
Abstract
Introduction
Multimodal agility-based exercise training (MAT) has been described as a framework for fall prevention in the elderly but might also be a valuable concept for exercise training in persons with Multiple Sclerosis (pwMS).
The Problem
Current recommendations advise pwMS to perform a multitude of different exercise training activities, as each of these has its separate evidence. However, pwMS struggle even more than the general population to be physically active. Additionally, Multiple Sclerosis often leads to co-occurring mobility and cognitive dysfunctions, for which simultaneous, time-efficient, and engaging training approaches are still limited in clinical practice and healthcare.
The solution
The MAT framework has been developed to integratively improve cardiovascular, neuromuscular, and cognitive function by combining aspects of perception and orientation, change of direction, as well as stop-and-go patterns (ie, agility), in a group-training format. For pwMS, the MAT framework is conceptualized to include 3 Components: standing balance, dynamic balance (including functional leg strength), and agility-based exercises. Within these Components sensory, cognitive, and cardiovascular challenges can be adapted to individual needs.
Recommendations
We recommend investigating multimodal exercise interventions that go beyond easily standardized, unimodal types of exercise (eg, aerobic or resistance exercise), which could allow for time-efficient training, targeting multiple frequent symptoms of persons with mild disability at once. MAT should be compared to unimodal approaches, regarding sensor-based gait outcomes, fatigue-related outcomes, cognition, as well as neuroprotective, and (supportive) disease-modifying effects.
Introduction
Multimodal agility-based exercise training (MAT) refers to a framework aimed at integratively improving cardiovascular, neuromuscular, and cognitive function in a group-training format. “Agility-based” describes tasks, that require changes of direction, stop-and-go patterns, turns, and changing footwork strategies, with or without responding to a stimulus. The framework was first described by Donath et al 1 in the context of exercise-based fall prevention in the elderly. However, as discussed in this paper, several aspects make it valuable as a framework for exercise-based neurorehabilitation for persons with Multiple Sclerosis (pwMS).
Multiple Sclerosis (MS) is the most common, non-traumatic, neurological disorder among middle aged adults. Initially characterized as an inflammatory demyelinating disease of the central nervous system, neurodegenerative processes lead to progressive disability during later disease stages. 2 Importantly, the resulting lesions in the central nervous system often lead to co-occurring mobility and cognitive dysfunctions. 3
Even though disease onset is most common in early adult life, pwMS fall more than older adults without MS.2,4 Over 50% of pwMS fall once within 3 months, with falls occurring soon after disease onset and later increasing in frequency. Developing fear of falling can lead to decreased social participation and problems in the work environment, considering that many pwMS are in a working age.
Preceding falls, disease processes in MS lead to gait and balance deficits, along with muscle weakness, spasticity, impaired sensation, vestibular function, oculomotor, and visual impairments. This can also lead to limited walking distance, further aggravated by motor fatigability. 5
However, there is also a high number of pwMS with only mild disability, demonstrating only subtle gait and balance deficits. According to the Reserve framework, 6 the best treatment for MS might be prevention of functional and structural decline. Aging plays a major role in a declining reserve and the development of a secondary progressive disease course, which entails marked increases in functional disability. 7 Thus, as described by others for drug treatments 7 and exercise, 8 actions should be taken early, that is, in patients that are typically younger, and with only mild functional disability. This “open window of opportunity” might be especially sensitive for the MAT framework that is discussed in this paper. As argued below, the MAT framework could provide multi-sensory challenges (eg, agility-like exercises, sensory, and cognitive challenges), resulting in central nervous system adaptations, that go beyond those elicited by “unimodal” approaches or traditional recommendations. Improving gait and balance as well as reestablishing high-level mobility functions (eg, running, jumping, agility-like functions) 9 could be regarded as the most proximal targets of MAT for pwMS, whereas improvement of central nervous system reserve would be the distal target.
By providing this conceptual basis of MAT for rehabilitation therapists working with pwMS, we want to facilitate the uptake of integrative exercise programs in clinical practice.
