
Abstract
Background:
Mobility is a key priority for stroke survivors. Worldwide consensus of standardized outcome instruments for measuring mobility recovery after stroke is an essential milestone to optimize the quality of stroke rehabilitation and recovery studies and to enable data synthesis across trials.
Methods:
Using a standardized methodology, which involved convening of 13 worldwide experts in the field of mobility rehabilitation, consensus was established through an a priori defined survey-based approach followed by group discussions. The group agreed on balance- and mobility-related definitions and recommended a core set of outcome measure instruments for lower extremity motor function, balance and mobility, biomechanical metrics, and technologies for measuring quality of movement.
Results:
Selected measures included the Fugl-Meyer Motor Assessment lower extremity subscale for motor function, the Trunk Impairment Scale for sitting balance, and the Mini Balance Evaluation System Test (Mini-BESTest) and Berg Balance Scale (BBS) for standing balance. The group recommended the Functional Ambulation Category (FAC, 0–5) for walking independence, the 10-meter Walk Test (10 mWT) for walking speed, the 6-Minute Walk Test (6 MWT) for walking endurance, and the Dynamic Gait Index (DGI) for complex walking. An FAC score of less than three should be used to determine the need for an additional standing test (FAC < 3, add BBS to Mini-BESTest) or the feasibility to assess walking (FAC < 3, 10 mWT, 6 MWT, and DGI are “not testable”). In addition, recommendations are given for prioritized kinetic and kinematic metrics to be investigated that measure recovery of movement quality of standing balance and walking, as well as for assessment protocols and preferred equipment to be used.
Conclusions:
The present recommendations of measures, metrics, technology, and protocols build on previous consensus meetings of the International Stroke Recovery and Rehabilitation Alliance to guide the research community to improve the validity and comparability between stroke recovery and rehabilitation studies as a prerequisite for building high-quality, standardized “big data” sets. Ultimately, these recommendations could lead to high-quality, participant-specific data sets to aid the progress toward precision medicine in stroke rehabilitation.
This is a visual representation of the abstract.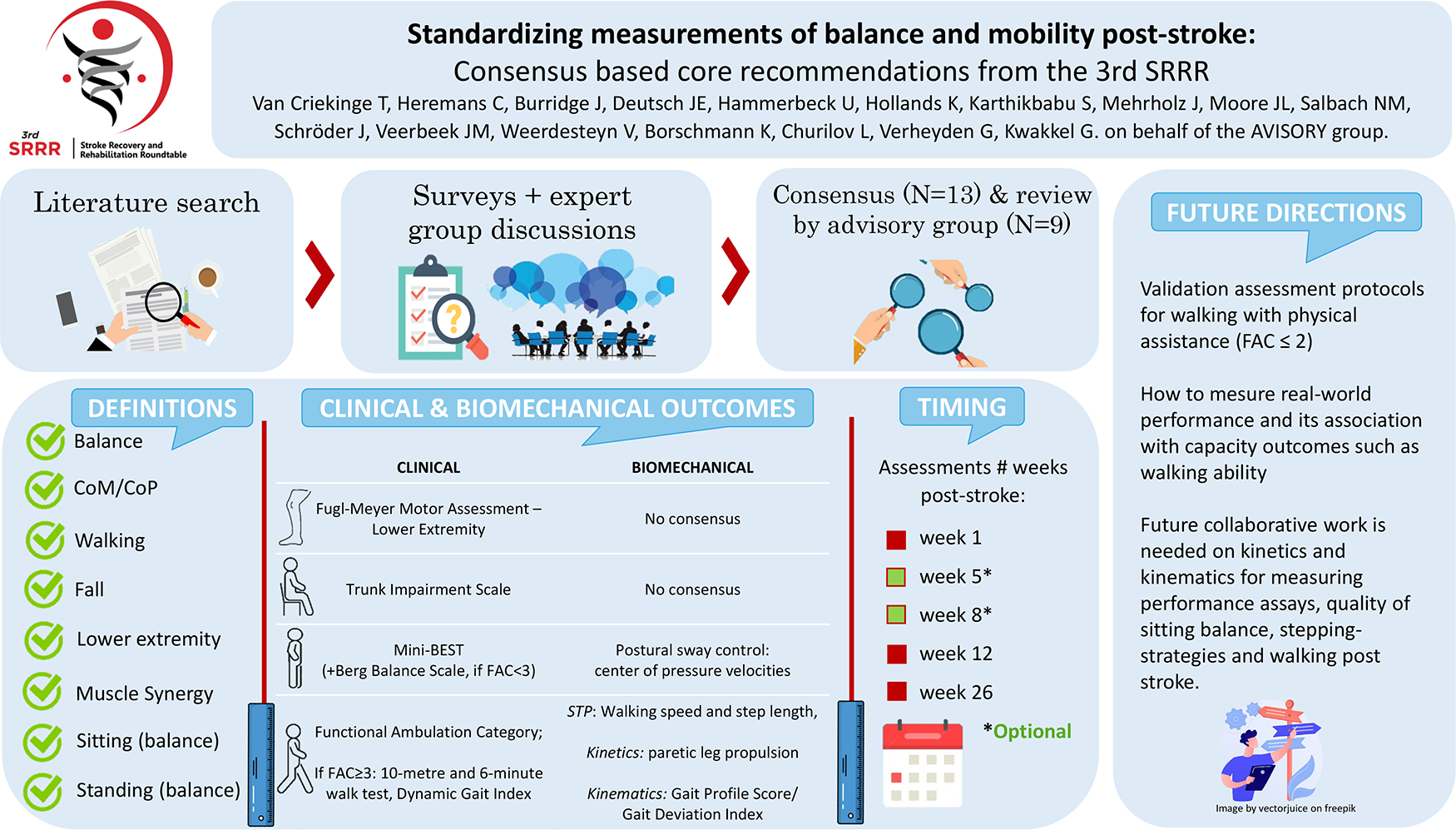
Introduction
Stroke is a major disabling condition in the adult population worldwide, and recovery of post-stroke mobility is largely dependent on the ability to regain lower extremity function, sitting, and standing balance. 1 The International Classification of Functioning, Disability and Health (ICF) framework 2 defines “mobility” as: (1) changing and maintaining body position (d410-d429), (2) carrying, moving, and handling objects (d430-d449), (3) walking and moving (d450-d469), and (4) moving around using transportation (d470-d489). 2 These functions determine independence in mobility and are often chosen as a rehabilitation priority by stroke survivors. 3 Consequently, improving mobility is selected as a primary objective in stroke recovery and rehabilitation trials.4,5 Although epidemiological studies remain scarce, 6 prospective cohort studies suggest that 80 7 –95% 8 of people with stroke regain walking independence, with or without the use of walking aids, within the first 3–6 months post-stroke. 6 This rate drops to 60% in individuals unable to walk in the first week post-stroke. 9 Besides the strong time-dependency of using outcome measurement instruments (OMIs) in the first 3 months, 10 recovery of walking has been significantly associated with factors, such as an intact corticospinal tract, 11 muscle strength of the most affected lower extremity, 11 continence, 11 sitting, 12 standing balance, 13 and cognition. 11
