
Abstract
Background
Mobility impairment is common in older persons with multiple sclerosis (MS), and further compounded by general age-related mobility decline but its underlying brain substrates are poorly understood.
Objective
Examine fronto-striatal white matter (WM) integrity and lesion load as imaging correlates of mobility outcomes in older persons with and without MS.
Methods
Fifty-one older MS patients (age 64.9 ± 3.7 years, 29 women) and 50 healthy, matched controls (66.2 ± 3.2 years, 24 women), participated in the study, which included physical and cognitive test batteries and 3T MRI imaging session. Primary imaging measures were fractional anisotropy (FA) and WM lesion load. The relationship between mobility impairment, defined using a validated short physical performance battery cutoff score, and neuroimaging measures was assessed with stratified logistic regression models. FA was extracted from six fronto-striatal circuits (left/right): dorsal striatum (dStr)-to-anterior dorsolateral prefrontal cortex (aDLPFC), dStr-to-posterior DLPFC, and ventral striatum (vStr)-to-ventromedial prefrontal cortex (VMPFC).
Results
Mobility impairment was significantly associated with lower FA in two circuits, left dStr-aDLPFC (P = .003) and left vStr-VMPFC (P = .004), in healthy controls but not in MS patients (P > .20), for fully adjusted regression models. Conversely, in MS patients but not in healthy controls, mobility impairment was significantly associated with greater lesion volume (P < .02).
Conclusions
Comparing older persons with and without MS, we provide compelling evidence of a double dissociation between the presence of mobility impairment and two neuroimaging markers of white matter integrity, fronto-striatal fractional anisotropy, and whole brain lesion load.
Keywords
Introduction
Multiple sclerosis (MS) is an immune-mediated, neurodegenerative disease of the central nervous system, affecting close to one million people in the United States; 40% of patients aged 55 years or older. 1 Mobility impairment, a clinical hallmark of MS, 2 is defined by the limitation in the ability to move independently from one location to another, 3 and is associated with many adverse outcomes including disability, falls, and mortality; 4 recent data have shown the compounding effects of aging and MS on mobility impairment. 5 Focal brain lesions are noteworthy in the diagnosis of MS, 6 but knowledge concerning the relationship between mobility impairments and lesion volume and with brain structures and white matter (WM) integrity in MS is limited.
Previous work has shown associations between aspects of mobility function in MS patients and cortical7,8 and subcortical grey matter,9,10 and lesion volume.11,12 However, this literature is almost exclusively limited to young and middle-aged patients. Recent epidemiological evidence suggests a shift in the peak prevalence of MS into older age groups, 13 but information specifically related to brain control of mobility in older persons with MS (PWMS) remains unknown. In normal aging, there are meaningful associations between executive functions, subserved by the prefrontal cortex, 14 and mobility performance. 15 Consistent with these findings, review and meta-analytic studies have identified both fronto-striatal grey and WM as critical in brain control of locomotion in older adults. 16 Diffusion tensor imaging (DTI) is an effective tool for elucidating changes in WM integrity, and can detect WM abnormalities not revealed on conventional MR imaging. DTI studies have demonstrated changes in WM integrity related to mobility impairments in middle-aged PWMS.17,18 Results in older adults without MS have shown similar utility of DTI in the assessment of gait impairments, although the effects of WM lesion burden on results varies across studies.19,20
Because of the well-established role of the fronto-striatal executive networks and prefrontal cortex in cognitive control of mobility,21 -23 our goal was to investigate the relationship of microstructural WM integrity, within well-defined executive fronto-striatal circuits, to mobility function in older PWMS and healthy controls. This has not to our knowledge been previously reported. Studies have suggested that aging is associated with functional dedifferentiation of brain activity, 24 changes that may be further compounded by diseases, such as MS. By focusing on specific brain regions, investigations may elucidate the underlying mechanisms of mobility impairment and their distributions across the brain, which may in turn offer unique targets for clinical intervention. The current study was thus designed to address this important knowledge gap, and test the hypothesis that higher WM integrity of the fronto-striatal circuits is associated with lower odds of mobility impairment. Furthermore, the study was specifically designed to compare and contrast the differential association of fronto-striatal integrity and WM lesion load with mobility impairment in PWMS and healthy age-matched controls. Specifically, we used DTI-based fractional anisotropy (FA) values in three executive circuits, defined via an established fronto-striatal atlas consisting of portions of the dorsal and ventral striatum (vStr) and extending to dorsolateral (dorsolateral prefrontal cortex [DLPFC]) and ventromedial prefrontal cortex (VMPFC). We then determined the differential associations of WM integrity in these three executive circuits, and of global WM lesion burden, with performance on the short physical performance battery (SPPB) 3 in older PWMS and demographically matched controls, while controlling for confounders.
Methods
Participants
The sample was drawn from a cohort of older adults, with and without MS, enrolled in an ongoing study, “Brain Predictors of Mobility and Falls in Older Adults with Multiple Sclerosis.” Participants were recruited and tested between September 2019 and August 2021. MS participants were recruited from regional treatment centers and patient registry lists. Using revised McDonald criteria, 25 all patients had physician-confirmed MS diagnoses as determined by medical record review. Controls were recruited from publicly available population lists stratified by zip code, age and sex, and were first contacted through an institutional review board (IRB)-approved letter, followed by a phone call. Both cohorts were screened via a structured telephone interview to obtain verbal consent, screen for dementia, assess medical and psychological history, as well as mobility and functional abilities to determine initial study eligibility. Exclusion criteria included diagnosis of major neurological, psychiatric, or medical disease (excluding MS), inability to ambulate independently, MRI contraindications, vision or hearing impairment that would negatively impact testing, and difficulty understanding or speaking English. All participants were right-handed. Cognitive status was determined via established clinical case conference procedures through medical records, neuropsychological tests scores, and data concerning instrumental activities of daily living, cognitive complaints, and mood. 26 Eligible, participants were invited for two in-person visits. The first in-person study visit consisted of written informed consent, neuropsychological test battery, mobility protocols (including SPPB), and questionnaires. MRI brain scans and additional questionnaires were collected at a second visit, on average 15 days after the first visit (COVID-19-related scheduling delays resulted in 2 participants with 7 months between visits, and 8 participants with 1-3 month intervals). The study was approved by the IRB of Albert Einstein College of Medicine. The work described in this manuscript was executed in adherence with The Code of Ethics of the World Medical Association (Declaration of Helsinki).
