
Abstract
Background
Parkinson’s disease can negatively affect vocal functioning and social wellbeing, particularly in the latter stages of disease progression. Face-to-face group singing interventions can improve communication and wellbeing outcomes, yet not all people can access in-person sessions. To help overcome barriers to participation, exploration of the feasibility and utility of online therapeutic singing programs is needed.
Objectives
To evaluate the feasibility, acceptability, and preliminary efficacy of a 12-week ParkinSong Online intervention on speech and wellbeing for people with Parkinson’s disease.
Methods
A total of 28 participants with idiopathic Parkinson’s disease were recruited to a single-arm feasibility study. Weekly 90-minute online sessions were co-facilitated by a music therapist and speech pathologist. Speech and wellbeing assessments were conducted pre and post intervention. Participant and facilitator surveys were administered after each session, with focus group interviews at the end of the program.
Results
The recruitment rate was high (90%) with no attrition, adverse events, or safety issues. There was good intervention fidelity, attendance (average 89%), and positive participant experience. Feasibility was good, with technology reported as the main challenge (connecting and navigating Zoom). No improvements were seen in voice measures or wellbeing outcomes in this small trial. The online format used in this study did not provide the same benefits as in-person ParkinSong sessions.
Conclusions
ParkinSong Online is feasible for recreational purposes and social engagement provided that people have adequate technological knowledge or support. The optimal online delivery format to achieve communication improvements in Parkinson’s awaits confirmation.
Introduction
People living with Parkinson’s disease, a progressive neurological disorder affecting movement and cognition, 1 frequently experience motor symptoms affecting their voice and breathing that impact their psychosocial wellbeing.2-7 To ameliorate these symptoms, in-person group singing interventions have been advocated, with research demonstrating improvements in vocal loudness and voice-related quality of life.8-12 Such interventions are based on neuroscientific evidence showing that singing shares neural circuitry with speaking, 7 and demands greater respiratory support and vocal effort than speaking. 13 Considering restrictions to movement during the COVID-19 pandemic, and in response to geographical or economical barriers to accessing in-person singing interventions, there is a pressing need to investigate alternative delivery formats, such as using online platforms, to maintain and improve accessibility of therapeutic group singing programs for people with Parkinson’s and related disorders. 14
Telehealth and virtual clinic consultations for people with Parkinson’s have been found to have similar benefits to in-person visits for a range of activities, such as exercise, 15 dance therapy,16,17 and cognitive-behavioral therapy, 18 with the added value of reducing time and financial costs.19,20 Increasing use of telehealth has also meant that Parkinson’s measures typically administered in-person needed validation for online administration.21,22
There has been little research on online or remote delivery platforms for group singing interventions for people with Parkinson’s. A pilot study used pre-recorded vocal and singing exercises for 2 Parkinson’s groups in rural areas. 23 In this study 10 participants met together in local community venues where recordings were projected onto a large screen for participants to follow. A similar pattern of results was achieved to a parallel in-person group singing intervention. 24 Another small randomized trial reported a reduction in dysphagia symptoms following a combined singing and speech therapy program for 35 individuals with Parkinson’s delivered via telehealth. 25
Recent surveys have shown that many different formats for online choirs were used during the COVID-19 pandemic and that similar themes emerged for therapeutic and non-therapeutic choirs alike, particularly surrounding technology issues.26,27 The primary limitation for online group singing is latency, or lag time, necessitating the use of the mute function while participants sing along with a facilitator. This inherent latency in videoconferencing platforms makes synchronous group music-making difficult to achieve online. Solutions for reducing online latency are emerging, but these currently require additional equipment and technological set up that is too complex for many novice users. While there is evidence that in-person singing groups have therapeutic value for diverse populations 28 including those with Parkinson’s,29,30 stroke,31,32 mental health conditions such as anxiety and depression,33,34 dementia,29,30 and chronic obstructive pulmonary disease, 35 there is little evidence for functional, social, or health-related benefits of online singing groups. The feasibility and potential benefits of an interactive online group singing approach, where participants join from individually convenient locations (eg, home), with pre and post assessments also completed online, have not been explored. It is important to explore the feasibility of remote data collection, both from an equity perspective (ie, allowing recruitment of geographically remote participants and reducing participant burden to travel for assessments), as well as to reduce risks related to infection control with vulnerable populations (particularly in the context of COVID-19). Remote data collection also provides an opportunity to minimize missing data. The growing need for alternative and accessible delivery models, in combination with the lack of research evidence, justify the need to explore online models for therapeutic singing groups. The aim of the current study, therefore, was to investigate the feasibility, acceptability, and preliminary efficacy of a 12-week online singing intervention (ParkinSong Online) and the feasibility of completely online data collection.
Methods
The ParkinSong Online feasibility study was designed to investigate the viability of adapting the usual in-person ParkinSong group intervention into an online format during the COVID-19 pandemic. The target sample size was 30 participants (2 groups of 15). Both groups received an identical experimental protocol, with separation into 2 groups due to maximum size limits for therapeutic and practical purposes only. Eligibility criteria included: a diagnosis of idiopathic Parkinson’s; no previous neurological, head and neck, or respiratory disorders; no visual or auditory impairment not remedied by aids; English speaking, a computer with high-speed internet (≥10 mbps download; 1 mbps upload) and web camera; available for the dates of the study; and Montreal Cognitive Assessment 36 (MoCA) score ≥ 18 (or if between 10 and 17, a carer was required to assist the participant for each session). Initial phone screening for eligibility, safety, and environmental assessment was conducted prior to obtaining informed consent from all participants via REDCap, 37 an electronic data capture tool hosted at the University of Melbourne. Ethics approval was provided by the University of Melbourne Human Research Ethics Committee (2021-14465-16053-3); and a peer reviewed protocol was published prior to commencement of data collection. 14 Due to recruitment challenges, 1 change from the published protocol paper was the relaxing of the required condition of “reported changes in communication” (self-reported or reported by their caregiver or health professional); nevertheless 81% (n = 25) of participants still met this criterion. Recruitment was conducted through Fight Parkinson’s with the study promoted via online advertisements, email distribution, and referrals from local speech pathologists. Following initial telephone screening and consent, a time was scheduled to complete stage 2 of the screening (online administration of the MoCA, and the baseline assessment).