Currently, the comparison or pooling of existing prognostic stroke studies and trials applying similar interventions is hindered by the heterogeneity of mobility-related OMI.11,14 For example, many different distances are used in the literature to measure walking speed, such as the 3, 5, 7, 8, 10, or 12 meters. 15 Each walking speed test is based on different testing protocols resulting into different psychometric properties. 15 Standardization of OMI allows for meta-synthesis of data from different studies needed for adequate power exploration of the many complex body functions that underpin independent mobility. Thus, there is an urgent need for a recommended core set of OMI allowing synthesis and comparison of participant data. Ultimately, these recommendations could lead to high-quality, participant-specific data sets to aid the progress toward precision medicine in stroke rehabilitation.
So far, no overarching recommendations for using the same OMI and biomechanical metrics for balance and mobility exists in the stroke research community. Existing recommendations15,16,17 that guide clinical practice are too elaborate, as they recommend without substantiating multiple OMI for the same construct 16 whereas recommendations on biomechanical metrics are lacking for measuring balance and mobility. Consensus on measuring the fine-grained movement quality measures that are sensitive and specific, able to capture small behavioral changes, is imperative, not only for distinguishing behavioral restitution from compensation in stroke recovery and rehabilitation trials, but also to make proper interpretation of longitudinal neuroimaging studies (e.g. functional magnetic resonance imaging (fMRI), diffusion tensor imaging (DTI), and electroencephalography (EEG)) that may underly functional recovery post-stroke. 18
The International Stroke Recovery and Rehabilitation Alliance aims to facilitate breakthroughs for stroke survivors through global collaborations on specific themes. 19 Through this initiative, we invited international experts in the field of stroke mobility to take part in the third Stroke Recovery and Rehabilitation Roundtable (SRRR3). The SRRR3 builds on achieved consensus on defining different time points post-stroke, 20 recommended core set of OMI (SRRR1) 21 and biomechanical metrics to measure quality of upper extremity movement (SRRR2). 18 These metrics allow us to differentiate between recovery achieved from behavioral restitution or compensation. 22 Furthermore, the achieved consensus is based on different ICF constructs and includes recommendations on standardized assessment protocols, and equipment for quantitative assessment of mobility. Therefore, the work in this SRRR3 addressed the following questions to aid future stroke rehabilitation and recovery studies:
Which baseline characteristics for participants should be added to the SRRR1 recommendations in the field of lower extremity motor function, balance, and mobility?
At what time points within the first 6 months post-stroke should lower extremity motor function, balance, and mobility outcomes be measured?
How should constructs of lower extremity motor function, balance, and mobility be defined?
Which core set of OMI and accompanying assessment protocols should be recommended for investigating lower extremity motor function, balance and mobility post-stroke?
Which biomechanical metrics should be recommended for quantifying quality of balance and mobility recovery post-stroke?
Which types of technological equipment should be recommended for measuring quality of balance and mobility recovery post-stroke?
