
Abstract
Background
Rehabilitative treatments that promote neuroplasticity are believed to improve recovery after stroke. Animal studies have shown that cardiovascular exercise (CE) promotes neuroplasticity but the effects of this intervention on the human brain and its implications for the functional recovery of patients remain unclear. The use of biomarkers has enabled the assessment of cellular and molecular events that occur in the central nervous system after brain injury. Some of these biomarkers have proven to be particularly valuable for the diagnosis of severity, prognosis of recovery, as well as for measuring the neuroplastic response to different treatments after stroke.
Objectives
To provide a critical analysis on the current evidence supporting the use of neurophysiological, neuroimaging, and blood biomarkers to assess the neuroplastic response to CE in individuals poststroke.
Results
Most biomarkers used are responsive to the effects of acute and chronic CE interventions, but the response appears to be variable and is not consistently associated with functional improvements. Small sample sizes, methodological variability, incomplete information regarding patient’s characteristics, inadequate standardization of training parameters, and lack of reporting of associations with functional outcomes preclude the quantification of the neuroplastic effects of CE poststroke using biomarkers.
Conclusion
Consensus on the optimal biomarkers to monitor the neuroplastic response to CE is currently lacking. By addressing critical methodological issues, future studies could advance our understanding of the use of biomarkers to measure the impact of CE on neuroplasticity and functional recovery in patients with stroke.
Introduction
Neuroplasticity can be broadly defined as the capacity of the nervous system to adapt and, more specifically, as the functional and structural changes that occur in the nervous system in response to intrinsic and extrinsic stimuli. Following stroke, the adult brain demonstrates a remarkable capacity to repair itself by undergoing plasticity of the surviving neural systems, a state of neural malleability that contributes to recovery and forms the basis for rehabilitation. 1 Potentiating this neuroplastic capacity of the nervous system to adapt is a primary goal of poststroke neurorehabilitation.
Therapeutic interventions that facilitate neuroplasticity are thought to improve functional recovery after stroke. Neurorehabilitation and pharmacological interventions amplify neuroplasticity beyond spontaneous neurological recovery, resulting in larger improvements across multiple functional domains, including motor, somatosensory, cognitive, and language recovery. 2 However, unlike animal experiments, where molecular and cellular processes can be studied invasively, in humans, we are still far from understanding the specific neurobiological mechanisms that underpin stroke recovery. 3
Biomarkers, which are indicators of disease state that reflect molecular and cellular changes, 4 can be categorized as neurophysiological, neuroimaging, and blood biomarkers (Figures 1-3; Boxes 1-3). 4 The study of biomarkers is an emerging area in the field of stroke recovery and rehabilitation because they can quantify not only the extent of the neurological damage and thus help predict long-term recovery outcomes but also enable the measurement of neurobiological events in response to rehabilitative therapies, providing, in turn, mechanistic insights about their potential to promote neuroplasticity and brain repair. 5
Neurophysiological biomarkers.
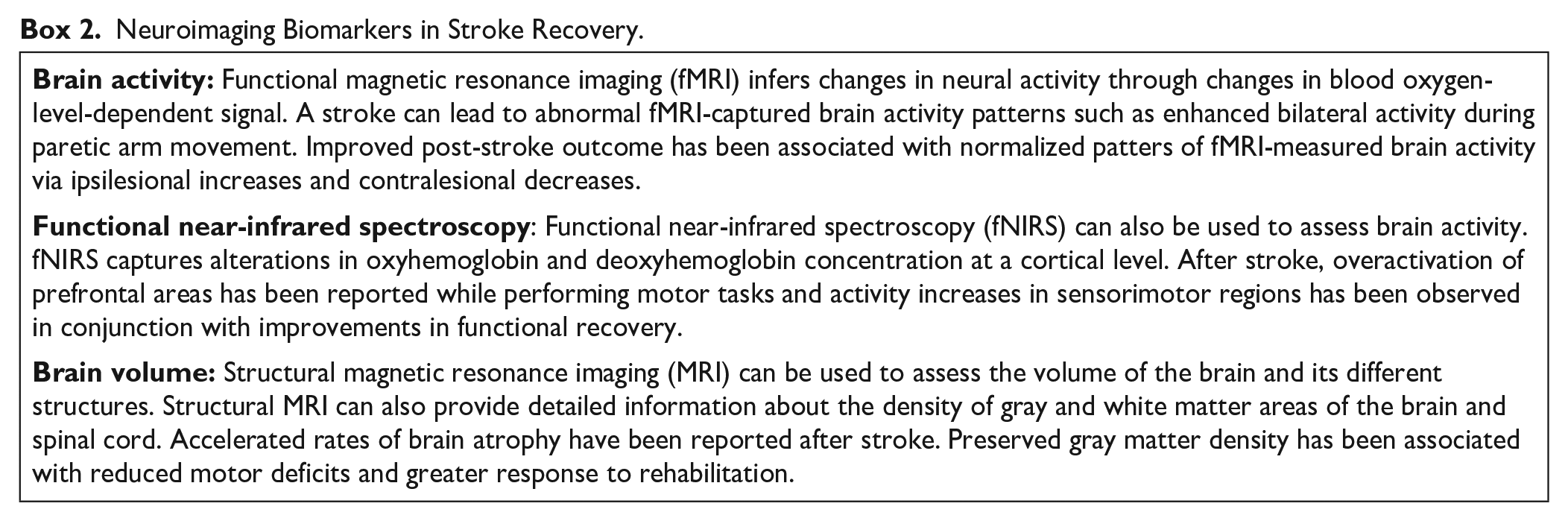
Neuroimaging biomarkers.
Blood biomarkers.
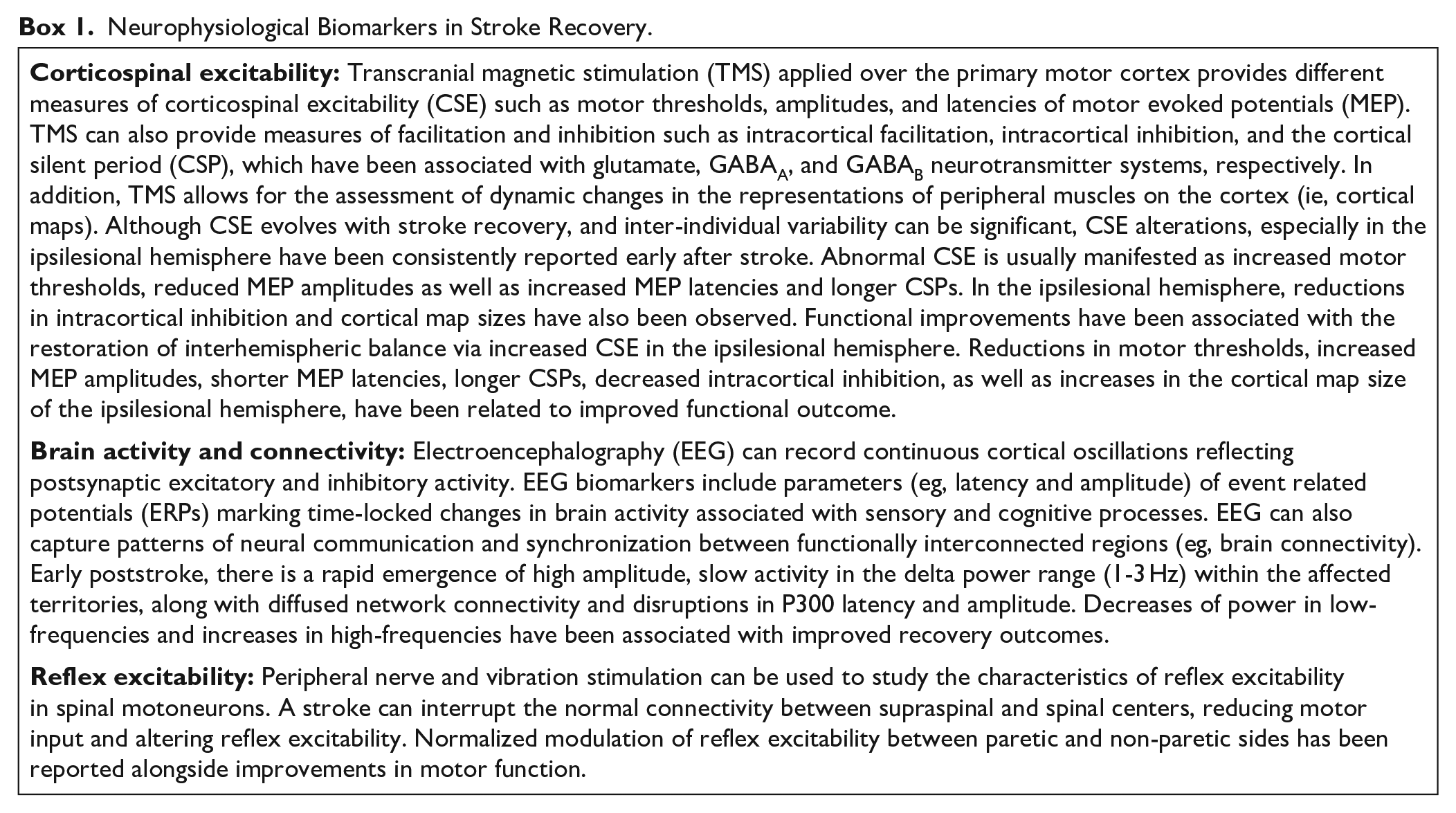
Neurophysiological Biomarkers in Stroke Recovery.