Measurements
The main measure of intervention effect was speech loudness during conversational speech (ie, monolog). The hardware configuration was piloted and calibrated using a sound pressure level meter. This was then piloted in a patient to ensure compliance. Reliability and consistency of metrics of interest were examined and confirmed prior to data collection. We also assessed speech loudness in terms of sound pressure levels during reading (Rainbow passage), reading over background noise (crowd noise played through headphones), and an instructed loud phrase. The background sound file intensity was set at 85 dB during the recording process. All participants were provided with headset microphones (Microsoft LifeChat LX-3000 USB microphone) containing in-built headphones to control the proximity of sound source to receiver (ear). Other voice outcomes included: maximum phonation time, syllable repetition (diadochokinetic rate), and composite scores of intelligibility, naturalness, and disease severity. 38 Composite scores were calculated using a combination of acoustic features representing vocal control, voice quality, and timing derived from tasks within the speech battery. The composites are proprietary of Redenlab and have been validated against perceptual ratings conducted by 2 expert raters blinded to disease and severity (N > 1000). Speech and voice data were captured at baseline and follow up time points using Redenlab Online™ remote data collection software (via participant computers) with a headset microphone (at a mouth-to-microphone distance of 10 cm) connected to the participant’s computer. Data were sampled at 44.1 KHz, 16-bit quantization and saved via lossless .wav format.
Adherence to study requirements was optimized through several approaches, including standardised hardware, software, training, and stimuli. Hardware was standardized via a USB-connected head-mounted microphone. This was selected to mitigate potential challenges of bring-your-own-device protocols and variable mouth to microphone distances (important for loudness outcomes). USB-based microphones bypass inbuilt sound cards, converting analogue signals to digital signals before they reach the device. This plug and play approach is easy to use. Participants received training on the study protocol and a mock run was elicited prior to formal testing. Speech tasks are brief, can be easy to produce, stable in the absence of true change, and are used across multiple neurological populations.39-41 Recording protocols were designed and implemented based on recommendations from multiple method studies and expert reviews.42-46
Quality of life and wellbeing measures administered at baseline and follow up assessments included the Dysarthria Impact Scale, 47 Depression Anxiety and Stress Scale (DASS-21), 48 and Lille Apathy Rating Scale—Short Form (LARS-SF). 49 To measure Parkinson’s symptoms at baseline and follow up, the following measures were used: the Parkinson’s Disease Questionnaire (PDQ-39) 50 and a modified Movement Disorder Society – Unified Parkinson’s Disease Rating Scale (MDS-UPDRS) for online assessment (tests of rigidity and postural instability omitted for Part III motor assessment).21,22,51
Participants completed a brief survey before and after each ParkinSong Online session to confirm they were in a hazard-free environment and to capture self-reported mood and energy levels using the Affect Grid. 52 Participants were asked to report any practice between sessions using ParkinSong Online materials or other singing resources. A post-session survey captured participants’ overall experience of each session using a 5-point Likert scale. Survey questions included rating engagement in vocal and singing exercises, enjoyment of the session, and any difficulties related to the vocal exercises, songs, or technology. At the end of the intervention period, the Acceptability, Appropriateness, and Feasibility of Intervention Measure (AAFIM) 53 was completed by facilitators, and participants were invited to take part in focus group interviews about their experiences.
Intervention
The ParkinSong Online protocol consisted of 12 weekly 90-minute sessions based on our previous face-to-face intervention, 9 but delivered via Zoom. Group size was limited to no more than 16 participants to maximize potential for individualized therapeutic intervention and group connection. Each group was co-facilitated by a music therapist and a speech pathologist using a transdisciplinary approach and optimizing Zoom audio settings for live music sharing (ie, “Original sound for musicians” and “High-fidelity music mode”). The format of each session was developed by the facilitators, within general guidelines provided by a facilitator manual and informed by participant preferences for genres of music and specific songs. A typical session consisted of breathing exercises and vocal singing warmups (approximately 15 minutes), speech exercises (approximately 10 minutes), intensive high effort singing, that is, with a strong focus on respiratory support, vocal technique, and loud vocal projection, as opposed to singing for purely recreational purposes (approximately 35 minutes), and finally 30 minutes of social communication practice in small groups (using the breakout group function of Zoom). Within this format, facilitators educated participants on optimal posture and vocal care for voice projection, muted participants as required during the voice exercises and singing, and facilitated social interactions in the breakout groups to practice using techniques taught during the first part of the session. Due to latency issues, participants were required to stay muted whilst singing. They could therefore only hear their own voice and the facilitator’s voice. The singing and voice exercises part of the sessions was recorded and made available to participants via a secure online platform (Canvas) hosted by the University of Melbourne for practice during the week and to catch up on missed sessions. These recordings were also used for fidelity checking of adherence to the intervention protocol.
Outcomes Analysis
Feasibility results for recruitment, retention, fidelity, safety, attendance, and acceptability, are reported descriptively. Baseline and follow up data for preliminary efficacy testing were analyzed using descriptive and inferential statistics (pairwise comparisons) with IBM SPSS Statistics version 27. 54 Qualitative interview data were analyzed using thematic analysis 55 with an inductive approach. To ensure a rigorous analysis, 1 author became familiar with the interview data, generated initial codes, and used these to develop themes. From here, a second author reviewed and verified the codes and themes generated, and suggested new themes.
Costs Analysis
Intervention costs were estimated, including facilitator and technical support costs. Computer and internet costs were not included as these are already available for most people and the Zoom video conferencing software was free. Although each group was designed to have a maximum of 16 participants, we conservatively estimated facilitator costs for 14 participants, which would be closer to an implementation scenario (15% vacancy in each group). For travel costs, we estimated the cost of car travel, 56 plus a conservative 1 hour per session for a carer to drive a participant to a face-to-face session. Travel costs were calculated by multiplying the distance by AUD$0.72/km, using cents-per-kilometer methods to claim business deductions per the 2021 to 2022 Australian Tax Office Guidelines with conservative estimates of 10 to 30 km distance traveled. Transportation time costs were calculated using the Fair Work Ombudsman Passenger Vehicle Transportation Award (MA000063) grade 3 ordinary hour rate in December 2022 of AU$ 31.05 per hour.
Results
Recruitment commenced in March 2022 and ceased in April 2022 when a total of 28 participants with idiopathic Parkinson’s (16 male) were recruited, with a recruitment rate of 90% and no dropouts during the 12 weeks of online sessions. Recruitment rate is an upper estimate based on number of REDCap screening surveys opened; some initial inquirers may have been identified as not eligible before proceeding to screening in REDCap. Figure 1 shows the participant flow through the study. Group A ran from 31st March to 16th June 2022 and Group B ran from 2nd June to 18th August 2022.
