
Abstract
Background. Communication impairment is one of the most common symptoms of Parkinson’s disease (PD), significantly affecting quality of life. Singing shares many of the neural networks and structural mechanisms used during speech and, thus, has potential for therapeutic application to address speech disorders. Objective. To explore the effects of an interdisciplinary singing-based therapeutic intervention (ParkinSong) on voice and communication in people with PD. Methods. A controlled trial compared the effects of the ParkinSong intervention with an active control condition at 2 dosage levels (weekly vs monthly) over 3 months, on voice, speech, respiratory strength, and voice-related quality-of-life outcomes for 75 people living with PD. The interdisciplinary ParkinSong model comprised high-effort vocal and respiratory tasks, speech exercises, group singing, and social communication opportunities. Results. ParkinSong intervention participants demonstrated significant improvements in vocal intensity (P = .018), maximum expiratory pressure (P = .032), and voice-related quality of life (P = .043) in comparison to controls. Weekly ParkinSong participants increased vocal intensity more than monthly participants (P = .011). Vocal intensity declined in nontreatment control groups. No statistical differences between groups on maximum phonation length or maximum inspiratory pressure were observed at 3 months. Conclusions. ParkinSong is an engaging intervention with the potential to increase loudness and respiratory function in people with mild to moderately severe PD.
Keywords
Introduction
Speech and communication disorders are common and debilitating in people with idiopathic Parkinson’s disease (PD). 1 Although up to 90% of people living with PD experience voice and speech impairments, few seek help. 2 Dysarthria is common in PD 3 and is characterized by reduced loudness, limited respiratory support for speech, harsh or breathy voice quality, a monotone voice, dysprosody, or imprecise articulation. 4 Medications traditionally used to treat PD can initially have a positive response for some disease symptoms, yet often have limited impact on speech symptoms. 5 Deep-brain stimulation (DBS) yields equivocal results, with speech often deteriorating following stimulation. 6
Speech production in people with PD can improve with face-to-face speech therapy programs.7,8 This can be time intensive, requires specialized training, and can be costly to deliver and uses drill-like repetitive exercises. The development of therapies that are easily accessible, enjoyable, and engaging as well as therapeutically beneficial may facilitate compliance, adherence, and longer-term maintenance of voice and speech.
Nonmotor symptoms are prevalent in PD and can have a negative effect on participation and health-related quality of life. 9 There can also be cognitive-linguistic impairments, poor self-perception of speech, and neuropsychiatric symptoms, such as depression and anxiety. 10 In combination, these can lead to failed communication attempts and self-consciousness around communication as well as avoidance of social interactions that require speaking. 11
Singing is a promising therapeutic modality for improving speech in people living with neurodegenerative diseases. 12 It generates widespread neural activation and uses many of the structures and mechanisms used for speech (such as the inferior precentral and postcentral gyrus, superior temporal gyrus, and superior temporal sulcus bilaterally).13,14 Singing demands increased respiratory support, louder and more sustained phonation, and greater pitch variation and articulation than talking, 15 thus theoretically targeting many elements of impaired speech in PD. Singing can also activate the reward, arousal, and emotion networks in the brain through stimulating the release of dopamine, oxytocin, serotonin, and endorphins and reducing cortisol levels. 16 Singing in a group context enables social connection, increases in conversation, and shared emotional states, which facilitate empathy, cohesion, and bonding. 17
The therapeutic benefit of singing for people with PD has not been verified. A recent systematic review reported limited and inconsistent evidence on the effects of singing on communication and well-being for people with PD. 18 Of the 9 studies identified, all had single-group, repeated-measures designs; a high risk of selection bias; and small sample sizes (4-28 participants). Conflicting results were obtained, with some studies suggesting improvements in voice outcomes, such as vocal intensity, intelligibility, and maximum phonation time19-25 and others reporting no change.26,27 Building on existing research from both music therapy and speech pathology fields, we examined the effects of an integrated, therapeutic group singing intervention (“ParkinSong”) on voice and communication in a larger, controlled clinical trial. ParkinSong utilizes the motivating aspects of singing to achieve voice and speech goals in a group context. The group context of ParkinSong encourages social engagement and bonding and helps foster motivation and compliance with therapy. The primary research question was the following: Can ParkinSong improve communication outcomes for people living with PD as compared with an active control intervention? Vocal intensity was chosen as the primary outcome because (1) reduced loudness is the most prominent speech problem in PD and (2) improvements in vocal intensity theoretically lead to increases in intelligibility and communication confidence. 28 Vocal intensity is correlated with respiratory function, 29 and singing demands high respiratory effort.30,31 Therefore, we also measured maximum respiratory pressures to investigate potential mechanisms for the beneficial effects of singing on vocal intensity. Related speech outcomes that were measured were intelligibility and maximum phonation length because these are affected by vocal intensity and respiratory support, and voice-related quality of life. To examine dosage, we compared participants with PD who attended weekly and monthly ParkinSong groups with participants with PD who attended weekly and monthly active control groups.
Methods
A controlled clinical trial design was used to investigate the effect of the ParkinSong interdisciplinary singing and speech protocol (provided at weekly and monthly intervals) on speech, voice, respiratory function, and voice-related quality-of-life outcomes in PD. This article presents the primary 3-month time point results within a 12-month study. We compared the ParkinSong groups with active control conditions (also weekly and monthly) rather than standard care to control for potential effects of group participation and social interaction on communication. The active control groups included PD support programs that did not involve singing (eg, peer support, painting, dancing, or tai chi). The study was approved by Human Research Ethics Committees at The University of Melbourne (1544384) and Monash Health (15355A), and written informed consent was obtained from all participants. The study was also registered with the Australian New Zealand Clinical Trials Registry (ACTRN12617000528358).