Problem
Prevalence of Subtle Gait and Balance Impairments in MS
Prevalence of gait and balance impairments in pwMS is high. 10 Gait impairments can be quantified via spatiotemporal gait characteristics (eg, gait speed, step length, cadence, stance phase etc.) measured using instrumented walkways, wireless inertial sensors, or 3D motion capture. A recent systematic review reported a positive linear relationship between spatiotemporal gait characteristics and disability (measured using the Expanded Disability Status Scale [EDSS]), as expected. 11 For example, according to the meta-regression, increasing from 2.0 to 3.0 on the 0 to 10 EDSS results in a reduction in comfortable or self-selected gait speed from 1.17 m/s (4.22 km/h) to 1.06 m/s (3.8 km/h). The meta-analysis also showed that being classified as a “faller” was significantly associated with slower gait speed. The authors further reported that individuals with low levels of disability had spatiotemporal gait characteristics very similar to the general population when walking in their comfortable gait speed. However, when instructed to walk as fast as possible for 6 minutes, persons with low EDSS (1.5-2.0) differed significantly from healthy controls in their mean gait speed, stride length, and stance phase time. 12 The use of technology has substantiated other subtle gait impairments. When looking at gait kinematics, pwMS with very mild disability (EDSS = 0.0-2.5) walk with less hip extension at toe-off and more hip flexion during swing than healthy controls. 13 Electromyography has also shown a decrease in gastrocnemius activity during walking over a 1-year period in pwMS with EDSS ≤ 3.0. 14 Taken together, technology-based measures have shown ample evidence of subtle gait impairments in persons with mild disability, which are not well quantified in routinely applied clinical tests. 15
Similarly, several studies have detected subtle balance impairments using different devices, which are often neglected in clinical assessments, such as the EDSS. 16 For example, static posturography performed using a force plate showed significant differences between healthy controls and pwMS with EDSS 2.0 to 2.5 as well as EDSS 0.0 to 1.5 (which would be rated as no clinical disability with or without minimal signs of the disease). 17 Importantly, clinical assessments using more challenging tasks than conventional tests seem to better determine balance impairments in persons with low disability. In persons with a median EDSS of 1.0 dynamic balance during tandem walking on balance boards was worse compared to healthy controls. 18
Several authors have also noted the influence of balance on gait performance.4,11,13,18 Recently, Carpinella et al 19 showed that sensor-based outcomes recorded while walking with horizontal head turns (a task particularly challenging to maintain balance during walking) discriminated between healthy controls and “normal walking” pwMS (EDSS ≤ 2.5). This again draws a picture of subtle balance impairments in persons with low disability that can be “unmasked” by technology or more challenging tasks. 20
There also is considerable evidence that cognition plays a primary role in balance, gait, and falls. A well described phenomenon is cognitive-motor interference, where a cognitive and a motor task interfere with each other when performed simultaneously. 21 Similarly, these types of dual-tasks have been reported to uncover deficits in balance via increased challenge in persons with clinically minimal balance and cognitive deficits. 21
However, a recent study on cognitive-motor interference during gait did not find a dual-task condition (eg, subtracting sevens while stepping over obstacles) that was able to discriminate between healthy controls and pwMS, even though pwMS reported having more problems in dual-task situations in daily life. 22 Reasons for this might have been the relatively short task duration of 60 seconds, potentially reducing the effects of fatigue, a small sample size, or type and difficulty of cognitive tasks.
Cognitive functions also play an important role in the construct of walking adaptability, which is necessary, when the complexity of the task exceeds the demands of basic stepping, such as uneven terrain, obstacles, turning, or negotiating a narrow path. 23 It also includes cognitive-motor dual-tasking while walking (eg, having a conversation while walking, scanning for an object while walking through a grocery store), but also motor-motor dual-tasking (eg, walking while throwing and catching). The concept of walking adaptability might comprise more aspects of real-life situations (including ambient demands, physical load, and time constrains) than highly standardized tasks mostly performed in MS trials on dual-task costs (of course, the downside of heightened ecological validity can be compromised reliability of assessments 23 ). Unfortunately, the concept has been largely restricted to stroke research, so there is no data on differences in walking adaptability between healthy controls and pwMS.
As observable in this section, studies have applied different ranges of EDSS, when evaluating persons with “mild” disability. Currently, there is no clear definition of what constitutes mild disability in terms of EDSS, and the reported studies might have included persons with very different levels of “high-level mobility” (ie, mobility more advanced than independent level walking, such as running and jumping). 9 However, all ranges reported here have in common, that patients do not need an assistive device to ambulate and are mostly able to work full time.
Current Recommendations for Exercise Training in pwMS
Currently, authoritative recommendations for exercise training in pwMS with mild impairments (classified here as EDSS 0.0-4.5) include aerobic, resistance, flexibility (not discussed here), and neuromotor exercise. 24 In the following, we will determine aspects of these recommendations and current clinical practice that might benefit from a MAT framework.
First, some aspects could be improved with the integration of sensory (ie, visual, somatosensory, vestibular), and cognitive challenges. Aerobic exercise has been increasingly studied as a form of disease-modifying therapy for pwMS, investigating outcomes such as annual relapse rate, or global brain atrophy, with the treatment ingredient of interest being cardiovascular challenge. 25 However, these types of studies have often relied on stationary ergometer exercise, even in pwMS with mild disability, potentially providing low challenge to the sensory and cognitive system. 3 Greater specificity to mobility tasks, with a simultaneous cardiovascular stimulus could yield added benefits, even though this might challenge standardization in interventional trials. 26
Regarding resistance exercise, we advocate targeting modes, positions, and muscles that are “functional” for gait, challenge balance, and do not solely focus on improving force production as noted by Mañago et al. 27 This, again, could mean reducing the amount of seated exercises (primarily in weight training machines) as their review showed that out of the 6 resistance exercise studies that improved gait, 4 implemented exercises in a standing position, and 2 used modes other than machines. The question of exactly how increased strength acquired from resistance training can be incorporated to gait kinetics seems to be very important. 28
Besides this potential for increasing sensory challenge, there might be an equivalent potential for including cognitive challenges as stated before.3,29
Neuromotor training is a third type of exercise recommended for pwMS, specifically targeting fall prevention, postural stability, coordination, and, importantly in the present context, agility. 24 Referred modalities include a diverse range of pilates, dance, yoga, Tai chi, hippotherapy, virtual reality, and balance and motor control training. Even though there have been beneficial results on gait and balance improvement in these separate modalities, the range of modalities is so diverse, that it is hard to identify which treatment ingredients are specifically responsible for these improvements (eg, do pilates and virtual reality training decrease falls and improve postural stability via a common pathway?; what kind of ingredients are essential in a given pilates session to be successful?). 30 Studies on the modality of balance and motor control training have provided detailed treatment manuals and the challenges provided to pwMS can be regarded as quite specific.26,31,32 However, the extent to which studies also included cognitive challenges differed. Even though agility has been named as a target for neuromotor training it has to be noted that studies on agility in pwMS are basically non-existent (a PubMed search with the search string “agility AND multiple sclerosis” performed in March 2022 retrieved only 6 hits). It is unclear what concept of agility is studied in the MS literature. As described in more detail in the later sections, we do not think that current trials on neuromotor training adequately target agility, as these trials do not specifically include start-stop, acceleration, and deceleration, turns etc., or responding to a stimulus. This is also the case for the core exercises of a recent complex multicomponent fall-prevention intervention that has been systematically developed and includes many of the other aspects already mentioned, but lacks any kind of agility exercises. 33 Interestingly, this high diversity of modalities in the neuromotor training section is similar to the gerontology literature. Nonetheless, within the field of gerontology, the agility framework has provided some common ground for a meta-analysis. 34 Thus, a framework for pwMS could provide some commonality as well.