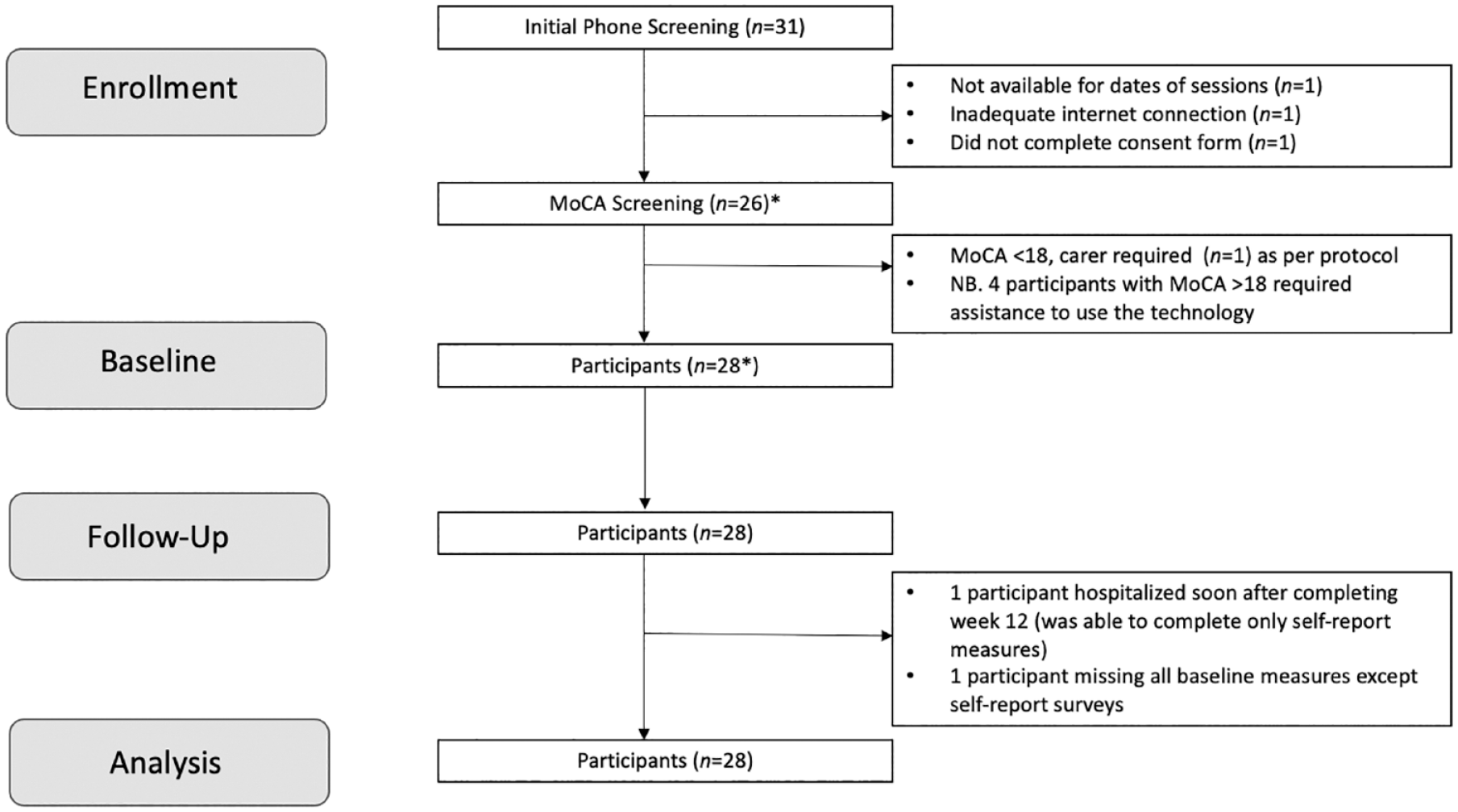
CONSORT flowchart.
Baseline demographics are presented in Table 1. Most participants were in the earlier stages of disease progression and had minimal cognitive impairment. Twenty-five participants were taking Levodopa medication over the course of the intervention and 4 participants had received deep brain stimulation more than 6-months prior to enrolment. The majority enjoyed singing and half had previously attended group singing activities.
Baseline Demographics.
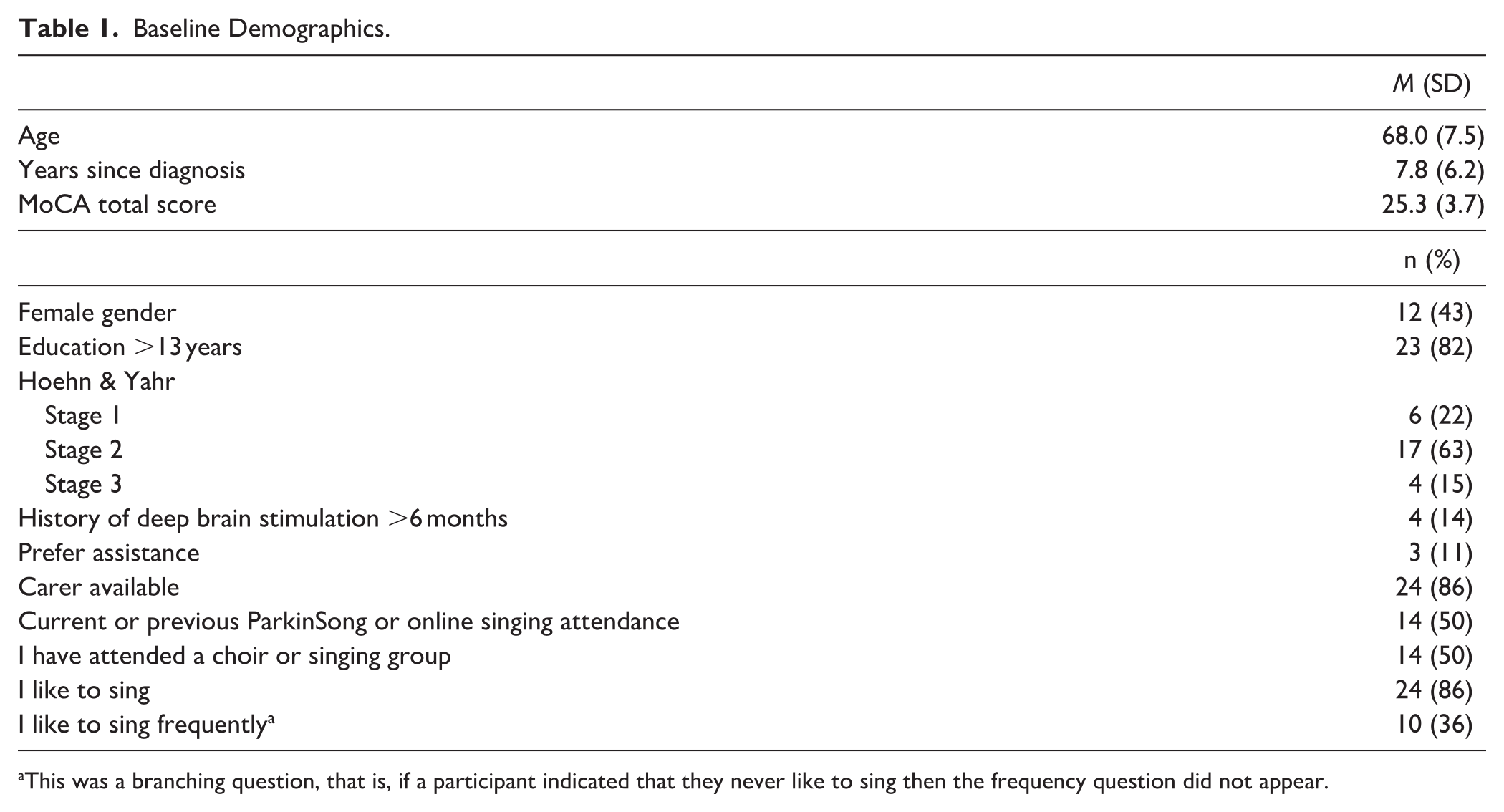
This was a branching question, that is, if a participant indicated that they never like to sing then the frequency question did not appear.
Session attendance was high, ranging from 67% to 100% or 8 to 12 sessions, with average compliance 89% or 10 to 11 sessions. Reasons given for absenteeism included accidents, injuries, operations, poor sleep the night before, previously planned trips or social events, and unforeseen family demands. There were no adverse events or safety issues reported. Intervention fidelity (determined from session recordings) and acceptability (determined from facilitator and participant feedback) were high. Online intervention costs included staffing costs totaling AUD$586 per participant