Structural Image Acquisition
MRI was performed in a 3T Philips scanner equipped with a 32-channel head coil (Elition 3.0T X, Philips Medical Systems, Best, The Netherlands) at the Gruss Magnetic Resonance Research Center of Albert Einstein College of Medicine. High resolution 3D T1-weighted (MPRAGE) structural brain images were acquired for registration, WM segmentation and to identify T1-hypointense MS lesions (echo time-TE/repetition time-TR/inversion time-TI: 4.6/9.7/900 milliseconds, voxel size: 1 mm isotropic, flip angle: 8°). 3D fluid-attenuated inversion recovery (FLAIR) images were acquired for identification of hyper-intense T2 lesions (TE/TR/TI: 365/4800/1650 milliseconds, voxel size: 1 mm isotropic); both FLAIR and T1 images were used to identify and quantify MS lesions (see below).
Diffusion Tensor Imaging
DTI images were obtained for tractographic construction of the fronto-striatal atlas and quantification of WM integrity (FA) using a three-shell single-shot spin echo echo-planar imaging sequence (b: 500, 1000, 2000 s/mm2 with 16, 32, 64 directions respectively, TE/TR: 88/3800 milliseconds, voxel size: 2 mm isotropic, matrix: 128 × 128, SENSE acceleration: 1.4, multi-band: 3). A second complete set of DTI images with flipped phase encode and diffusion gradients allowed distortion and motion correction with FSL’s topup and eddy functions. 27 The b1000 shell was used for extraction of FA values via FSL’s dtifit. Tractography-based atlas construction used all three shells. Analyses were implemented through FSL (v. 6.0.1, https://fsl.fmrib.ox.ac.uk/fsl/fslwiki) and MRtrix3 (v. 3.0_RC3). 28
Study-Specific Fronto-Striatal Circuit Atlas Generation
Unbiased fronto-striatal WM integrity measures were extracted using a study-specific fronto-striatal atlas (Figure 1), constructed in 1 mm Montreal Neurological Institute (MNI) space. 29 Briefly, probabilistic tractography was used to construct fronto-striatal tract probability maps in a subset of 10 control participants. We used the Oxford-GSK-Imanova striatal connectivity atlas 30 for striatal seeds, and the Sallet dorsal cortical 31 and Harvard-Oxford cortical 32 atlases for three distinct cortical targets: anterior dorsolateral prefrontal cortex (aDLPFC), posterior DLPFC (pDLPFC), and VMPFC. We extracted the DLPFC mask from the Sallet atlas 31 (Sallet regions 5, 6, and 7), separated into anterior (Brodmann areas 9, 10, and 46), and posterior DLPFC (Brodmann areas 9, 46d, and 9/46v). The aDLPFC atlas comprised Sallet region 7 and the anterior portion of region 6, while the pDLPFC atlas comprised Sallet region 5 and the posterior portion of region 6; region 6 was bisected at the frontal pole-medial-frontal gyrus boundary of the Harvard-Oxford cortical atlas. 32 Thus, our final aDLPFC atlas consisted of Sallet region 7 and the anterior portion of region 6, while the pDLPFC atlas consisted of Sallet region 5 and the posterior portion of region 6. The VMPFC mask used the Harvard-Oxford atlas frontal pole (region 1), after eliminating dorsal segments (ie, the entire Sallet atlas). The (right-sided) Sallet atlas was mirrored about the mid-sagittal plane to construct left-sided regions. The striatal regions were taken directly from the Oxford-GSK-Imanova striatal connectivity atlas 30 (regions 2 and 3 for ventral and dorsal striatum [dStr] respectively). We applied 2-mm Gaussian dilation to extend all regions into the adjacent WM.
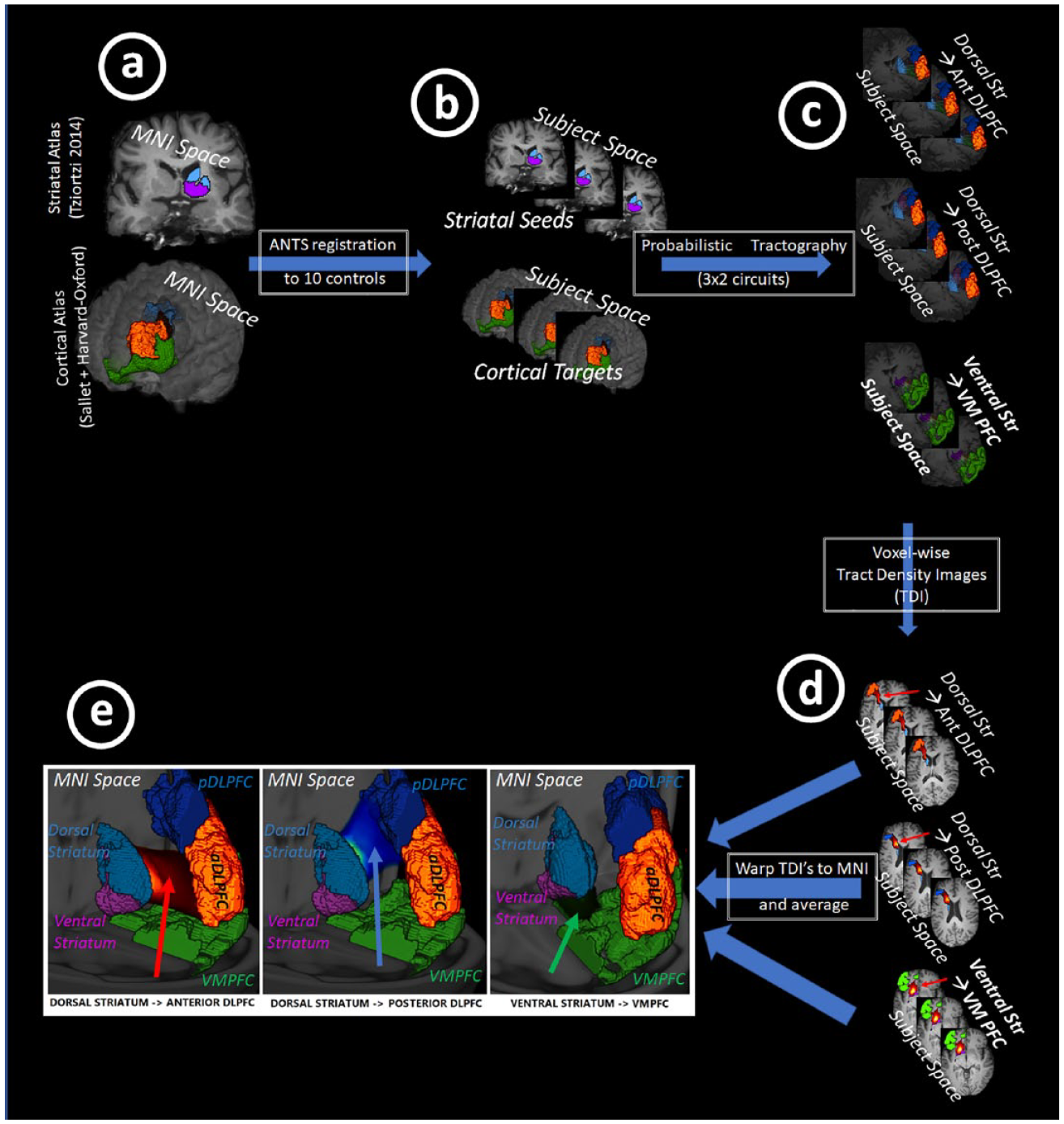
The fronto-striatal atlas construction pipeline, which consisted of: (A) identification of MNI-based striatal seed regions and prefrontal cortical targets, (B) T1-based registration of seeds and targets to 10 control participants, (C) subject-space probabilistic tractography of 3 circuits × 2 (right/left), (D) calculation of voxel-wise, TDIs (ie, per-circuit probability maps), (E) registration of TDI back to MNI space and averaging to obtain MNI-based tract probability maps. Not shown are subsequent steps of (F) registration of MNI-averaged circuits into subject space, for all participants in the study, (G) multiplication by subject FA maps, and (H) extraction of mean per-circuit, per-subject FA values for entry into logistic regression models.
