number of PAT sessions by excluding outliers who were 1.5 IQR below the 1st quartile and above the 3rd quartile of LOS and by including LOS in all the regression models described below. The alpha level for all tests was set at .05.
Regarding CBS Change, the predictive model included number of PAT sessions as the primary variable, and added LOS, age, CBS at baseline, and time between diagnosis and admission because these factors play significant roles in SN recovery. 20,36 -38 Although there was no evidence supporting that sex, diagnosis, or neglected side of space predicted PAT treatment effect or rehabilitation outcome, 11,39,40 we added these variables to the model to explore potential correlations. We repeated the same regression model based on the severity classification of SN to explore whether the impact of number of PAT sessions was more prominent in a specific patient group defined by SN severity at baseline.
Regarding FIM Gains, each predictive model included the same variables as described above and an additional variable for functional status at admission, i.e., Total, Motor, or Cognitive FIM at admission (respectively chosen based on the dependent variable).
Lastly, as proof of concept, we conducted three separate multiple linear regression models to verify that SN improvement (CBS Change) predicted rehabilitation outcomes (Total, Motor, and Cognitive FIM Gains) while controlling for age, sex, diagnosis, time post diagnosis at admission, respective FIM score at admission, CBS at baseline, neglected side, number of PAT sessions, and LOS.
Results
Patient Characteristics
4454 patients’ data were reviewed. The median LOS was 17 days (IQR = 13–23). Patients were assessed with the KF-NAP 4 days (IQR = 2–6) after admission. 2491 (55.9%) had SN (CBS > 0). Of the patients with SN, 1559 (62.6%) had left-sided neglect, 878 (32.3%) had right-sided neglect, and the side of neglect was not specified in 54 (2.2%) patients. Left-sided neglect (median CBS = 8.75, IQR = 3.8–15.6) was more severe than right-sided neglect (median CBS = 5.56, IQR = 2.2–10). 1071 (40.1%) of patients with SN were treated following the KF-PAT protocol.
Characteristics of Patients.
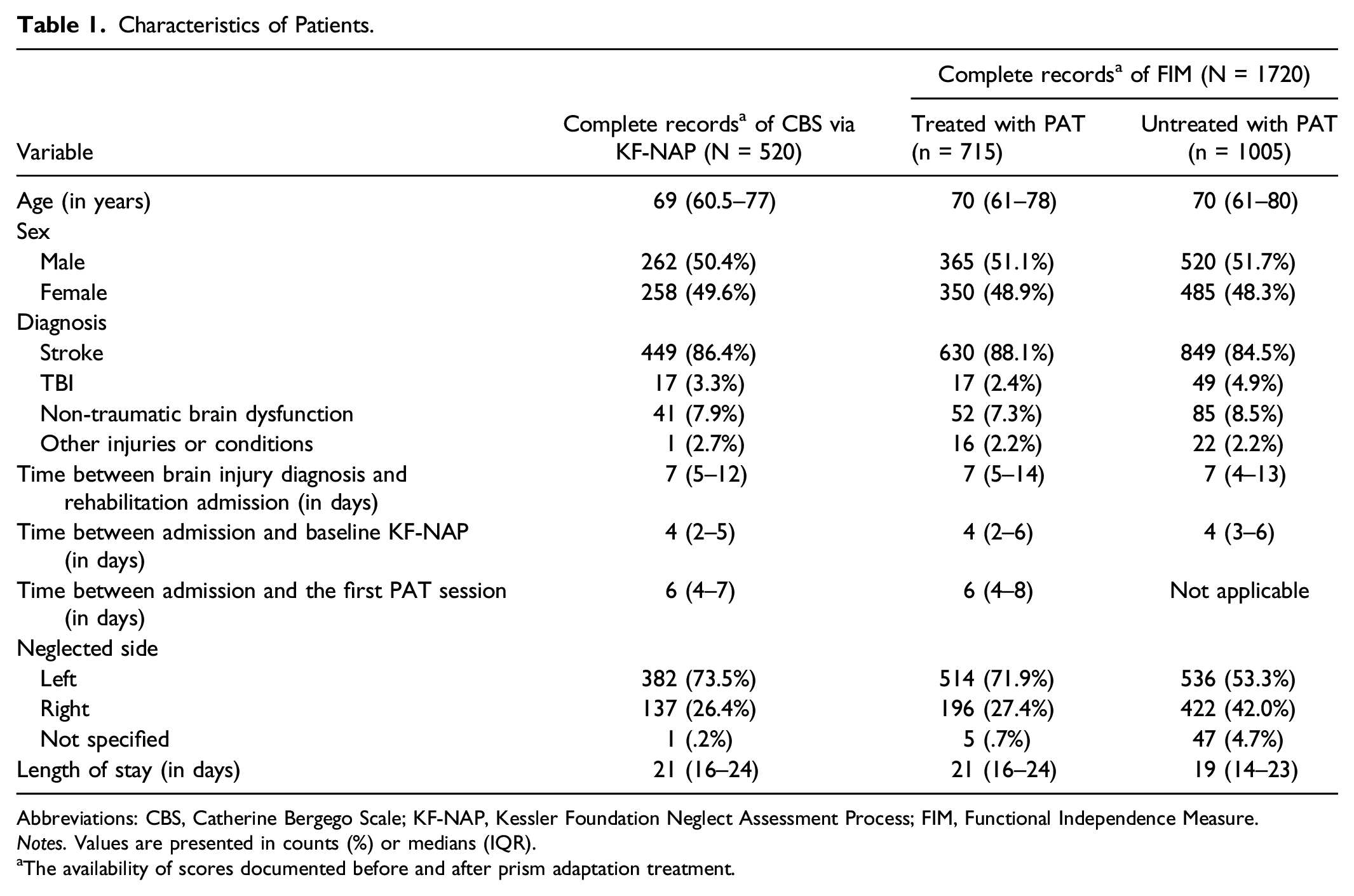
Abbreviations: CBS, Catherine Bergego Scale; KF-NAP, Kessler Foundation Neglect Assessment Process; FIM, Functional Independence Measure.