for the 12-week program or AUD$41 per session. In comparison, in a hypothetical scenario where participants would spend 1 hour for a 30 km round trip to attend 12 in-person sessions, it would cost AUD$ 632 or AUD$53 per session.
There were no improvements in any secondary (preliminary efficacy) outcomes from pre- to post-intervention in this feasibility study. As predicted with a progressive condition, there were small overall declines on most outcomes, and these reached statistical significance for decibel levels on the loud sentence task and anxiety ratings on the DASS. Tables 2 and 3 show the preliminary efficacy testing results for speech and voice outcomes and wellbeing outcomes respectively. Overall, 33% of participants increased their speech loudness on the monolog task, and 67% declined.
Speech and Voice Results.
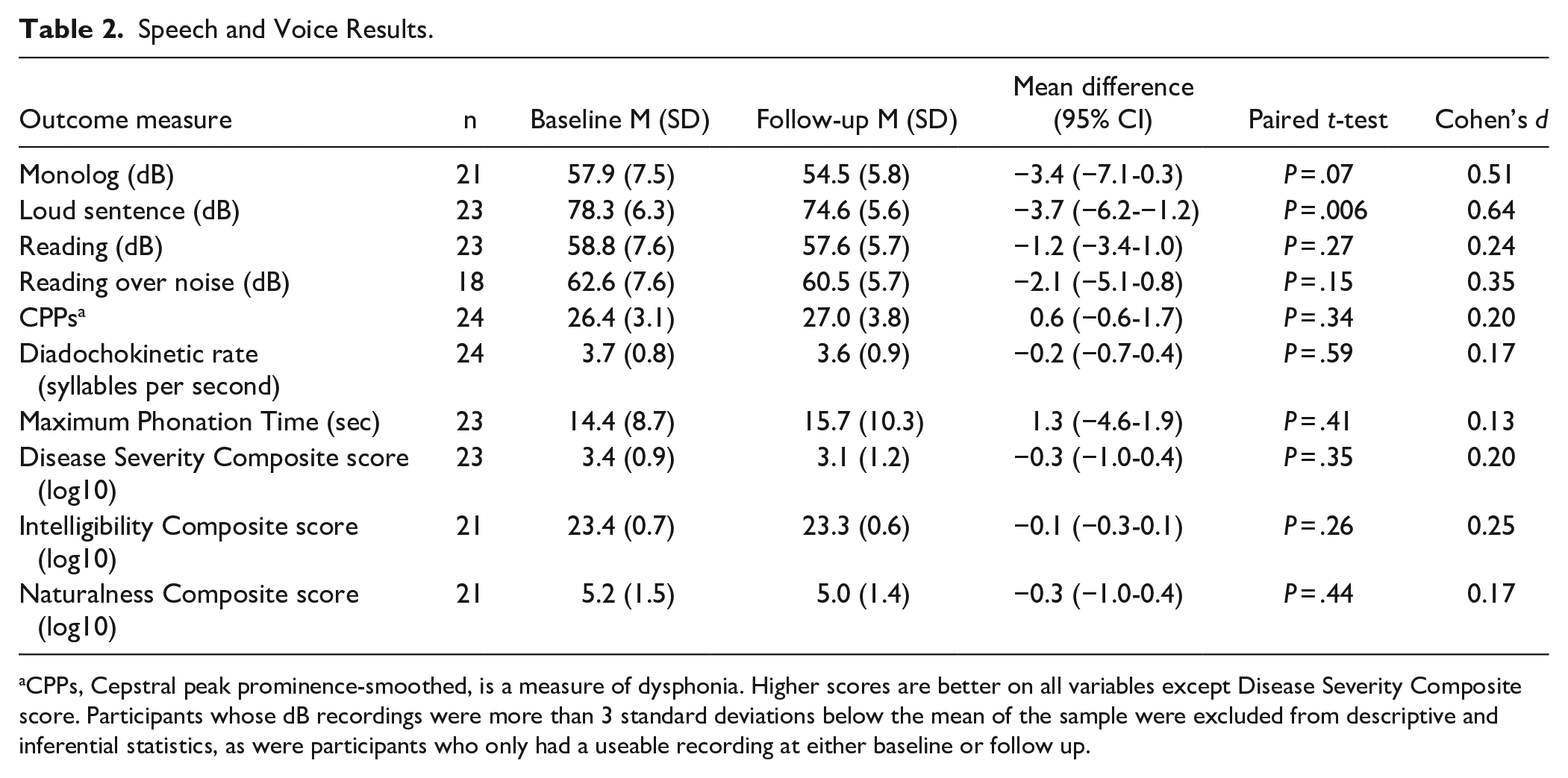
CPPs, Cepstral peak prominence-smoothed, is a measure of dysphonia. Higher scores are better on all variables except Disease Severity Composite score. Participants whose dB recordings were more than 3 standard deviations below the mean of the sample were excluded from descriptive and inferential statistics, as were participants who only had a useable recording at either baseline or follow up.
