
Abstract
Background
Prospective memory (PM) failure can limit independence and productivity following traumatic brain injury (TBI). Compensatory strategy use may ameliorate the effect of PM impairment on daily life but requires sufficient self-awareness. Metacognitive skills training (MST) can facilitate self-awareness and strategy use and may improve the efficacy of PM rehabilitation.
Objective
To evaluate the effectiveness of compensatory strategy training (COMP) with an MST component (COMP-MST) for reducing everyday PM failure and improving psychosocial integration in adults with moderate–severe TBI, compared to COMP alone and a control condition. Secondary aims were to evaluate the effect of training on psychometric PM test scores, strategy use, self-awareness, and level of care.
Methods
Assessor and participant-blinded randomized controlled trial with 52 participants (77% male, mean age = 39.0. SD = 13.6) allocated to 3 groups: COMP-MST, COMP, and waitlist control. Interventions were delivered over 6 weekly sessions. Measures were collected pre- and post-intervention and 3-month follow-up. Data were analyzed using unstructured linear mixed-effects modeling for repeated measures and planned contrasts between time-points for each group.
Results
The models showed no significant differences between the groups on primary or secondary outcome measures. Significant pre–post intervention improvements were found for significant other’s ratings of everyday PM failure for both intervention groups but not the control group, with medium to large effect sizes. Clinically relevant improvements on primary outcomes were found for participants across all 3 groups.
Conclusions
This study found no significant benefits of combining MST with COMP for improving everyday PM and psychosocial integration.
Clinical Trial Registration:
Australian and New Zealand Clinical Trials Registry https://www.anzctr.org.au/ ACTRN12615000996561
Keywords
Introduction
The most commonly reported cognitive problem after traumatic brain injury (TBI) is memory impairment.1 -3 Prospective memory (PM) is the ability to remember and carry out plans and intentions in the future, which is a critical skill used daily for independent living.4,5 Examples of PM include remembering to attend an appointment, take medications as prescribed, or pay a bill on time. PM is a complex process involving not only retrospective memory to recall the intended action, but also executive functions to enable planning of timely actions, and metacognitive skills for self-evaluating and monitoring performance.3,6 The anterior prefrontal cortex and frontoparietal networks, which are vulnerable to trauma, are considered to be the neural basis for PM and are also involved with executive and metacognitive functions.2,7,8 Studies show that people with TBI have more difficulty with prospective remembering than people without brain injury.8 -11 Furthermore, those who experience PM problems require greater levels of care, and have poorer social and work participation.5,12,13 Optimizing PM function through rehabilitation is, therefore, important to enhance community re-integration outcomes.
PM rehabilitation encompasses remedial or restorative approaches which aim to retrain PM through repetitive practice of PM activities, and compensatory approaches which aim to minimize the effect of PM impairment through the use of external aids or strategies such as diary training.3,12 -14 There are potential benefits of compensatory approaches over remedial approaches. The intensity and duration of training required for improvement in PM in daily life is not as high for compensatory interventions. 12 Additionally, although remedial approaches have been shown to improve PM task performance in within-subjects designs,13,15 skills generalization beyond training activities to everyday situations has not been established. In a broader neurological sample, das Nair and Lincoln 16 found that individuals reported better emotional status following compensatory memory rehabilitation compared to those receiving a remedial intervention. Compensatory PM approaches include training in strategy use such as note-taking, making lists, establishing routines, and training in the use of assistive technology. 3 Assistive technology traditionally involved paper-based diaries and calendars, and alarms. Advances in technology have seen increasing use of electronic devices such as pagers, mobile phones, desktop calendars, and smart watches to compensate for impaired PM by cueing actions through timely reminders.17 -19 Compensatory strategies have relevance to everyday life, and their use can be generalized into real life contexts, as well as having the beneficial effect of reducing cognitive demand.3,20 Despite these potential benefits and common prescription in brain injury rehabilitation, 19 the most effective methods to train individuals with severe TBI to use compensatory strategies in daily life are yet to be established.
Studies with small TBI samples have shown that memory problems can be reduced by training in the use of environmental alarms and reminders, 21 calendar software, 22 television assisted prompting, 23 content-free cueing via text messaging,14,24 smartphones combined with internet-based calendars, 25 and smartwatches. 26 A randomized controlled trial (RCT) 27 of 63 participants with TBI that used a waitlist control group found that an alphanumeric paging system (NeuroPage) significantly reduced everyday PM problems. Another RCT 28 with 42 participants with acquired brain injury found handheld mobile personal digital assistants with built in auditory alarms and calendars (technology now commonly incorporated into smartphones) improved everyday memory functioning relative to standard care. Our previous RCT with 45 participants with TBI, found that training in the use of paper-based diaries (incorporating note-taking and cueing strategies to develop habitual use) also improved PM and strategy use compared to an active control condition. 29
Notwithstanding these positive findings, the uptake of compensatory strategies in everyday life may be compromised by impaired self-awareness following TBI due to damage to the frontal lobes and connecting pathways.30,31 Self-awareness, or metacognitive knowledge, refers to the ability to recognize limitations, understand the functional implications of changes due to brain injury, anticipate when a problem may occur and select an appropriate strategy to avoid it. 30 Impaired self-awareness poses a major obstacle to rehabilitation engagement and outcomes. 32 Our previous RCT compared 8-sessions of compensatory strategy training (COMP) to a control condition involving remedial, repetitive practice of PM tasks. 29 The COMP group demonstrated greater improvements in PM performance and strategy use but these did not extend to significantly greater everyday PM performance or psychosocial functioning. Half of the sample in the trial was also randomized to receive 2 sessions of self-awareness training prior to the PM training. Contrary to the hypothesis, self-awareness training did not result in better generalization of strategy use to daily life. Two sessions may have been insufficient to have a treatment effect on level of self-awareness, or alternatively, retention of new knowledge from these sessions 2 weeks prior to the commencement of PM training may have been limited. Potentially, outcomes may be enhanced by incorporating self-awareness training concurrently with PM compensatory training in each session.
Recommendations for rehabilitation of people with impaired self-awareness following TBI support incorporating metacognitive strategy training or metacognitive skills training (MST). 33 The aim of MST is to coach individuals in self-monitoring performance, identifying and self-correcting errors and generating strategies for future use. 3 Techniques used in MST, such as therapist and video feedback, self-prediction and self-evaluation of performance, structured opportunities for participant identification and self-correction of errors during performance, and self-instructional and role-reversal techniques, have been demonstrated to improve self-awareness and self-regulatory skills.34 -39 Apart from our previous trial that incorporated brief self-awareness training (2 sessions) prior to PM strategy training, 29 there has been no research on the application of MST to PM rehabilitation. Therefore, we developed a compensatory PM training program with MST techniques (COMP-MST) embedded in the training over 6 weekly sessions. The aim of the MST was to provide opportunities for patients with TBI to gain self-awareness of personal PM challenges and the potential usefulness of strategies, self-reflect on their PM performance, learn to self-monitor their performance, and to self-correct and prevent PM failures. We proposed that individuals receiving COMP-MST would become more aware of the extent of their PM failures, which in turn would contribute to gains in everyday PM performance due to generalization of strategy use beyond the therapy setting.