Notes. Values are presented in counts (%) or medians (IQR).
aThe availability of scores documented before and after prism adaptation treatment.
SN Improvement (N = 520)
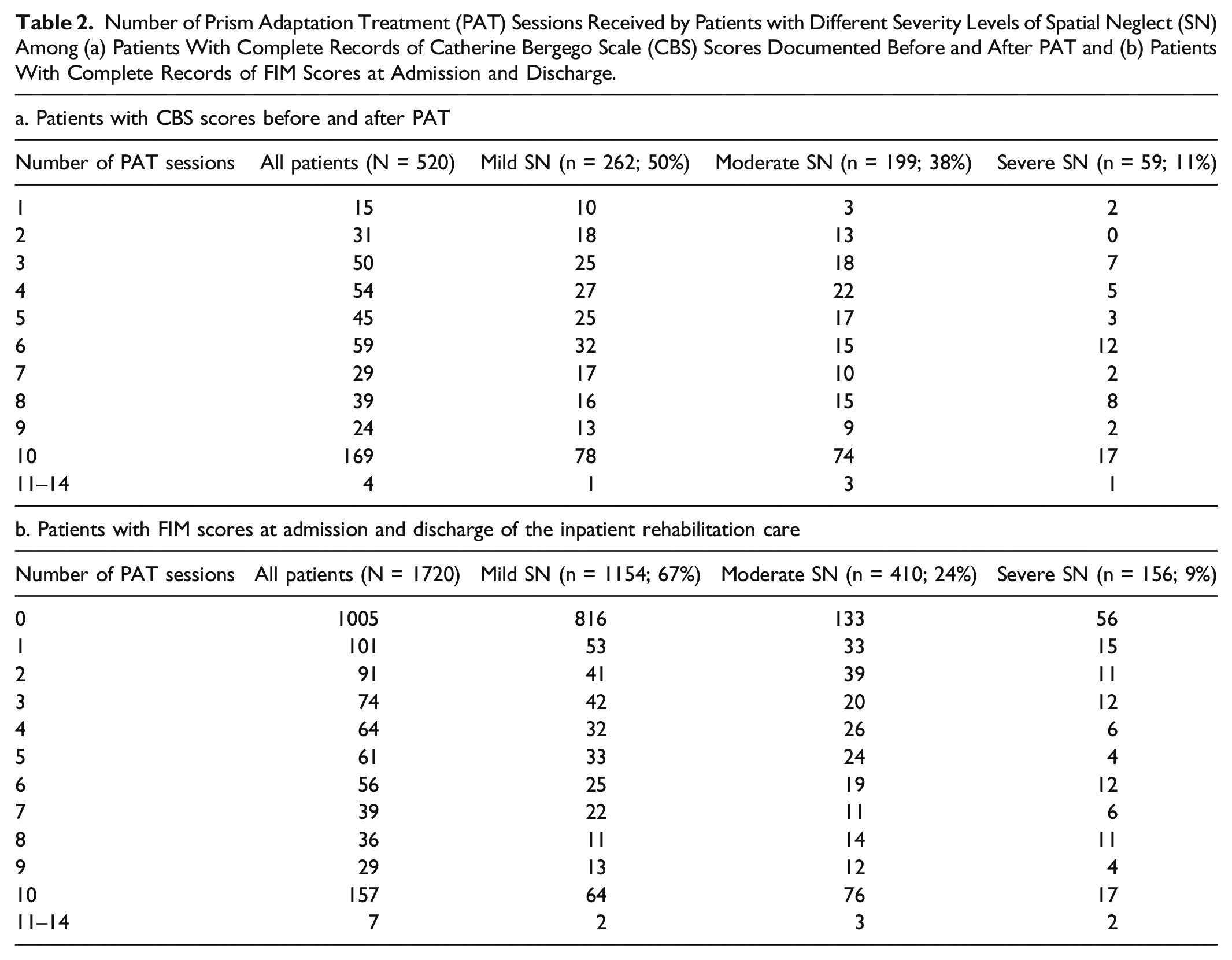
Number of Prism Adaptation Treatment (PAT) Sessions Received by Patients with Different Severity Levels of Spatial Neglect (SN) Among (a) Patients With Complete Records of Catherine Bergego Scale (CBS) Scores Documented Before and After PAT and (b) Patients With Complete Records of FIM Scores at Admission and Discharge.