These atlas regions were next registered, via the MNI T1 image, to the T1 images of 10 pseudo-randomly selected control participants, with the only selection criterion being that the mean and standard deviation of the age and sex distribution matched that of the entire study cohort. Prior studies showed this number to be appropriate for tractography-based template generation. 31 Registration used the Anatomical Normalization Tools (ANTs v2.3.1), 33 applied to non-brain-extracted T1-weighted images.
Fiber orientation distribution (FOD) images were processed for these 10 participants through the standard MRtrix pipeline. 34 WM FOD’s were used to generate six circuits (right and left dStr-to-aDLPFC, dStr-to-pDLPFC, and vStr-to-VMPFC). Tractograms were converted to tract density images (TDI), 35 rigid-body transformed to subject T1 space and back into MNI space to allow averaging across subjects. The mean TDI’s thus created were voxel-wise tract probability maps. Atlas maps were confined to WM by masking with an average FA map and minimum FA threshold of 0.2. To determine an appropriate TDI threshold for each circuit, the six mean TDI maps were visualized together; we chose the final threshold empirically to ensure both a continuous striatum to frontal cortex representation and minimal overlap between anterior and posterior DLPFC circuits. The final TDI thresholds correspond to a mean of approximately 7 to 10 streamlines per voxel, in good agreement with prior definitions of streamlines needed for reliable tractography. 36 The final result was a study-specific, six circuit, fronto-striatal atlas (Figure 2).

Illustration of the striatal (light blue/purple) and cortical (blue/orange/green) regions used for fronto-striatal atlas tractography, along with the three resultant fronto-striatal circuit: (A) dStr → aDLPFC circuit (left panel, red arrow), (B) dStr → pDLPFC circuit (middle panel, blue arrow), and (C) vStr → VMPFC circuit (right panel, green arrow).
Circuit-Specific FA Measures
Using the same registration methodology described above, the standard atlas was transformed from MNI space into the T1 space for all participants in the study, followed by rigid body registration into subject FA space. Non-WM voxels were excluded at the subject level by multiplying FA maps with T1-based WM masks from FSL-FAST. 37 Thresholded TDI images were binarized, multiplied with the participant’s FA map, and mean FA values were extracted to obtain subject-wise, circuit-based FA values as input into logistic regression models (see below).
Lesion Load
Total lesion volume was calculated using the lesion segmentation toolbox (LST), 6 which uses both T1 and FLAIR images for identification of WM hypo/hyperintensities. While MS lesions were not expected in control participants, age-related hyperintensities of other origin (eg, small vessel disease) were expected and thus were collected for both study groups. Whole brain lesion volume was included as a predictor in logistic regression models.
We chose to focus on whole brain lesion load as an imaging covariate because this global measure has been used in many prior studies. At the same time, we recognize its lack of spatial specificity compared to our spatially-focused FA metrics of the executive-frontal circuits. Fully adjusted analyses were repeated utilizing tract-specific lesion load measures and are provided as supplemental data (Supplemental Table S1).
Short Physical Performance Battery
SPPB served as the primary outcome of mobility impairment for the study, and includes tests of balance, gait speed, and chair rise, with each portion scored on a scale of 0 to 4 (ie, total score ranging from 0 to 12, with higher scores indicative of better performance). The SPPB takes approximately 5 minutes to complete and is a well-validated measure of physical ability. 3 We dichotomized SPPB score based on an established cutoff score of 10 (ie, scores of 10 and lower are indicative of the presence of mobility impairment).3,38
Covariates
Covariates included: age, sex, education, global health status (GHS), repeatable battery for the assessment of neuropsychological status (RBANS), and patient determined disease steps (PDDS).
GHS: The GHS scale included presence/absence of the following conditions (max score 10): diabetes, chronic heart failure, arthritis, hypertension, depression, stroke, Parkinson’s disease, chronic obstructive lung disease, angina, and myocardial infarction. 26
RBANS: This well-validated battery consists of 12 subtests spanning five cognitive domains: immediate memory, visuospatial/constructional abilities, language, attention, and delayed memory. 39 Herein, the RBANS total index score was used as a proxy for general level of cognitive function.
PDDS: Overall functional disability was measured in the patient group only with the 8-point, self-reported PDDS scale, which has been shown to strongly correlate with the gold standard Expanded Disability Status Scale. 40 PDDS scores range from 0 (no disability) to 8 (bedridden).
Sensitivity Analysis
While the state-of-the-art ANTs package used for nonlinear registration from MNI to subject DTI space has excellent performance, and specifically is the best package for assuring accurate registration even in the presence of anatomical variations such as enlarged cerebral ventricles, this method relies on T1-based registration which cannot account for variations in tract-related anatomy. An alternate method would use both T1 and FA maps for registration. Thus, we performed a sensitivity analysis to explore the effect of registration method on the statistical model results. For these analyses, a combined T1/FA image pair was used to generate a new MNI to DTI space transformation, utilizing the JHU FA map (as provided with FSL) to form a combined MNI-space T1/FA map. The ANTs registration package was again used for this registration, with a 1.0/0.5 relative weighting of the T1/FA images and a small degree of smoothing of the FA maps; both of these steps minimize potential registration bias from altered/pathological FA changes. While this process potentially provides a more accurate registration of the WM tracts, the potential for bias still exists, given that the registration process in this case is itself being guided by the FA outcome measure. We therefore chose to use the standard T1-based registration for our primary analyses, and explore as a sensitivity analyses the effect of the modified registration on the statistical model results.