This study aimed to evaluate the effectiveness of COMP-MST for reducing the frequency of everyday PM failure and improving psychosocial integration in adults with moderate to severe TBI living in the community, compared to COMP training alone and to a waitlist control condition. Secondary aims were to evaluate the effect of COMP-MST on psychometric PM test scores, strategy use, self-awareness, and level of care following TBI. We hypothesized that:
COMP training will demonstrate significant improvement at post intervention and maintenance at 3-months post intervention on everyday PM performance and level of psychosocial integration compared to no intervention (ie, waitlist), and that compensatory PM rehabilitation combined with metacognitive skills training (COMP-MST) would be more effective than COMP training alone;
COMP training will demonstrate significant improvement post-intervention and at 3-months follow-up on secondary outcomes (namely PM function on psychometric testing, strategy use, self-awareness, and level of support needs) compared to no intervention (ie, waitlist) and, that COMP-MST training will be more effective than COMP training alone.
Methods
Setting, Study Design, and Participants
The Consolidated Standards of Reporting Trials Statement (CONSORT) was used to guide the reporting of this study (see CONSORT Checklist in Supplemental file). The design of the study was an assessor and participant-blinded RCT with 3 arms: COMP-MST, COMP, and waitlist control. Outcome measures were collected at pre- and post-intervention and 3-month follow-up. Full details of the methods have been outlined previously. 40 There were no changes to the methods after the trial commenced. Ethical approval was granted by the Metro South Human Research Ethics Committee (HREC/15/QPAH/090), the University of Queensland Medical Research Ethics Committee (2015000644), and the Griffith University Human Research Ethics Committee (PSY/93/15/HREC). The trial was registered with the Australian and New Zealand Clinical Trials Registry (ACRN12615000996561).
Individuals with moderate to severe TBI and their significant others (SOs) were recruited from the community via referrals from a specialist brain injury rehabilitation unit, a state-wide brain injury outreach service, and private rehabilitation practices in Brisbane, Australia. Inclusion criteria were: (i) diagnosis of moderate or severe TBI (as determined by Glasgow Coma Scale [GCS] score and/or duration of post-traumatic amnesia [PTA]); (ii) adults in the working age range; (iii) had a SO available to participate in the study; (iv) scored within the impaired range on baseline PM test performance or PM problems reported on the Brief Assessment of Prospective Memory (BAPM) by the participant or their significant other; (v) at least 1 month post discharge from hospital; (vi) no prior brain injury or hypoxic injury; (vii) adequate receptive and expressive English communication skills; (viii) ambulant or independently mobile in manual or electric wheelchair; and (ix) able to attend the hospital for the 6-week intervention. Individuals were excluded if they were unable to provide informed consent, had not emerged from PTA, were confused or disoriented, had communication difficulties limiting their comprehension of written or spoken language, and/or were assessed by their treating occupational therapist as having very severe global cognitive impairment.
Procedures
Following recruitment, demographic and diagnostic variables were collected from medical records and self-report. Participants completed baseline assessments and were randomly allocated to 1 of the 3 groups. At baseline, participants completed a brief battery of neuropsychological tests of attention (Digit Span, Trail Making Test A), memory (eg, Hopkins Verbal Learning Test), and executive function (Controlled Oral Word Association Test, Trials B, Hayling Sentence Completion Test) and the Test of Premorbid Functioning 41 to summarize and describe participants’ level of cognitive impairment. The COMP-MST and COMP groups completed a 6-week program (see “Interventions”), and the waitlist control group received care as usual for 6 weeks. Participants were re-assessed following the initial 6-week intervention period and again at a 3-month follow-up by an assessor who was blind to group allocation. Participants in the waitlist control group were then offered the COMP-MST program.
Randomization
Randomization, stratified according to PM function on the CAMPROMPT 42 (“impaired/borderline,” “less impaired”), was undertaken after baseline assessment. The random allocation was conducted independent of staff involved in the interventions and data collection. The sequence was developed using permuted block randomization. Sequentially numbered and sealed opaque envelopes containing group allocation were used to conceal allocation to the pre-determined sequence.
Interventions
Both the COMP and COMP-MST interventions had manualized protocols and were conducted by 4 occupational therapists who had prior experience working with people with brain injury. A researcher provided 1 to 2 training sessions initially to therapists and ongoing supervision in which reflective learning was encouraged. Fidelity checks were completed using a structured checklist for a random sample (20%) of sessions using audiotaped recordings by a research assistant not otherwise involved in the study. The interventions were delivered 1:1 in an outpatient clinic setting. Sessions were comprised of 0.5 hour metacognitive skills training plus 1.5 hour compensatory training (COMP-MST) or 0.5 hour active control plus 1.5 hour compensatory training (COMP). If applicable, participants continued to receive other outpatient rehabilitation services during the intervention period that were not focused on PM rehabilitation or metacognitive strategies.
Compensatory Strategy Training (Completed in COMP and COMP-MST)
COMP included: education on PM and the impact of TBI on PM and selection of an appropriate assistive technology to compensate for PM impairment (eg, smart phone or electronic calendar) (session 1); practice in using the assistive technology and effective notetaking skills for recording reminders (session 2); explaining their strategies to a family member or friend to reinforce habit development at home (session 3); development of time management skills through documenting a weekly routine on a planner and use of a “to do” list, organizational strategies such as a designated station for keeping keys, wallet, and phone at home, and an effective method of transporting them (eg, backpack, hand bag) and use of reminder alerts ahead of scheduled events to allow time for preparation (session 4); and reinforcement of strategy use, training for strategy generalization to everyday life, generation of PM strategies during discussion of a video of everyday PM scenarios, and a maintenance plan for ongoing use of the assistive technology (sessions 5 and 6).
Metacognitive Skills Training (Completed in COMP-MST Only)
MST techniques were incorporated within each PM training session alongside COMP. Each week participants completed a “memory journal” to record any specific instances of PM failure or independent strategy use in everyday life. The journal was discussed in each session, accompanied by anticipation of potential PM failures in relation to forthcoming events/activities in the next week, and identification of preventative strategies. Manualized MST activities were used in each session including: Training in use of memory journal (session 1); a role modeling activity involving watching a video of 2 individuals with TBI describing their PM failures and strategies, and discussion of similarities in their own life with the therapist (session 2); experiential feedback from engagement in a board game activity with embedded PM tasks accompanied by self-predictions beforehand and self-evaluations afterward (session 3); video-feedback of their performance on the board game activity from the previous week, and self-evaluation (session 4); written feedback in the form a progress report from the therapist (session 5); and a self-awareness generalization activity involving an interview about the broader implications of their TBI and future goals (session 6).