Neuroimaging Biomarkers in Stroke Recovery.
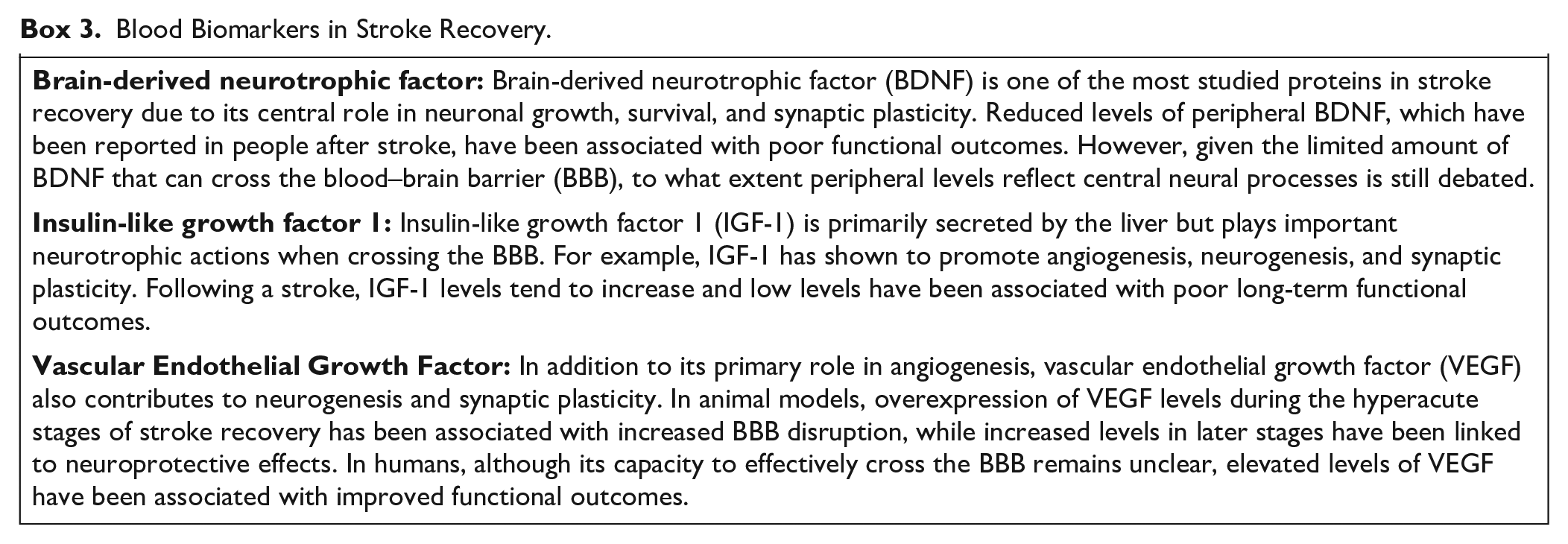
Blood Biomarkers in Stroke Recovery.
Cardiovascular exercise (CE), defined as any physical rhythmic activity maintained continuously that involves large muscle groups and targets the cardiorespiratory system, has demonstrated to be a safe and effective intervention to improve walking capacity, cardiovascular health, and quality of life in people with stroke. 6 Given its potential to also mitigate the risk of stroke recurrence, and simultaneously improve cardiorespiratory, metabolic, and neural recovery targets, CE is recommended as a core component of stroke rehabilitation. 7 Evidence from animal studies supports the beneficial effects of CE on brain recovery via multiple mechanisms, including reductions in the size of the lesion, oxidative damage, inflammation, as well as increases in growth factors, cellular metabolism, synaptic and dendritic plasticity, angiogenesis, and neurogenesis. 8
CE can protect and maintain brain function by promoting changes in the nervous system. 9 However, its effects on neuroplasticity and brain recovery in individuals after stroke remain largely unknown. 8 This could be, in part, because of the inadequate use of biomarkers capturing the neuroplastic response to this intervention. Without a better knowledge of the effects of CE on neuroplasticity, there is little chance of objectively quantifying the potential restorative capacity of this intervention, limiting, in turn, its evidence-based implementation to maximize stroke recovery. 4
The aim of this point of view manuscript is to present a critical analysis of the biomarkers currently utilized to assess neuroplasticity in CE studies in people after stroke. Additionally, we provide context to these findings within the current state-of-the-art use of biomarkers in stroke recovery, identify gaps in knowledge and propose directions to guide future studies. A systematic search in accordance with PRISMA guidelines was conducted to identify relevant studies. Details on the methodology used and the main results of the search are provided as supplementary material.
Neurophysiological Biomarkers
Corticospinal Excitability
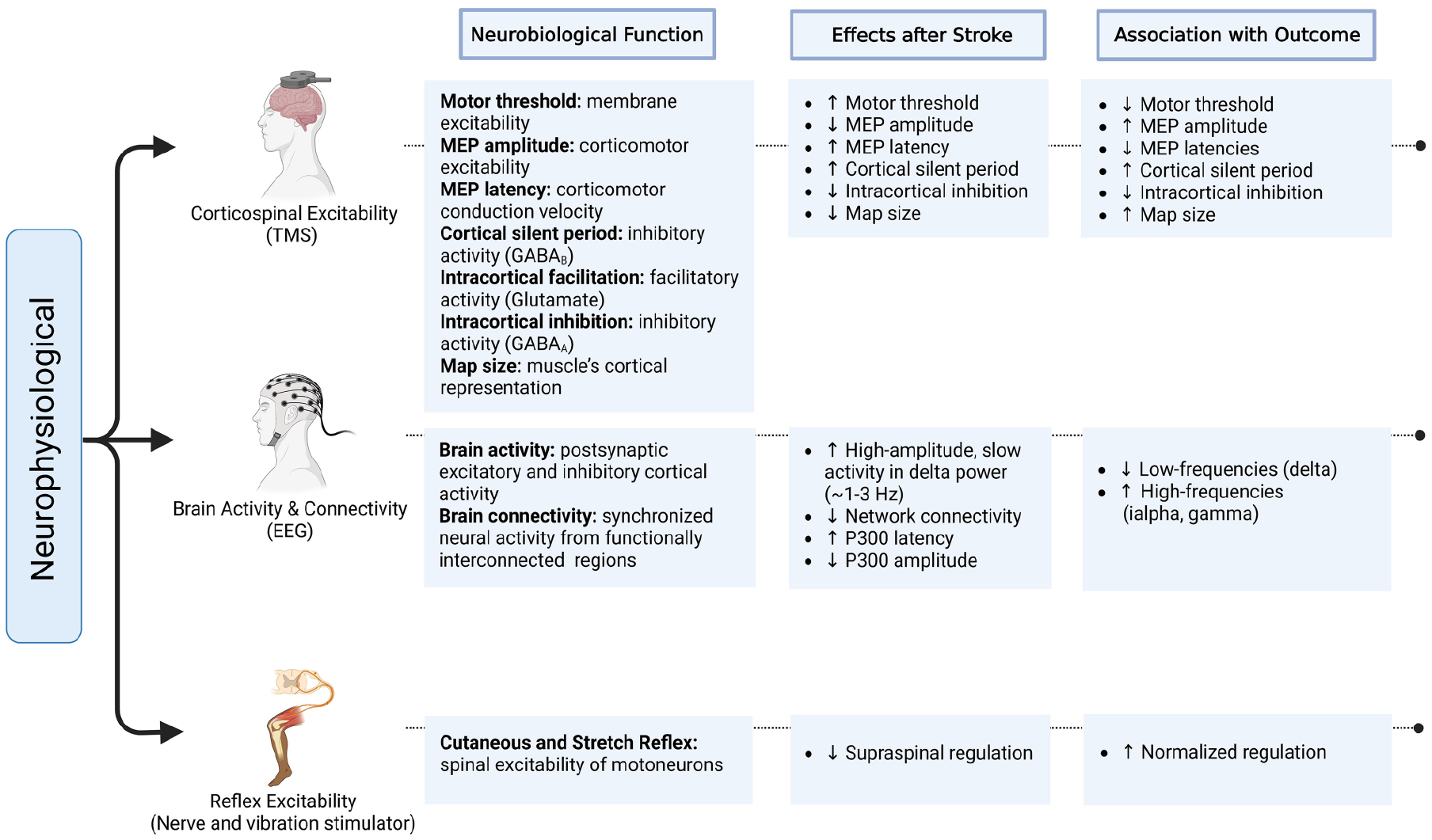
Obtained via single or paired-pulse transcranial magnetic stimulation (TMS) protocols, different corticospinal excitability (CSE) measures can capture multiple excitability and connectivity alterations in cortico-cortical and cortico-spinal pathways after a stroke (Figure 1; Box 1). The acute and chronic responses to CE in terms of changes in CSE are examined with a single and multiple training sessions, respectively. Eight acute10-17 and 3 chronic18-20 studies used TMS to assess different markers of CSE in response to CE (Table 1). Seven out of 8 acute studies reported significant changes following a single bout of CE. One study showed that 5 minutes of exercise at vigorous intensity increased the amplitude of the resting motor evoked potential (MEP) on the ipsilesional hemisphere. 10 Two studies investigated acute CSE changes following a graded exercise test,11,16 with only 1 study showing significant changes via decreases in short-interval intracortical inhibition on the ipsilesional hemisphere leading to a reduction of excitability imbalances between hemispheres. 16
Main Characteristics of the Studies Including Neurophysiological Biomarkers.