Lastly, the most substantial benefits of a multimodal framework might lie in the lack of time-efficiency of current exercise recommendation for pwMS. The recommendations include 3 to 6 sessions of neuromotor, 2 to 3 aerobic, daily flexibility, and 2 to 3 resistance exercise sessions per week. Comparable to recommendations for older adults it seems time-consuming for pwMS to follow all these separate recommendations.1,34 Especially, when considering the evidence for even lower physical activity in pwMS than in the general population, and the efforts being undertaken to get pwMS moving at all. 35
There have been some interventions applying a combination of exercise approaches in pwMS. 36 However, components are often still split to different sessions or parts (ie, sessions target 1 component at each time). Studies mostly focus on the “classic” components of exercise training (eg, endurance, strength, balance). Aspects such as agility or the incorporation of cognitive challenges have been studied less frequently.
Taken together, there is evidence of subtle gait, and balance impairment in pwMS with clinically mild disability, but exercise interventions frequently lack sensory and cognitive challenge even though the impairment of central sensory integration has been described several times.3,13,37 Agility has not been studied as a relevant component of fall-prevention in pwMS and is seldomly included in exercise intervention studies. A framework for time-efficient exercise training is lacking.
Solution
What is MAT for pwMS?
The MAT framework has been developed by Donath et al 1 to combine aspects of perception and orientation, change of direction and stop-and-go patterns (ie, agility), including reactive muscle work, with cardiovascular stimuli while at the same time adapting intensity, complexity, and cognitive challenge to individual needs in a group-training format. 34 As such, it could provide a valuable framework for multimodal exercise training in pwMS aiming to improve gait, balance, endurance, and strength. As many pwMS also exhibit problems with processing speed or attention and MAT also includes cognitive challenges, it could further provide a practical framework for combined motor and cognitive rehabilitation in pwMS. 29 This could lead to downstream positive effects on subjective fatigue via reduced effort perception. A recent network-level meta-analysis reported that balance exercises had the largest effect on fatigue compared to usual care among all other types of exercise and behavioral interventions. 38 Another recent study on vestibular function in pwMS postulated that correlations between posturography measures and processing speed might represent a shared utilization of central sensory processing by balance and cognitive pathways. 37
In MAT for pwMS, agility-based exercises are 1 Component of 3: (I) standing balance, (II) dynamic balance (including functional leg strength), (III) agility-based exercises (see Figure 1 and Table 1). Components can be targeted in different modules, that describe the basic setting of a drill. Each drill can then be progressed via the complexity of the drill itself and via specific sensory (visual, somatosensory, vestibular) and cognitive (dual-tasks related to memory, attention, etc.) modifications. Whereas cognitive modifications target cognitive-motor dual-tasking, motor-motor dual-tasking is included in the progressions on task complexity. In every module, various options for progression exist by combining different aspects of complexity, sensory, or cognitive modifications. Components I and II mainly include content similar to other balance and motor control training studies,26,32 whereas Component III is based on agility. As there have been reports on difficulties in replicating rehabilitation interventions, and translating research to clinical practice, besides describing theoretical aspects of the 3 Components, example Modules will be described for each Component (see Tables 2–4).30,39
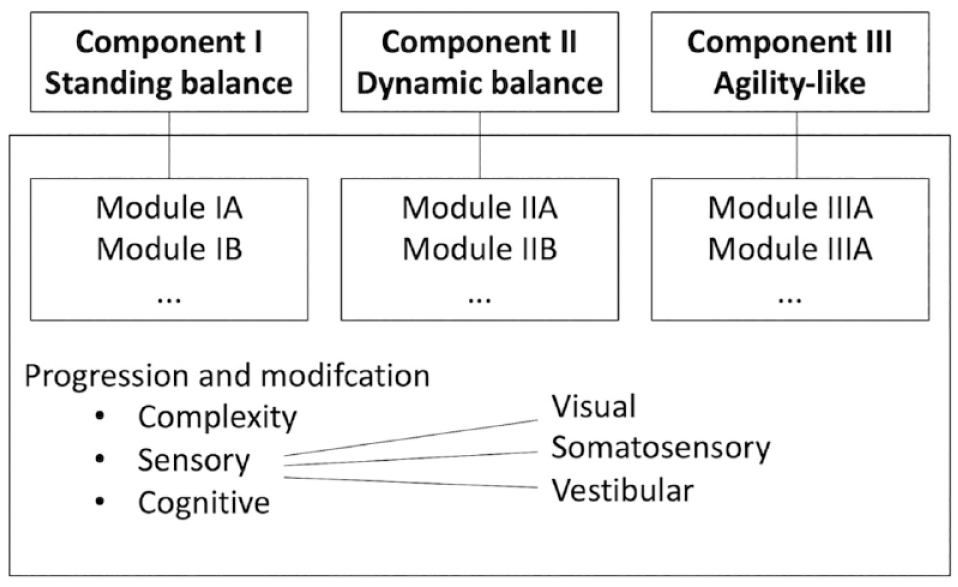
Structure of the MAT framework for pwMS.