Active Control for Metacognitive Skills Training (Completed in COMP Only)
Participants in the COMP group received a similar amount of therapy time allocated to “warm up” cognitive workbook exercises involving attention, visual processing, or information processing tasks that were unrelated to PM or self-awareness (eg, cancellation tasks, word searches, problem solving, calculation tasks, mazes). The COMP group did not receive feedback on their performance on the workbook activities.
Measures
Primary Outcomes
Everyday PM failure was measured using the BAPM, 43 which includes 16 items assessing the frequency of PM failure during basic and instrumental activities of daily living over the past month. Items are rated on a 5-point scale (1 = never to 5 = very often, with a not applicable option). Average scores across all applicable items are calculated with lower scores representing less frequent PM failure. The BAPM has established reliability, a robust factor structure, and criterion-related validity. 43 The level of psychosocial reintegration was assessed using the Sydney Psychosocial Reintegration Scale version 2 (SPRS-2; Form B),44,45 which includes 12 items assessing functioning in the domains of work and leisure, living skills, and interpersonal relationships since injury. Items are rated on a 5-point scale indicating the degree of change since injury (0 = extreme to 5 = not at all). Total scores range from 0 to 60 with higher scores representing better psychosocial integration. There is strong evidence for the reliability and validity of the SPRS-2. 45 The BAPM and SPRS were completed by participants’ SOs to overcome the influence of impaired self-awareness in self-reports by TBI participants.
Secondary Outcomes
The Cambridge Prospective Memory Test (CAMPROMPT) 44 was used to assess PM performance and strategy use (ie, spontaneous note-taking during test performance recorded as yes/no). Global and PM-specific self-awareness were measured using the discrepancy (self-ratings minus significant other ratings) on the Awareness Questionnaire (AQ), 46 and the BAPM. 43 The Care and Needs Scale (CANS) 47 was used to assess level of support needs. All secondary outcome measures have well-established psychometric properties.
Sample Size Estimation
Using G-Power and setting power to .80, alpha to .05, and an effect size of 0.70, it was calculated that 90 participants would be necessary. 40 The effect size was based on the between-group difference in total SPRS score between the COMP-MST and COMP groups in the previous trial 29 (Cohen’s d = 0.70). The SPRS score was chosen because it was the primary outcome variable with the most conservative effect size. The estimated sample size was 26 per group which we increased to 30 to factor in possible attrition based on data from another trial in the same setting (10% dropout). 39
Statistical Analysis
Data analysis was conducted using SPSS version 25 (SPSS, Inc., Chicago, IL). Demographic variables and neuropsychological measures collected at baseline were compared between groups using one-way ANOVAs for continuous variables and Chi-square tests for categorical variables. Discrepancy scores were calculated for the BAPM total scores and AQ score by subtracting the SO’s score from the participant’s score (ie, participant total minus significant-other total). Descriptive statistics were generated for baseline measures and all outcome measures for each group at each time point and variables were checked for normality. An outlier was detected with a PTA duration of 912 days. Missing data were handled using intention-to-treat (ITT) analysis wherein the most recent available data were imputed. 48 Data were examined for demographic or neuropsychological variables that were significantly associated with the outcomes and unevenly distributed between the groups.
Seven unstructured linear mixed-effects modeling for repeated measures (MRMM) tests with maximum likelihood estimation were used to test for group differences on the primary and secondary outcomes, with group allocation (waitlist control, COMP, COMP-MST) as the between-subject factor, and time (baseline, post intervention, 3-month follow-up) as the within-subject factor. The MRMM handles both between- and within-subject variance and specifically accounts for the correlation between the repeated measures. 49
The primary outcome measures included SPRS SO total score and BAPM SO total score and were entered as dependent variables in separate analyses. The secondary outcome variables were CAMPROMPT Total, Note-taking on the CAMPROMPT, AQ discrepancy, BAPM discrepancy, and CANS level, also entered as dependent variables in separate analyses. Fixed effects of group, time, and interaction of group by time were the main estimates (categorical variables) to identify differences between the 3 groups, changes over the course of treatment, and group and time interaction. The MRMMs tests were repeated with baseline performance entered as a covariate (fixed effect) to control for baseline performance. To reduce multicollinearity, all variables included in the model as fixed effects were centered. 50 Random intercepts for participants were included in the model for the correlation of within-person factors at baseline and an unstructured covariance structure was used in the analyses. Analyses were repeated with outliers removed to confirm there were no changes to the results. Planned contrasts between baseline (T1) and follow-ups (T2 and T3) were conducted for each group for primary outcome variables using paired t-tests and Cohen’s d to determine effect size. An alpha level of .05 was employed. To determine if a clinically relevant change occurred for individual participants on the primary outcomes, the reliable change index (RCI) was used. 51 For the BAPM, the RCI was calculated using the baseline standard deviation and the test–retest reliability coefficient (.76), 52 resulting in a change of .74 indicating a reliable change. For the SPRS, an improvement in logit score of 8.23 was considered a reliable change. 45 The number of participants with clinically relevant improvements at T2 and T3 were inspected in each group and for those categorized as having impaired self-awareness versus no impairment of self-awareness on the AQ.
Results
Participant Characteristics
Between October 2015 and June 2019, 76 adults with TBI were screened, 64 were assessed as eligible and 52 were randomized to the waitlist (n = 18), COMP (n = 17), and COMP-MST (n = 17) groups (Figure 1). The sample included 40 males (77%) and had a mean age of 39 years (SD = 13.6). Post-intervention assessments were completed by 49 participants with data missing for 3 participants from the COMP group (14/17, 82%), and 3-month assessments by 45 participants (waitlist control: 16/18, 89%; COMP: 13/17, 76%; COMP-MST: 16/17, 94%). SO data were not returned for 2 participants at any of the time points. Therefore, only the CAMPROMPT (secondary outcome) was able to be analyzed for these participants. All other participant data were analyzed following ITT principles according to original assigned groups. Participant characteristics are presented in Table 1 and baseline neuropsychological test results in Table 2. There were no significant differences between groups on demographic or injury-related variables, or baseline neuropsychological test scores. Approximately half of the participants demonstrated impaired self-awareness at baseline according to discrepancy scores of 4 or greater on the AQ 52 and were evenly distributed amongst the groups (waitlist control: 8/18, 44%; COMP: 9/17, 52%; COMP-MST: 9/17, 52%). Of the 18 participants in the waitlist control group, 15 proceeded to complete the full COMP-MST program, 1 completed 1 session and then withdrew, 1 chose not to do the program, and 1 was uncontactable.