Multiple Linear Regression Results for the Change of the Catherine Bergego Scale (CBS) Scores From Before to After Prism Adaptation Treatment (PAT), that is, CBS Change.
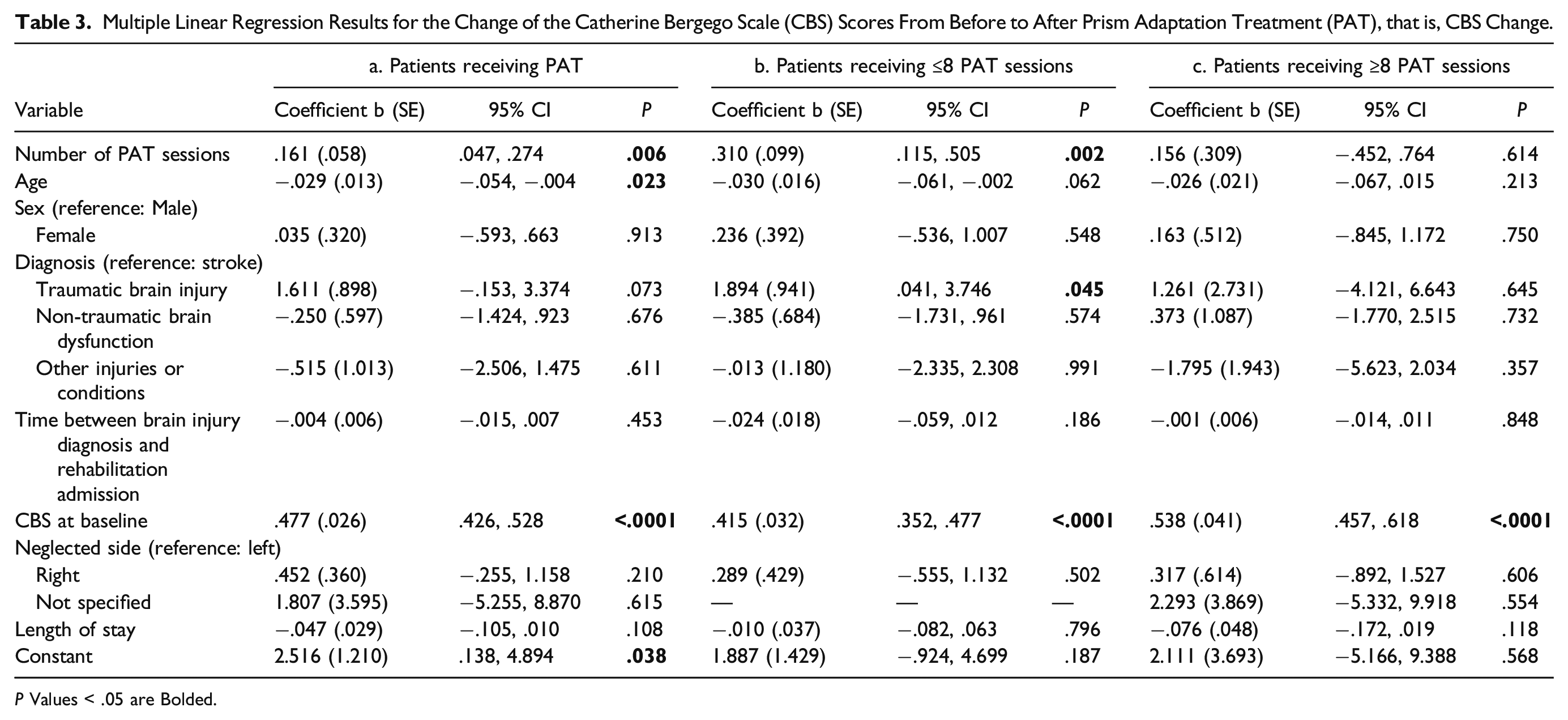
P Values < .05 are Bolded.