Definitions.

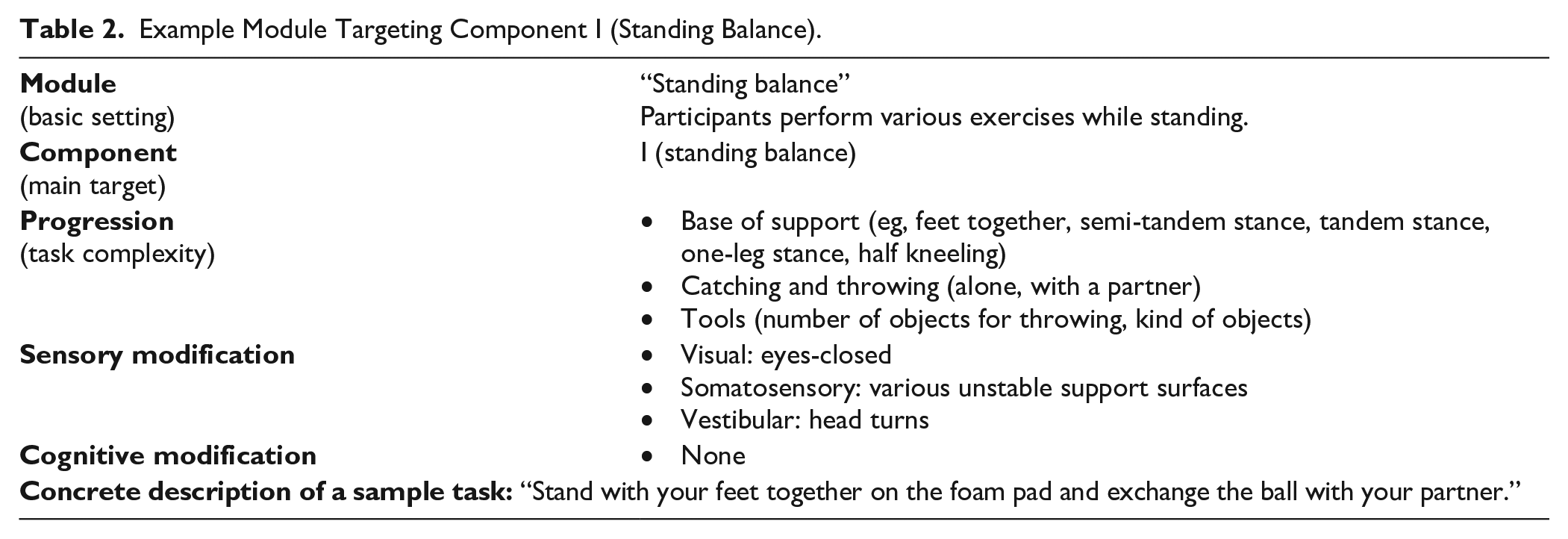
Example Module Targeting Component I (Standing Balance).