Participants
Participants were recruited through Parkinson’s Victoria (Australia) peer support group networks and website. All participants had been diagnosed with PD by a neurologist using the Movement Disorder Society (MDS) criteria 32 and were English speaking with no cognitive impairment (Mini Mental State Exam [MMSE] > 24), or mild cognitive impairment (MMSE = 18-23), 33 with mandatory carer support. Exclusion criteria were moderate to severe cognitive impairment (MMSE < 18) or memory problems and severe language problems or hearing impairment. We did not exclude participants with atypical PD or DBS for this pragmatic trial. Participants were not randomly assigned to conditions for this study but were able to select the ParkinSong group intervention or another peer support group (control condition) and provided informed consent to participate. We recorded medication use and additional therapy intervention.
Assessment Procedures
Demographic data collection and assessments of disease severity and cognitive function were conducted at baseline. Assessments of speech, voice, respiratory function, and voice-related quality of life were conducted at baseline and 3 months by trained assessors (speech pathologist, music therapist, and speech pathology master’s students). We were not able to blind all assessors to group allocation, but all raters of speech outcomes were blinded to condition/group.
The speech and voice assessment protocol included 3 maximum phonations of a sustained vowel /a:/, a loud sentence, a monologue about leisure interests, and the Speech Intelligibility Test (SIT), 34 which includes randomly generated lists of sentences increasing in length from 5 to 15 words. Participants were instructed to complete all vocal tasks at a comfortable pitch and loudness, except for the loud sentence, where they were instructed to intentionally say this as loudly as possible. Where possible, baseline and 3-month assessments were conducted at the same time of day post–medication dosage with participants in an “on” state. Speech was recorded using a Shure SM35-XL headset microphone with RPM626 XLR preamp (with a mouth-to-microphone distance of 5 cm), via Roland UA-55 Quad-Capture. All recordings were deidentified prior to analyses.
Measurements
Disease severity was assessed using the International Parkinson and MDS’s Unified Parkinson’s Disease Rating Scale (MDS-UPDRS) 35 and cognitive function using the MMSE. 36 The primary outcome measured was vocal intensity. Secondary outcomes were speech intelligibility, maximum phonation length, maximum respiratory pressures, and voice-related quality of life. Acoustic analyses were conducted using PRAAT 37 software to measure intensity (from the loud sentence task and monologue with silent periods excluded) and maximum phonation time (best of 3 attempts on the sustained vowel task). Vocal intensity was measured via sound pressure level (SPL) in decibels. The SPL measured by PRAAT was calibrated with a sound level meter. Intelligibility was measured using the SIT and blinded perceptual ratings. The SIT sentences were transcribed by expert raters blinded to group and time point to generate a percentage intelligibility score. Interrater reliability was calculated using intraclass correlation coefficients. Perceptual consensus ratings of intelligibility were conducted on the monologue by 2 expert listeners blinded to group and time point. Respiratory muscle strength was assessed by measuring maximal inspiratory pressure (MIP), maximal expiratory pressure (MEP), and sniff nasal inspiratory pressures (SNIPs) 38 using a portable MicroRPM respiratory pressure meter, in accordance with American Thoracic Society/European Respiratory Society guidelines. 39 Each maximal respiratory pressure measurement was repeated at least 3 times until the best 2 values matched to within 10%. Voice-related quality of life was measured using the Voice Activity and Participation Profile (VAPP), a 28-item self-assessment tool that evaluates the perception of voice problem, activity limitation, and participation restriction using the World Health Organization International Classification of Impairments, Disabilities, and Handicaps concept. 40
Intervention
The ParkinSong protocol began with 30 minutes of high-intensity music-based vocal exercises incorporating respiratory control, vocal loudness, and pitch control activities as well as some vocal exercises targeting speech loudness, self-monitoring, and speech clarification strategy practice. This was followed by 60 minutes of singing popular and traditional songs and rounds with a focus on loud voice projection and increased respiratory support. Each session concluded with 30 minutes of social interaction and conversation practice over morning or afternoon tea, where participants were encouraged to use the strategies for generating loud voice that had been practiced during the session. Weekly ParkinSong sessions were delivered by a registered music therapist, speech pathologist, and allied health assistant. Monthly ParkinSong sessions were delivered by community musicians and volunteers with support and training from therapists. The ParkinSong protocol was the same for both monthly and weekly groups. The same training was provided to all facilitators, and regular observation of sessions from all groups was conducted by members the research team to ensure treatment fidelity. Weekly control participants attended weekly painting, dancing, or tai chi sessions, and monthly control participants attended monthly peer support groups. All control groups also included the opportunity for social interaction over morning or afternoon tea.
Analysis
Continuous outcomes were summarized as mean (SD) and analyzed via SPSS 41 software using 1-way analysis of covariance, with baseline scores used as a covariate and an α level of .05. Group allocation was considered as a single factor with 4 levels, corresponding to the different combinations of activity and frequency. Pairwise comparisons were obtained from this analysis to estimate the mean differences between the groups. Differences between groups in baseline demographics were tested using 1-way analysis of variance for continuous measures and the Fisher exact test for categorical variables
Results
Demographic and Attendance Data
Recruitment commenced in December 2015 and ceased in November 2016 when a total of 75 participants (61% male) were recruited (Figure 1), with an average age of 74 years (range 51-93 years). There were 8 participants with atypical PD (Lewy body dementia, n = 5; progressive supranuclear palsy, n = 2; multiple system atrophy, n = 1) spread across all conditions. Although participants were not randomly allocated to treatments for this study, disease severity, cognitive function, and speech severity did not differ statistically between groups (see Table 1). All except 4 participants were taking PD medication over the course of this study and were responsive to medication. Eight participants (spread across all conditions) had received DBS prior to enrolment. Medication changes were reported for 44% of participants at 3 months, but these participants were spread between groups (weekly ParkinSong, 55%; monthly ParkinSong, 44%; weekly control, 36%; monthly control, 38%).