Statistical Analysis
Continuous demographic, clinical, and imaging measures were compared between the experimental groups using independent t-statistics. Primary models used multivariate logistic regression analysis, stratified by participant group, with the SPPB measure of mobility impairment as a dichotomous outcome (0/1 corresponding to absence/presence of mobility impairment) and mean FA in each fronto-striatal circuit served as predictor to identify the strength of association between predictor and outcome variables. The following models were included, for each participant group: Model 1: unadjusted; Model 2: adjusted for age, sex, education, GHS, lesion load, and cognitive score (RBANS); and Model 3: added PDDS score, within MS patients only. Results are reported as odds ratio (OR), their 95% confidence intervals (CI) and P-values, for FA and all covariates. All measures were standardized prior to analysis, so that ORs indicate the increase in odds of mobility impairment for an increase (or decrease) of one standard deviation in the independent variable (eg, FA). Statistical analyses were performed using Matlab’s statistical software (R2021a, The Mathworks, Natick, MA), and statistical significance was considered for P ≤ .05.
Data Availability
All data used in this manuscript will be provided upon requested by qualified investigators.
Results
Participants
From an initial pool of 105 participants (51 patients) who completed the imaging portion of the study, four control participants were excluded (two because of missing or poor-quality FLAIR images, and two because of poor T1 registration to the MNI template). Thus, the final cohort for the study included 51 older MS patients (mean age = 64.9 ± 3.7 years, 29 females) and 50 healthy older controls (mean age = 66.2 ± 3.2 years, 24 females). As expected, there was a statistically significant difference between the groups on the SPPB physical function measure (P < .001), but importantly, there was no difference between the groups on either the global health scale (P = .18) or cognitive function (RBANS, P = .33). The low GHS scores in both groups suggest relatively overall good health of the sample, and the mean RBANS scores are in line with average cognitive function. Demographic and clinical measures, and statistical comparisons are summarized in Table 1.
Demographic, Clinical, and Brain Imaging Measures.
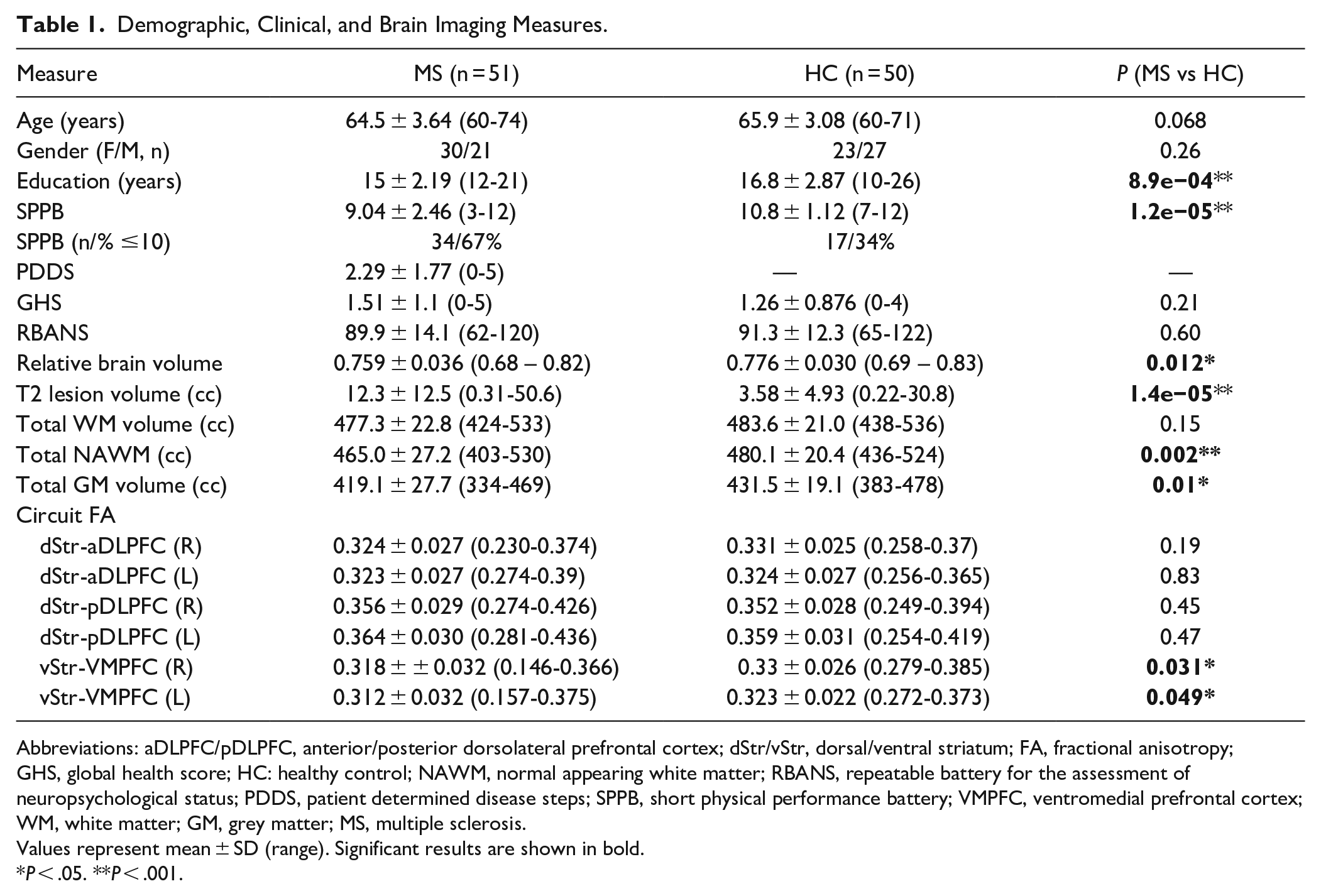
Abbreviations: aDLPFC/pDLPFC, anterior/posterior dorsolateral prefrontal cortex; dStr/vStr, dorsal/ventral striatum; FA, fractional anisotropy; GHS, global health score; HC: healthy control; NAWM, normal appearing white matter; RBANS, repeatable battery for the assessment of neuropsychological status; PDDS, patient determined disease steps; SPPB, short physical performance battery; VMPFC, ventromedial prefrontal cortex; WM, white matter; GM, grey matter; MS, multiple sclerosis.