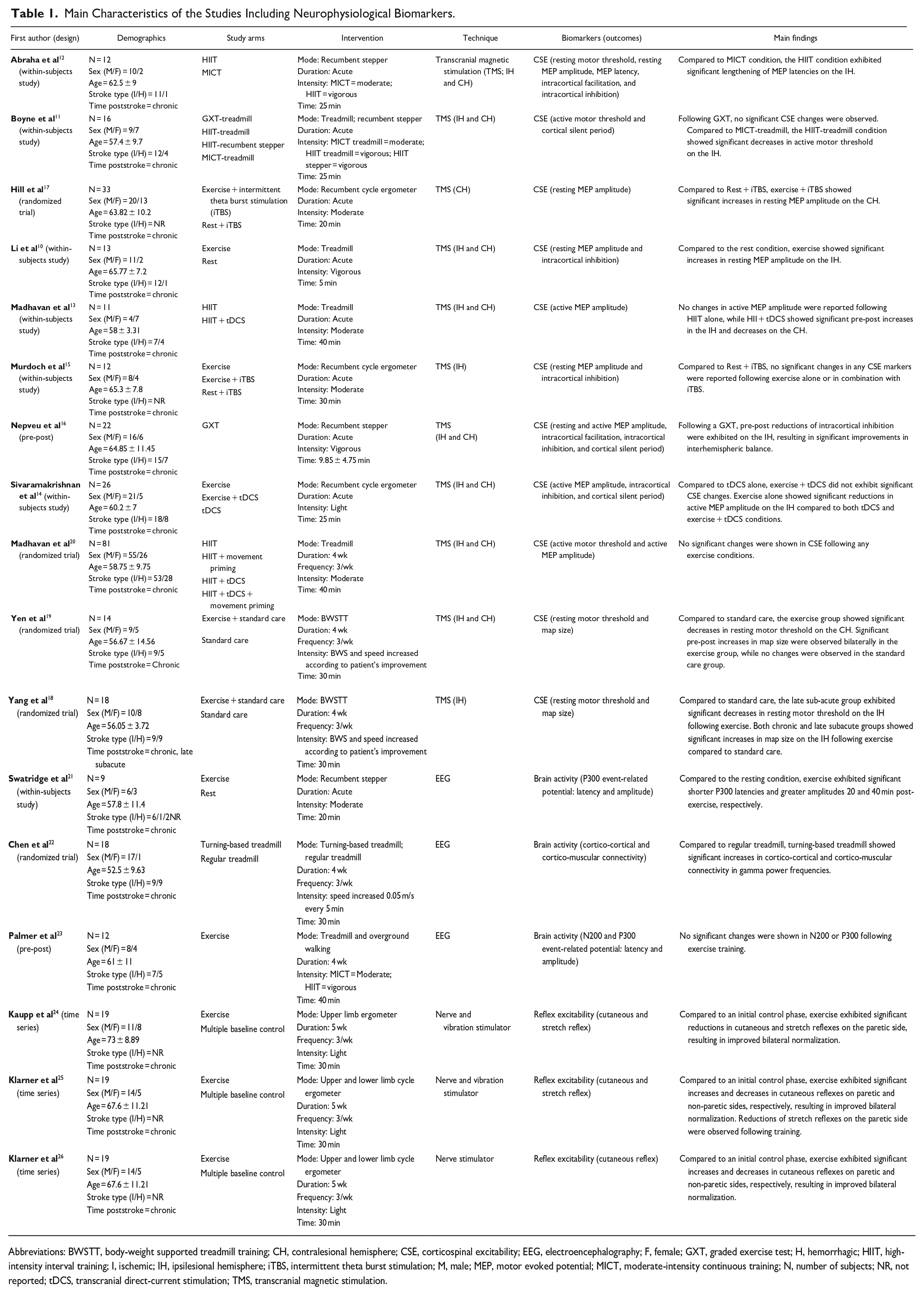
Abbreviations: BWSTT, body-weight supported treadmill training; CH, contralesional hemisphere; CSE, corticospinal excitability; EEG, electroencephalography; F, female; GXT, graded exercise test; H, hemorrhagic; HIIT, high-intensity interval training; I, ischemic; IH, ipsilesional hemisphere; iTBS, intermittent theta burst stimulation; M, male; MEP, motor evoked potential; MICT, moderate-intensity continuous training; N, number of subjects; NR, not reported; tDCS, transcranial direct-current stimulation; TMS, transcranial magnetic stimulation.
Two acute studies investigated the impact of CE intensity on CSE by comparing the effects of a single bout of moderate-intensity continuous training (MICT) to high-intensity interval training (HIIT).11,12 In both studies, HIIT evoked larger changes in CSE than MICT on the ipsilesional hemisphere that manifested in reductions of motor threshold during a low force isometric muscle contraction (ie, active motor threshold) 11 and increases in MEP latency. 12 In one of the studies, the association between the acute CSE responses to MICT and HIIT with upper limb function measured with the box and blocks test and handgrip maximal voluntary contraction was examined, with no significant results. 12 This result reinforces the complex functional relationship between CSE and motor function, and the importance of interpreting the information provided by MEPs with much caution. 27
Four acute studies explored the priming effects of non-invasive brain stimulation facilitatory protocols in combination with a single bout of CE on CSE.13-15,17 While no significant effects were observed following exercise alone, 1 study showed significant increases in the amplitudes of active MEPs on the ipsilesional side and reductions on the contralesional side when anodal transcranial direct current stimulation (tDCS) was applied prior to HIIT. 13 A second study showed that, compared to anodal tDCS applied alone or during exercise, a single bout of light-intensity cycling exercise alone exhibited greater reductions in the amplitudes of active MEPs on the ipsilesional hemisphere. 14 Finally, 2 studies applied intermittent theta burst stimulation (iTBS) delivered through TMS following CE,15,17 with only one showing significant priming effects on CSE on the contralesional hemisphere. 17
Two chronic studies found increases in CSE following 4 weeks of treadmill training via reductions in the resting motor threshold on the ipsilesional 18 and contralesional 19 hemisphere. The same studies demonstrated increases in the size of the cortical map bilaterally 19 and ipsilesionally. 18 One of these studies showed a significant association between reductions in the resting motor threshold and increases in the map size on the contralesional hemisphere with improvements in balance and step length, respectively. 19 Another study failed to show any significant effect on CSE after 4 weeks of MICT treadmill provided alone or following other interventions including movement-based priming and anodal tDCS. 20
In summary, CE appears to modulate some aspects of CSE in people with stroke, but the effects vary substantially among studies. Changes in CSE, which are more often detected in the ipsilesional hemisphere, include increases in the size of the cortical map, longer MEP latencies and greater amplitudes, as well as reductions in resting motor thresholds and interhemispheric imbalances. In neurotypical individuals, a single vigorous bout of CE has shown to elicit acute increases in CSE. 28 In individuals after stroke, exercise intensity could modulate the CSE in response to acute CE, with higher intensities evoking more pronounced CSE changes on the ipsilesional hemisphere. Whether both acute and chronic CE can augment the priming effects of tDCS or iTBS on CSE is unclear. Furthermore, while most CSE changes reported here have been previously associated with recovery improvements (Figure 1; Box 1), whether CE can modulate CSE in patients at earlier stages of recovery and to what extent these changes are associated with functional improvement is yet to be determined. 27
Brain activity and Connectivity
Brain activity and connectivity recorded with electroencephalography (EEG) can capture brain oscillations reflecting postsynaptic excitation and inhibition, both of which have been used in the diagnosis of cerebral ischemia, outcome prediction, and treatment response after stroke (Figure 1; Box 1). Three studies used EEG to examine the effects of CE on brain activity and connectivity poststroke21-23 (Table 1). In 1 study, acute changes in brain activity were examined while performing a modified Eriksen Flanker executive function task following a single bout of stepping exercise performed at moderate intensity. 21 Exercise evoked shorter latencies and increased amplitudes in the P300 wave measured from the ipsilesional hemisphere. Increases in amplitude and reduced latencies in P300 have been associated with better cognitive performance. Given that cognitive and perceptual impairments along with disruptions in the P300 wave are prevalent after stroke, 29 this waveform could provide insights into exercise-induced cognitive improvements in this population. The chronic changes in brain activity were examined in a similar study using the same stimulus-evoked paradigm to study cortical inhibition (N200) and facilitation (P300) over the frontal cortical region following 4 weeks of treadmill and overground walking. 23 While no significant changes in cortical activity were evoked with CE, a positive association between cortical (N200 latency) and behavioral (response inhibition in Flanker task) inhibitory indices was found after the intervention, suggesting a link between cortical processing and cognitive inhibitory responses.