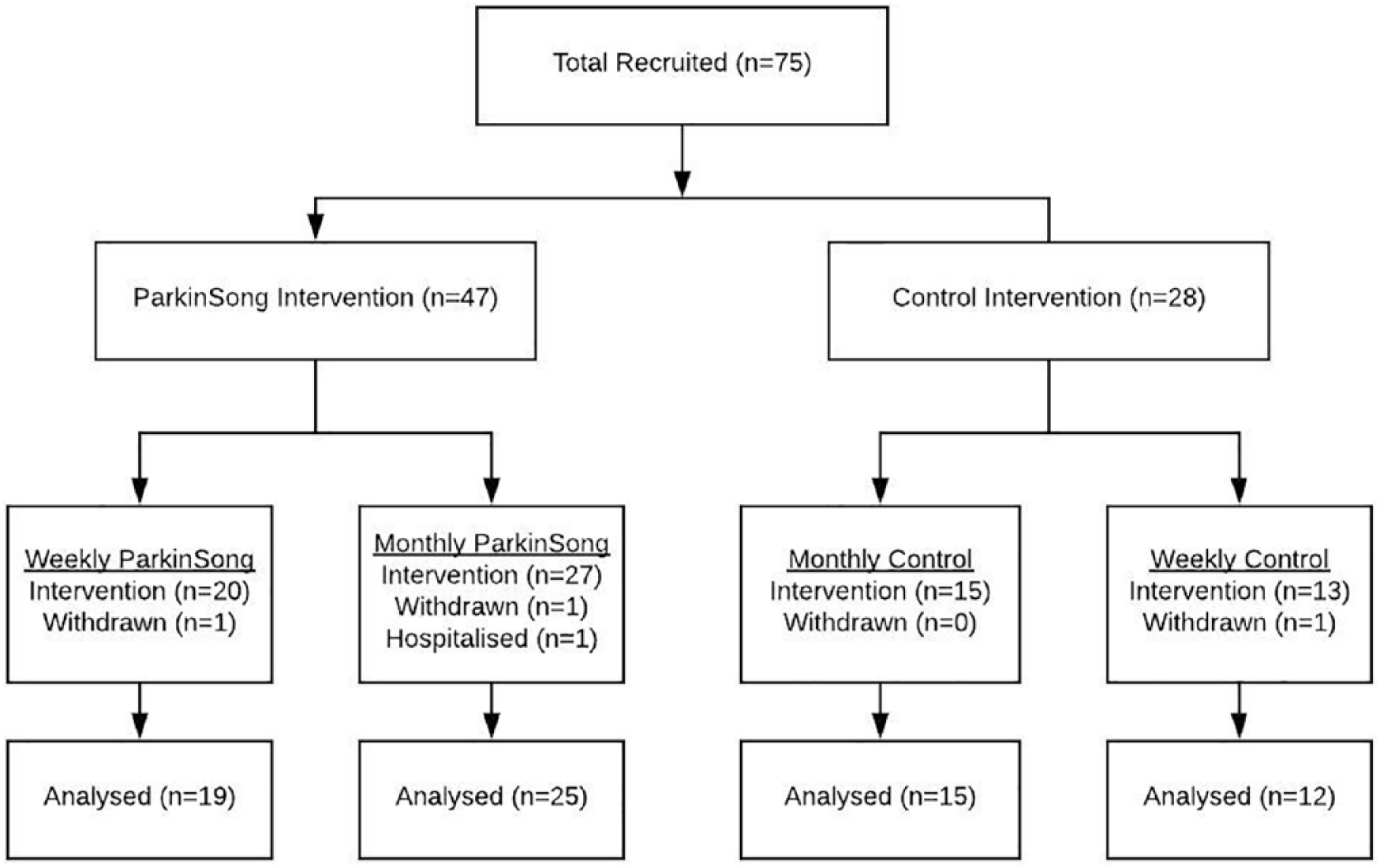
Consort flowchart.
Baseline Demographics of Participants.