Values represent mean ± SD (range). Significant results are shown in bold.
P < .05. **P < .001.
Atlas Generation
The atlas generation process delineated well-circumscribed circuits from striatum to frontal cortex (Figure 2). The dorsal circuit volumes were largest, with the anterior circuit slightly larger than the posterior (11.1/11.3 vs. 12.4/12.5 cc, L/R) compared to the ventral circuits (7.4/8.2 cc).
Mean FA Results
Mean FA across all six circuits can be found in Table 1; only the ventral circuits demonstrated group FA differences. Between circuits, there was a statistically significant pattern, with FA increasing progressively from ventral → anterior dorsal → posterior dorsal regions.
Logistic Regression Model Results
The results of all five logistic regression models are shown in Tables 2 through 4.
Unadjusted Logistic Regression Model (Outcome: SPPB).
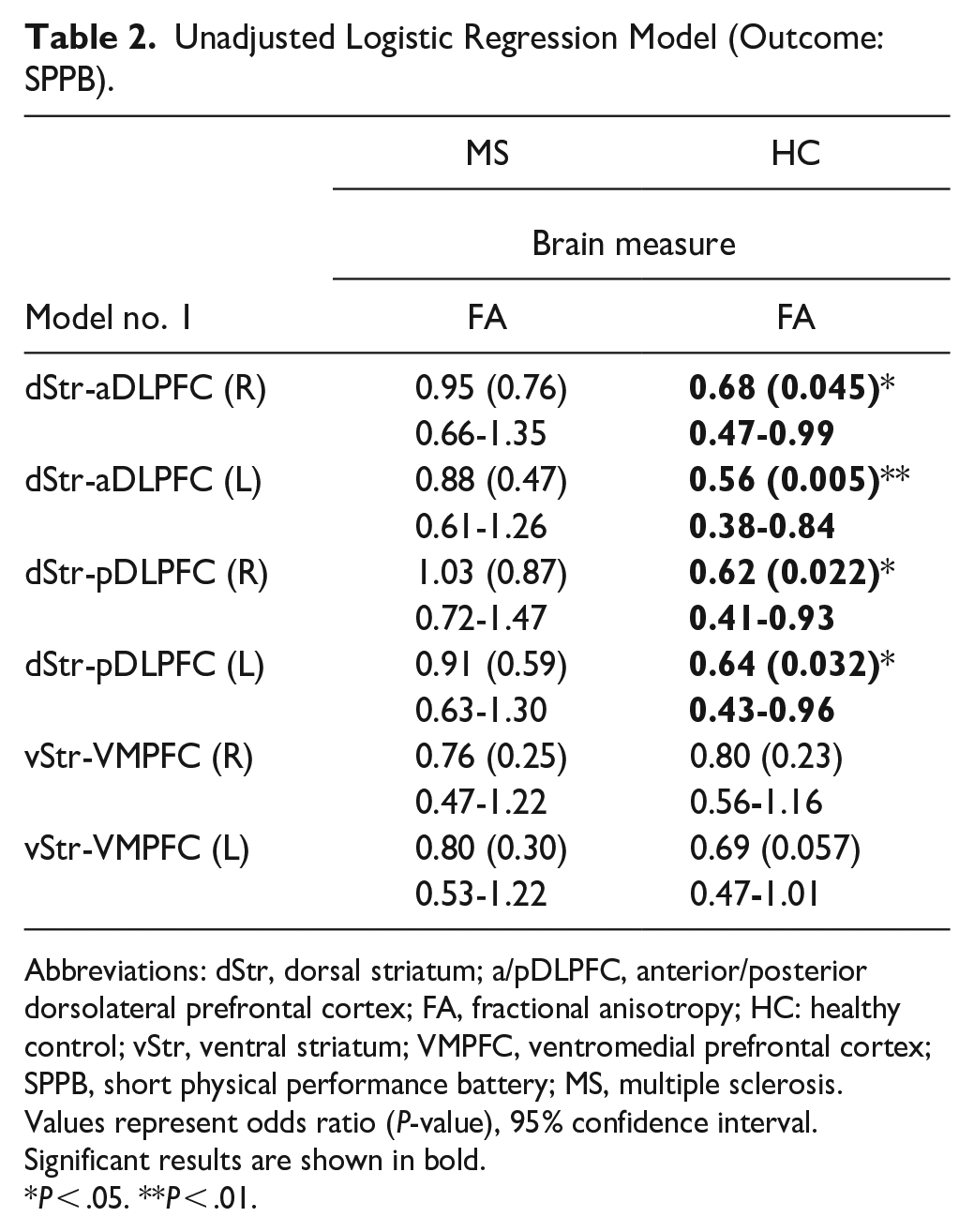
Abbreviations: dStr, dorsal striatum; a/pDLPFC, anterior/posterior dorsolateral prefrontal cortex; FA, fractional anisotropy; HC: healthy control; vStr, ventral striatum; VMPFC, ventromedial prefrontal cortex; SPPB, short physical performance battery; MS, multiple sclerosis.
Values represent odds ratio (P-value), 95% confidence interval. Significant results are shown in bold.
P < .05. **P < .01.
Logistic Regression (Outcome: SPPB), Adjusted for Demographic, Lesion and Cognition Measures.