Wellbeing Results.
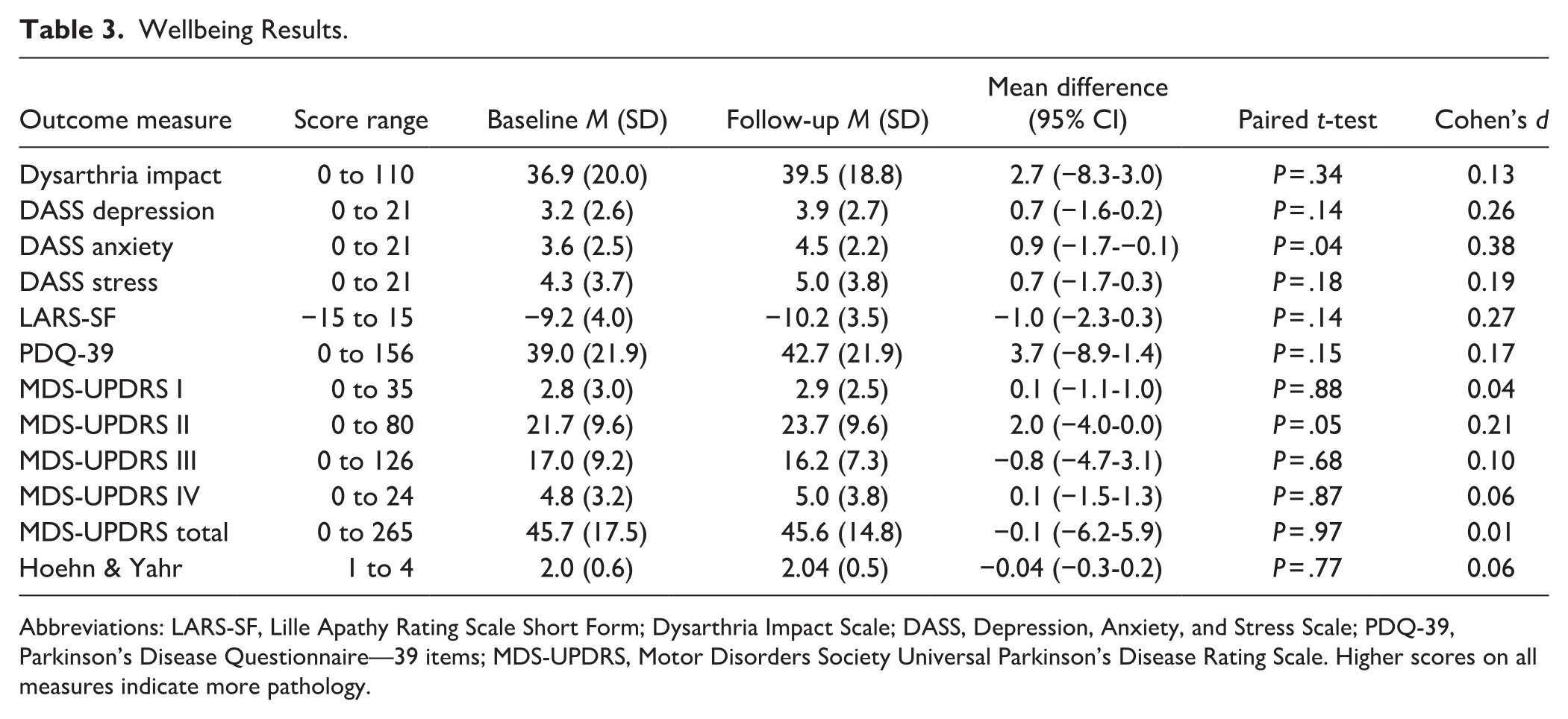
Abbreviations: LARS-SF, Lille Apathy Rating Scale Short Form; Dysarthria Impact Scale; DASS, Depression, Anxiety, and Stress Scale; PDQ-39, Parkinson’s Disease Questionnaire—39 items; MDS-UPDRS, Motor Disorders Society Universal Parkinson’s Disease Rating Scale. Higher scores on all measures indicate more pathology.
Affect Grid mood and energy scores (ranging from 1 to 9) were recorded by each participant before and after each ParkinSong Online session. Average scores were calculated for each participant and aggregated to compare difference between pre and post energy and mood levels for the overall cohort. No significant changes in aggregated scores were observed pre to post session for either mood or energy levels. Practice between sessions ranged from 0 to 6 practice sessions per week, with average overall practice for individual participants ranging from 1 to 4 times a week. Some participants used the session recordings, while other preferred to sing with YouTube clips or radio.
Overall experience reported at the end of each ParkinSong Online session was very positive with an average score of 3.3 (0.4) from a possible range of 0 (“Unsatisfactory”) to 4 (“Great”). The pace of the sessions had a possible range of 0 (“Very slow”) to 4 (“Very fast”), with 2 being “Just right.” On average participants perceived initial sessions as “a bit slow” (rating of 1), after which most sessions were rated close to or exactly “Just right.” No participants found the sessions “Too fast.” Feedback was similar from the 2 groups, suggesting consistency across the different facilitators.