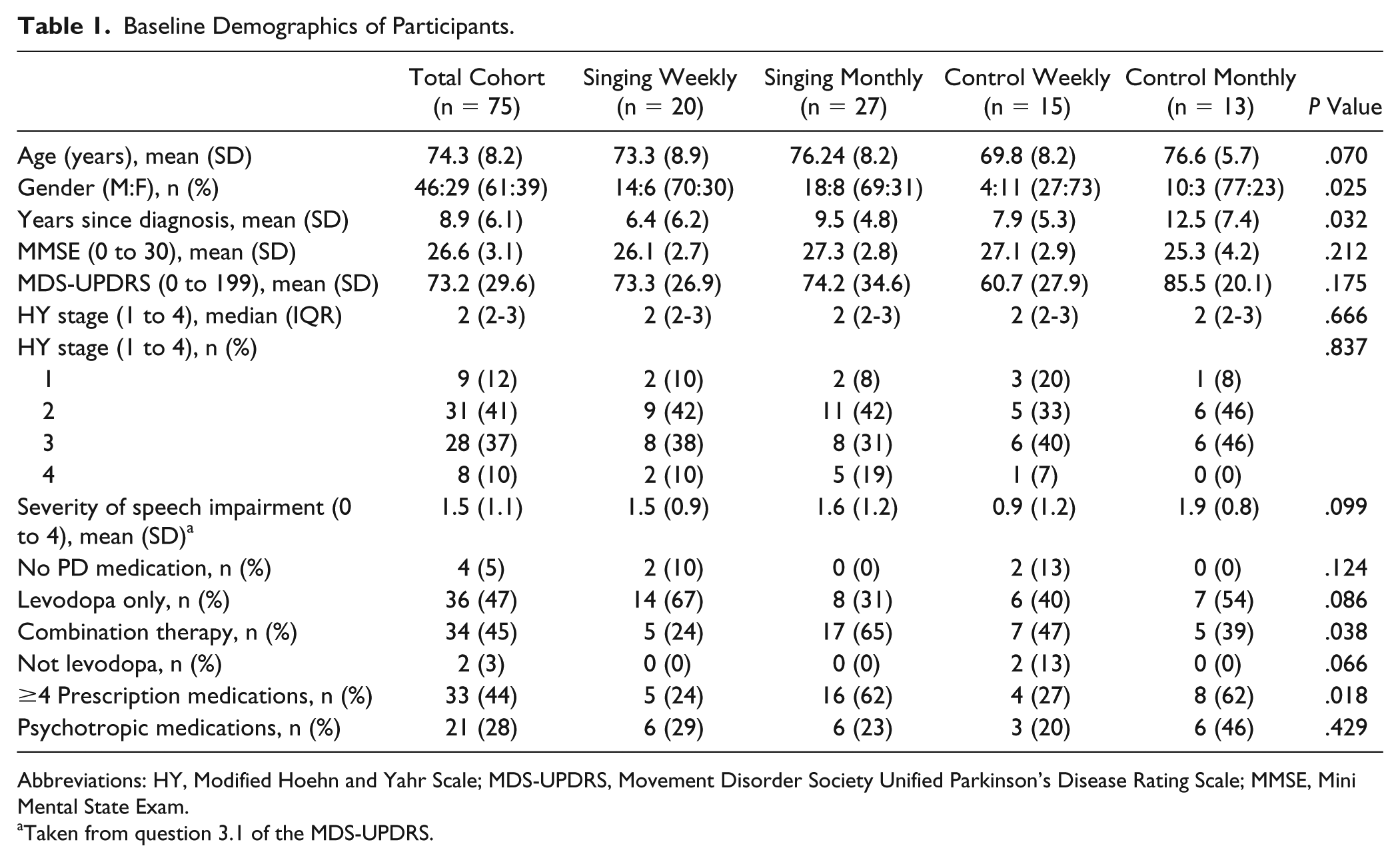
Abbreviations: HY, Modified Hoehn and Yahr Scale; MDS-UPDRS, Movement Disorder Society Unified Parkinson’s Disease Rating Scale; MMSE, Mini Mental State Exam.
Taken from question 3.1 of the MDS-UPDRS.
Participants had a mean baseline UPDRS score of 73.1 (SD = 29.7; range = 10-161) and Hoehn and Yahr median score of 2 (IQR = 2-3). There were no statistically significant differences between the 4 groups on the UPDRS at baseline (P = .175; Table 1). On average, all groups attended at least 80% of sessions over 3 months. A subset of 20 participants attended additional therapy during the study period. In all, 16 attended physical therapy and 6 attended speech therapy (3 monthly controls, 2 monthly singers, 1 weekly singer). None participated in Lee Silverman Voice Therapy (LSVT-Loud) treatment during the study. There were 7 instances (across 3 conditions) where participants were “on” (in terms of their optimal medication state) at baseline and “off” at 3 months (2 weekly singers, 4 weekly controls, 1 monthly singer). The trial ended after the 12-month final assessment. All 75 participants were assessed at baseline; there were small numbers of missing values at the 3-month time point.
Primary Outcome: Vocal Intensity
We found statistically significant between-group differences (P = .018) for mean SPL on the monologue task (see Table 2 for all summary statistics and P values). The weekly singers had higher mean scores than each of the other groups, by 5.7 dB or more at 3 months. The weekly (and to a lesser extent monthly) singers increased vocal intensity of conversational speech over 3 months, whereas the vocal intensity decreased for the control participants (Figure 2).
Baseline and 3-Month Mean Scores for All Measures.
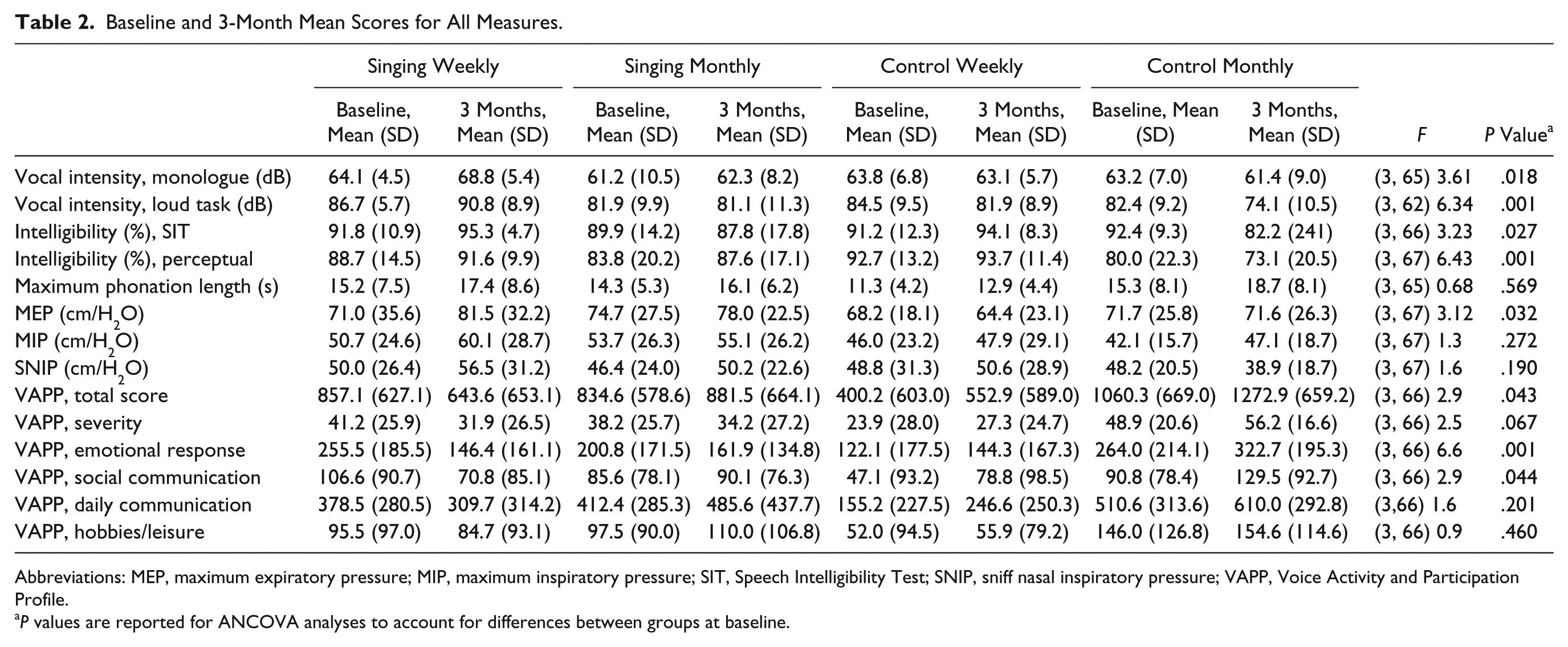
Abbreviations: MEP, maximum expiratory pressure; MIP, maximum inspiratory pressure; SIT, Speech Intelligibility Test; SNIP, sniff nasal inspiratory pressure; VAPP, Voice Activity and Participation Profile.