The other study that employed EEG investigated chronic changes in cortico-cortical and cortico-muscular connectivity (ie, coherence) by comparing regular treadmill with turning-based treadmill training. 22 Compared to a conventional treadmill walking, 4 weeks of a turning-based treadmill intervention led to significant increases in cortico-cortical and cortico-muscular coherence in gamma power frequencies (23-40 Hz) over the frontal-central-parietal areas of the brain. Importantly, increases in brain connectivity correlated with improvements in gait symmetry only after turning-based training, suggesting that adding more cognitively challenging motor actions during walking may enhance functionally relevant brain connectivity. These findings align well with the hypothesis that increased connectivity in high-band frequencies may signal motor improvements following rehabilitation. 30
Taken together, the results of these 3 EEG studies reinforce the potential use of this technique to measure brain activity and connectivity as biomarkers to detect changes in cortical function in response to CE. CE has been shown to induce acute increases in brain activity among neurotypical individuals, increasing the amplitude in the P300 waveform 31 and enhancing power in both low and high-band frequencies. 32 Nevertheless, in stroke, more studies are needed to identify which specific EEG patterns provide the most sensitive measures to monitor the effects of CE on brain activity and connectivity and their associations with functional recovery.
Reflex Excitability
Reflexes evoked through both nerve and vibration stimulation can characterize mechanisms associated with neurophysiological integrity and neuroplasticity in both healthy individuals and neurological patients (Figure 1; Box 1). Following stroke, spinal networks tend to be relatively preserved, however, disruption in descending motor commands from the brain to the spine can negatively impact rhythmic motor limb activities such as walking or cycling. 33 Normalized modulation of reflex excitability accompanies improvements in motor function following motor training interventions in individuals after stroke. 34
Three studies examined the chronic effects of CE on cutaneous24-26 and stretch24,25 reflex excitability (Table 1). Reflexes were measured by capturing the response to nerve and vibration stimulation before and after 5 weeks of light-intensity CE while performing rhythmic motor tasks such as walking or arm and leg cycling. Upper-limb ergometry training induced a significant inhibition of cutaneous reflexes on the paretic side, resulting in more normalized amplitudes between the paretic and non-paretic sides. 24 Similarly, following 5 weeks of upper and lower limb ergometry, 2 studies reported enhanced bilateral symmetry of cutaneous reflexes that were driven by increases in excitability in the paretic side and decreases in the non-paretic side.25,26 Significant training-induced effects were also observed in stretch reflexes, where reductions on the paretic side led to more normalized patterns of excitability.24,25
In summary, these results provide preliminary evidence supporting the use of reflex excitability as a potential biomarker to assess neurophysiological changes following CE training in individuals poststroke. In non-neurological populations, changes in reflex excitability, measured with the H-reflex, have been reported following acute bouts of CE. 35 The studies reviewed revealed that CE training modulates both cutaneous and stretch reflexes, suggesting that this type of exercise can help restore the imbalances in reflex excitability typically observed between affected and unaffected limbs after stroke and promote neural activity patterns similar to those observed in neurotypical individuals. 34 However, whether these changes in reflex excitability can be used to predict improvements in functional recovery and thus guide clinical practice has yet to be demonstrated.
Neuroimaging Biomarkers
Brain Activity
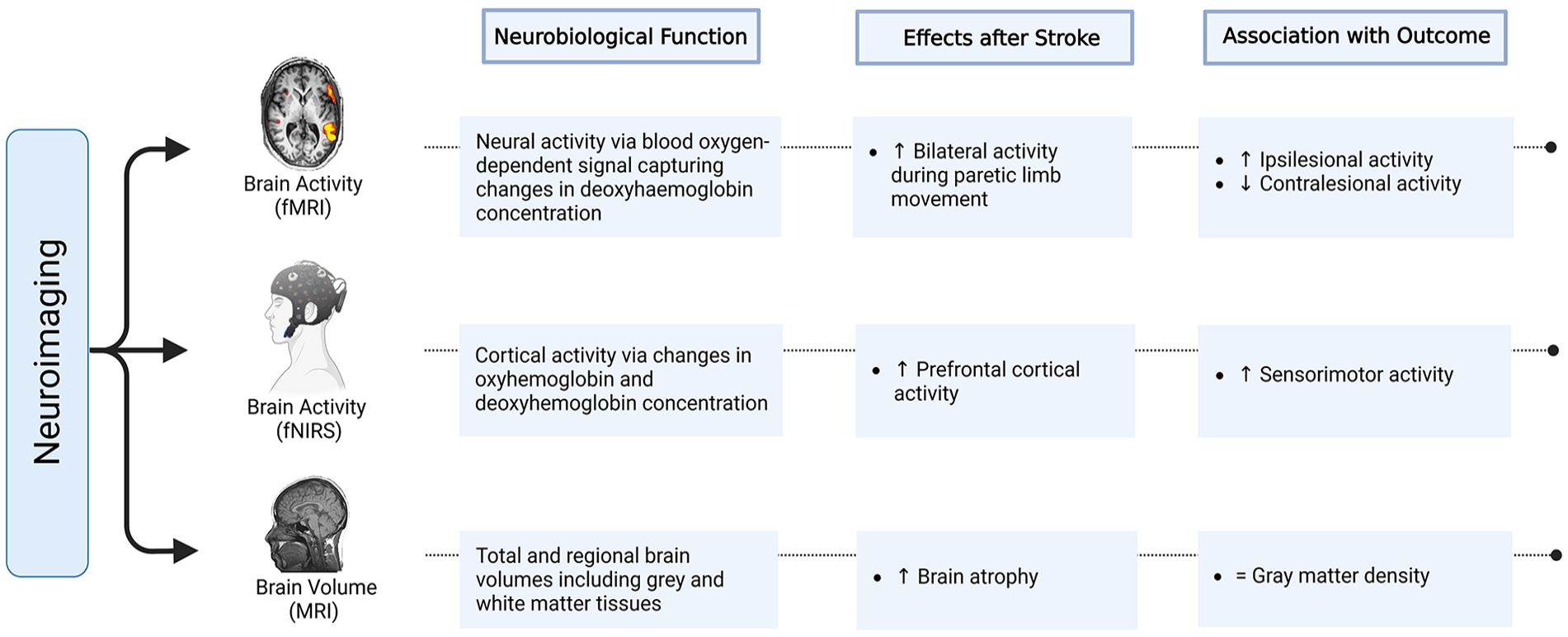
Besides EEG, brain activity can also be assessed using functional neuroimaging techniques that can monitor hemodynamic responses associated with changes in neural activity (eg, neurovascular coupling; Figure 2; Box 2). These neuroimaging techniques characterize recovery and can measure neuroplastic changes following different treatments poststroke. Functional magnetic resonance imaging (fMRI) based applications such as blood oxygen-level-dependent signal estimate changes in brain activity from fluctuations in the ratio of oxyhemoglobin and deoxyhemoglobin. Despite the idiosyncratic heterogeneity common in stroke, disproportionate increases in bilateral activity during the paretic hand movement have been reported in fMRI studies. 36 Normalized brain activity patterns via ipsilesional increases and contralesional decreases have been shown to be associated with better recovery after different rehabilitative motor inter-ventions. 37
Three of the 4 studies38-41 examining the effect of chronic CE on brain activity measured with fMRI reported significant changes after training (Table 2). One study with sub-acute ischemic patients undergoing 3 weeks of virtual reality-enhanced treadmill training reported augmented brain activity during paretic limb movement in the ipsilesional primary sensorimotor cortex and bilateral supplementary motor areas. 38 Furthermore, this increased activity on the ipsilesional sensorimotor cortex was positively associated with improvements in walking speed.
Main Characteristics of the Studies Including Neuroimaging Biomarkers.