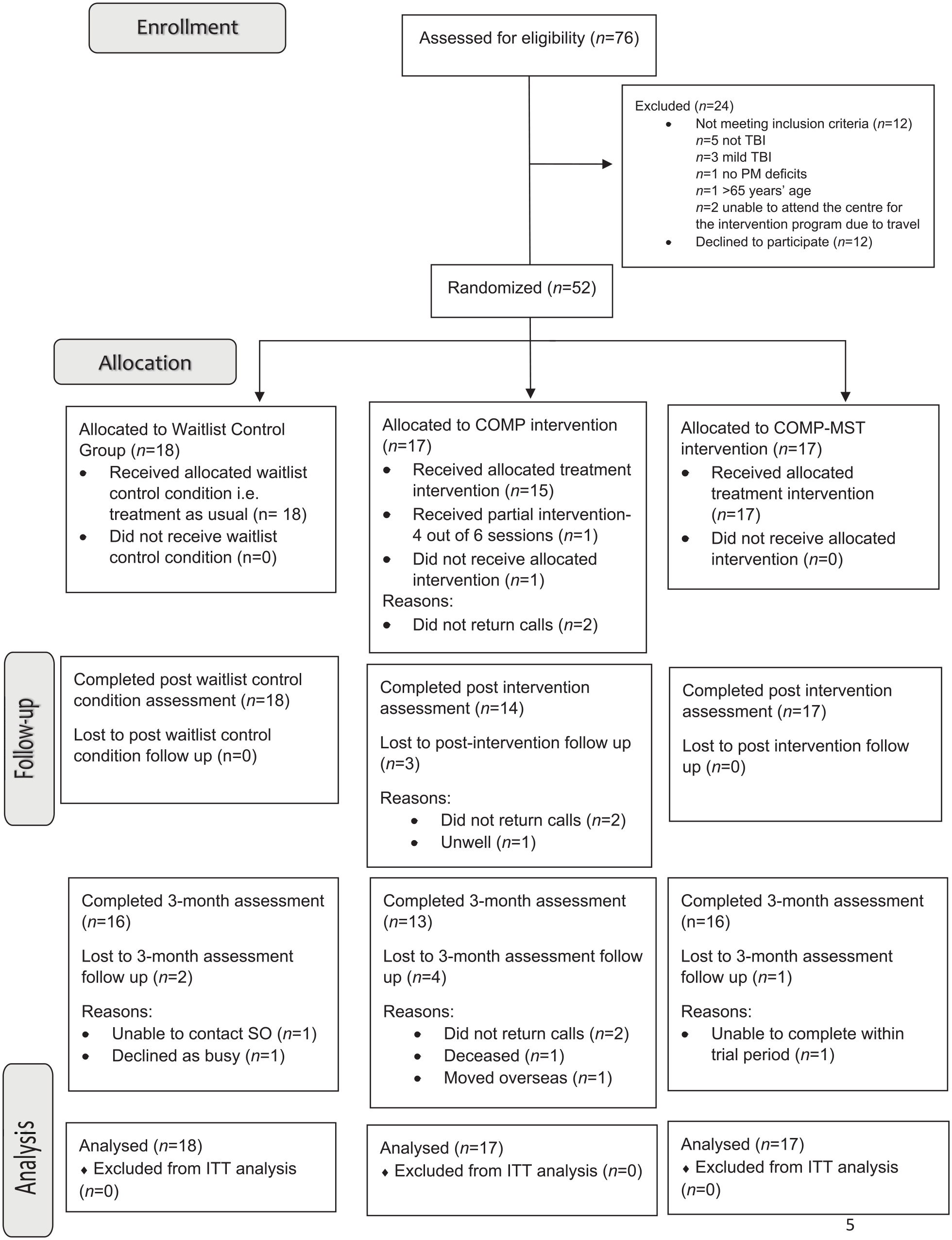
Flow of participants through the trial.
Descriptive Statistics for Each Experimental Group.
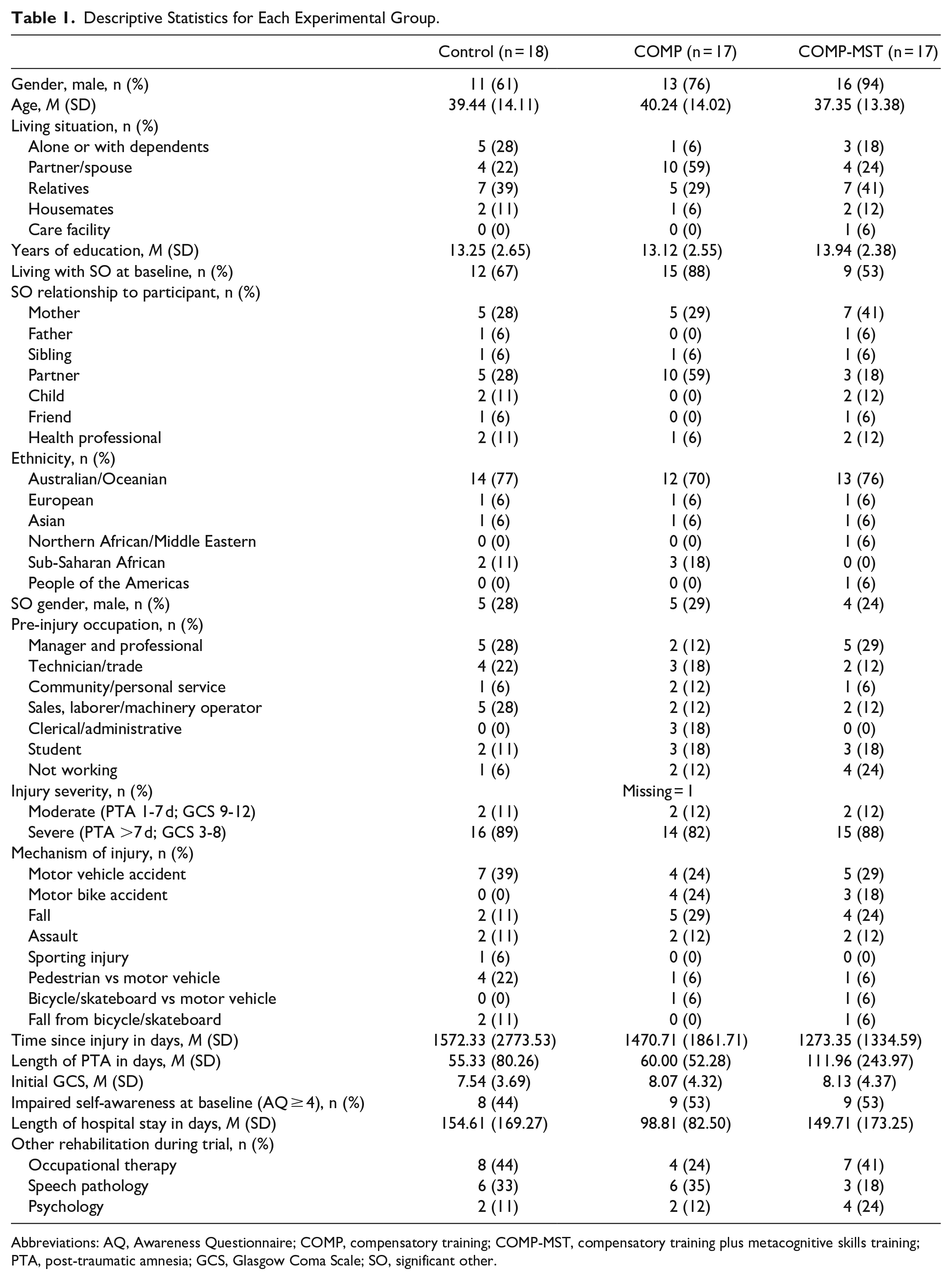
Abbreviations: AQ, Awareness Questionnaire; COMP, compensatory training; COMP-MST, compensatory training plus metacognitive skills training; PTA, post-traumatic amnesia; GCS, Glasgow Coma Scale; SO, significant other.