P values are reported for ANCOVA analyses to account for differences between groups at baseline.
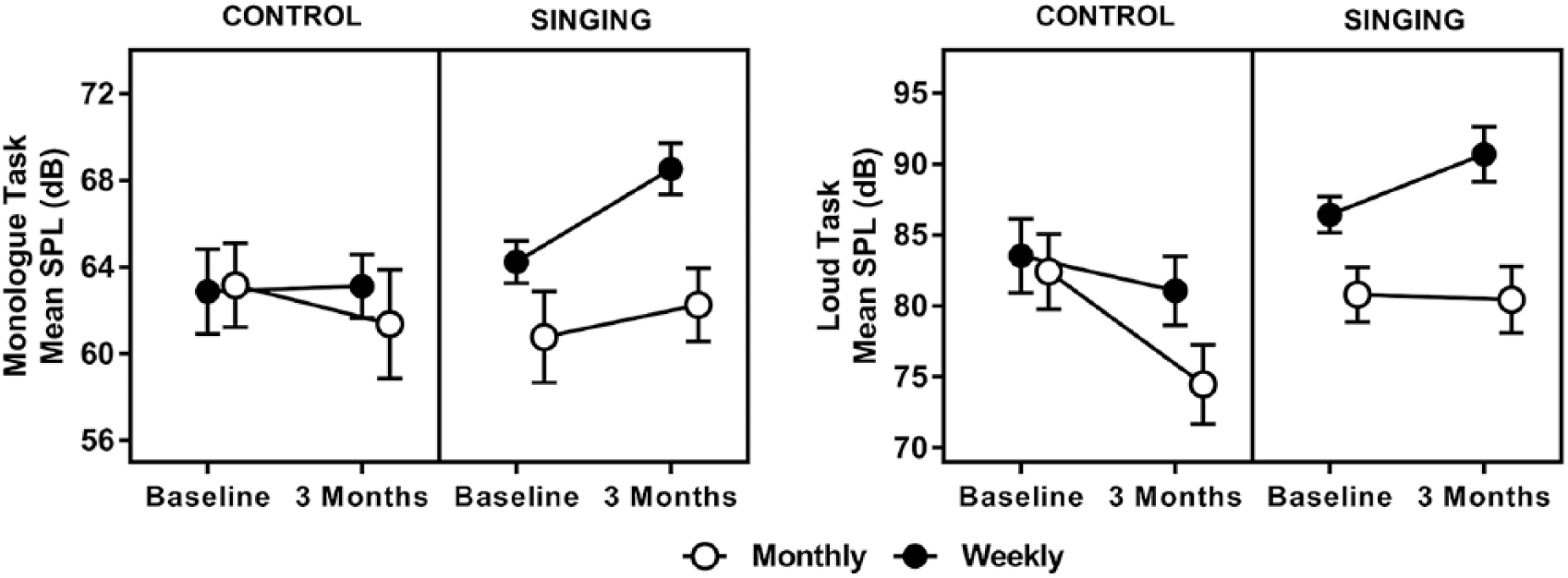
Speech intensity results raw means have been plotted with standard error reflected by error bars.
Pairwise comparisons revealed that 3-month mean SPL (adjusted for the baseline covariate) was higher for weekly singers than weekly controls (5.6 dB; 95% CI = 0.67 to 10.6, P = .027) and monthly controls (7.1 dB; 95% CI = 2.2 to 12.1, P = .006). There was also a dosage effect, where weekly singers had an adjusted mean SPL that was 5.6 dB louder than monthly singers at the 3-month time point (95% CI = 1.3 to 9.8; P = .011). There were small and statistically nonsignificant mean differences between 3-month SPL on the monologue task for monthly singers and monthly controls (mean difference = 1.5 dB; 95% CI = −3.2 to 6.3; P = .518), and between weekly controls and monthly controls (mean difference = 1.5 dB; 95% CI = −3.9 to 6.9; P = .582).