Methods
Consensus building
The SRRR3 started with a “preparatory group” of four members (GK, GV, TVC, CH) who formulated the research questions (GK and GV), prepared evidence tables, and designed questionnaires (TVC and CH). Two methodological experts (KB and LC) were consulted, and all 11 stroke research experts from North America (3), Europe (7), and Asia (1) accepted the invitation to join the “core group.” Established experts as well as emerging leaders were selected based on their professional background (physiotherapy and movement sciences) and impact of their scientific publications in the fields of balance and/or mobility post-stroke. None of the invited experts of the core group had a conflict of interest. A five-stage process following a voting-based graph theory was undertaken to form consensus (Figure 1), 23 consisting of three online questionnaires followed by three online meetings and one hybrid meeting to discuss the six research questions. The methods employed were the same as in previous SRRR.18,21
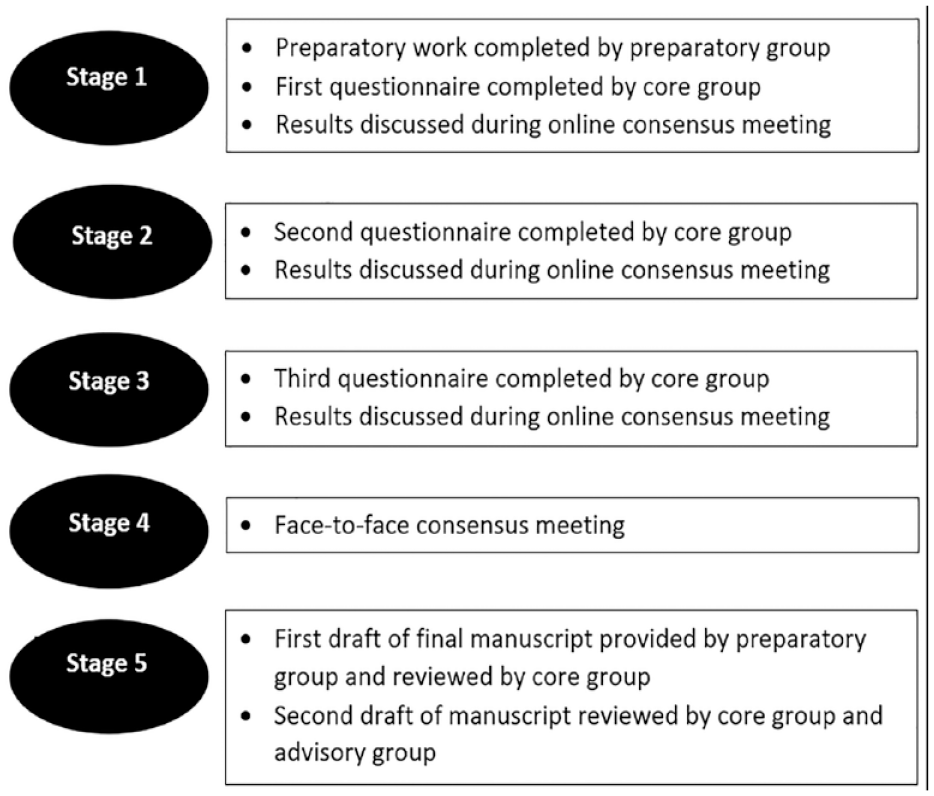
Stages of consensus building.
Stage 1
Prior to administering the online questionnaires, the preparatory group performed a scoping review to identify current OMI being used in stroke research, by compiling the evidence of 60 reviews on mobility interventions and on measurement properties. Subsequently, a summary of balance and mobility-related definitions, measurement properties of OMI, and biomechanical metrics in stroke rehabilitation was extracted from 220 studies (167 clinical and 53 biomechanical studies) and presented in a tabular overview (see Supplemental Appendix 1). Relevant studies were only included when OMI and assessment protocols were published in a peer-reviewed journal and at least one of the following measurement properties was reported: reliability, validity, internal consistency, ceiling/floor effects, responsiveness, minimal detectable change, minimal important clinical difference, and measurement error. Tables were structured in agreement with the international consensus guidelines of COSMIN 24 and COMET. 25 The tables in Supplemental Appendix 1 representing the candidate measurement instruments were part of the first online consensus meeting with the consensus group. While completing each questionnaire, the expert of the core group was able to consult these resource tables. Questionnaires were created and administered using QualtricsXM software (QualtricsXM PlatformTM, Utah, US), and focused on finding consensus for research questions 2–6 presented in the introduction of this article. For each question, different answers were presented to elicit individual panel members’ preferred ranking of presented answers. Therefore, the core group was asked to rank the provided answers (e.g. definitions, OMI, equipment) from highest to lowest priority within each ICF construct, based on their expert opinion and the measurement properties presented in the tables.
The first questionnaire included an option “other” or “user-specific answer” where experts could provide a unique response not included in the provided ranking options. The results were summarized by two members of the preparatory group who did not participate in the questionnaire (TVC–CH) and data analyses were performed by an independent statistician (LC) who was not involved in the consensus meetings. Individual responses were combined into one group-level ranked list, by aggregating individual rank-ordered lists using a robust graph theory-based voting system,23,26 which was implemented as a decision-support tool in Microsoft Excel. The analysis of the voting-based graph theory resulted in Condorcet’s of ranked outcomes, from “most preferred” to “least preferred.” In cases of a clear “most preferred” option (or winner, with no equal number of votes), the core group achieved consensus in stage 1. Results of the data analysis were discussed during a subsequent 2-h online consensus meeting within the core group.
Stages 2 and 3
To resolve disagreements from stage 1, a second online questionnaire was created with alterations in ranked answer options for questions without a “most preferred” winner. For these questions, the following methods were used: (1) when response options received the same ranking (tied with an equal number of votes), answers were again presented with either the same or altered ranking options, based on the received feedback from the core group during the consensus meeting and (2) when a new, user-specific answer was proposed by an expert, the “most preferred” option (in case of a “winner”) or all options were offered together with the new, user-specific answer. Data analysis was performed as described in stage 1 and followed by a second online meeting. The same methodology was adopted in stage 3.
Stage 4
A 2-day hybrid (in-person and online) meeting was held (Vienna, Austria, December 2022), where core group members discussed the results of stage 3 and reviewed the structure of the first draft of the article. In addition, potential experts in the field of stroke research for the “advisory group” were selected to review the recommendations and article. The advisory group was chosen based on their track record of publications in the field of post-stroke balance and/or mobility, as well as their professional background in movement science, physiotherapy, or bioengineering. None of the invited experts of the advisory group had a conflict of interest.
Stage 5
The first draft of the final recommendations was provided by the preparatory group and reviewed by the core members. The pre-final draft of the recommendations was reviewed by the core and advisory group.
Results
Consensus approach
During SRRR3, we agreed to focus on the evaluation of “balance” and “mobility” defined by the core groups as “the act of maintaining, achieving or restoring a state of control during any posture or activity” and by ICF as “changing and maintaining body position” and “walking and moving.” 2 The structure of the three questionnaires and the responses received from the core group are included in Supplemental Table 1.
Agreed baseline characteristics for lower extremity motor function, balance, and mobility studies
Box 1 shows in bold the recommended baseline characteristics that should be collected in addition to the minimal core set (SRRR1) 21 within the first 24 h after stroke in studies investigating recovery of balance and/or mobility post-stroke.