While number of PAT sessions and SN improvement were correlated, we investigated whether this linear relation stopped at a certain number of sessions. Because therapists reported difficulties providing 10 once-daily sessions to every patient (due to LOS and other factors),
29
the following post hoc analysis may provide insight into whether fewer than the suggested dosage of 10 sessions could be enough for similar SN improvement. Visual examination of CBS Change by number of PAT sessions (Figure 1) indicated a more prominent linear relationship between session attendance and gains in patients attending 8 or fewer sessions. As a post hoc analysis, two independent models were tested to examine patients with ≥8 PAT sessions (n = 237) compared to patients with ≤8 sessions (n = 322). Patients completing 8 sessions were included in both models for there was no reason to exclude “8 sessions” from either model. We found that every PAT session completed predicts .310 increase in CBS Change (95% CI = .115–.505) among patients receiving ≤8 sessions (Table 3b). However, we found no significant linear correlation between number of PAT sessions and CBS Change among patients who received ≥8 PAT sessions (Table 3c). Scatter plot showing the change of Catherine Bergego Scale scores (CBS Change) from before to after prism adaptation treatment as the function of the number of PAT sessions.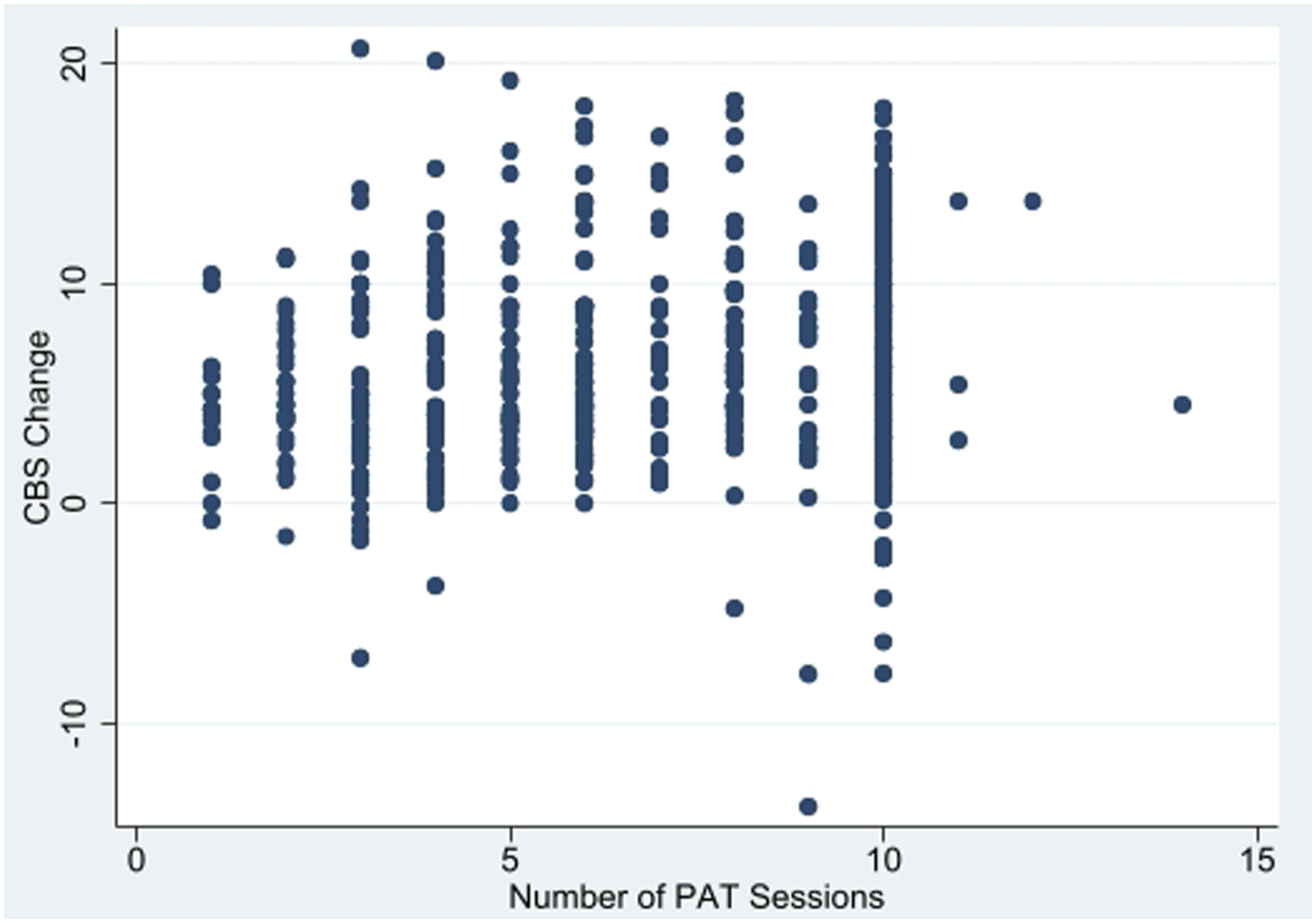
We further hypothesized that frequency of PAT sessions, rather than total number of PAT sessions, would be more important in the cohort of patients who received ≥8 PAT sessions. Therefore, a new model was run to determine the impact of the PAT frequency (i.e., number of sessions over number of days from the first to last sessions) on CBS Change when added to a predictive model including the same covariates as described above. The model significantly predicted CBS Change, F(11,216) = 16.61, P < .0001, adjusted R 2 = .431, and the frequency of PAT sessions was correlated with CBS Change, b = 4.305 (SE = 2.110), 95% CI = .145–8.464, P = .043. Thus, receiving PAT at a higher frequency (i.e., fewer days between two consecutive sessions) for at least 8 sessions predicted better SN improvement.