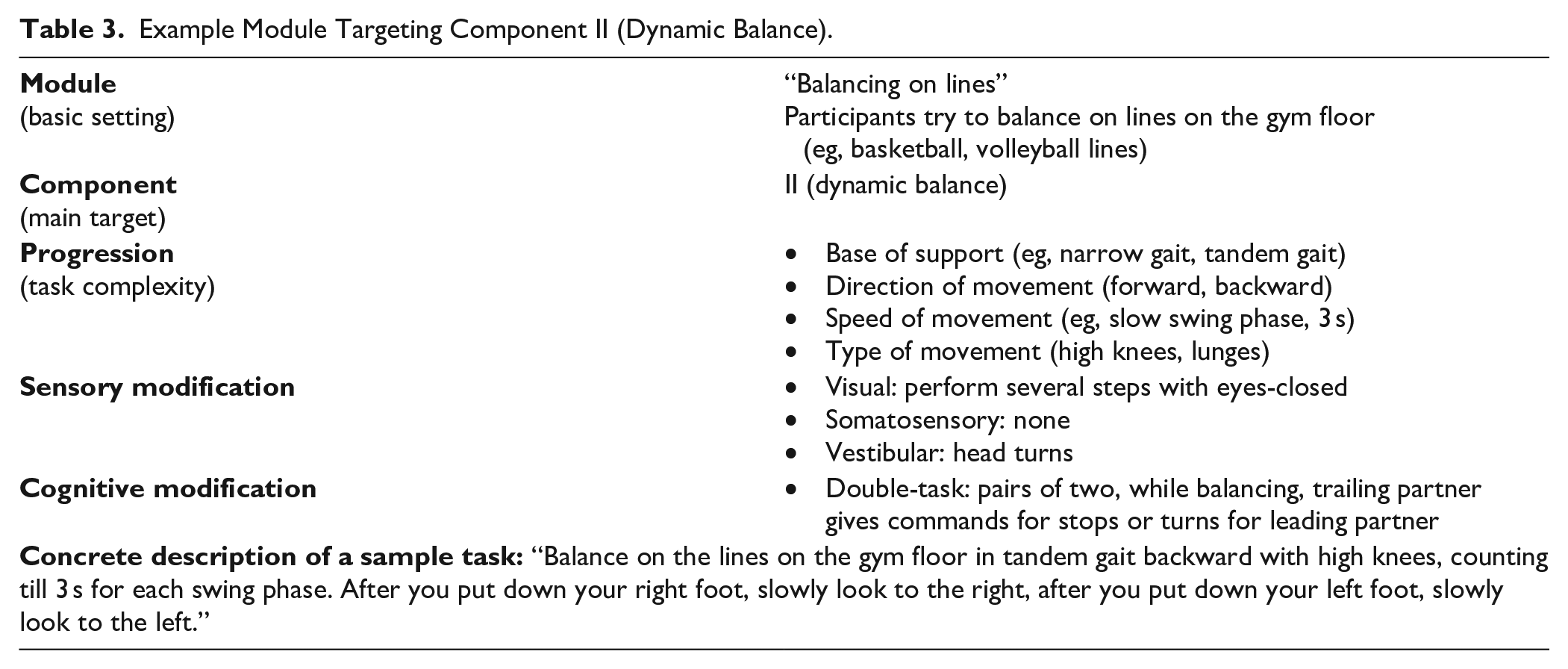
Example Module Targeting Component II (Dynamic Balance).
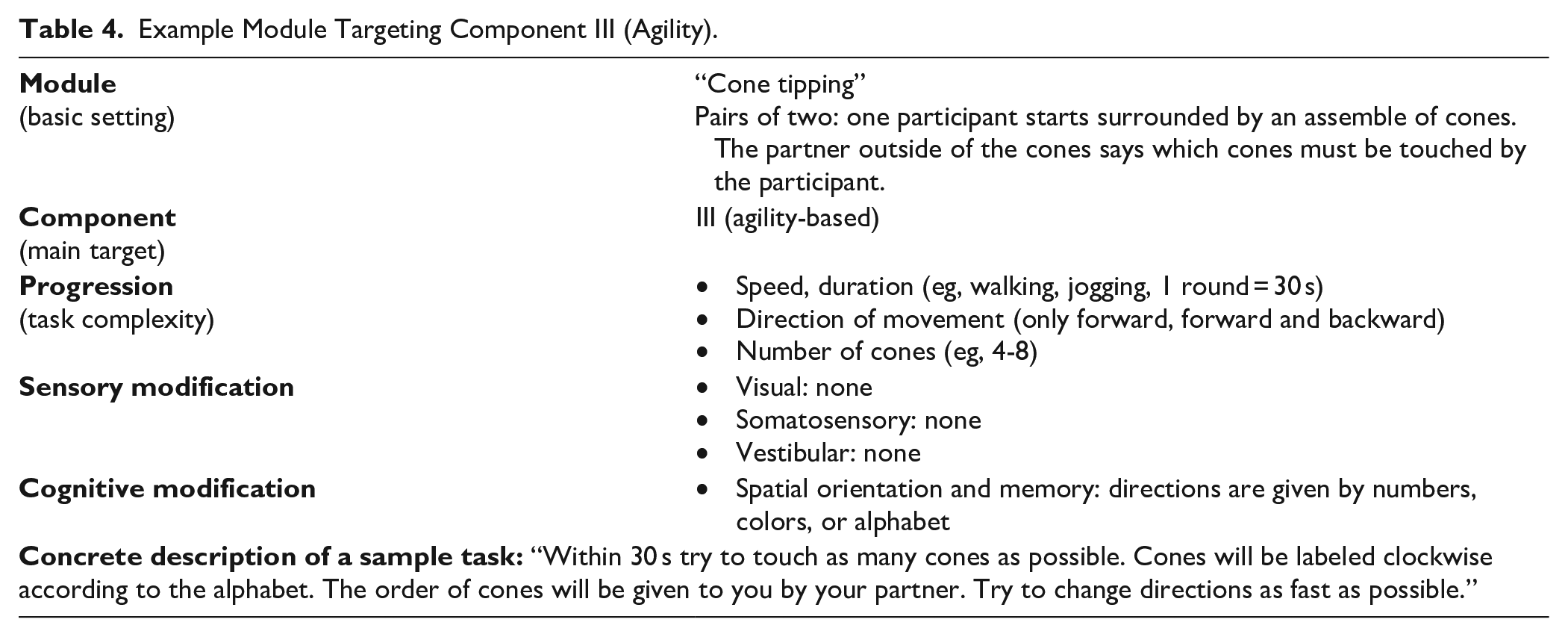
Example Module Targeting Component III (Agility).