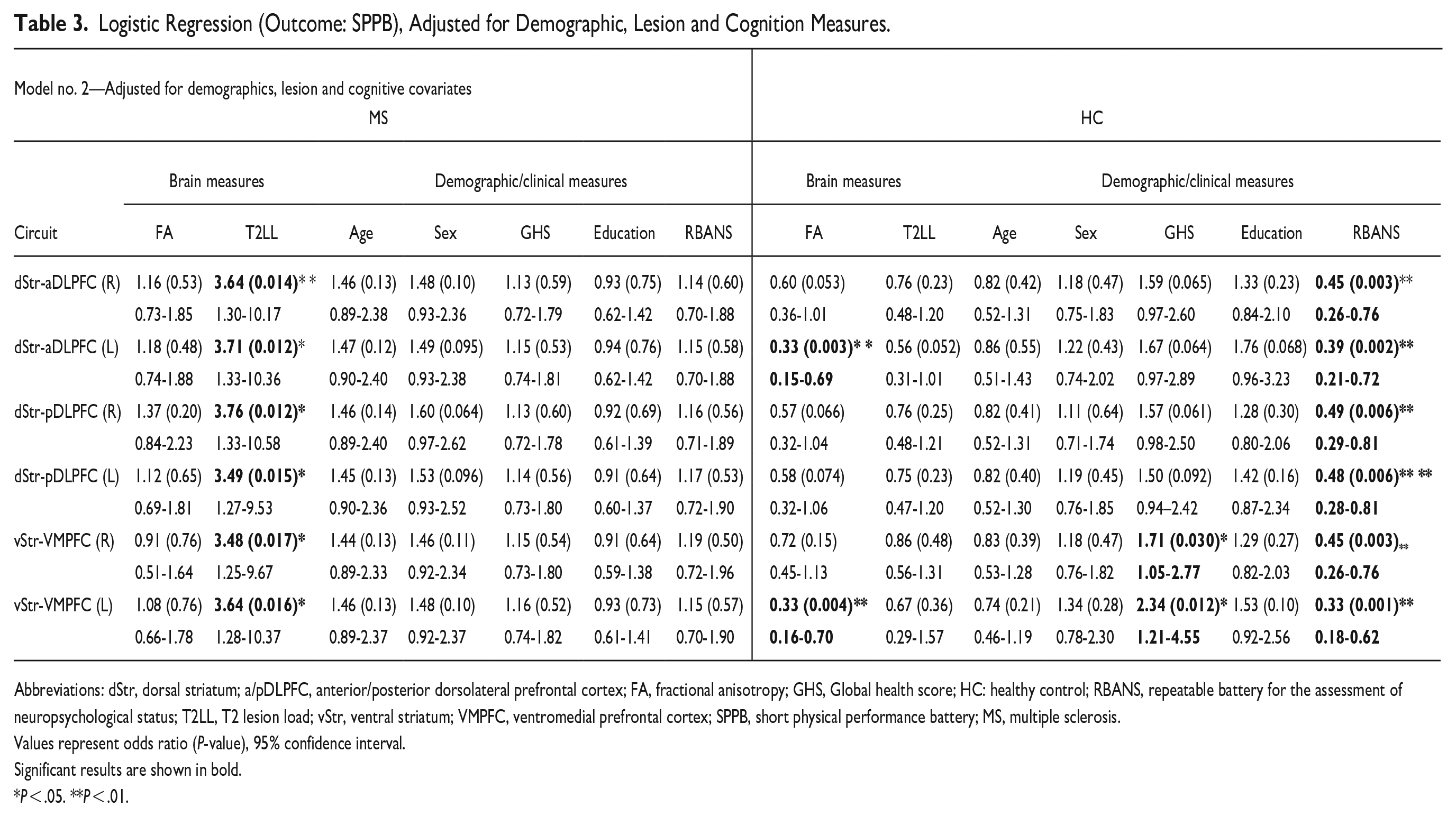
Abbreviations: dStr, dorsal striatum; a/pDLPFC, anterior/posterior dorsolateral prefrontal cortex; FA, fractional anisotropy; GHS, Global health score; HC: healthy control; RBANS, repeatable battery for the assessment of neuropsychological status; T2LL, T2 lesion load; vStr, ventral striatum; VMPFC, ventromedial prefrontal cortex; SPPB, short physical performance battery; MS, multiple sclerosis.
Values represent odds ratio (P-value), 95% confidence interval.
Significant results are shown in bold.
P < .05. **P < .01.
Logistic Regression Model (Outcome: SPPB) in MS Patients Only, Adjusted for Demographic and Lesion Measures, Cognition and Patient Reported Ambulatory Function (PDDS) Scores.
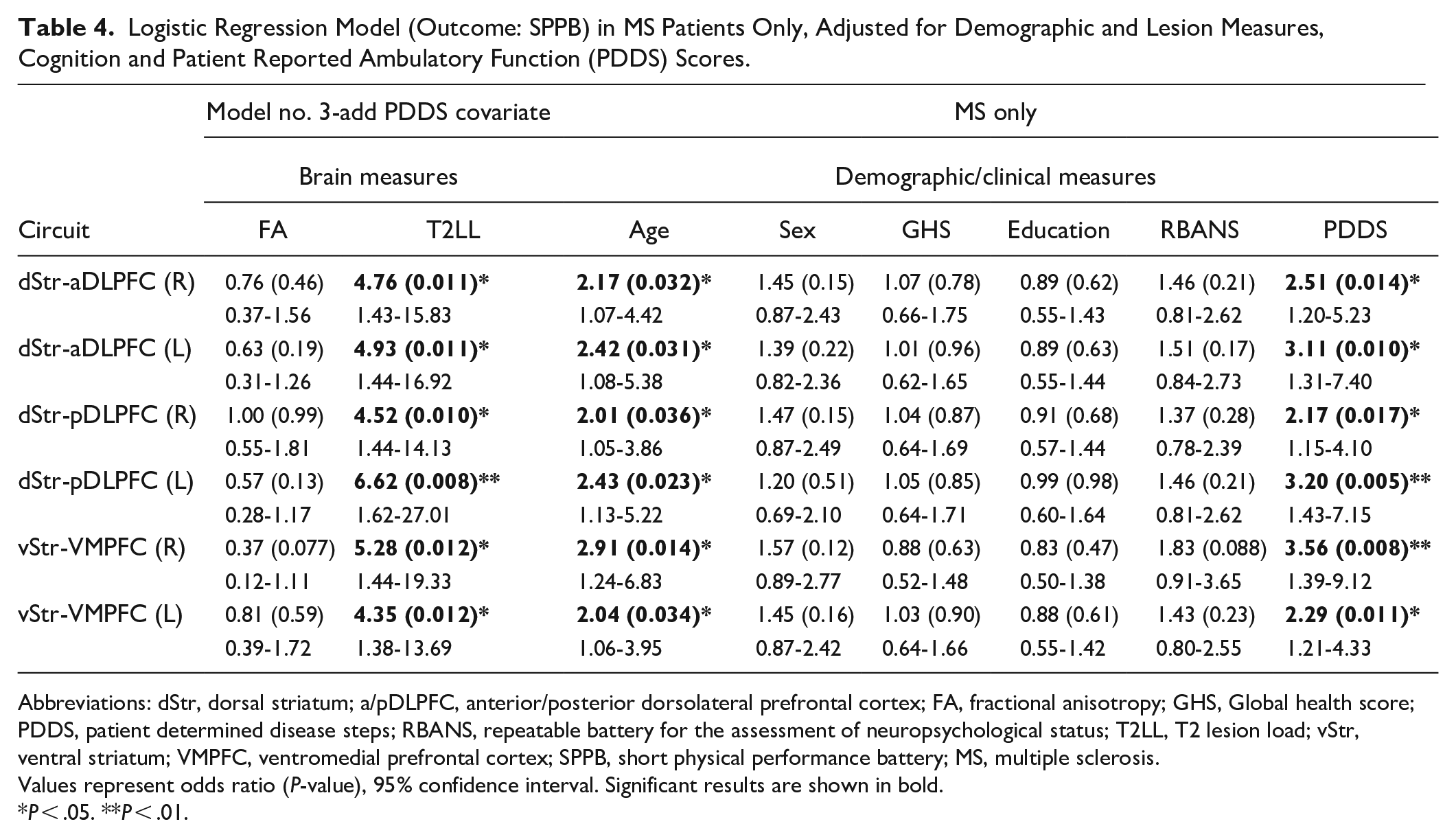
Abbreviations: dStr, dorsal striatum; a/pDLPFC, anterior/posterior dorsolateral prefrontal cortex; FA, fractional anisotropy; GHS, Global health score; PDDS, patient determined disease steps; RBANS, repeatable battery for the assessment of neuropsychological status; T2LL, T2 lesion load; vStr, ventral striatum; VMPFC, ventromedial prefrontal cortex; SPPB, short physical performance battery; MS, multiple sclerosis.