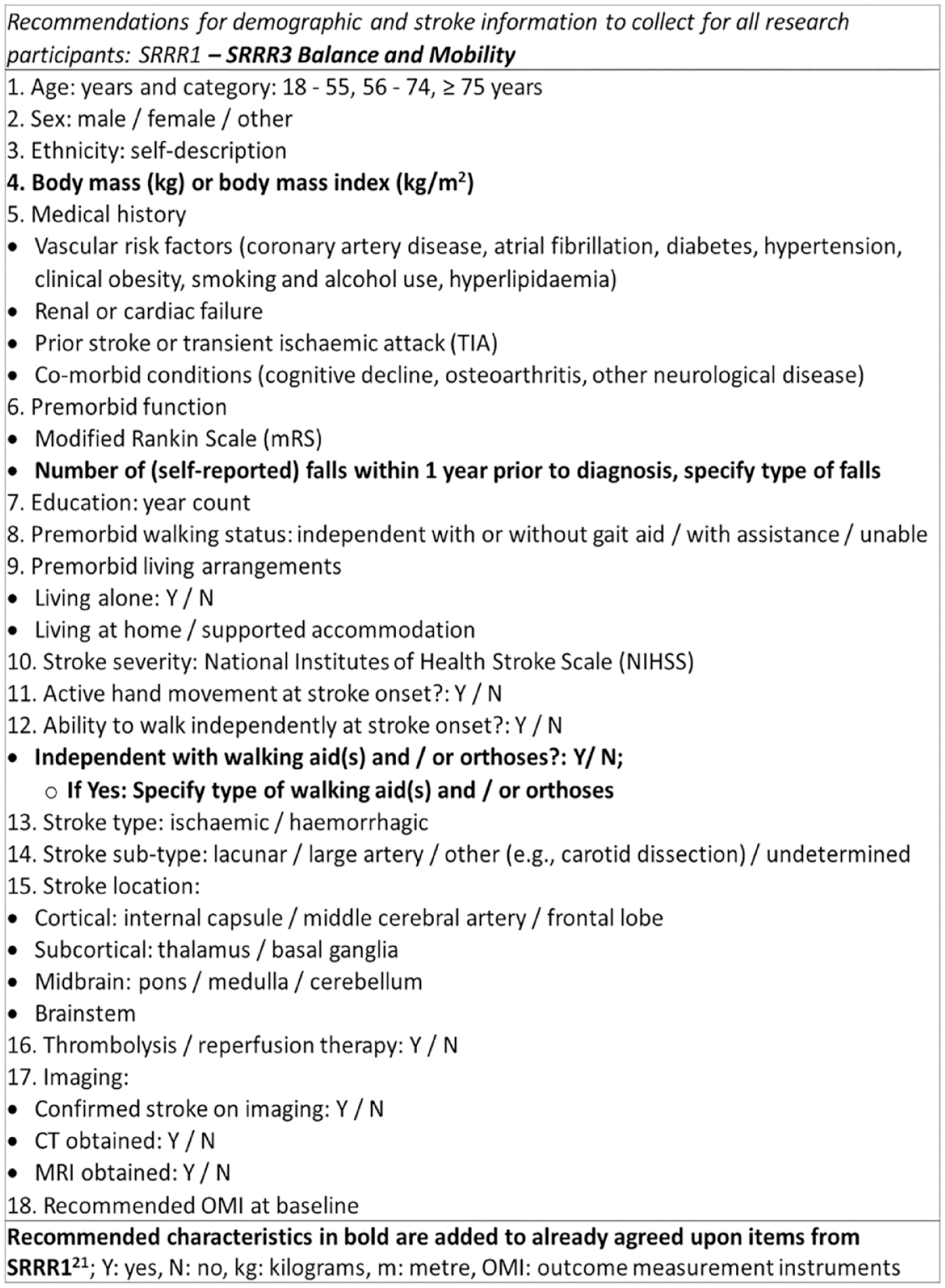
SRRR1 and SRRR3 recommendations for baseline characteristics in lower limb motor function, balance and mobility studies.
Agreed timing of assessments
Timing of assessments was in accordance to SRRR1, 21 as the time course of upper- and lower-extremity motor recovery is similar within the first 6 months post-stroke. 27 Minimal time points are therefore within the first week (day 5), at 12 and 26 weeks (months 3 and 6) post-stroke, with recommended time points at weeks 5 and 8. As it is suggested that recovery or decline of mobility may take longer than 6 months, 28 we recommend to repeat the same OMI in the chronic phase. However, no specific time points were recommended, as this was beyond the scope of SRRR3. In agreement with SRRR1, 21 the time points of measurements should always refer to time post-stroke onset and not the time of admission or enrollment in the trial.
Agreed measurement properties
Content validity was our top prioritized item guiding our choice of OMI for the different constructs of recovery post-stroke and was defined according to COSMIN as “the degree to which a measurement is an adequate reflection of the construct to be measured.” 24 In addition, we agreed that OMI have to be reliable and sensitive to change in the proposed construct to be recommended for studies.