Baseline Neuropsychological Test Means (SD).
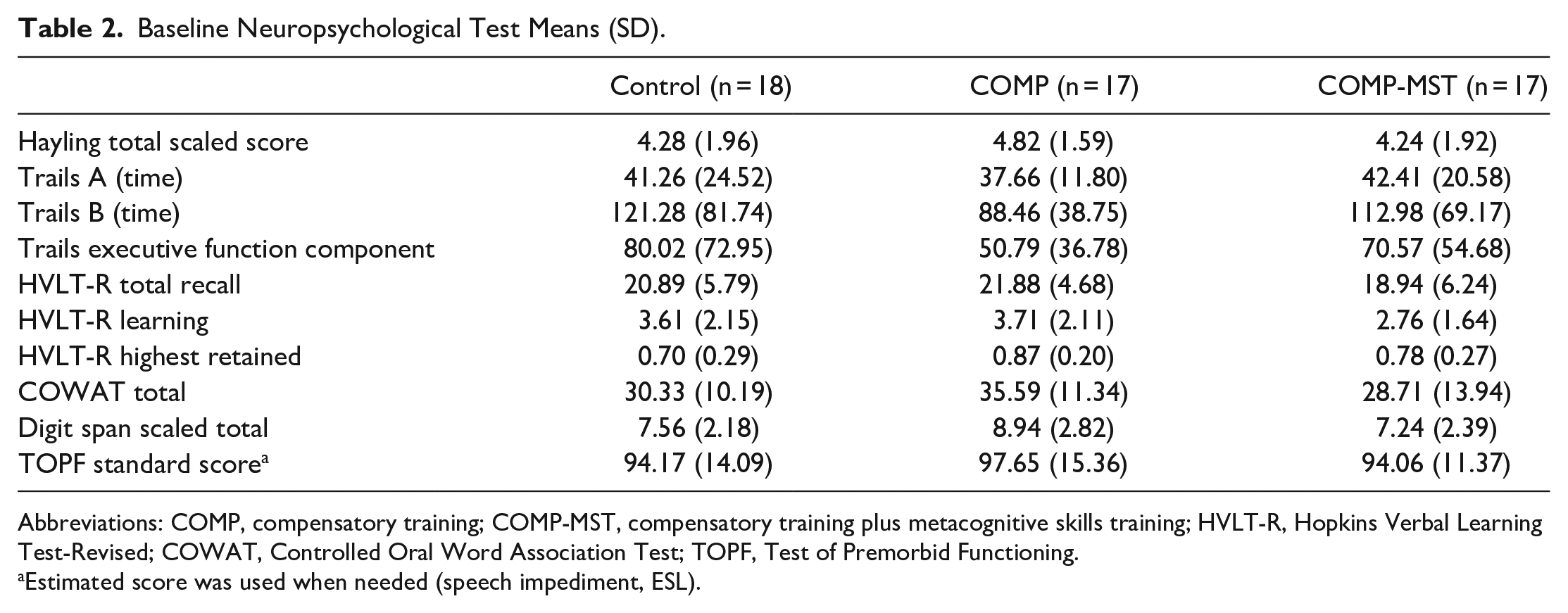
Abbreviations: COMP, compensatory training; COMP-MST, compensatory training plus metacognitive skills training; HVLT-R, Hopkins Verbal Learning Test-Revised; COWAT, Controlled Oral Word Association Test; TOPF, Test of Premorbid Functioning.
Estimated score was used when needed (speech impediment, ESL).
Intervention Fidelity
Fidelity checking showed that the interventions were delivered with 97% adherence (98% COMP, 96% COMP-MST). Variations to protocol occurred due to combining content from 2 sessions, inability to do some tasks with 1 participant who selected a voice-activated personal assistant as his compensatory strategy, sessions varying in length, and components completed in different sessions. Some participants received other rehabilitation services unrelated to PM function during the intervention period (see Table 1) which was not significantly different between groups. The blinded assessors reported that they did not become aware of the group allocation of any participants. One participant partially completed the program (4 out of 6 sessions completed) and 1 participant did not complete any sessions (see Figure 1). There were no adverse events related to the trial.
Effect of Intervention
Primary Outcomes
Data on the outcome measures for the 3 groups at each time point are presented in Table 3. Two outliers were found on the BAPM SO total. Removal of these outliers did not change the results; therefore, they were kept in the analyses. BAPM SO total was found to be significantly skewed. Transformation did not change the overall results, so the untransformed data are reported. Linear mixed models for repeated measures were used to test for group differences on the primary outcomes while controlling for baseline performance (See Table 4). There were no statistically significant mean differences between groups for BAPM SO total score across the time points (F = 0.36, P = .834). A significant group effect was found for SPRS-2 SO total score (F = 4.28, P = .019), however this was no longer significant when baseline performance was entered into the model as a covariate (F = 1.84, P = .169). A significant effect of Time was found for BAPM SO total score (F = 10.38, P < .001) and SPRS-2 SO total score (F = 5.64, P = .005) with improvement over time; however, there were no significant group by time interactions found for either primary outcome variable.
Primary and Secondary Outcome Measures at Baseline, Post-Intervention, and 3-Month Follow Up.