Component I: Standing Balance
As described, pwMS exhibit deficits in the control of their center of mass during quiet stance. Furthermore, pwMS exhibit deficits in central sensory integration, that is, pwMS have problems integrating incoming sensory information through the visual, somatosensory, and vestibular channels. 40 Exercising in different sensory contexts (eg, eyes-closed, standing on a compliant surface, performing head turns) and different standing positions (eg, normal stance, feet together, tandem stance etc.) can provide a useful and clinically feasible way to improve standing balance and sensory integration.1,40 Standing balance exercises can furthermore be easily progressed with secondary tasks such as catching an object, alone or with a partner, to provide external perturbations, and even cognitive-motor dual-tasking. As such, these exercises give the executing therapist good options for individualization to the needs of the participating individuals. Standing balance exercises should always be performed with sufficient challenge.1,16,21,26,41 Providing the right amount of challenge can be regarded the primary objective of the therapist, especially if participants are inexperienced with this type of training, and if they have to perform movements, they normally tend to avoid.26,32 Fear of falling and general deconditioning can result in reduced self-efficacy regarding balance. 21 Therefore, pwMS should be encouraged to exercise to their limits of stability, 16 while the therapist is responsible to monitor safety.
Component II: Dynamic Balance (Including Functional Leg Strength)
There is evidence for high task-specificity related to balance training in healthy individuals. 42 The capacity to balance is based more on the sum of specifically learned balance tasks, rather than on a general capacity that can be improved irrespective of the balance tasks that were trained in the past. 42 Recent systematic reviews have advocated the adoption of ecologically relevant balance tasks. 16 Therefore, dynamic balance tasks, including stepping, and locomotion, play an important role in MAT besides standing balance. Importantly, depending on the configuration of the drill, challenges for reactive balance can and should also be incorporated (eg, when reacting to commands of the partner or the therapist, see Table 3). Reactive balance can be characterized by motor control strategies applied in response to postural perturbations such as trips. Impairment in reactive balance might be a major cause for falls. A recent meta-analysis has shown that pwMS have worse reactive balance compared to healthy controls across a range of measures (eg, shorter reactive step, more recovery steps needed), which might be caused by a considerably longer response time to initiate balance recovery. 43 Critically, the meta-analysis also indicated that adaptability of reactive balance is still intact in pwMS, mainly via improved “feedforward” mechanisms (ie, using prior knowledge to predict and fine tune motor commands).
Lastly, Component II can also include tasks that involve a higher demand for functional (eccentric) leg strength (eg, variations of lunging, that also provide reduced base of support), with a more conventional way of prescribing exercise such as repetitions and sets. For reasons already mentioned, no seated exercises or weight training machines are part of MAT.
Component III: Agility-Based Exercises
In the exercise sciences, agility has been defined as “a rapid whole-body movement with change of velocity or direction in response to a stimulus” by Sheppard and Young 44 (eg, an attacker evading a defender in football). This whole-body movement is connected to diverse footwork strategies at various speeds. It has received the most interest from the field of team-sports. Although there have been some inconsistencies, it is generally accepted that “agility has both movement and reactive elements.” 45 Agility is different from “simple” change of direction tasks, as the movement is not executed pre-planned, but in response to a stimulus. On a playing field, it includes a high degree of complexity, variability, and unpredictability. Regarding fall prevention, agility seems to be critical, as situations predisposing a fall never occur pre-planned. In this context “perception-action coupling,” (ie, feedback mechanisms 43 ) might be as important to evade a fall, as it is to evade a defender in football. It has been shown that kinematic and kinetic variables differ when comparing planned versus unplanned side-stepping, suggesting different motor control strategies when reacting to a stimulus. 46 A key difference of conventional dual-task training and agility is, that dual-task training frequently involves performing predetermined tasks, like subtracting sevens while walking on a treadmill. Hence, the participant has prior knowledge of the task he is supposed to perform, and when to perform.
In the first meta-analysis related to MAT in older adults, studies were required to include at least 2 “traditional” training domains (strength, balance, endurance) plus mandatory agility-like exercises. 34 Agility-like exercises were described as comprising coordination or change of direction and velocity tasks. Thus, the authors did not require the agility-related tasks to include responding to a stimulus. Hence, to date it is still unclear to what extent agility-related exercises for older adults and pwMS should focus on responding to a stimulus, or whether “mere” change of direction training (including cutting maneuvers, turns, stop, and go patterns) can already be beneficial for these target groups.
In MAT for pwMS a clear separation of Component III from the first 2 Components exists in the speed of movement. Component III specifically includes fast locomotion, including fast gait, and running, if possible. Tasks here also involve the highest amount of reactive balance with demands for feedback control mechanisms (ie, exposure to perturbations that remain highly unpredictable), 43 such as in passing and stopping a soccer ball with a moving partner. Further, the Modules also provide the highest cardiovascular challenge with an interval training-like stimulus, which can be regulated via the duration of a drill.