Agreed definitions of underlying constructs of lower extremity motor function, balance and mobility
Box 2 shows in alphabetic order the agreed definitions of the different a priori chosen constructs related to balance and mobility post-stroke, and other commonly used terms. We defined “balance” as “steady-state,” “proactive,” and “reactive” balance but rejected the distinction between “static” and “dynamic” balance, as the act of balancing is always dynamic in its nature. Performance assay was defined as “an isolated core motor execution capacity tested outside of a functional task context.” 18
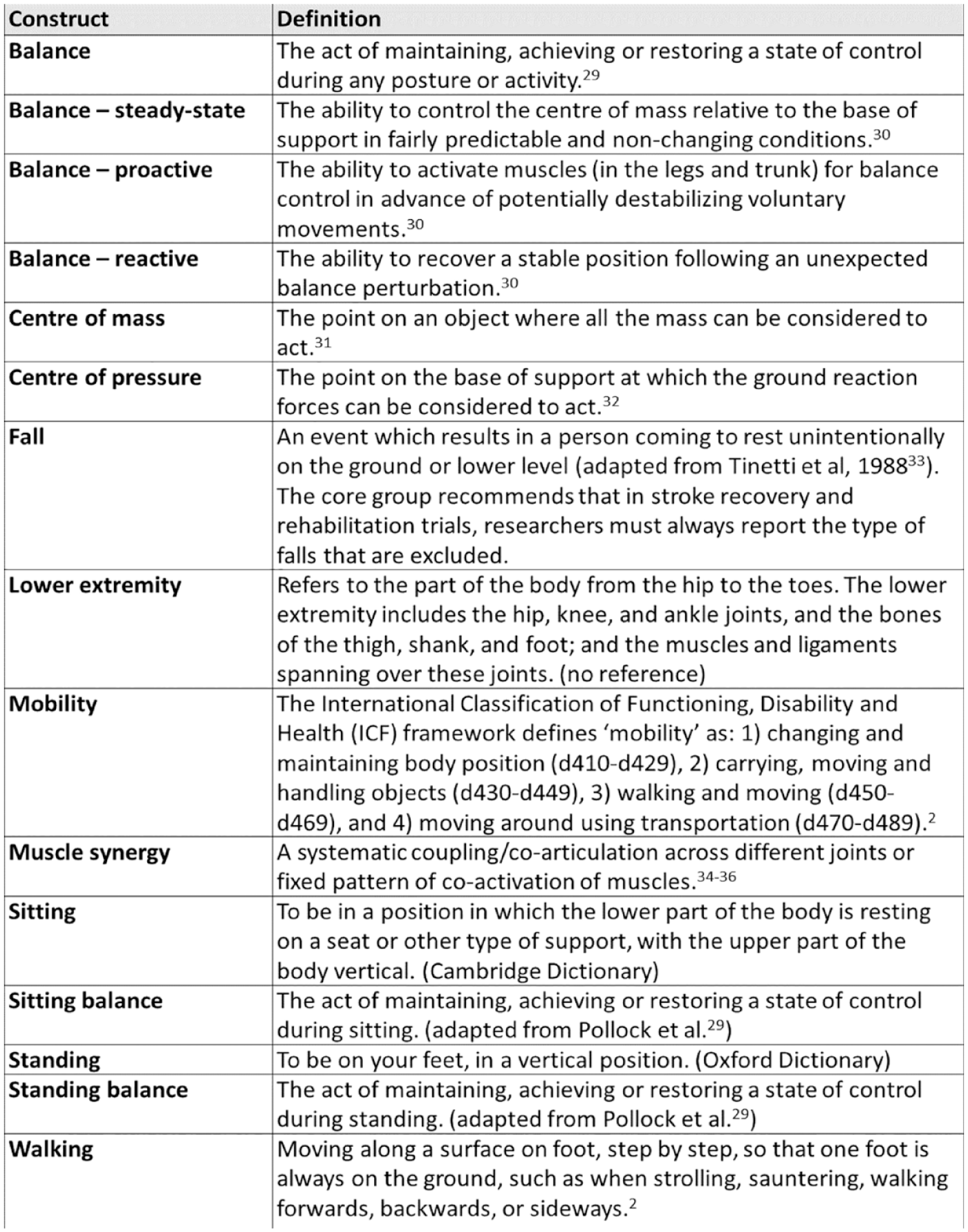
SRRR3 agreed definitions of constructs in the field of lower extremity motor function, balance, and mobility post-stroke in an alphabetic order.
Agreed core set of OMI for measuring lower extremity motor function, balance, and mobility
Box 3 presents the core set of OMI for lower extremity motor function, balance, and mobility in stroke recovery and rehabilitation studies within the first 6 months post-stroke. For measuring motor function of the most affected lower extremity, we recommend the Fugl-Meyer Motor Assessment lower extremity (FMA-LE) subscale 37 . The SRRR3 was unable to give recommendations with respect to a specific performance assay.
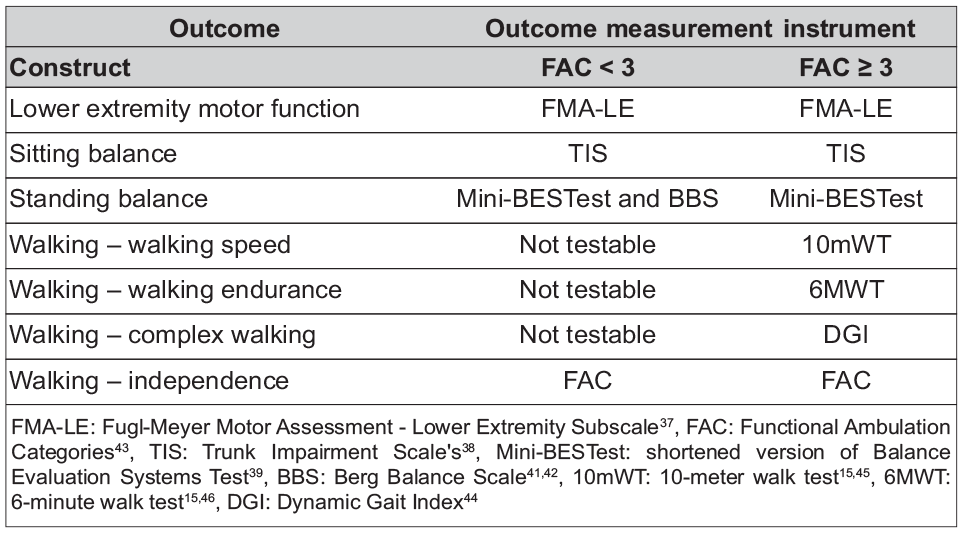
SRRR3 recommendations for a core set of assessment tools for measuring lower extremity motor function, balance, and mobility post-stroke.