Rehabilitation Outcomes (N = 1720)
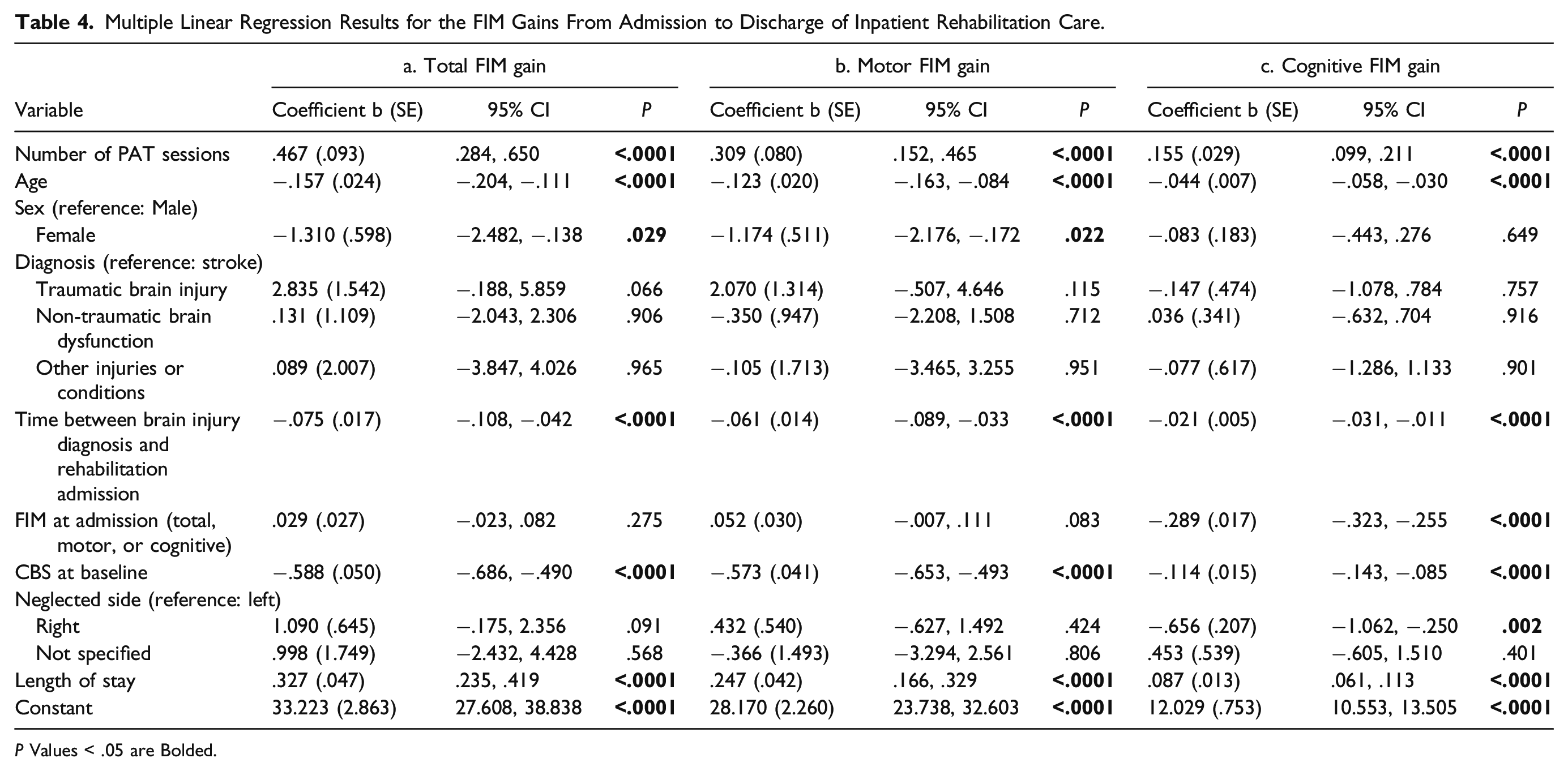
Multiple Linear Regression Results for the FIM Gains From Admission to Discharge of Inpatient Rehabilitation Care.
P Values < .05 are Bolded.
When predicting each FIM Gain by SN severity, three multiple linear regression analyses that included the same variables as those in Table 4 were conducted in patients with mild, moderate, and severe neglect. Results showed that greater number of PAT session correlated with greater Total FIM Gain in patients with mild (b = .413, SE = .134, P = .002), moderate (b = .536, SE = .174, P = .002), and severe neglect (b = .620, SE = .236, P = .009), with greater Motor FIM Gain in patients with mild (b = .251, SE = .115, P = .029), moderate (b = .380, SE = .144, P = .009), and severe neglect (b = .442, SE = .201, P = .030), and lastly, with greater Cognitive FIM Gain in patients with mild (b = .156, SE = .041, P < .0001), moderate (b = .146, SE = .052, P = .005), and severe neglect (b = .237, SE = .071, P = .001). Thus, receiving more once-daily PAT sessions was associated with greater functional gains in motor and cognitive independence regardless SN severity at baseline.
A sub-group of patients (N = 1092) had itemized FIM scores available. Thus, we further explored the impacts of number of PAT sessions on gains of different categories within the motor domain by repeating the same predictive model. Number of PAT sessions positively correlated with gains in self-care (b = .124, SE = .057, P = .029), sphincter control (b = .130, SE = .027, P < .0001) and transfers (b = .135, SE = .033, P < .0001) but did not correlate with gains in locomotion (b = .041, SE = .028, P = .141).