To assess feasibility from the facilitator perspective we used the AAFIM. 53 Individual facilitator ratings (n = 4) were averaged for the subdomains of acceptability, appropriateness and feasibility. From a score range of 4 to 20, the mean scores of 17.0 (2.0) for acceptability, 16.8 (2.2) for appropriateness, and 17.8 (2.1) for feasibility corresponded to a high degree of facilitator endorsement for the ParkinSong Online intervention. Despite this, facilitators also identified challenges within sessions as they were required to manage multiple tasks simultaneously and were unable to hear individual voices to give targeted feedback. Tasks included muting participants who had difficulty with the technology, changing online slides with lyrics or exercise instructions, pinning the main facilitator for view layout, and monitoring participant engagement while modeling and leading exercises or songs.
Qualitative Results
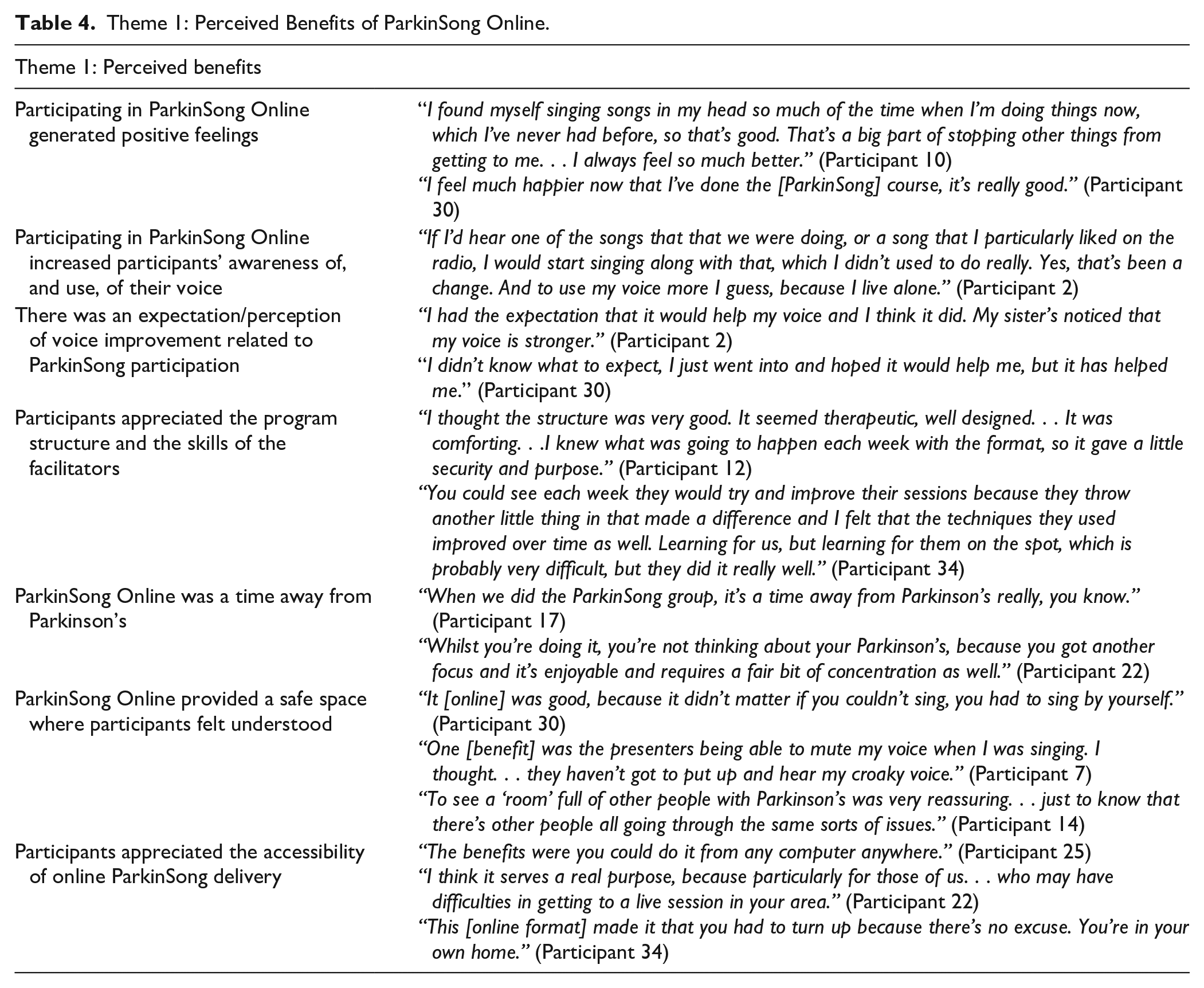
The thematic analysis of qualitative data identified 2 overall themes directly related to participants’ experience of the ParkinSong Online intervention in terms of: (1) perceived benefits (Table 4), and (2) perceived challenges (Table 5). There were 7 subthemes under the overall theme of perceived benefits. Many reported that their participation in ParkinSong Online generated positive feelings (subtheme 1.1), and increased their awareness of, and use of their voice (subtheme 1.2). There was an expectation and perception of voice improvement related to ParkinSong participation (subtheme 1.3) and participants appreciated the program structure and the skills of the facilitators (subtheme 1.4). They experienced ParkinSong Online as “a time away from Parkinson’s” (subtheme 1.5), suggesting joyful moments of respite from the challenges of Parkinson’s and valuing it as a safe space where they felt understood (subtheme 1.6). They also appreciated the accessibility of the online delivery (subtheme 1.7), particularly those for whom a face-to-face ParkinSong program was not available in their area.
Theme 1: Perceived Benefits of ParkinSong Online.
Theme 2: Perceived Challenges of ParkinSong Online.