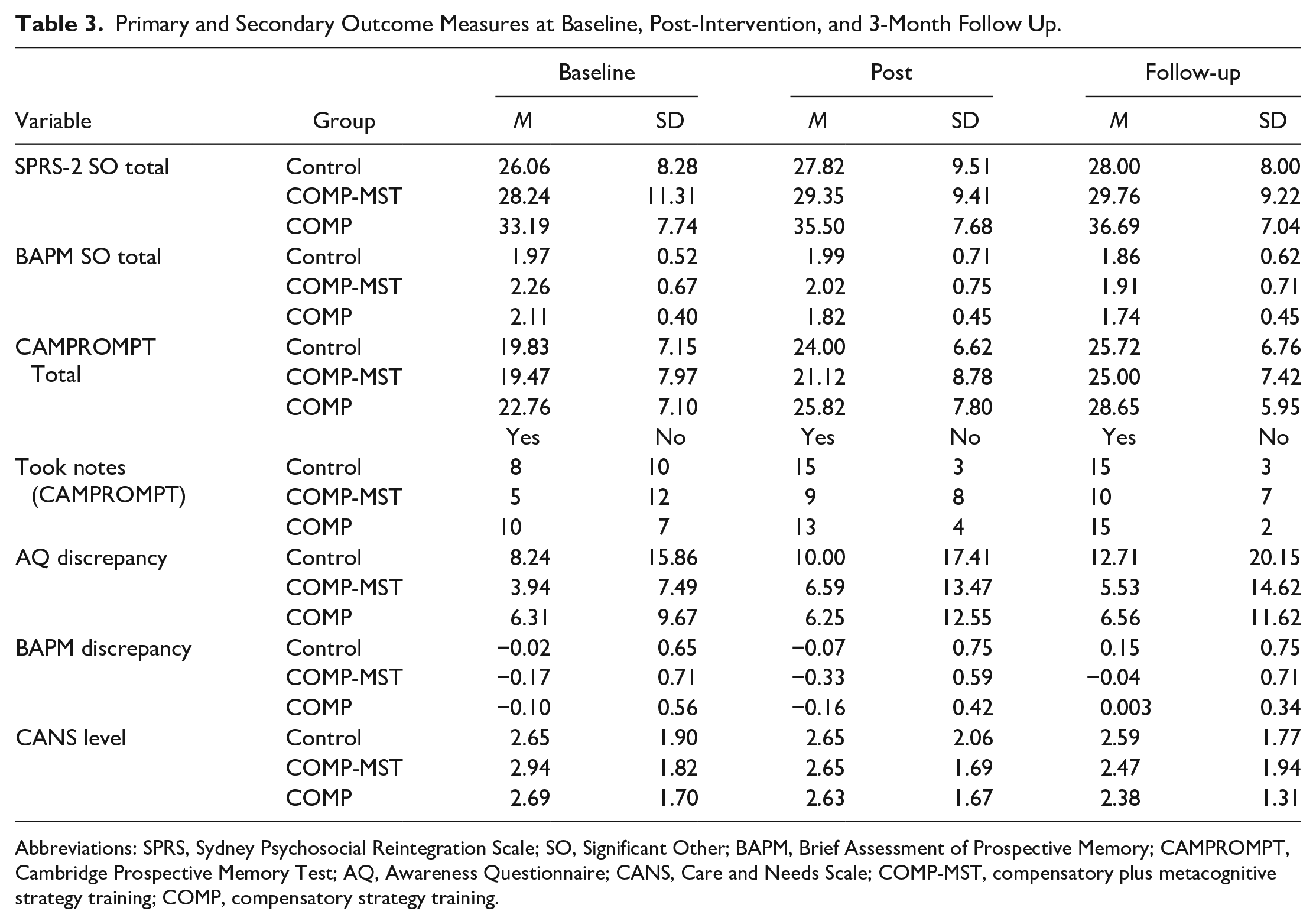
Abbreviations: SPRS, Sydney Psychosocial Reintegration Scale; SO, Significant Other; BAPM, Brief Assessment of Prospective Memory; CAMPROMPT, Cambridge Prospective Memory Test; AQ, Awareness Questionnaire; CANS, Care and Needs Scale; COMP-MST, compensatory plus metacognitive strategy training; COMP, compensatory strategy training.
Fixed Effects Estimates for Each Dependent Variable.
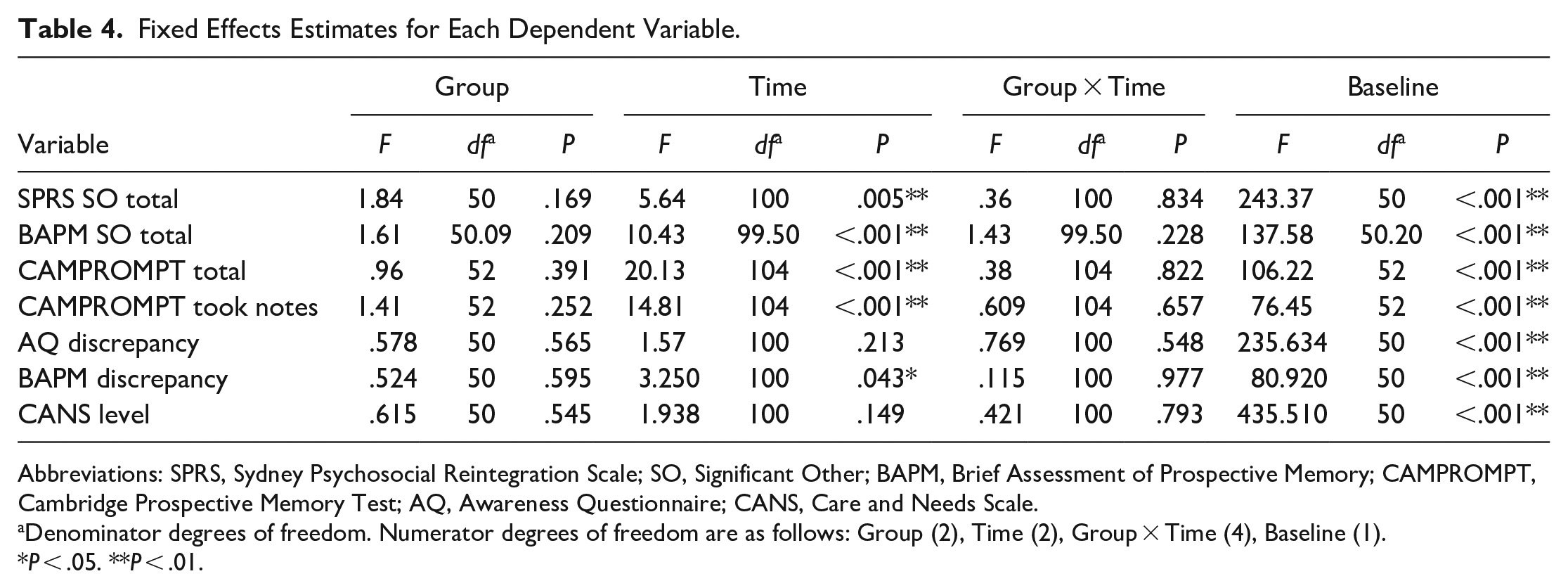
Abbreviations: SPRS, Sydney Psychosocial Reintegration Scale; SO, Significant Other; BAPM, Brief Assessment of Prospective Memory; CAMPROMPT, Cambridge Prospective Memory Test; AQ, Awareness Questionnaire; CANS, Care and Needs Scale.