Spatial Neglect Improvement and Rehabilitation Outcomes (N = 349)
Multiple linear regression results for the FIM Gains from admission to discharge of inpatient rehabilitation care among patients (N = 349) who had the Catherine Bergego Scale (CBS) scores before to after prism adaptation treatment.
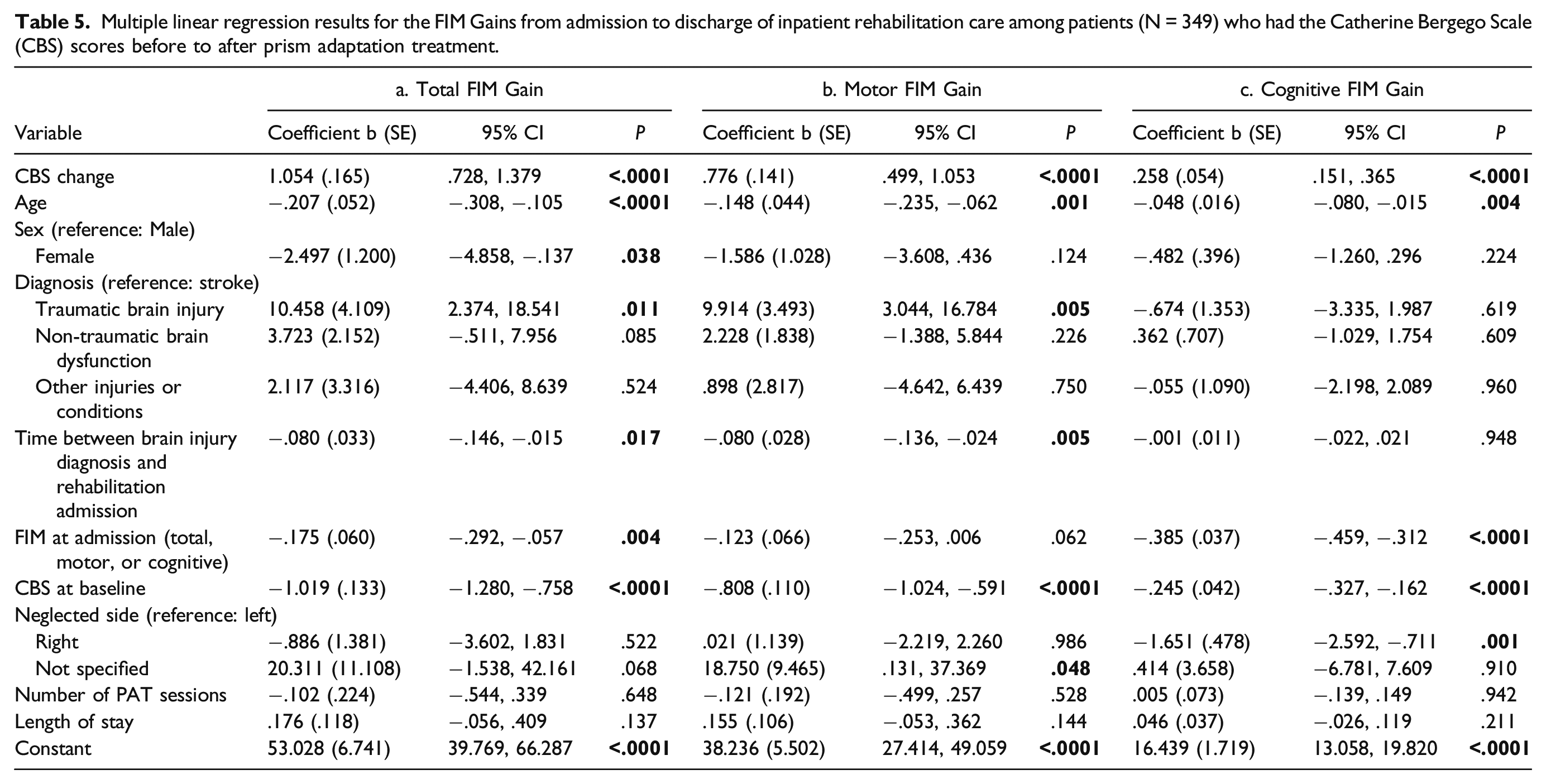
There were other findings from this set of analyses (Table 5). Younger age and milder SN severity predicted greater gains in Total, Motor, and Cognitive FIM. Having traumatic brain injury (in comparison to stroke) and shorter time between diagnosis and admission predicted greater Total and Motor FIM Gains. Being male (in comparison to female) and lower FIM score at admission predicted greater Total FIM Gain. Lower Cognitive FIM at admission and left-sided neglect (in comparison to right-sided neglect) associated with greater Cognitive FIM Gain.
Discussion
The present study was based on clinical records. Standardized SN assessment and PAT were completed during regular occupational therapy practice. We found SN improvement predictive of motor and cognitive outcome measures (Table 5). Importantly, more once-daily PAT sessions predicted greater SN improvement (Table 3) and rehabilitation outcomes (Table 4). This linear relationship was observed in patients completing 8 or fewer PAT sessions. In patients who received 8 or more sessions, higher frequency (i.e., fewer days between two consecutive PAT sessions) predicted even greater SN improvement. These findings suggest that PAT dosage plays a key role in the beneficial impact of the treatment.