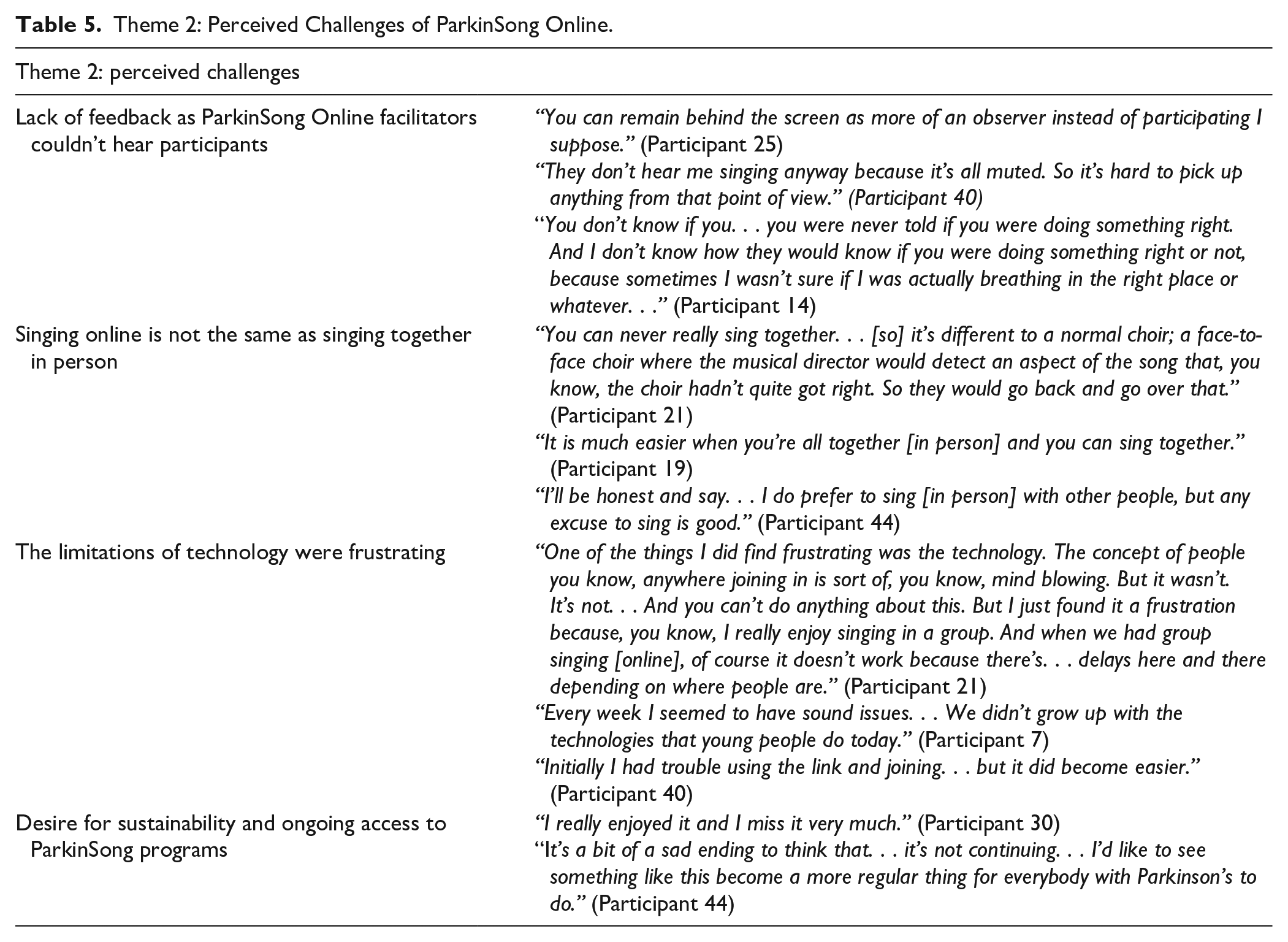
The main challenges cited by participants related to inherent limitations of the online platform (such as needing to mute during synchronous exercises or singing), learning to use, and needing assistance with the technology. Participants understood that the muting requirement during group singing meant that ParkinSong Online facilitators could not hear them and were thus unable to provide feedback (subtheme 2.1). The need for participants to stay muted during group singing differentiated the experience from in-person singing (subtheme 2.2) and caused frustrations with the technology (subtheme 2.3). However, participants all enjoyed the ParkinSong Online program, were disappointed when it ended, and talked about their desire for ongoing access and sustainable therapeutic singing programs (subtheme 2.4).
Discussion
Based on participant data and facilitator responses to feasibility measures, the ParkinSong Online intervention was feasible to administer despite some technological challenges for some participants. Recruitment rate was high, with no dropouts or adverse events reported during the intervention period. The online data collection protocol also worked well, although there was some missing or unusable speech data, so the remote collection of recorded speech data with this population may need further exploration. Acceptability of the intervention was good, with strong attendance, high facilitator ratings for intervention acceptability, and many positive comments in the qualitative data. However, despite these indications of acceptability, both participants and facilitators reported frustrations with the lack of capacity for participants to sing together off mute due to latency issues. The ramifications were that participants did not experience the Lombard effect (where they would have to project their voice over the group sound), nor were they able to benefit from facilitator feedback as no one could hear them. Thus, it is perhaps understandable that we found no improvements in speech outcomes, in contrast to our previous in person ParkinSong study findings. 9 It is likely that the restrictions to group singing caused by online latency had 2 limiting factors: (1) facilitators could not hear participants’ voices or see their full upper body, and thus could not provide appropriate guidance and feedback, and (2) the intervention did not stimulate high enough vocal effort to reach the threshold for a therapeutic effect on speech loudness. As participants were aware that no one could hear them, it is also possible that they felt less motivated or accountable to deliver maximum vocal effort.
It should be noted that the study design was primarily to evaluate feasibility and as such was not powered for efficacy testing. Further, in a degenerative condition, a pre-post study with no control group is not an ideal design for evaluating treatment efficacy. With that caveat in mind, the wellbeing measures also did not change from baseline to follow-up, apart from anxiety, although a mean increase from 3.6 to 4.5 on this 21-point scale is not clinically important. 57 Furthermore, it should be noted that most wellbeing measure scores were already low at baseline, indicating a group of individuals who were already coping well. Although apathy, depression, and anxiety are commonly reported non-motor symptoms of Parkinson’s, it is possible that people experiencing difficulty with such symptoms are less likely to volunteer for an interventional research study. Consequently, our recruited participants may represent a skewed sample with higher levels of baseline wellbeing and motivation. This may also explain the aggregated minimal change in affect from pre to post session, as most participants were already feeling positive prior to the session. However, despite the lack of change on quantitative measures, participants reported positive impacts on mood in the qualitative results.
Our feasibility results are consistent with other recent studies23,25 indicating that therapeutic singing interventions can be delivered remotely to increase accessibility for people with Parkinson’s. The differences in intervention effect can possibly be explained by the various delivery methods. The Mohseni study 25 used an individual intervention and was thus not limited by latency. Facilitators could hear participants and provide targeted feedback, however, a critique for this approach is that individual therapy is less cost effective than group therapy. The Stegemöller study 23 used a hybrid model, where groups met together to sing in remote locations following facilitator instructions from previously recorded group sessions. In this study, participants had a standard in-person group singing experience where the Lombard effect was likely activated.