We recommend the Trunk Impairment Scale 38 (TIS) for assessment of sitting balance and a shortened version of the Balance Evaluation Systems Test 39 (Mini-BESTest) for measuring standing balance. Although the Mini-BESTest shows excellent measurement properties even in mildly impaired participants and includes items assessing steady-state, proactive, and reactive balance, it has significant floor effects. 40 Therefore, the addition of the Berg Balance Scale41,42 (BBS) to the Mini-BESTest is recommended for individuals requiring physical assistance for walking ability (defined as Functional Ambulation Category 43 (FAC) < 3). When the BBS is selected, we recommend that it is used throughout the research trial, even in cases where the FAC improves to ⩾ 3.
The FAC was recommended to classify walking ability and walking independence. In case of an FAC score ⩾ 3, the 10-meter walk test (10 mWT), 6-Min Walk Test (6 MWT), and Dynamic Gait Index 44 (DGI) are recommended for assessing walking speed, walking endurance, and complex walking, respectively, and should ideally be performed without the use of a walking aid. However, the use of a walking aid is permitted and should always be documented. In case of an FAC < 3 (i.e. physical assistance by another person is required), further performance on walking tests should be documented as “Not Testable” instead of assigning a value of “zero,” acknowledging that the inability to walk is not the same as having a walking speed of zero. The proportion of participants able to walk independently and safely (FAC ⩾ 4) or not (FAC < 4), should also be reported.
As shown in protocols provided in Supplemental Appendix 2, the 10 mWT should be tested at a comfortable pace on a straight and level 14-meter walkway, a 10-meter timed distance and a 2-meter acceleration deceleration distance, respecitvely.15,45 The 10 mWT should be administered three times and based on the average time taken to walk 10 meters (in seconds). Walking speed (in meters per second) should be the reported outcome. The 6 MWT should be administered once on a straight 30-meter walkway with standardized encouragement phrases each minute,15,46 and without a practice trial. 47 The total distance walked should be reported (in meters). When a walking aid and/or orthosis is used to perform walking tests, the type of aid and/or orthosis should be documented, and the same aid should be used during retest. For safety reasons, the evaluator should walk on the affected side, but slightly behind the participant. The detailed assessment protocols with full instructions and scoring sheet of all OMI can be found in Supplemental Appendix 2.
Agreed biomechanical metrics for measuring quality of sitting, standing, and walking
Box 4 presents the preliminary core set of biomechanical metrics for assessing balance and mobility in stroke recovery and rehabilitation studies within the first 6 months post-stroke. For measuring quality of sitting, we are unable to provide recommendations on how to measure sitting balance in a biomechanical way due to a lack of validated instruments and robust protocols.
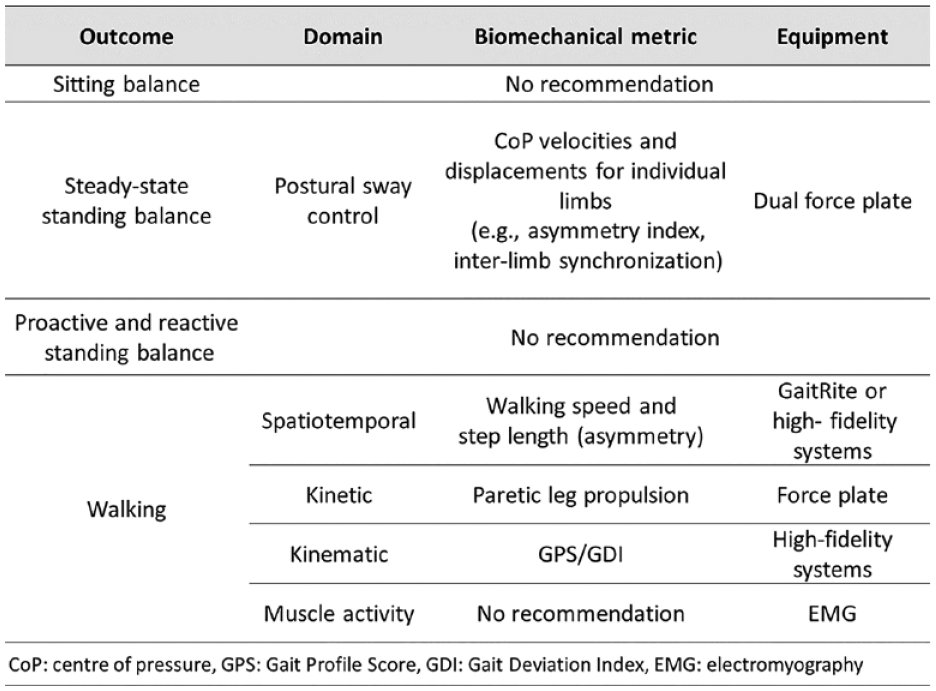
SRRR3 recommendations for biomechanical metrics and corresponding technological equipment for measuring balance and mobility post-stroke.
For assessing quality of steady-state standing balance, we prioritized center of pressure (CoP) measurements of each individual limb using a dual force plate. More specific, CoP velocity metrics, expressed as asymmetry indexes 48 and inter-limb synchronization measures 49 are of interest, as descriptors of the relative paretic leg contribution to postural sway control. The participant should be assessed barefoot in at least two core conditions: eyes open and eyes closed for at least 30 s per condition, in-line with the slightly adjusted assessment protocol of Mansfield and Inness. 50 An average of three successive trials should be reported to maximize reliability of CoP outcomes. 51 However, we could not reach consensus on a definitive biomechanical core set for steady-state, proactive, and reactive balance outcomes and, therefore, recommend a further roundtable with experts in the field of biomechanical measurements.