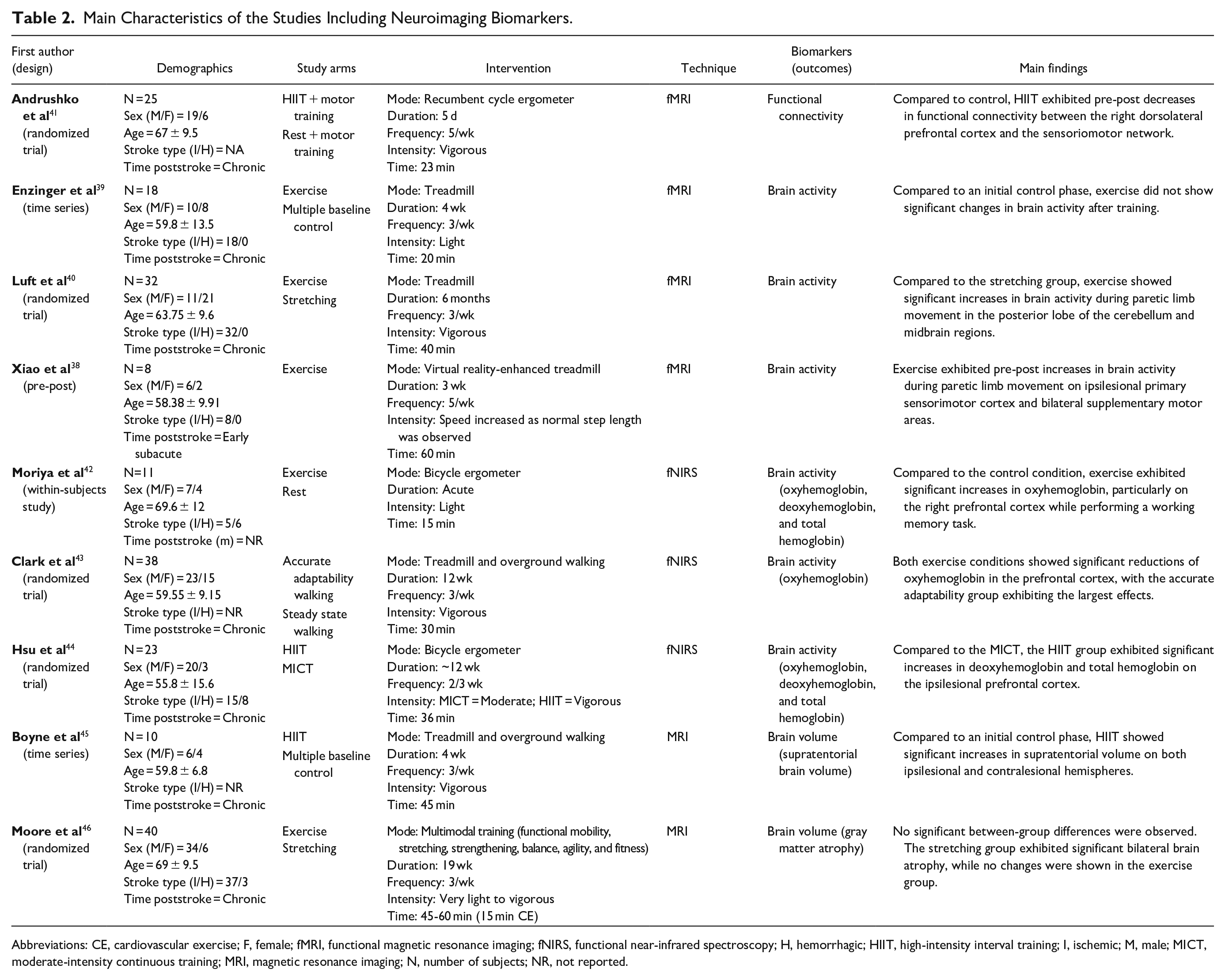
Abbreviations: CE, cardiovascular exercise; F, female; fMRI, functional magnetic resonance imaging; fNIRS, functional near-infrared spectroscopy; H, hemorrhagic; HIIT, high-intensity interval training; I, ischemic; M, male; MICT, moderate-intensity continuous training; MRI, magnetic resonance imaging; N, number of subjects; NR, not reported.
In another fMRI study, despite significant improvements in walking speed and endurance after 4 weeks of light-intensity treadmill training, no significant brain activity changes were observed. 39 However, improvements in walking endurance were positively associated with increases in brain activity in bilateral sensorimotor cortex, cingulate motor areas, caudate nuclei, and the ipsilesional thalamus. A third study reported significant increases in brain activity during paretic limb movement in cerebellar and midbrain regions that were correlated with walking speed gains after 6 months of vigorous-intensity treadmill training. 40 Finally, the most recent study showed significant decreases in resting-state functional connectivity between the right dorsolateral prefrontal cortex and the sensoriomotor network following 5 consecutive days of HIIT paired with motor training compared to a control group. 41 Regardless of the group, decreases in functional connectivity correlated to improved processing speed in a cognitive-motor task, suggesting a reduced dependence on cognitive resources to complete a demanding motor task.
Another neuroimaging technique that can estimate brain activity is functional near-infrared spectroscopy (fNIRS; Figure 2; Box 2). With fNIRS, brain activity is inferred from changes in oxyhemoglobin and deoxyhemoglobin concentration in superficial areas of the cortex. Studies using fNIRS have shown that stroke individuals performing motor tasks such as walking tend to over-activate the prefrontal cortex to compensate for motor deficits. 47 Furthermore, rehabilitative interventions such as intensive physical therapy have been shown to heighten fNIRS-measured cortical activity in brain regions responsible for the planning and acquisition of complex movements such as the supplementary motor areas. 48
The 3 studies that examined changes in brain activity using fNIRS revealed significant effects after CE42-44 (Table 2). One acute study comparing a single bout of 15 minutes light-intensity cycling to a resting control condition showed significant post-exercise increases in oxyhemoglobin on the right prefrontal cortex while performing a working memory task. 42 The remaining 2 studies examined the chronic effects of CE. In 1 study, when comparing 12 weeks of accurate adaptability walking to a steady state walking, both at vigorous intensities, the 2 groups exhibited significant decreases in prefrontal cortex oxyhemoglobin during walking, with the accurate adaptability group showing larger reductions. 43 However, no significant correlation was observed between brain activity changes and walking function post-intervention. Finally, another study examined intensity-dependent effects by comparing 12 weeks of cycle ergometry HIIT vs. MICT, 44 with the HIIT group exhibiting larger increases in deoxyhemoglobin and total hemoglobin on the ipsilesional prefrontal cortex during a graded exercise test.
In summary, fMRI studies have provided inconsistent results in terms of changes in brain activity after chronic CE interventions although associations with changes in function were observed in all the studies analyzed. Taken together, the results of the fNIRS studies showed that a single bout of light-intensity CE elevated oxyhemoglobin in the prefrontal cortex while chronic interventions resulted in significant reductions in oxyhemoglobin and increases in deoxyhemoglobin and total hemoglobin, suggesting increased and/or more efficient brain oxygen utilization. In neurotypical populations, CE interventions have been shown to increase brain connectivity, as measured by fMRI, in regions subserving motor and cognitive processes. 49 Additionally, in fNIRS studies, a single bout of CE has shown significant increases in prefrontal cortex activity, 50 while chronic interventions resulted in reduced activity. 51 Despite these promising findings, to validate fMRI and fNIRS as potential biomarkers in response to CE, further studies should investigate whether such changes in neural activity are associated with improvements in behavioral outcomes.
Brain Volume
Structural neuroimaging techniques such as magnetic resonance imaging (MRI) provide relevant information regarding the structural integrity of the CNS, improving our capacity to predict recovery outcomes poststroke and monitor treatment response following rehabilitative interventions (Figure 2; Box 2). In stroke, functional impairment is directly associated with the extent of structural damage in the brain. 52 Total and regional brain volumes measured with MRI tend to show accelerated atrophy following brain ischemia. Indeed, accelerated brain atrophy is a common hallmark in stroke that correlates with residual motor and cognitive deficits as well as reduced improvements in motor function in response to rehabilitation. 53
Structural MRI studies in neurologically intact older populations have shown that CE can protect against aging-related brain atrophy by preserving or even increasing brain volumes. 54 In agreement with this evidence, 2 studies also showed that chronic CE can preserve or increase brain volumes in stroke survivors45,46 (Table 2). The first study compared changes in brain volume after 4 weeks of walking HIIT and a control phase with no intervention. 45 Following HIIT, the supratentorial volume of both ipsilesional and contralesional hemispheres exhibited significant increases compared to the control phase. The other study compared a 19-week multimodal exercise program, which included 15 minutes of CE per session, to a stretching control group. 46 Despite no differences between groups, the control group was the only one to exhibit significant pre-post bilateral atrophy of the medial temporal lobe, while in the exercise group, brain volumes remained preserved. The reason why 1 study showed volume increase 45 and the other preservation 46 is not clear, but could be due to differences in the CE interventions (eg, 4 vs 19 weeks of training) or the areas of the brain investigated (supratentorial vs medial temporal lobe). Regardless, these findings suggest that CE may potentially confer protection from the rapid atrophy that the brain experiences poststroke and emphasize the potential use of structural MRI biomarkers such as brain volume to detect neuroplastic changes in response to CE.