Values represent odds ratio (P-value), 95% confidence interval. Significant results are shown in bold.
P < .05. **P < .01.
MS cohort: There were no significant effects of FA on SPPB outcome in any of the circuits (Table 3: OR = 0.76-1.38, P ≥ .20), whether or not adjusting for covariates. In contrast, the regression models demonstrated a significant association of higher lesion burden and higher PDDS disability scores with higher odds of SPPB impairment (Table 3: Lesion OR = 3.02-3.76, P < .02; Table 4: PDDS OR = 2.17-3.56, P < .02).
Control cohort: By comparison, there were significant FA effects in a few of the circuits, all corresponding to lower FA with higher odds of SPPB-measured impairment (ie, ORs < 1). The unadjusted model identified significant effects in all four DLPFC circuits (Table 2: L-aDLPFC: OR = 0.68, P = .045, R-aDLPFC: OR = 0.56, P = .005, L-pDLPFC: OR = 0.62, P = .022, R-pDLPFC: OR = 0.64, P = .032), with a statistical trend in the left VMPFC circuits (OR = 0.69, P = .057). After adjusting for demographic, lesion load and cognitive covariates, the only circuits demonstrating a significant association were left anterior DLPFC (Table 3: OR = 0.33, P = .003) and left VMPFC (Table 3: OR = 0.33, P = .004); associations in the remaining DLPFC circuits were diminished to the trend level. Lesion burden, in contrast to the patients, was not significant in the models, even though the distribution of lesion burden included some participants with marked lesion levels. Finally, better RBANS cognitive scores across all six tests was associated with lower SPPB-measured impairment odds (Table 3: OR = 0.33-0.49, P < .01).
Logistic Regression Models With Tract-Specific Lesion Load
In controls, results were unchanged, with two left-sided circuits demonstrating significant associations of dichotomized SPPB with circuit FA, and no associations with lesion load. In MS patients, circuit FA relationships remained non-significant, while associations between SPPB and local lesion load were mostly no longer significant (Supplemental Table S1).
Sensitivity Analyses
The alternate registration process resulted in statistically significant changes in tract-based mean FA values across the entire cohort (1-2% increase); there were, however, no differences in these changes between the two groups and there were no changes in the results of the statistical models examining associations of tract-specific FA and SPPB (Supplemental Table S2).
Discussion
The goal of this study was to compare and contrast the distinct roles of three fronto-striatal executive circuits and WM lesion load in mobility function in older adults with and without MS. Our hypothesis, that there was a relationship between higher WM integrity and lower odds of mobility impairment, was only confirmed in healthy controls. We also found an intriguing double dissociation between the aforementioned measures of brain integrity/pathology and the presence of mobility impairment as a function of group status. Specifically, among PWMS, higher, whole-brain lesion burden, but not lower fronto-striatal FA, was associated with higher odds of having mobility impairment. In contrast, among healthy older adults, lower FA in executive fronto-striatal circuits, but not higher lesion burden, was indicative of the presence of mobility impairment.
We thus provide compelling evidence for the role of the executive fronto-striatal circuitry in mobility for healthy older adults, adding to previous findings on the role of higher order cognitive control of locomotion in healthy aging. 21 Our control cohort data (model #3) provide further evidence for the non-overlapping roles of fronto-striatal WM integrity and global cognition in supporting mobility performance. Among PWMS, however, brain control of mobility appears to be affected primarily by whole brain WM lesion volume, even after controlling for cognition and demographic differences. This divergent pattern of findings suggests that in contrast to a more nuanced and tract-specific executive control of mobility in normal aging, a global measure of brain pathology mediated by disease plays a key role in mobility function in older PWMS. In concert with the concept of dedifferentiation of brain function in older adults, 24 our results may indicate a synergy of aging and disease (ie, MS) leading to the effect of global rather than local brain changes as the driving factors of brain control of mobility. This notion is further supported by our supplemental analyses, revealing that WM lesions in fronto-striatal tracts were also not related to mobility impairment in PWMS (with the exception of the right ventral circuit which also demonstrated reduced FA in PWMS compared to healthy controls, indicating some degree of coupling between FA and lesion load).
Major successes of disease-modifying therapies in MS in the last decade have pushed the importance of understanding the impact of MS on older patients to the forefront. Even in the absence of MS pathology, mobility impairment is a common concern in older adults. 21 Furthermore, extensive work over the last 10 to 15 years have established the importance of cognitive function in the control of gait 41 as well as its role in gait impairment both in the presence of pathology42 -44 and in healthy aging.21,45 The fronto-striatal brain system is a key component of cognitive control of walking, 46 thus motivating our focus on DTI measures of fronto-striatal WM integrity and its relationship to gait function in older MS patients. Thus, there is good support for the importance of the fronto-striatal circuitry in gait function in older adults; our results are in line with these findings in healthy older adults, that is, our control cohort. Our work further builds on this knowledge by showing the dissociation of the dependence of physical function outcomes on fronto-striatal integrity in older PWMS, with this dependence being subsumed by WM lesions.