A Symbiosis? The MAT, PRIMERS, and Reserve Frameworks
Why is a skill originally developed in the context of team sports and the exercise sciences important for exercise training in pwMS? Are complex, variable, and unpredictable movements important at all for patients, never on a playing field? One answer could lie in the “Prevention Model of Reserve and Brain Maintenance in Multiple Sclerosis.” 6 One premise of this model is, that the best treatment for MS might be prevention of decline. The concept of reserve was based on the observation that pwMS can have similar burden of disease but very different functional impairments. 47 Thus, there must be factors that protect one person against functional decline more than others. A patient will “enter” the disease with a certain amount of reserve in different categories. Besides cognitive reserve, as stated by Brandstadter et al, 6 there might be something like physical or motor reserve as well, protecting somebody with good premorbid balance from gait impairments for a longer time. Interestingly, like the concept of agility, the concept of brain maintenance has been taken from the aging literature to characterize the modulation of reserve over time through protective and risk factors. MAT might be a way for persons with mild disease to improve their functional reserve via processing and integrating multisensory exercise-related stimuli, which builds a bridge to another recently proposed exercise framework for pwMS: PRIMERS (PRocessing, Integration of Multisensory Exercise-Related Stimuli). 3 In 2018, Sandroff et al published this framework to answer the question “what is it about exercise, in particular, that might induce brain changes and secondary behavioral/performance improvements?” in pwMS. They framed exercise as a highly complex behavior involving the coordinated activation of nearly every physiological system in the human body. Among the implications of their framework, they state that exercise training interventions that involve a greater degree of neurophysiological sensorimotor demands should result in more robust brain and behavioral adaptations. MAT for pwMS could offer just that. The group-training format could further act as an enriched environment compared to exercising in isolation. 3
Recommendations
Providing the MAT framework to the field of MS could act as a reference for future multimodal group-training studies and clinical practice. Especially, as standardized research methodology and innovative training programs directed toward meeting the demands of “real-life” situations are lacking for pwMS. 48 It might also serve to introduce the concept of agility to the field of MS, as it has been confined to the fields of athletic performance and aging. It could further provide a framework that is testable in clinical research and has a theoretical basis, potentially improving consistency of interventions in research studies. 4
With respect to recommendations for practice, establishing MAT in routine care will necessitate the use of implementation methodology. 49 The group-training format requires the establishment of sound in- and exclusion criteria. At this point, we propose pwMS should be able to perform several steps in a jogging motion, be relatively pain-free, and without serious cognitive impairments, that interfere with understanding of the instructions. We would also consider age above 70 years for pwMS to be a barrier for participation, as the aging process on top of MS could be too much of a security risk when performing certain aspects of MAT and severe cognitive problems are more common. In our experience, the inclusion criteria mostly apply to pwMS still in a working age, who walk without an assistive device. However, there might occasionally be persons using a cane or walker in daily life, who are still able to participate when managed with close attention from the therapist. Due to the many possibilities of progression, there is no “upper limit” for inclusion. Regarding patient characteristics, that might be favorable for responding to MAT participation, in our experience, motivation and prior experience with exercise play an important role. If a patient has the goal to improve his or her balance or get back to high-level mobility tasks (“I want to run again”) this psychological level could impact physical outcomes in MAT.
MAT might also be suitable as a framework for interventions in a group-setting with mixed neurological diagnoses. To maximize the use of resources, combining pwMS, stroke, and Parkinson’s Disease in group-settings has recently been proposed as a promising approach for falls prevention research. 50 This might be equally useful when establishing MAT group-training in inpatient and outpatient neurological settings. Regarding equipment and staff, we recommend a group with a maximum of 8 participants in a room equivalent to 1 basketball court, to provide enough space for accelerating and decelerating etc. A skilled clinical exercise professional, that can progress and modify Modules according to participating individuals is a cornerstone of MAT. Again, we refer to the cautious gait pattern, low balance self-efficacy, and the avoidance of certain movements in many pwMS.21,26,32 Targeting these aspects might require directly supervised training. While one goal of MAT is to challenge pwMS in multiple areas, inactive pwMS might be at risk of heightened fatigue, when starting MAT. Participants should be advised to take brakes and monitor their fatigue. Considering the higher risk for falls in the described population, especially for Component III an individualized dose is required to minimize falls but still achieve measurable benefits. If a participant has a high risk of falling, it is likely that he or she will experience benefits even if the complexity of agility-based tasks is reduced. Conversely, improvements will be less likely if individuals with higher gait stability do not receive the challenge they need.