For the loud sentence task, there were group differences in mean SPL (P = .001). The weekly singers increased their mean maximum loudness, whereas the other groups decreased to varying degrees (Figure 2). Pairwise comparisons revealed that 3-month mean SPL (adjusted for baseline) was higher for weekly singers than weekly controls (8.5 dB; 95% CI = 1.3 to 15.6, P = .021) and monthly controls (15.7 dB; 95% CI = 8.3 to 23.1, P < .001). Again, there was a dosage effect, where weekly singers had an adjusted mean SPL that was 8.7 dB louder than monthly singers at 3 months (95% CI = 2.4 to 14.2; P = .008). The mean difference between monthly singers and monthly controls was 7.1 dB (95% CI = 0.3, 14.1; P = .049), and between weekly and monthly controls, it was 7.3 dB (95% CI = −0.7, 15.1; P = .072).
Secondary Outcomes
Intelligibility
Statistically significant between-group differences were found for speech intelligibility as measured by SIT scores (P = .027). The main reason for this difference between groups was a 10% decrease in intelligibility from the monthly control participants, whereas all other groups remained relatively stable. Average overall baseline intelligibility measured by the SIT was around 90% for the sample as a whole. Similarly, there was a statistically significant between-group difference on perceptual intelligibility consensus ratings (P = .001). The decrease in intelligibility for monthly controls was statistically significantly different (Figure 3) from that for weekly controls (P = .001), monthly singers (P ≤ .001), and weekly singers (P < .001).
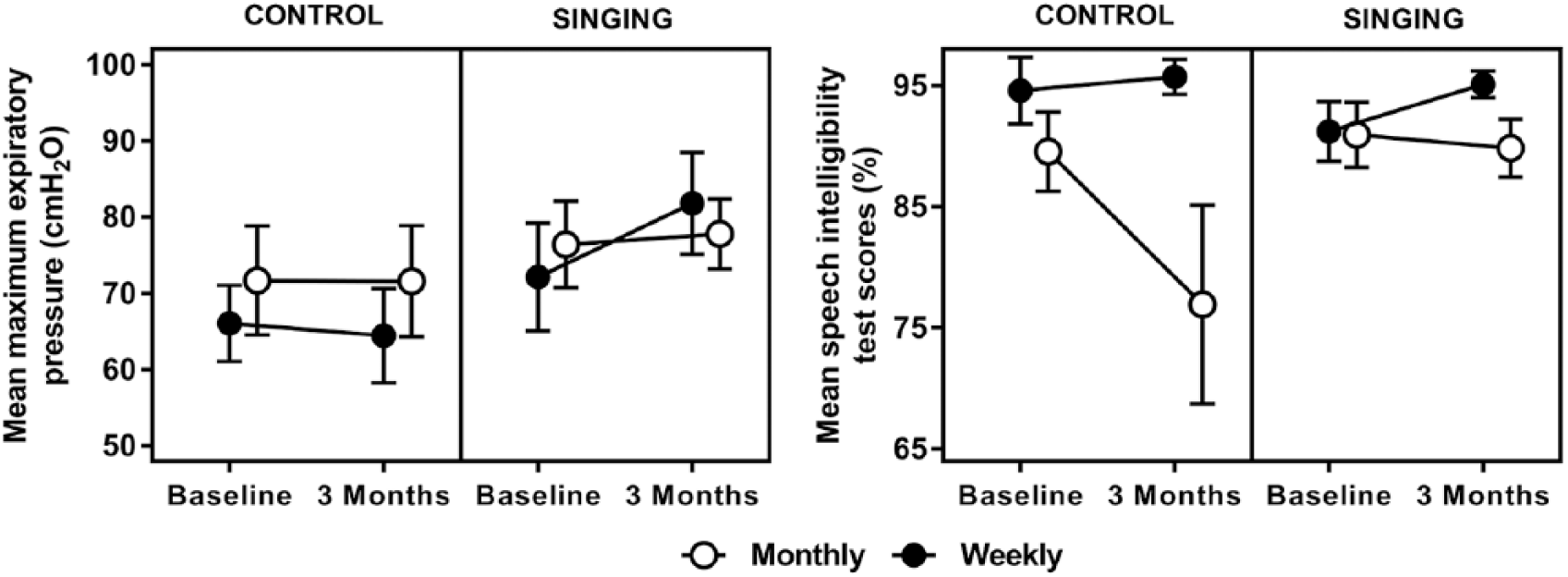
Maximum expiratory pressure and intelligibility results raw means have been plotted with standard error reflected by error bars.
Interrater reliability was deemed acceptable, with raters within 3% of each other 84% of the time and within 5% of each other 97% of the time (ICC = 0.992; P < .001).
Maximum Phonation Length
There were no statistical differences between groups on change in maximum phonation length over 3 months (P = .569), with all groups producing longer phonation time between baseline and 3-month assessments (Table 2).
Respiratory Pressures
MEP differed by group and dosage (P = .032). The weekly (and to a lesser extent monthly) singers increased MEP scores between baseline and 3-month assessments, whereas controls decreased or remained stable (Figure 3). Pairwise comparisons revealed that 3-month mean MEP (adjusted for baseline) was higher for weekly singers than weekly controls (14.9 cm/H2O; 95% CI = 4.7 to 25.0, P = .005) and also higher than monthly controls (10.4 cm/H2O; 95% CI = −0.002 to 20.8, P = .050). Monthly singers presented with higher MEP scores than weekly controls (8.5 cm/H2O; 95% CI = −1.1 to 18.1, P = .081). No statistical differences were observed between groups for MIP scores (adjusted for baseline; P = .272) or SNIP scores (P = .190).
Voice-Related Quality of Life
Voice-related quality of life (as measured by VAPP scores) differed between intervention frequency and group (P = .043; Figure 4). Pairwise comparisons revealed a mean difference between the total VAPP score for weekly singers compared with monthly controls (−478.0; 95% CI = −809.9 to −146.0, P = .005); mean scores decreased from baseline for weekly singers but increased for monthly controls.