The minimal reporting requirement to measure quality of walking is spatiotemporal parameters (i.e. walking speed and step length), followed by, in order of priority: kinetics, kinematics, and muscle activity. Kinetic metrics are prioritized for their insights into propulsion mechanisms. Asymmetry metrics are especially recommended to provide greater insights into compensatory mechanisms and underlying kinematic strategies, 52 together with stride-normalized ground reaction forces to measure the relative contribution of the paretic leg to propulsion generation. 53 Furthermore, we recommend the use of a multivariate kinematic metric, such as the Gait Profile Score 54 or Gait Deviation Index, 55 which provides a comprehensive and clinically meaningful interpretation of walking. Finally, surface electromyography was proposed for measuring muscle activity, yet at this stage, we are unable to recommend a single prioritized metric. Similar to CoP measurements of steady-state balance, we provide global recommendations for the assessment of quality of walking and propose a next separate SRRR round to provide more specific recommendations. Concerning data acquisition, the task force recommends that participants perform tests of walking quality with and without the use of orthoses, walking aids, and footwear, to allow comparison with and between OMI over time.
Agreed technological equipment for measuring quality of balance and mobility
Concerning biomechanical assessments of balance and mobility, we recommend using force plates (sampling frequency ⩾ 100 Hz) 51 and high-fidelity optoelectronic measurement systems 18 (e.g. 3D motion capture systems with sampling frequency ⩾ 60 Hz). These high-fidelity systems should be applied by people with expertise and access to these technologies, without limiting to specific brands. However, we recommend, at this point, not to use portable equipment (e.g. gaming devices, pressure plates) or wearable equipment (e.g. inertial devices, gyroscopes, and accelerometers) for measuring balance and mobility in recovery studies due to a lack of validated assessment protocols and reliable biomechanical metrics extracted from this equipment. In contrast, for spatiotemporal parameters, we agreed that the GaitRite is the prioritized, non-optical, measurement tool with sufficient reliability and validity. 56
Discussion
The current consensus builds on previous SRRR18,21 and provides recommendations for recovery and rehabilitation studies with respect to definitions of balance and mobility, a minimal core set of baseline characteristics, OMI and biomechanical metrics with standardized assessment protocols, and preferred measurement time points. Unfortunately, different protocols are being used for the same test worldwide, which may prevent comparison of results. Therefore, we included assessment protocols with standardization of, for example, walkway length, walking speed, instructions, use of aids, as well as differences in scoring when the participant is unable to walk. These OMI are core outcomes for the various proposed constructs. It is therefore recommended to first define the study construct before choosing the appropriate OMI from the core set related to this construct. In contrast, the SRRR3 could only provide global recommendations concerning biomechanical metrics and recommends that further collaborative work is needed on establishing core metrics. Particularly, studies adhering to the recommended timing of assessment post-stroke are needed to investigate the longitudinal associations between the different underlying constructs within participants. Therefore, the current results should be seen as a first step toward defining constructs and standardization of testing protocols as a conditional for pooling studies and individual data. Ultimately, the current recommendations could lead to high-quality, participant-specific data sets to aid the progress toward precision medicine in stroke rehabilitation. This step is important, acknowledging that stroke is a heterogeneous disorder. Current stroke rehabilitation approaches are based on the “one-size-fits-all” principle, which treats patients as an “average” person and ignores the individual differences. Precision medicine, on the other hand, uses “big data” from clinical and multimodal MRI to tailor the treatment and prevention strategies to each patient’s specific needs.20,57,58 Ultimately, these big data sets allow us to classify pheno(sub)types at a participant-specific level and to identify those who do and do not respond to an evidence-based intervention.
Strengths and limitations
To develop recommendations for measuring balance and mobility in stroke recovery and rehabilitation studies, we undertook an extensive literature review, consulted experts, and applied decision analytics. The latter was based on the voting-based graph theory resulting into ranked outcomes instead of the commonly used Delphi method. The Delphi method is more time-consuming, requires interpretation of complex language, and recommends only one outcome, while the adopted methodology is a time-efficient process creating manageable lists with ordinal preference scores per outcome. 26 There are some limitations to consider. First, ICF-mobility items 2 “carrying of objects” and “using transportation,” as well as risk of falls 59 were not included in the SRRR3. The ability to be mobile in the presence of external demands or in challenging environments are seen as important factors in regaining independence during activities of daily living. As there are currently no reliable and valid OMI available to assess daily life abilities, the development of these OMI are a research priority. Second, although the optional recommended time points for assessments on weeks 5 and 8 were chosen relatively arbitrary, there is some recent evidence supporting this statement. Recent research of Schröder et al. suggested that a plateau of recovery around week 8 for the majority of measures assessing lower limb function and standing balance. 60 Only the weight-bearing asymmetry improved until week 12 (month 3). Therefore, we have set these time points as optional yet recommended. Third, we acknowledge that some of our recommended OMI have significant limitations, such as the FMA-LE, which lacks responsiveness, shows ceiling effects, and is confounded by muscle strength requirements. 61 Yet, no better psychometrically sound alternative is currently available for assessing pathological synergistic movements of the lower extremity post-stroke. In the future, this void may be filled by using kinematic and kinetic metrics for assessing quality of movement. Fourth, we acknowledge that recommended OMI show some overlap in their underlying constructs such as the Mini-BESTest measuring not only aspects of balance but also mobility, such as compensatory stepping in different directions, change in walking speed, and “timed up and go.” In addition, we are aware that applying the whole recommended core set may oblige researchers to make prioritizations to reduce the overall testing time. Fifth, in contrast with SRRR2, 18 we were unable to recommend performance assays for measuring behavioral restitution at the ICF level of body functions of the lower extremity, nor a standardized test at the level of daily activities for identification of compensation post-stroke. For this standardized test, we need a large age- and sex-matched normative data set captured with a high-fidelity 3D system. Subsequently, although some recommendations were provided as a first step toward global recommendations, further work on biomechanical metrics in a future consensus meeting is required. These recommendations should be based on principles derived from motor control and include the technological equipment and validated assessment protocols for measuring quality of balance and mobility post-stroke. Finally, the recommended OMI were selected by researchers, although some members of the core and advisory group also had clinical training; the recommended OMI might not represent the preferences and priorities of practicing clinicians and/or patients.