Denominator degrees of freedom. Numerator degrees of freedom are as follows: Group (2), Time (2), Group × Time (4), Baseline (1).
P < .05. **P < .01.
Secondary Outcomes
Two outliers were found on the AQ discrepancy score. Removal of these outliers did not change the results, therefore they were kept in the analyses. Notetaking on the CAMPROMPT, AQ discrepancy score, and CANS level were found to be significantly skewed. Transformation of these variables did not change the overall results, therefore untransformed data have been reported. There were no between-group differences for any of the 5 secondary outcome measures (See Table 4). A significant effect of Time was found for CAMPROMPT total score (F = 20.13, P < .001), Note-taking on the CAMPROMPT (F = 16.36, P < .001), and BAPM discrepancy score (F = 3.25, P = .043) with all variables showing improvement over time. No significant group by time interactions were found for any secondary outcome variable in either model.
The results of planned contrasts between T1 and post-intervention follow-ups for BAPM and SPRS significant other ratings are displayed in Table 5. There were no significant improvements for the waitlist control group. On the BAPM there was a significant improvement between T1 and both post-intervention time points for the COMP and COMP-MST groups with medium to large effect sizes. There was a medium significant effect for SPRS ratings in the COMP group indicating improvement in psychosocial functioning at the 3-month follow-up. No other contrasts were significant for SPRS ratings.
Planned Contrasts.
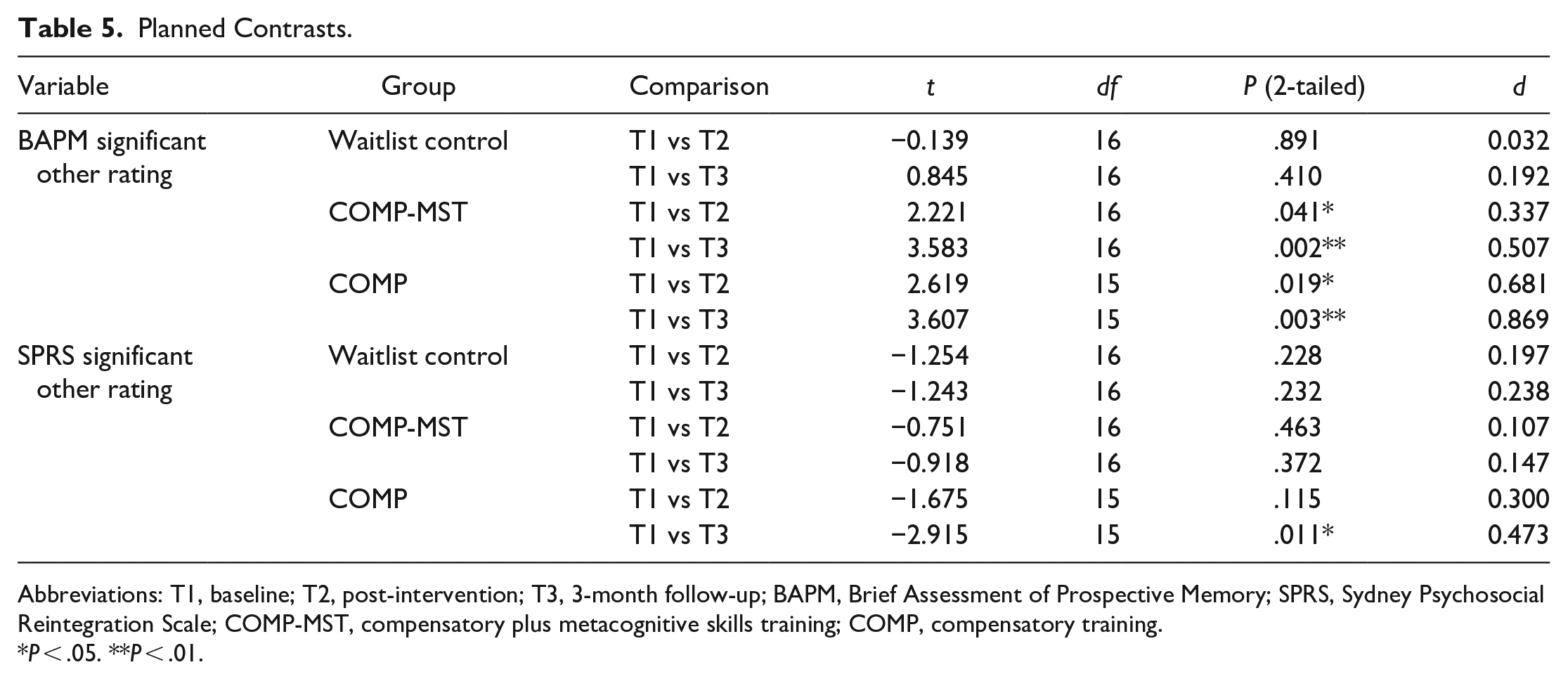
Abbreviations: T1, baseline; T2, post-intervention; T3, 3-month follow-up; BAPM, Brief Assessment of Prospective Memory; SPRS, Sydney Psychosocial Reintegration Scale; COMP-MST, compensatory plus metacognitive skills training; COMP, compensatory training.
P < .05. **P < .01.
According to the RCI, there was a clinically relevant improvement on the BAPM at T2 for 3 participants (2 COMP; 1 COMP-MST). Of these 1 had a baseline AQ discrepancy score indicating impaired self-awareness and 2 did not. Compared to T1, there was a clinically relevant improvement at T3 on the BAPM for 7 participants (2 waitlist control; 2 COMP-MST; 3 COMP). Of these, 6 had impaired self-awareness at baseline and 1 did not.
On the SPRS, there was a clinically relevant improvement at T2 for 7 participants (2 waitlist control; 2 COMP-MST; 3 COMP). Of these, 3 had impaired self-awareness at baseline according to AQ discrepancy scores. Compared to T1, there was a clinically relevant improvement on the SPRS at T3 for 8 participants (1 waitlist control; 3 COMP-MST; 4 COMP). Of these, 4 had impaired self-awareness at baseline.