Blood Biomarkers
Brain-Derived Neurotrophic Factor
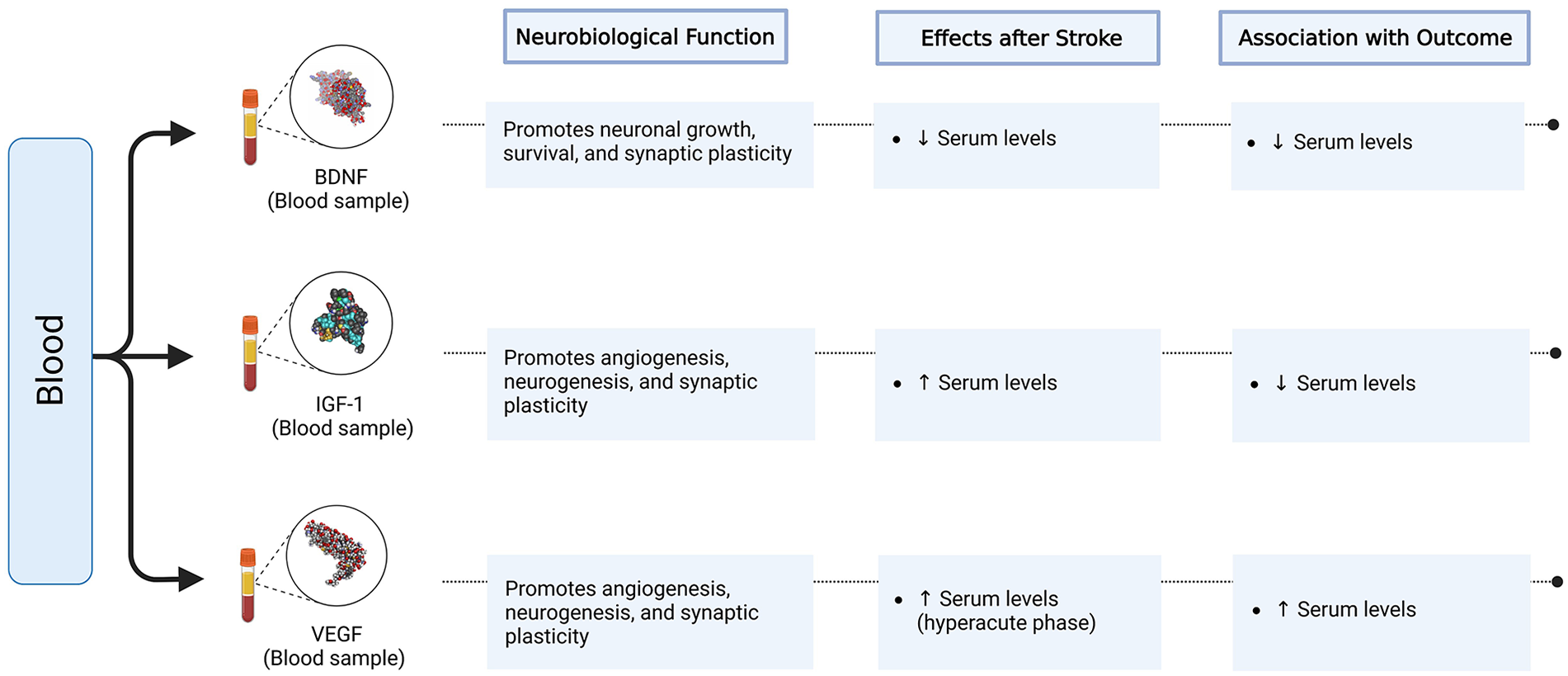
The inaccessibility to directly study molecular changes in the human brain makes blood biomarkers collected peripherally potential surrogates of central neurobiological processes and recovery poststroke (Figure 3; Box 3). Brain-derived neurotrophic factor (BDNF) is the most abundant neurotrophin in the brain, playing a central role in neuronal growth, survival, and synaptic plasticity. 55 Animal studies confirm that ensuring BDNF availability following brain ischemia is critical for promoting neuroplasticity, recovery, and rehabilitation-induced motor improvements. 56
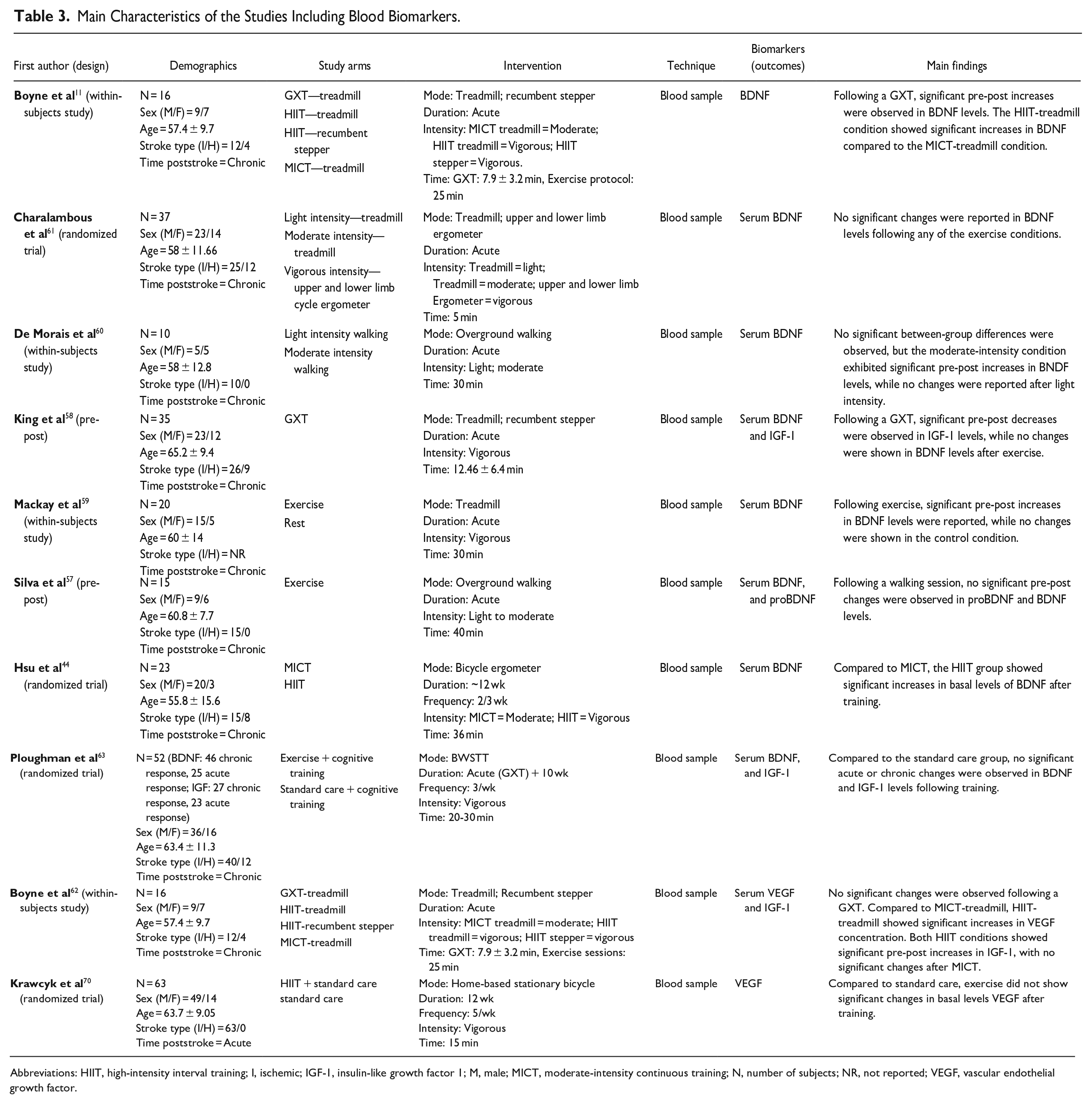
Six studies investigated acute BDNF changes after a single bout of exercise,11,57-61 with 3 showing significant changes (Table 3). One study revealed that 30 minutes of treadmill CE at vigorous intensity promoted significant increases in BDNF levels, while no changes were observed in the resting control group. 59 However, no significant associations between CE-induced BDNF changes and post-exercise improvements in the performance of a sensorimotor adaptation task were found.
Main Characteristics of the Studies Including Blood Biomarkers.
Abbreviations: HIIT, high-intensity interval training; I, ischemic; IGF-1, insulin-like growth factor 1; M, male; MICT, moderate-intensity continuous training; N, number of subjects; NR, not reported; VEGF, vascular endothelial growth factor.