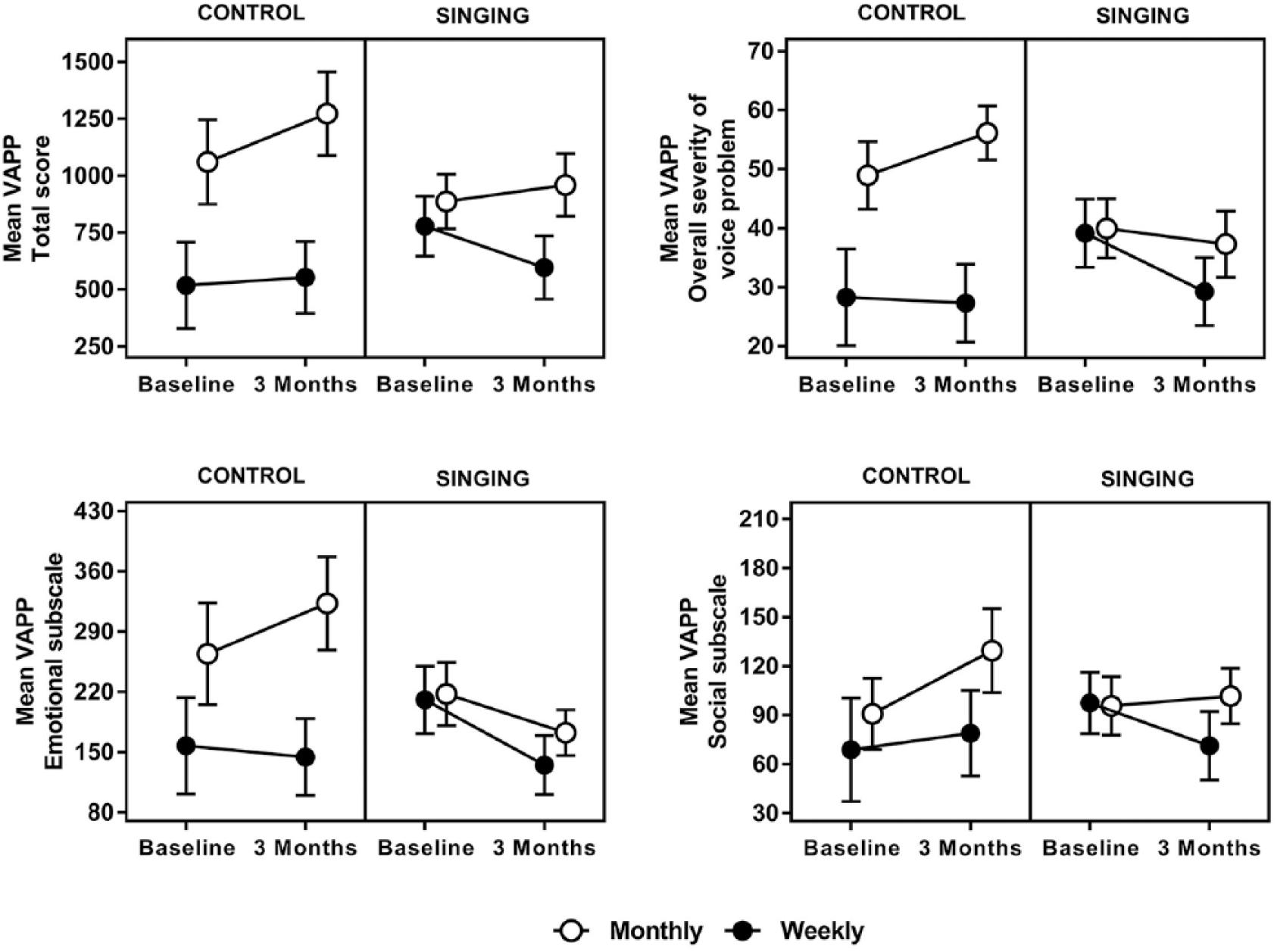
Voice Activity and Participation Profile (VAPP) results raw means have been plotted with standard error reflected by error bars.
Between-group differences for changes in perceived voice problem severity were not statistically significant (P = .067). There were differences between groups on the social communication subscale of the VAPP (P = .044), with weekly singers perceiving a mean decrease in perceived social communication problems in contrast to the mean increase experienced by monthly controls (mean difference = −68.8; 95% CI = −117.5 to −20.1; P = .006). There were also differences between groups on the emotion subscale of the VAPP (P = .001), with weekly singers perceiving a mean decrease in negative emotional responses to their voice problem in contrast to the mean increase experienced by weekly controls (mean difference = −74.8; 95% CI = −147.5 to −2.1; P = .044) and monthly controls (−157.0; 95% CI = −229.7 to −84.2; P < .001). This mean difference was also present to a lesser degree between monthly singers and monthly controls (−117.9; 95% CI = −187.5 to −48.4; P = .001). There were no statistical differences detected between groups for the daily communication or leisure interest subscales.
Discussion
Vocal intensity increased for ParkinSong participants with PD receiving weekly intervention to a greater degree than PD participants who received monthly ParkinSong sessions. This was in contrast to a decline in the vocal intensity that occurred over time for control participants with PD who attended weekly painting, dancing, or tai chi or monthly peer support groups. Greater decline in vocal intensity was observed in the monthly PD control group compared with the weekly PD control group. These results were consistent for both conversational speech (monologue) and intentionally loud speech. Improvements in conversational speech intensity (mean 4.7 dB) following 3 months of weekly ParkinSong sessions (12 sessions) were comparable to those reported in a recent trial of daily LSVT-Loud delivered face to face (mean 5.2 dB) over a 4-week period (16 sessions) for participants with PD. 8
The increase in expiratory pressure exhibited by ParkinSong participants suggests that increased expiratory strength was the mechanism used to increase vocal intensity. These results support previous research reporting improvements in respiratory pressures post–singing intervention.20,25 Significant differences between groups in intelligibility after 3 months were due to decreases in intelligibility for monthly controls. High baseline intelligibility for all groups caused a potential ceiling effect for the SIT measure. The blinded perceptual ratings also identified a decrease in intelligibility for monthly controls. A perceptual measure of intelligibility based on a monologue rather than read sentences may be a more sensitive measure of intelligibility in PD however, because it indicated lower baseline intelligibility.