Discussion
This study aimed to investigate the effectiveness of incorporating MST into a compensatory PM rehabilitation program (COMP-MST). No significant differences were detected between groups receiving COMP-MST, and compensatory training without MST, and waitlist controls. Therefore, the addition of MST provided no benefits over PM compensatory training, which has previously been found to be effective relative to standard care after TBI. 29 Notably, planned contrasts between pre–post intervention scores on primary outcome measures indicated improvements in everyday PM functioning as reported by significant others for both intervention groups (COMP and COMP-MST) but not for the control group. Effect sizes were medium to large suggesting that the interventions may show some promise. Larger effect sizes were found for the COMP group than for the COMP-MST group. Therefore, the results of the planned contrasts did not support the hypothesis that MST would enhance COMP. The MST training did not include any practice of real-life activities in the person’s everyday context such as home or work. Instead, each treatment session only involved discussion about performance on everyday activities over the past week. This may have reduced the effect of the MST component.
Recruitment for this study coincided with the opening of a new transitional rehabilitation service for people with acquired brain injury. Consequently, previous unmet needs for ongoing rehabilitation in the community for people with TBI may have been being met, resulting in fewer participants interested in being involved in a research intervention trial. Despite pursuing multiple avenues to increase the sample size, the final sample of 52 participants fell considerably short of the estimated required sample of 90 participants. Hence, the trial was underpowered in relation to the original estimated sample size, and in relation to the obtained effect sizes. Spontaneous recovery may have presented a confounding factor given that participants were only required to be 1-month post-discharge to be eligible for the study, and that some participants in the wait-list control group showed reliable improvements. However, most participants were more than 2 years post-injury.
The participants in the study may not be representative of the broader populations with moderate to severe TBI. Discrepancy scores on the AQ were generally low, and approximately half of sample did not display impaired self-awareness. The mean AQ discrepancy score for the COMP-MST group, was not in the range indicating impaired self-awareness (ie, ≥4). 53 Awareness of the presence of memory problems impacting on their daily lives may have provided participants with the impetus to volunteer for a PM rehabilitation trial, thus reducing the potential benefits of MST. It is estimated that 76% to 97% of people with severe TBI display impaired self-awareness 54 suggesting that the sample in our study may not be typical. This highlights one of the difficulties in conducting research on interventions for self-awareness after TBI—it may be difficult to recruit those who need it due to the nature of the impairment itself. Another of the pitfall of self-awareness intervention research is the tendency for self-reports of function to be worse post-intervention due to improved awareness of the extent of problems as a direct result of the intervention. We attempted to overcome this by reliance on SO reports of functional abilities instead of self-reports. However, it is possible that SOs’ knowledge of the participants’ daily function may not have been adequate or sufficiently current to be sensitive to change over a relatively short time frame. Although family members were invited to attend sessions with the participant, only a small number attended across all groups, indicating that SOs may not have had accurate updated information on the participants’ everyday PM performance at the post-intervention assessment.
Most outcome measures were selected to detect changes in functioning in daily life, or generalization of strategies to minimize the impact of PM impairment on independent living, social functioning, activities of daily living, and productivity. As such, the measures may not have been sensitive to specific gains in compensatory strategy use because of the program. A clinically relevant change was detected at 3-months follow-up for 8 participants on the SPRS (including 1 waitlist control) and 7 participants on the BAPM (including 2 waitlist controls) whereas only 3 showed improvements immediately post-intervention on each measure. Although the changes between T1 and T3 may reflect general recovery, the higher number of COMP-MST and COMP participants with reliable improvement at T3 suggests that time may be required for use of strategies to have an effect in daily life. Moreover, a 3-month follow-up timeframe may also be too short to detect changes in psychosocial integration.
Use of more targeted outcome measures, such as Goal Attainment Scaling, 55 may have led to different results. The CAMPROMPT was the only outcome measure that attempted to measure the underlying impairment in PM. As the intervention targeted the use of compensatory strategies and did not aim to restore damaged memory functions, we did not anticipate that the CAMPROMPT would show marked improvements as a result of compensatory PM training. We hypothesized that performance on the CAMPROMPT may improve as a result of increased use of spontaneous note-taking in the intervention groups, as we saw in our previous RCT. 29 However, all groups including the waitlist control group, improved in the proportion of participants who took notes. Indeed, across many outcome measures, the trend was for improvement over time regardless of group membership. This may be due to natural recovery or therapeutic gains derived from engagement in the baseline assessment and anticipation of a rehabilitation program.
Although blinded assessors were used in this study, the participants and SOs who provided the outcome data were not blind to group allocation as some were allocated to a waitlist control group and the others to an intervention group. It was also not possible for the therapists delivering the intervention to be blinded.
The non-significant findings in this study highlight the value of Phase II feasibility trials to inform the development of full-scale RCTs, 56 establish multi-site recruitment approaches to ensure adequate recruitment rates and selection of outcome measures that are sensitive to the intervention targets. Consideration of other outcomes such as consumer satisfaction and qualitative reports of the changes that participants have experienced in their lives as a result of participation are also important alongside the quantitative evidence. 57 While there can be a tendency for researchers to only report the results of trials with significant findings, it is also important to report non-significant findings to avoid systemic bias in the published research evidence. 58
This study found no significant effects for a 6-week compensatory PM strategy training program (both with MST and without) on the frequency of PM failure and psychosocial integration for people with moderate to severe TBI. The significant improvements for the intervention groups found in pre–post planned contrasts suggest this may be due to the insufficient sample size. Future research using a larger sample size informed by the effect sizes generated in this study and use of client-centered outcome measures such as Goal Attainment Scaling, may be more effective in establishing the best way to train people with TBI to use compensatory memory strategies in everyday life.
Supplemental Material
sj-doc-1-nnr-10.1177_15459683221110886 – Supplemental material for Efficacy of Prospective Memory Rehabilitation Plus Metacognitive Skills Training for Adults With Traumatic Brain Injury: A Randomized Controlled Trial
Supplemental material, sj-doc-1-nnr-10.1177_15459683221110886 for Efficacy of Prospective Memory Rehabilitation Plus Metacognitive Skills Training for Adults With Traumatic Brain Injury: A Randomized Controlled Trial by Jennifer Fleming, Tamara Ownsworth, Emmah Doig, Christy Hogan, Caitlin Hamilton, Sarah Swan, Janelle Griffin, Melissa Kendall and David Shum in Neurorehabilitation and Neural Repair
Footnotes
Acknowledgements
The authors wish to acknowledge the contributions of Marika Mussawir, Kylie Watson, Jasmine Koo, Giverny Parker, and Freyr Patterson to the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Health and Medical Research Council of Australia, Project Grant APP1083064.
Supplementary material for this article is available on the Neurorehabilitation & Neural Repair website along with the online version of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.