Three studies examined the intensity-dependent effects of a single bout of CE on BDNF concentrations.11,60,61 Twenty-five minutes of treadmill CE showed significantly larger BDNF increases following HIIT compared to MICT. 11 Furthermore, in the same study, significant increases in BDNF were observed following a maximal treadmill graded exercise test. In another study, walking at moderate intensity for 30 minutes resulted in greater BDNF elevation than walking at light intensity. 60 Finally, compared to 5 minutes of treadmill walking at light intensity, 5 minutes of moderate-intensity treadmill or vigorous-intensity ergometry did not elicit significantly larger increases in BNDF levels. 61
Only one of the 2 studies44,63 examining the chronic effects of CE in BDNF reported significant changes following training (Table 3). Ploughman et al 63 examined the interaction between chronic and acute responses to CE by measuring basal BDNF levels post-training as well as before and immediately after a graded exercise test. Compared to a group undergoing standard therapeutic activity, 10 weeks of vigorous-intensity treadmill training did not induce any acute or chronic significant change in BDNF. Intensity-dependent effects were investigated in another study comparing 12 weeks of cycling MICT and HIIT. 44 The HIIT group showed significantly greater increases in basal BDNF concentrations following training.
BDNF secretion in response to CE is highly variable and can be influenced by multiple factors. In non-disabled individuals, while peripheral levels of BDNF transiently increase following acute CE, especially when performed at higher exercise intensities, the long-term effects of chronic CE interventions are less consistent. 64 The results analyzed here indicate similar findings in stroke survivors, with circulating levels of BDNF transiently increasing following single vigorous exercise sessions and, less consistently, after a period of chronic CE. In any event, whether the peripheral upregulation of BDNF triggered with CE translates to improvements in recovery has yet to be demonstrated.
Insulin Growth Factor 1
Insulin growth factor 1 (IGF-1), a pleiotropic protein involved in neuroplasticity and neurogenesis, promotes the upregulation of BDNF expression and vascular endothelial growth factor (VEGF) production in the brain (Figure 3; Box 3). In animal models, elevated IGF-1 expression has been associated with improvements in recovery poststroke and neural repair through neovascularization and neurogenesis. 65 In people poststroke, similar findings support the association between increased IGF-1 levels and improved motor outcomes. 66 Research in neurotypical individuals has reported disparate results following CE, with most studies showing increases in circulating IGF-1 in response to acute CE 67 and chronic studies reporting reductions in basal levels at the end of the training intervention. 68
Two of the 3 studies58,62,63 examining CE-induced effects on IGF-1 poststroke reported significant changes (Table 3). One study reported significant reductions in IGF-1 levels following a graded exercise test. 58 Another study investigated the intensity-dependent effects of circulating IGF-1 by comparing a single bout of HIIT to MICT. 62 Although no differences were observed between groups, 25 minutes of HIIT on either treadmill or recumbent stepper promoted significant increases in IGF-1 levels, while no changes were reported following treadmill MICT. Finally, Ploughman et al 63 examined the acute and chronic responses on IGF-1 concentrations, with no significant changes following 10 weeks of vigorous-intensity treadmill training paired with cognitive training.
Vascular Endothelial Growth Factor
Besides playing a central role in angiogenesis, VEGF is an essential protein regulating neurogenesis and synaptic plasticity via stimulation of neural stem cells, endothelial cells, and production of BDNF and IGF-1 (Figure 3; Box 3). In stroke, the overexpression of VEGF during early stages of recovery has been associated with suboptimal recovery. In contrast, in later stages poststroke, increased VEGF has been associated with neuroprotective effects facilitating recovery. 69
In neurotypical populations, CE upregulates VEGF following acute and chronic CE.67,68 In stroke survivors, 2 studies were identified examining this neurotrophin in response to CE,62,70 with only one reporting significant changes (Table 3). Intensity-dependent effects on circulating VEGF were investigated by comparing a single 25-minute bout of treadmill HIIT and MICT. 62 Following the HIIT intervention, VEGF concentration levels increased significantly compared to MICT. Chronic effects were also investigated by comparing 12 weeks of home-based bicycle HIIT to standard care in patients at acute stages poststroke. 70 Compared to standard care, no significant changes in basal VEGF levels were reported following exercise.
Gaps and Future Directions
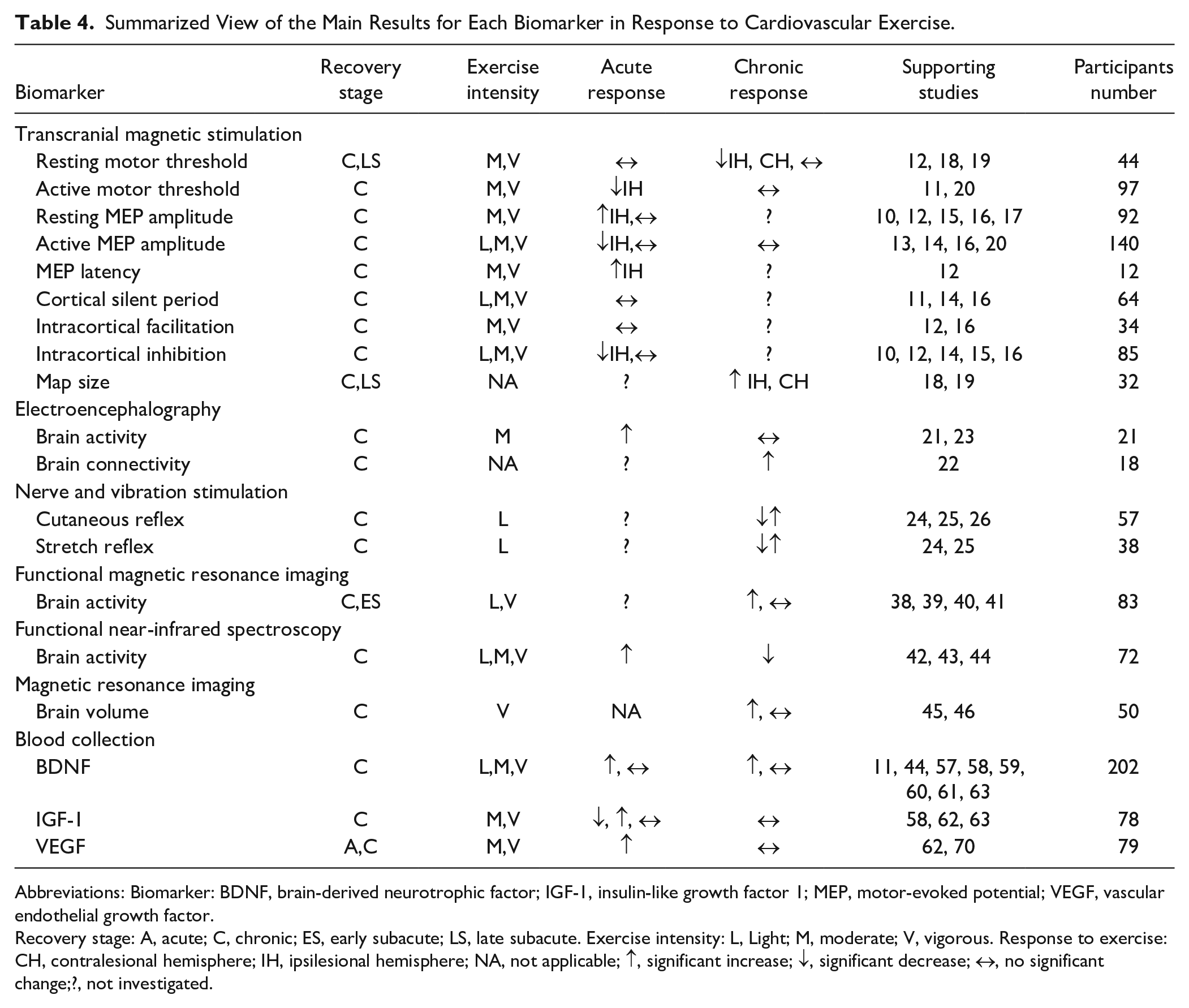
This paper presented a critical analysis regarding the use of biomarkers to assess the neuroplastic response to CE in individuals poststroke. The summarized view of the main results for each biomarker is presented in Table 4. From a methodological perspective, it should first be noted that only a few large studies examined the effects of CE on biomarkers after stroke, with the majority (78%) comprising studies with small sample sizes (n ≤ 30). Furthermore, only 14 studies (41%) were RCTs with a comparative non-exercise control group, which is essential to determine any causal effects induced by the CE. To draw more definitive conclusions, future CE studies using biomarkers to assess neuroplasticity should be carefully designed and adequately powered RCTs including a control group not receiving the exercise intervention.
Summarized View of the Main Results for Each Biomarker in Response to Cardiovascular Exercise.
Abbreviations: Biomarker: BDNF, brain-derived neurotrophic factor; IGF-1, insulin-like growth factor 1; MEP, motor-evoked potential; VEGF, vascular endothelial growth factor.
Recovery stage: A, acute; C, chronic; ES, early subacute; LS, late subacute. Exercise intensity: L, Light; M, moderate; V, vigorous. Response to exercise: CH, contralesional hemisphere; IH, ipsilesional hemisphere; NA, not applicable; ↑, significant increase; ↓, significant decrease; ↔, no significant change;?, not investigated.