Our findings, however, are inconsistent with results of recent meta-analyses. 27,28 Those analyses found no immediate benefits of PAT on SN improvement, measured using conventional paper-based neuropsychological tests or the CBS. Although data regarding CBS Change in patients who received no PAT was unavailable in the current study, our finding of a positive correlation between PAT dosage and SN improvement suggests a beneficial impact of PAT on SN. One possibility explaining this discrepancy in findings is that prospective RCTs often purposefully recruit patients in subacute or chronic stages, 28 while in the present study, the median duration between a brain injury event and the first PAT session was 15 days when patients’ SN was relatively acute, potentially more responsive to PAT. Another possibility is that the methods of delivering PAT differed across studies. Following the KF-PAT protocol in the present and a few previous studies, 22,24 patients performed line bisection and circle marking while wearing prism goggles. In many other RCTs, 19 -21,23,25,26 patients made fast pointing movements to visual targets with prism goggles on. Without a control group (i.e., no PAT), the effectiveness of PAT, following the KF-PAT protocol, on SN improvement could not be confirmed in the present study. However, a true control group does not exist in the clinical practice.
Considerations Based on Severity Level of Spatial Neglect
No correlation between PAT dosage and SN improvement was found in patients with mild SN (CBS = 1–10 at baseline). This may be related to the floor effect that their CBS scores were initially low, greatly restricting the range of measurable improvement. Nonetheless, number of PAT sessions was positively correlated with Total, Motor, and Cognitive FIM Gains for this patient group. Thus, we suggest that PAT be provided to patients with mild neglect. Clinicians should be aware that many assessments are not as sensitive as the CBS with or without following the KF-NAP 41,42 and may overlook patients with mild neglect.
Among patients with moderate-to-severe SN (CBS = 11–30 at baseline), receiving more once-daily PAT sessions predicted greater improvement in SN and rehabilitation outcomes. In contrast to the current findings, a sham-control RCT by Vilimovsky et al. 24 (N = 21) found no immediate or long-term effect of 10 PAT sessions on SN improvement in patients with moderate-to-severe SN. In particular, Vilimovsky et al. utilized the KF-NAP and KF-PAT (the standardized tools implemented in the present study) to administer CBS and PAT. 24 The present study, given its clinical nature, could not be compared directly to trials such as Vilimovsky et al. that revealed no reliable difference in SN improvement between PAT and sham treatment. 20,23,24 The control condition implemented in those trials, restricting patients’ visual experience with non-prismatic goggles while they performed visuomotor training, may have exerted a therapeutic effect on SN. 21 Vilimovsky et al. 24 also postulated that the sham-control condition could strengthen sustained attention, which in turn, activated attentional neural networks resulting in SN improvement. 43 Future studies are needed to investigate the mechanisms of PAT, 12 which is beyond the scope of the current discussion.
Mizuno et al. 20 ’s sham-control RCT (N = 38), 20 which like the present study, used Total FIM Gain as the measure for the rehabilitation outcome, found that patients with “mild neglect” showed greater improvement both immediately after completion of PAT and at the time of discharge, than those received sham treatment, while patients with “severe neglect” did not. SN severity was classified using a cutoff score of 55 (max = 81) on the behavioral, ecological subtests of the Behavioral Inattention Test. 44 It is unclear why patients with severe neglect were not as responsive to PAT as patients with milder neglect in Mizuno et al.’s study. Further investigations are needed to understand the mechanisms underlying sham treatment employed in Vilimovsky et al., Mizuno et al., and other RCTs. 21,23,24
Impact of PAT on Functional Gains in the Motor Domain
Studies have suggested that PAT improves the motor symptoms of SN 45,46 and functional abilities that require integration of spatial processing and movement control such as walking 47 and wheelchair navigation. 48,49 In the present study, the impact of PAT dosage was found on 3 of the 4 Motor FIM categories, including self-care, sphincter control, and transfers, but not on locomotion. Using the present dataset, we are unable to investigate how PAT facilitated improvement in these different motor functions due to the lack of information specifying the inpatient rehabilitative therapy activities. 50,51 While the FIM has been discontinued as the standard of rehabilitation outcome measure, we expect that its replacement, that is, the Continuity Assessment Record and Evaluation (CARE) Tool, 52 will demonstrate more detailed results on motor rehabilitation outcomes as it contains three times more items measuring transfers and locomotion than FIM.
Functional Gains in Inpatient Rehabilitation
While we primarily focused on the impact of PAT dosage, there were other findings revealed from our analyses suggesting important predictors of greater functional gains regardless of PAT (Tables 4 and 5). These predictors included milder SN severity at baseline, lower functional independence, younger age, and fewer days between diagnosis and inpatient rehabilitation admission. In addition, our analysis showed that being female was associated with poorer outcome than male, which may be related to the fact that women were on average 3.8 years older than men in this cohort. However, the sex difference was found after age and many other factors were controlled in the models. Overall, our findings were consistent with the literature 20,36 -38 suggesting that greater SN severity, older age, and longer period between diagnosis and inpatient rehabilitation impede rehabilitation outcome.