The fronto-striatal tracts delineated in our work can be divided into two broad categories: dStr-to-dorsolateral prefrontal cortex, associated primarily with executive motor control and vStr-to-VMPFC, associated primarily with decision making and emotional processing and regulation. 47 The relationship of the dorsal circuitry with executive motor function in healthy controls supports our finding of the association of physical functional outcome (ie, SPPB) and dorsal circuit integrity; these findings spanned both left and right circuits and connections to both anterior and posterior DLPFC, although only the left anterior circuit survived after adjusting for all covariates. Prior literature has shown hemispheric differentiation in the DLPFC, with left lateralized activation related to gait function in older adults. 48 Similarly, prior studies concerning the influence of negative affect on gait performance provide good support for the associations found in the left ventral circuit; 49 it is specifically the left vStr which projects to orbito/VMPFC, while right vStr projects primarily to uncus, insula and parahippocampal areas. 50
DTI has been used extensively to investigate WM changes in MS. These studies however have mainly been in the context of differentiating disease subtypes, 51 overall disability, 52 early detection (eg, clinically isolated syndrome) 53 or its relationship to cognition. 54 And while gait impairments are a very prevalent feature of the MS symptomatology, very little work has been focused on the relationship of DTI findings in MS and gait.55,56 Common assessments in MS include the EDSS and the MS Functional Composite (MSFC), which contain gait-related measures (eg, ataxia as part of the EDSS, and timed 25-foot walk of the MSFC). However, these are one small component of a larger functional assessment, so that the contribution of gait impairments to these functional outcomes and their relationship to DTI measures remain mostly unknown. Our work thus provides novel information to brain substrates of mobility impairment in older adults with and without MS.
We created a study-specific atlas of the fronto-striatal circuitry, based on striatal-to-prefrontal tractograms from 10 older healthy controls enrolled in the study. This is different from most prior studies in this field using region-of-interest (ROI), whole-brain (eg, voxel-based morphometry, VBM) 57 or tract-based methods (eg, tract-based spatial statistics, TBSS). 58 Each has unique advantages and disadvantages. ROI-based measurements maximize statistical power by limiting the regions tested, while VBM allows brain-wide conclusions to be drawn but require corrections for multiple comparisons across hundreds of thousands of voxels. TBSS lies somewhere in between but limits anatomical specificity by collapsing nearby tract information into a summary metric. 59 Given our focus on very specific and functionally unique segments of the striatal-to-frontal system, we adopted an ROI-based approach, but with tractography-based, study-specific definitions of the fronto-striatal regions-of-interest.
Strength, Limitations, and General Conclusions
This study evaluated executive fronto-striatal circuit WM changes in older MS patients and their relationship to mobility function. The use of the SPPB as the primary outcome measure was a particular strength of the study, in that it allowed us to identify changes in WM integrity related specifically to objectively defined mobility impairment, a much-understudied outcome in the MS imaging literature. We employed an hypothesis-driven, ROI-based approach to define the fronto-striatal circuits of interest. Overall, we identified two specific components of the fronto-striatal network implicated in influence of WM integrity on mobility function. We chose to focus on FA as the measure of WM integrity, while many other DTI-based metrics were available. FA provides a summary measure of WM integrity but lacks specificity to any particular underlying neuropathological process. Future work should examine more specific measures of WM integrity and their association with physical function in older adults with and without MS. The LST is one of many segmentation tools; machine learning algorithms have better performance but are not as readily available. All segmentations were carefully reviewed, and while we noted a slight underestimation in lesion volumes, in line with a recent comparison study, 60 there was no bias which would differentially affect the study groups. Utilizing an alternative registration method (Table S2) provided further confidence that the reported associations of FA in fronto-striatal tracts and mobility were robust. While the SPPB is a continuous measure, the distribution of scores were not normal, precluding linear regression. Moreover, we used an established and clinically validated cutoff score3,38 with sufficient numbers of mobility-impairment cases in each group, and the clinical context that aids interpretation of the findings. Patients with severe impairment were precluded by the parent study inclusion criteria and hence generalization of our findings to those with more severe impairment should be examined in future research. Finally, we did not have sufficient power to investigate differentiation of the WM integrity relationships with mobility impairment by MS subtype or SPPB subscores, and sample size can be a concern in imaging-based studies; all of these issues should be investigated in larger, follow-up studies.
In conclusion, we show compelling evidence for a double dissociation between two common measures of brain integrity/pathology and the presence of mobility impairment as a function of group status, in older persons with and without MS. Our data provide strong support of prior literature on the importance of the fronto-striatal system and the role of cognitive function toward mobility function and impairment in older persons. Finally, we present these data in the context of novel methodology for examining the structural integrity of the fronto-striatal system, which can be extended to the investigation of other measures of brain tissue integrity and its relationship to clinical outcomes.
Supplemental Material
sj-docx-1-nnr-10.1177_15459683231164787 – Supplemental material for Differential Associations of Mobility With Fronto-Striatal Integrity and Lesion Load in Older Adults With and Without Multiple Sclerosis
Supplemental material, sj-docx-1-nnr-10.1177_15459683231164787 for Differential Associations of Mobility With Fronto-Striatal Integrity and Lesion Load in Older Adults With and Without Multiple Sclerosis by Mark E. Wagshul, Frederick W. Foley, Kapil Chaudhary, Michael L. Lipton, Robert W. Motl, Meltem Izzetoglu, Manuel E. Hernandez, Mary Ann Picone and Roee Holtzer in Neurorehabilitation and Neural Repair
Supplemental Material
sj-docx-2-nnr-10.1177_15459683231164787 – Supplemental material for Differential Associations of Mobility With Fronto-Striatal Integrity and Lesion Load in Older Adults With and Without Multiple Sclerosis
Supplemental material, sj-docx-2-nnr-10.1177_15459683231164787 for Differential Associations of Mobility With Fronto-Striatal Integrity and Lesion Load in Older Adults With and Without Multiple Sclerosis by Mark E. Wagshul, Frederick W. Foley, Kapil Chaudhary, Michael L. Lipton, Robert W. Motl, Meltem Izzetoglu, Manuel E. Hernandez, Mary Ann Picone and Roee Holtzer in Neurorehabilitation and Neural Repair
Footnotes
Classification of Evidence
This study provides Class III evidence that different measures of white matter integrity are predictive of mobility impairment in older persons with and without MS, respectively, with white matter lesion load providing predictive power in MS patients, and DTI-based white matter integrity providing predictive power in healthy older individuals.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a National Institute of Neurological Disorders and Stroke grant (R01NS109023); the funding agency played no role in any aspect of the work described.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.