Online therapy programs offer greater access to services for people in rural and regional areas where there is a higher incidence and prevalence of Parkinson’s and limited healthcare facilities. 58 While facilitator costs to deliver the intervention would likely be similar for online and in-person sessions (apart from the need to provide technical support for online sessions), the expense and burden for participants is lower without travel requirements. Our study shows that accessibility and cost savings may be increased even further through the remote administration of diverse baseline and follow up measures. This is broadly consistent with recent findings of the feasibility of telemedicine assessment for individuals with Parkinson’s,19,20,59 including for motor symptoms. 21 One caveat is that carers may sometimes be required to help assist individuals with Parkinson’s use the technology. Although the MoCA score was used as a measure to determine who would require additional support for the ParkinSong Online sessions, this turned out to be a very approximate indicator, and further refinement of the screening process for people with Parkinson’s would be required to ensure availability of adequate technology support resources during online sessions.
The qualitative results revealed some unexpected findings on the unique virtues of the online delivery method, in particular the ease of access to attend from home and from remote locations (subtheme 1.7). However, as well as the affordances of accessibility, there were also frustrations with technology. In addition to connection and sound issues (subtheme 2.3) participants reported missing the experience of a group sound and hearing each other sing, as reported in other studies of online singing.60,61 Singing off mute was explored and the cacophony caused by latency effects was tolerated for periods by participants to experience the sense of singing together. On these occasions song choice was important (eg, slower songs with fewer participants worked better). Interestingly the need to stay muted when singing was perceived both positively and negatively by participants. It created a sense of safety (subtheme 1.6) as no one could judge their singing, but also was seen as a limitation because they couldn’t receive feedback from the therapists (subtheme 2.1).
As part of the facilitator guidelines within the ParkinSong Online protocol, there was opportunity for experimentation and modification of sessions considering participant feedback during and after each session. This responsiveness to participant feedback created a sense of ownership and co-development among participants within the group and contributed to subtheme 1.4 about participants’ positive experience of the session facilitation. Revisions to the protocol would be required to determine whether therapeutic benefits to voice outcomes are achievable. These revisions should include consideration of intervention dosage and intensity (to create conditions where participants are adequately vocally stimulated to reach thresholds required for therapeutic benefit), as well as creating opportunities for individual feedback on vocal output from therapists to combat vocal deterioration caused by Parkinson’s.
Despite only meeting virtually online, participants appeared to reap significant social benefits. They felt safe and understood in a group of other people with Parkinson’s (subtheme 1.6) and found it provided respite from Parkinson’s (subtheme 1.5). The opportunity for social interaction and communication were seen as positive aspects of online delivery and were not perceived as challenges. Although these are obviously different online when compared with face-to-face interaction, they were still perceived as positive opportunities. Many participants reported they would miss the group and wished to continue to meet after the trial finished (subtheme 2.4).
Limitations
Most participants (86%) reported that they liked to sing (in private, public, or both) and this may have led to a skewed sample of active singers. The main challenge to implementing ParkinSong Online was the need for technology support. For many participants this was only required initially, however, for some, ongoing support was needed. Ongoing technology support would be important to factor into future group-based telehealth singing interventions with this population in order for the sessions not to be disrupted. Therapists also need support for implementing online therapy as capability and experience with online platforms can be limited for therapists, 62 as well as the need to manage low digital literacy of some participants.
Conclusions
ParkinSong Online is a feasible and acceptable group singing intervention for people with Parkinson’s. It affords valuable social support and connection if participants are adequately screened for technology support where required. Further, online delivery offers potential for increasing cost effectiveness as well as accessibility. The social benefits of group participation can be considerable, given service access issues and social isolation experienced by many. Therefore, although further research is needed to determine therapeutic efficacy, online singing groups for Parkinson’s may be a welcome addition, supplement, or in some cases a necessary alternative to in-person singing groups.
Footnotes
Acknowledgements
We would like to acknowledge Fight Parkinson’s for their financial and in-kind support for the implementation of this research. We also thank the people living with Parkinson’s who participated in this trial and their partners/carers who supported them with the technology. Special thanks also to Helen Crouch, Bonnie Nilsson, Laura Murray, and Hannah Carter for their contribution as ParkinSong Online facilitators.
Correction (November 2024):
Table 1 and Table 3 have been amended with the correct Hoehn & Yahr data. These data table changes did not affect any of the results or conclusions.
Author Contributions
A/Prof. Tamplin was responsible for the conceptualization, design, and supervision of the study. She conducted some of the focus group interviews, led the analysis of qualitative data, contributed to the statistical analysis and interpretation of quantitative data, and drafting and revision of the manuscript.
Dr. Haines was the ParkinSong Online project manager. He scheduled and conducted assessments, provided technical support during the ParkinSong Online sessions, and conducted focus group interviews. He also led the statistical analysis and contributed to the qualitative analysis and drafting and revision of the manuscript. Prof. Baker contributed to design and conceptualization of the study, interpretation of data and manuscript preparation. Dr. Sousa contributed to design and conceptualization of the study, data collection, assessment of costs, interpretation of data, and manuscript preparation. Dr. Thompson contributed to data collection, interpretation of data, and manuscript preparation. Ms. Crouch contributed to data collection, interpretation of data, and manuscript preparation. Mr. Dunn contributed to design and conceptualization of the study, data collection, interpretation of data, and manuscript preparation. Mrs. Tull contributed to design and conceptualization of the study, data collection, interpretation of data, and manuscript preparation. Prof. Vogel contributed to design and conceptualization of the study, analysis and interpretation of data, and manuscript preparation. Prof. Morris contributed to design and conceptualization of the study, interpretation of data, and manuscript preparation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: A/Prof. Tamplin, Prof Baker, Dr Sousa, and Dr Thompson receive research funding from the Medical Research Future Fund, Australia (GNT20007411) and salaried support from The University of Melbourne. Dr. Haines, Ms Crouch, Ms Tull, and Mr Dunn report no disclosures. Prof. Vogel is an employee of Redenlab Inc. and receives salaried support from the Australian Research Council, Australia (220100253) and institutional support from The University of Melbourne. Prof. Morris receives research funding from the National Health and Medical Research Council, Australia (GNT11523) and has a joint appointment with Healthscope and La Trobe University.
Ethical Approval
Ethical approval was obtained from The University of Melbourne Human Research Ethics Sub-Committee (Approval no.: 2021-14465-16053-3, approval date: July 28, 2021).
Trial registration number
ACTRN12621000940875 (registered July 19, 2021).