With respect to recommendations for research, impact of MAT on several outcome measures will be worthwhile studying. Below, we will discuss some outcomes from proximal to more distal targets. As noted, sensor-based outcomes are appropriate to quantify spatiotemporal gait changes in milder disability.11,15 Besides spatiotemporal measures, other sensor-based outcomes might be useful to quantify whether MAT improves the efficiency and economy of motor control. These include measures of complexity51,52 or movement smoothness. 53 Another worthwhile measure would be the energetic cost of walking, which is based on oxygen consumption during walking. 54 Several studies have recently described associations of sensor-based outcomes during gait trials with perceived state fatigability (ratings of fatigue while performing a task), 55 objective motor fatigability (deterioration of objective performance during a motor task), 52 and trait fatigue (self-report of fatigue experienced over a longer time-period (eg, several weeks)).12,52 Sensor-based and fatigue-related outcomes of intervention studies applying MAT should be compared to more traditional, unimodal types of exercise (ie, aerobic, or resistance exercise) to confirm that incorporating more sensory and cognitive stimuli is superior in affecting these outcomes, and potentially superior as a reserve-building activity. On the other hand, it will be important to study whether MAT for pwMS can provide similar neuroprotective stimuli as has been shown for endurance-type training with high cardiovascular demands. 56 Exercise has also been proposed has a (supportive) disease-modifying therapy.57,58 Thus, MAT should also be compared to unimodal exercise programs that have been designed to study annual relapse rate and global brain atrophy derived from neuroimaging. 59
Lastly, it will be important to show how MAT is able to improve “classic” fitness parameters, such as maximal strength, or cardiorespiratory fitness in comparison to unimodal approaches. Not providing adequate benefits would result in MAT having only compromised value for general health. Table 5 provides an overview on research milestones for MAT in pwMS.
Research Milestones.
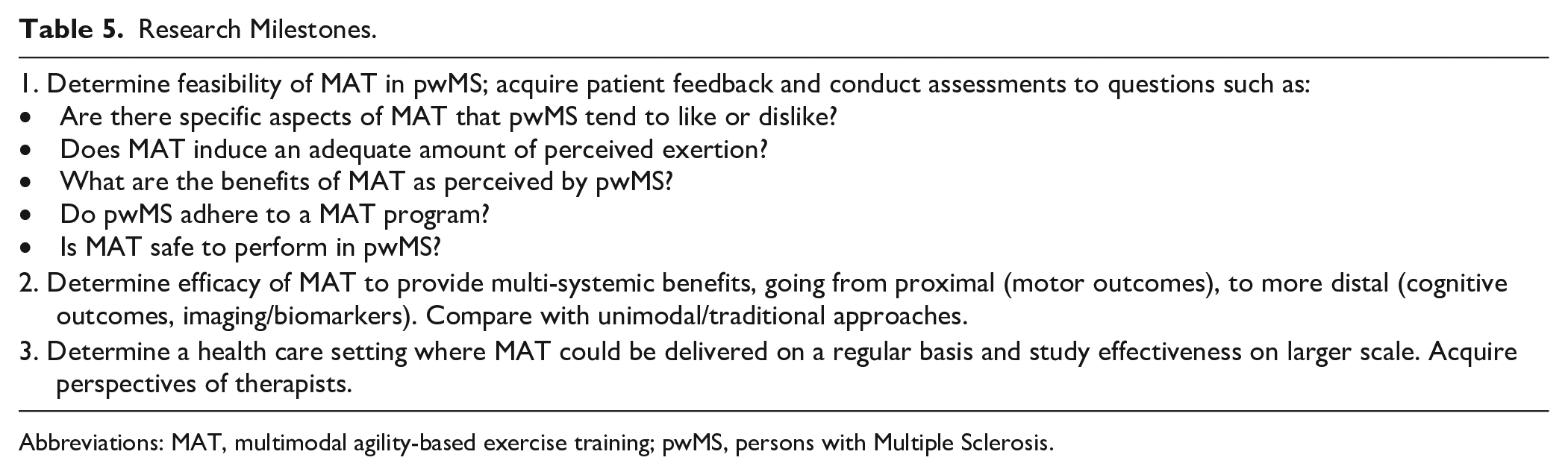
Abbreviations: MAT, multimodal agility-based exercise training; pwMS, persons with Multiple Sclerosis.
Interestingly, multimodal agility-based exercise has also been conceptualized 60 and already performed in patients with Parkinson’s Disease.61,62 In several papers, Tollár et al62,63 and Hortobágyi et al 64 applied similar aspects of training (eg, gait training, coordination training, balance exercises, including change of direction, and sensory integration) to the ones described here, while also incorporating exergaming (Xbox Kinect). They were able to show, that “supervised, high-intensity sensorimotor agility exercise” was able to improve motor outcomes, and quality of life, while also contributing to the least increase in levodopa intake with continued training over 6 years. 64 This also supports motor outcomes to be the most proximal targets of MAT for pwMS.
Regarding the concept of agility itself, debate of what constitutes agility in general is still ongoing. Thus, the aspects of agility, that are important for pwMS must be further elucidated (eg, change of direction, reacting to a stimulus, speed of movement, etc.). Similarly, the transferability of training effects to everyday function must be examined. 42 When considering MAT as a reserve-building activity, ongoing training may be needed to drive lasting neuroplasticity in pwMS. 65 Existing, evidence-based group-exercise programs such as FAME for stroke survivors can serve as a good example to develop MAT for pwMS. 66
In conclusion, when considering the gait and balance deficits with several underlying causes of pwMS, and the difficulties of pwMS to be physically active, an approach of exercise training that (I) addresses these multifaceted motor control problems, (II) is fun, social, relevant to daily life, and (III) is time-efficient, seems to be promising.
As already stated by Motl et al, 29 several things can be learned from the gerontology literature and applied to pwMS. The MAT framework might be one of them.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.