Future research
First, our recommendation to only assess walking when participants have an FAC score ⩾ 3 leads to missing data for those who can walk with some physical assistance from another person for balance control (FAC 2). We acknowledge that this restricts our ability to measure change in individuals with an FAC < 3, resulting in the loss of relevant information. There are several protocols in which physical assistance is allowed during walking, limited to support with one hand.62,63 We propose that future research should further validate these assessment protocols in which physical assistance is allowed. In addition, we only recommended OMI that are qualified as “capacity” (i.e. individual can complete in a standardized environment 2 ), as opposed to “performance” (i.e. what a person actually does in their usual environment 2 ). Of note, improvements in capacity may not directly translate into improvements in real-world performance, as research has demonstrated changes in capacity without observed performance improvements in individuals post-stroke undergoing walking interventions. 64 Moreover, walking independence that was defined in this study as FAC > 3 might have a different meaning to stroke survivors and could be entangled with measures of endurance or walking speed (e.g. the freedom to walk whenever they need to, for whatever distance, in whatever environment). This perceived independence of the subject was not part of the current consensus-based study. Yet, identifying the potential impact of rehabilitation interventions on both capacity and performance, and participants’ perceived change through self-report, is a necessity to gain further insights into the effectiveness of rehabilitation interventions and aid appropriate application of interventions into clinical practice. More research on the measurement of real-world performance requires validation of protocols in which portable and wearable instrumentation is applied.
Supplemental Material
sj-docx-2-nnr-10.1177_15459683231209154 – Supplemental material for Standardized measurement of balance and mobility post-stroke: Consensus-based core recommendations from the third Stroke Recovery and Rehabilitation Roundtable
Supplemental material, sj-docx-2-nnr-10.1177_15459683231209154 for Standardized measurement of balance and mobility post-stroke: Consensus-based core recommendations from the third Stroke Recovery and Rehabilitation Roundtable by Tamaya Van Criekinge, Charlotte Heremans, Jane Burridge, Judith E Deutsch, Ulrike Hammerbeck, Kristen Hollands, Suruliraj Karthikbabu, Jan Mehrholz, Jennifer L Moore, Nancy M Salbach, Jonas Schröder, Janne M Veerbeek, Vivian Weerdesteyn, Karen Borschmann, Leonid Churilov, Geert Verheyden and Gert Kwakkel in Neurorehabilitation and Neural Repair
Supplemental Material
sj-docx-3-nnr-10.1177_15459683231209154 – Supplemental material for Standardized measurement of balance and mobility post-stroke: Consensus-based core recommendations from the third Stroke Recovery and Rehabilitation Roundtable
Supplemental material, sj-docx-3-nnr-10.1177_15459683231209154 for Standardized measurement of balance and mobility post-stroke: Consensus-based core recommendations from the third Stroke Recovery and Rehabilitation Roundtable by Tamaya Van Criekinge, Charlotte Heremans, Jane Burridge, Judith E Deutsch, Ulrike Hammerbeck, Kristen Hollands, Suruliraj Karthikbabu, Jan Mehrholz, Jennifer L Moore, Nancy M Salbach, Jonas Schröder, Janne M Veerbeek, Vivian Weerdesteyn, Karen Borschmann, Leonid Churilov, Geert Verheyden and Gert Kwakkel in Neurorehabilitation and Neural Repair
Supplemental Material
sj-xlsx-1-nnr-10.1177_15459683231209154 – Supplemental material for Standardized measurement of balance and mobility post-stroke: Consensus-based core recommendations from the third Stroke Recovery and Rehabilitation Roundtable
Supplemental material, sj-xlsx-1-nnr-10.1177_15459683231209154 for Standardized measurement of balance and mobility post-stroke: Consensus-based core recommendations from the third Stroke Recovery and Rehabilitation Roundtable by Tamaya Van Criekinge, Charlotte Heremans, Jane Burridge, Judith E Deutsch, Ulrike Hammerbeck, Kristen Hollands, Suruliraj Karthikbabu, Jan Mehrholz, Jennifer L Moore, Nancy M Salbach, Jonas Schröder, Janne M Veerbeek, Vivian Weerdesteyn, Karen Borschmann, Leonid Churilov, Geert Verheyden and Gert Kwakkel in Neurorehabilitation and Neural Repair
Footnotes
Acknowledgements
The third international Stroke Recovery and Rehabilitation Roundtables are an initiative of the International Stroke Recovery and Rehabilitation Alliance. The authors acknowledge Drs Hayward and Kwakkel for co-chairing and convening the SRRRIII and Dalton for managing SRRRIII conduct and in-person meeting organization. They thank their Advisory Group members: Dr Martina Betschart, Dr Pierce Boyne, Dr Jaap Buurke, Dr Helen Dawes, Dr Avril Mansfield, Dr Sarah Moore, Dr Darcy Reisman, Dr Eva Swinnen, and Dr Ada Tang.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was aided with financial support from Canadian Partnership for Stroke Recovery, NHMRC Center of Research Excellence to Accelerate Stroke Trial Innovation and Translation (GNT2015705), and unrestricted educational grants provided by Ipsen Pharma and Moleac.
Statement of endorsement
World Stroke Organization (WSO) endorses the goals of the third international Stroke Recovery and Rehabilitation Roundtable (SRRRIII) research activity, which are consistent with the mission of the WSO.
Supplementary material for this article is available on the Neurorehabilitation & Neural Repair website along with the online version of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.