One interesting finding was that after controlling for SN severity at baseline and many other factors, right-sided neglect predicted lower Cognitive FIM Gain than left-sided neglect (Tables 4c and 5c). Wee et al. 9 showed that left-sided neglect was associated with poorer Total FIM Gain than right-sided neglect, but we did not observe this pattern in Total FIM Gain but the opposite pattern in Cognitive FIM Gain. Ten Brink et al. 39 found no association between neglected side of space and functional rehabilitation outcomes that focused mostly on self-care and mobility while we found a relative negative association between right-sided neglect and functional rehabilitation outcomes based on patients’ ability in communication, expression, social interaction, problem solving, and memory. It is possible that, in comparison to patients with left-sided neglect, patients with right-sided neglect are less likely to improve in those areas due to the extent of brain damage in the left hemisphere. However, we did not collect sufficient information to examine this hypothesis.
Study Limitations
One limitation of the present study was the heterogenous sample, which included all neurological patients under participating therapists’ care in the analysis. This sample included both patients with left-sided neglect and patients with right-sided neglect. We included patients who sustained a stroke, traumatic brain injury, or other brain injuries and conditions (Table 1) based on the coded rehabilitation impairment category used in the U.S. healthcare records. It is common that patients with subdural hematoma, for example, are coded as stroke. It is also possible that a patient coded as “traumatic brain injury” could have had a stroke too (e.g., the person fell and injured their head at the time experiencing a stroke). Although patients coded as stroke comprised most of the sample, we did not collect information regarding location of their brain lesions or prior neurological history (e.g., history of prior brain injury events, presence of bilateral lesions). Thus, we are unable to comment on a specific clinical population or compare results among different diagnoses. This is very different from prospective research protocols that have strict inclusion and exclusion criteria limiting the sampling noises.
In addition, whether or why patients received no or any number of PAT sessions were not entirely at random but determined by various factors, which is discussed in depth in a separate article. 29 Other than PAT, we had no information about types or total hours of therapies, or treatment activities within a therapy in which patients participated during their LOS. The noisy dataset may explain that in the present study, the multiple linear regression models predicting CBS Change accounted for less than 50% variance and less than 30% variance regarding FIM Gains. Thus, results from the present study must be interpreted with caution.
Conclusions and Clinical Implications
Greater SN improvement predicts better rehabilitation outcomes in terms of functional independence. Receiving more once-daily PAT sessions predicts greater SN improvement as well as rehabilitation outcomes. In addition, receiving PAT at a higher frequency (i.e., fewer days between two consecutive sessions) for more than 8 sessions predicts even better SN improvement. These conclusions are supported by the practice-based evidence found in the present study. We suggest initiate PAT as early as possible in inpatient rehabilitation programs to increase the likelihood that patients receive the treatment at a higher dosage to improve SN and enhance overall rehabilitation outcomes.
While the present analysis was focused on PAT dosage, more analyses have been planned to answer questions based on the clinical records gathered through the multi-site implementation project 29 such as whether patients with left-sided neglect and right-sided neglect differed in their outcomes associated with PAT, whether receiving PAT earlier or later during inpatient rehabilitation care predicted outcomes, and whether FIM Gains and changes in measures of the CARE Tool were comparable. However, some questions cannot be answered from this dataset. For example, as is typically the case in the U.S. healthcare system, long-term (i.e., post-discharge) information was not available for the current sample collected from inpatient rehabilitation hospitals. Future studies are needed to determine the long-term impact of PAT.
In conclusion, PAT is appropriate for clinical use as part of inpatient therapy sessions. Our findings provide direct support to the latest clinical practice guidelines generated by topic experts 53 that recommend the use of PAT for SN. It is known that unresolved SN symptoms can impede functional recovery, 54 slow community reintegration, 55 and increase caregiver burden. 56 Patients may benefit from additional PAT sessions in outpatient or home settings and continue improving functional abilities affected by SN. Further practice-based studies are needed to generate treatment guidelines and practical advice, compliant with the best standards for patient care development.
Footnotes
Acknowledgments
We thank all the occupational therapists and their supervisors of the participating sites for implementing the KF-NAP® and KF-PAT® protocols in their practice and for sharing clinical data for our analysis. We thank Kena Patel, Marinos Pylarinos, Grace Wells, Maria Mawhinney, Louis Varillas, Tamara Burdinoska, Jenny Masmela, and Emma Kaplan for administrative support and data management. We thank Nicole Diaz-Segarra for assisting in literature review. We thank John DeLuca for scientific advice.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The treatment equipment described in the article contains elements under the U.S. Patent Number 10,739,618, owned by Kessler Foundation. KF-NAP and KF-PAT are registered trademarks owned by Kessler Foundation. Two authors (PC and TJR) are employees of Kessler Foundation.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Kessler Foundation, Wallerstein Foundation for Geriatric Life Improvement, and the Charles and Ann Serraino Foundation.