The evidence reviewed herein suggests that there is little consensus regarding which biomarkers could best capture the neuroplastic changes taking place in response to CE and the implications for functional recovery after stroke. In most cases, the rationale for selecting the specific biomarker was not clearly articulated and presumably based on the availability of a specific technique rather than because the chosen biomarker was the most appropriate to investigate a specific aspect of neuroplasticity. Furthermore, associations between changes in biomarkers and recovery outcomes were either not investigated or not reported. Clearly, more investigation is needed to identify the most appropriate biomarkers to assess the neuroplastic effect of CE, standardize how they should be assessed and determine their implications in stroke recovery. In the next sections, we discuss the most important gaps in knowledge identified and suggest strategies to improve future studies.
Selection of Biomarkers
Lack of consensus and methodological quality issues such as the absence of validation, lack of association with clinically important differences, and small sample sizes are the main issues using biomarkers in stroke. 71 This critical view aligns well with the evidence collected here in response to CE. When designing CE studies, it is important to select biomarkers, which are supported by the strongest scientific evidence and, ideally, are also associated with changes in recovery outcomes that are clinically relevant (see next section). 72 The studies reviewed here that used techniques such as TMS, fMRI, or fNIRS, varied widely in their choice of primary measures, targeted brain regions, and timing of assessments. This heterogeneity contributed to the already large variability in the response to CE between individuals with stroke, making it difficult to compare results across studies and to determine the potential true effects of CE on neuroplasticity. Such variability undermines the understanding of which biomarkers and techniques can best capture mechanisms related to neuroplasticity and recovery. 5 Moreover, in addition to its effects on the nervous system, it is also important to consider the influence of CE on other mechanisms, including metabolic, vascular, or inflammatory processes. These mechanisms can also be independently implicated in the recovery process and may both interact with and influence neuroplasticity mechanisms. Finally, it is critical that advances in biomarkers progress in parallel with the evidence derived from preclinical animal models of stroke. The establishment of translational research, functioning in a bidirectional and iterative manner between animal and human studies is essential to enable the comparison and validation of biomarkers. Overall, this information is critical not only to develop more precise and relevant biomarkers for stroke recovery but also to improve the measurement of treatment-induced neuroplasticity and create a better consensus for establishing consistent methodological procedures for future studies.
Assessment of Function
Improving functional recovery through neural repair and plasticity is one of the primary goals of stroke rehabilitation.73,74 While behavior is undeniably the ultimate determinant of treatment effectiveness, a mechanistic understanding is essential for identifying biological targets to help elucidate the potential reparative capacity of an intervention or lack thereof, as well as for tailoring its application to maximize its effect on recovery. However, to determine the functional validity of a specific biomarker, it is essential to examine whether it is associated with recovery outcomes. 72 While most studies (78%) included functional measures to study the effects of CE on recovery, only a few (37%) investigated the association between behavior and biomarker changes. Although associations cannot confirm causality, without this analysis, it is impossible to determine whether neuroplasticity changes induced by CE can have a potential positive effect on functional recovery. To determine the neural reparative capacity of CE in people after stroke, future studies should investigate and report the associations between biomarker change and outcome improvement in response to this type of training. 75 Furthermore, in order to better capture mechanisms of true neuroplasticity and brain repair it is essential that future studies include the assessment of impairment in addition to activity limitation and participation outcomes. 74
Characterization of Patients
The characteristics of the brain injury and baseline function directly impact the individual’s capacity to recover after stroke. 76 Unlike animal models, where ischemic-induced lesions can be precisely induced, clinical studies include patients presenting with a broad range of lesion sizes, locations, and resulting impairments. This variability increases heterogeneity and limits the ability to determine the reparative potential of rehabilitative interventions. Most of the studies reviewed (79%) classified stroke types as either ischemic and hemorrhagic, with only a few (29%) providing more detailed information on aspects such as size and location of the stroke. Similarly, while most studies (95%) provided some baseline measures of severity, impairment, or disability, these measures varied significantly, with only a few following consensus-based recommendations. 75 Stratifying patients while ensuring generalizability will require concerted efforts in designing multisite studies to increase sample sizes. Ultimately, this is the only way to investigate how the characteristics of the patient can affect the neuroplastic response to CE. Furthermore, we observed that most patients in the selected studies presented mild degrees of disability and mobility problems, suggesting recruitment bias toward less disabled individuals. Selection bias, which is a recurrent issue in stroke rehabilitation research, may lead to overlook the potential therapeutic effects of CE in a substantial portion of the stroke population.
Consideration of Recovery Stage
Research in animals and humans has identified distinct critical timepoints after stroke, each involving unique neurobiological processes that interact with recovery. 73 While functional recovery can occur during chronic stages, a critical period for recovery exists within the first weeks to months post-stroke, when most functional improvements take place, and where greater gains can be achieved in response to rehabilitation.77,78 It is unclear if this optimal window of opportunity also applies to the introduction of CE. 79 Furthermore, the large majority (95%) of studies identified focused on patients at chronic stages poststroke (>6 months), while only a few included individuals from earlier stages. This constitutes a significant gap in the literature that limits the understanding of how CE interacts with the unique time-dependent neurobiological processes that occur after stroke. Furthermore, is important to note that promoting neuroplasticity is not always beneficial. The results from many animal studies 80 and indirect evidence from humans studies 81 suggest that, especially during very acute phases of recovery, the brain is highly sensitive to further stressors, including physical exercise. These stressors may exacerbate infarct lesions and impact behavioral outcomes by altering different aspects of brain activity. Clearly, more clinical research is needed to determine the optimal timing where CE should be introduced after stroke and how it should be implemented to ensure that any potential neuroplastic effect leads to a positive outcome for these patients. 74
Quantification of Exercise Stimulus
Individualizing exercise workloads and monitoring training stimulus is critical to minimize variability in response to CE and to better understand any potential dose-response relationship in neuroplasticity. Exercise stimulus in stroke patients can be quantified using the FITT (frequency, intensity, time, and type) principle. 82 Furthermore, a symptom-limited graded exercise test can increase safety and enable the accurate individualization of workloads based on each patient’s capacity. 83 Although all the reviewed studies reported and defined their exercise parameters, there was heterogeneity in the types of measures used, and only 34% of the studies employed an exercise test to individualize workloads. Employing well-established measures to quantify both internal and external exercise workloads would permit the accurate monitoring of training stimuli in patients with varying degrees of neurological impairment and fitness and examine potential associations with neuroplastic responses. Identifying significant associations will allow us to be more precise in the prescription of CE with the aim of promoting neuroplasticity. Finally, it is crucial to note that while studies performing a single exercise session can provide valuable mechanistic insights regarding the acute neurobiological responses to CE, whether these changes can be considered neuroplasticity, understood as persistent change in neural networks and synaptic connections is still open to debate. Implementing longitudinal interventions, coupled with measurements of neuroplasticity that capture more persistent effects, is indispensable to determine the potential effects of CE and their impact on recovery. 7
Summary
Given its multiple benefits, CE should be a core component of stroke rehabilitation. Preclinical evidence has linked CE-induced gains in functional recovery to neuroplastic changes in the nervous system. The use of biomarkers has opened a unique opportunity to investigate neuroplasticity processes during recovery and in response to treatment after stroke in humans. Although some biomarkers appear to be responsive to the effects of both acute and chronic CE interventions, the evidence supporting their use is still inconsistent. Small sample sizes, methodological variability, lack of information regarding patient’s characteristics, and inadequate standardization of CE parameters, in addition to lack of reporting of associations with functional outcomes, are the main barriers precluding the quantification of the true reparative neuroplastic effects of CE poststroke. To advance our mechanistic understanding of the impact of CE on neuroplasticity and recovery in people after stroke, it is imperative that we address all gaps and methodological issues identified in this paper. Only by addressing these challenges, we will be able to uncover the potential reparative capabilities of this intervention and inform clinical practice.
Supplemental Material
sj-docx-1-nnr-10.1177_15459683231223513 – Supplemental material for Measuring Neuroplasticity in Response to Cardiovascular Exercise in People With Stroke: A Critical Perspective
Supplemental material, sj-docx-1-nnr-10.1177_15459683231223513 for Measuring Neuroplasticity in Response to Cardiovascular Exercise in People With Stroke: A Critical Perspective by Bernat De Las Heras, Lynden Rodrigues, Jacopo Cristini, Kevin Moncion, Michelle Ploughman, Ada Tang, Joyce Fung and Marc Roig in Neurorehabilitation and Neural Repair
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: During this study, BDH and JC received doctoral scholarships from Fonds de La Recherche de Québec Santé (FRQS). KM is supported by an Ontario Graduate Scholarship. MR received a Salary Award Junior II from FRQS.
Supplementary material for this article is available on the Neurorehabilitation & Neural Repair website along with the online version of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.