Improvements in voice-related quality of life for ParkinSong participants support the pattern of improvement in acoustic measures of vocal loudness, with a perceived decrease in severity of voice problem, and less negative feelings about their voice problem. In comparison, the control participants exhibited decreases in voice-related quality of life, and monthly singers remained relatively stable.
Overall, there was a clear pattern of improvement for weekly singers with PD across multiple measures. Monthly singers with PD either improved to a lesser extent or remained stable, which is notable in a degenerative condition. We also found evidence for an intervention dosage effect, where weekly singing groups had a greater effect on improving vocal loudness than monthly singing groups, and also, nonsinging weekly group participation was better for maintaining vocal loudness than nonsinging monthly group participation.
This study is the first adequately powered controlled trial investigating the efficacy of a singing-based therapeutic intervention in PD. Our results demonstrated not only that vocal intensity increased following the ParkinSong intervention but that participants who did not sing declined in vocal loudness. Although the sample size in each group in the study was modest, we were able to detect clinically important mean differences in both speech parameters and respiratory outcomes; sample size did not prove to be a limitation for the study. The increase in vocal intensity following a targeted singing intervention supports previous smaller studies19,22 and also replicates results achieved from other intensive, nonsinging interventions.7,8 This article reports results only from 3 months of ParkinSong intervention. Because PD is a degenerative condition, we might expect to see a greater effect of ParkinSong in the longer term if control participants continued to deteriorate as expected and ParkinSong participants continue to improve or at least maintain their vocal function.
Study feasibility was high, with adequate numbers of participants recruited and a low attrition rate. Acceptance of the intervention and attendance rates were also good, with intervention participants campaigning to continue the ParkinSong groups at the end of the intervention period. They stated that it was “like being given a drug that is effective, and then having that drug taken away.” Subsequently, we worked with stakeholders to ensure that the groups were sustainable poststudy.
Limitations
In this trial, participants selected their group (ParkinSong or control), which created selection bias. People who choose a singing intervention may be more likely to improve because they enjoy singing and are motivated to participate. The weekly ParkinSong groups were facilitated by music therapists and speech pathologists, and the monthly groups were facilitated by volunteer musicians with support and training from therapists. It is possible that the degree of improvement in the weekly ParkinSong participants was a result of the higher dosage or expertise of the facilitators or a combination of both. A large-scale randomized controlled trial is needed to deal with the limitations of selection bias yielded in this study. Furthermore, given that the higher-intensity program (weekly) was more effective, future research could examine the effect of interventionist by providing weekly ParkinSong sessions to all intervention participants and comparing the effect of therapist interventionists versus volunteer musicians with support and training from therapists.
Speech intelligibility is a crucial aspect of functional communication. A significant increase in vocal loudness would be expected to improve overall speech intelligibility. Intelligibility measured from sentence reading tasks (eg, SIT) may not always reflect conversational intelligibility. In this study, SIT intelligibility was high at baseline in all groups and, thus, may reflect a ceiling effect. The baseline perceptual ratings of monologue speech intelligibility were lower and probably more reflective of true intelligibility. It may also be useful in future studies to control for the effect of intensity on intelligibility by using transcription of sentences taken from a conversational speech sample with a 0-dB sound-to-noise ratio at pretest as described by Moya-Galé. 42 We were not able to control for medication changes or additional therapy in this study; however, all medication changes and additional therapy attended were recorded, and these were comparable across groups.
Conclusions
High-dosage (weekly), therapeutically informed, intensive effort singing increased vocal intensity, MEP, and voice-related quality of life. Singing groups offer an engaging way to enhance voice and communication for people living with PD as well as providing opportunities for socialization.
Footnotes
Acknowledgements
We would like to acknowledge Parkinson’s Victoria, Monash Health, and the Hugh Williamson Foundation for their roles in supporting this research. We also thank the people living with Parkinson’s disease who participated in this trial. Special thanks also to Gustavo Noffs for his assistance with data collection.
Authors’ Note
Australian New Zealand Clinical Trials Registry number: ACTRN12617000528358. JT was responsible for the design and conceptualization of the study, statistical analysis and interpretation of the study data, study supervision, and drafting and revising the manuscript. MEM contributed to design and conceptualization of the study, interpretation of data, and manuscript preparation and revision. CM contributed to design and conceptualization of the study, data collection, interpretation of data, and manuscript preparation. FAB contributed to design and conceptualization of the study, interpretation of data, and manuscript preparation. APV contributed to design and conceptualization of the study, analysis and interpretation of data, and manuscript preparation and revision.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: JT is funded by the National Health and Medical Research Council (NHMRC) and Australian Research Council (Fellowship ID1106603) and The University of Melbourne. MEM is funded by NHMRC grants (APP1134495, APP1104237, APP1114210, APP11523) and has a joint appointment with Healthscope and La Trobe University. CM is employed by Parkinson’s Victoria. FAB is funded by NHMRC grants (APP1169867, APP1137853) and is employed by The University of Melbourne. APV is chief science officer of Redenlab who provided assistance with the acoustic analysis. He receives salaried support from the NHRMC (Fellowship ID1152223) and also receives institutional support from The University of Melbourne. This research was funded by The University of Melbourne.